
Theoretically Guided Iterative Design of the Sense2Quit App for Tobacco Cessation in Persons Living with HIV
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Recruitment and Eligibility
2.3. Procedures
2.4. Data Analysis
3. Results
3.1. Study Sample
3.2. Focus Group Findings
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- CDC. Estimated HIV Incidence and Prevalence in the United States, 2015–2019. 2021. Available online: https://www.cdc.gov/hiv/pdf/library/reports/surveillance/cdc-hiv-surveillance-supplemental-report-vol-26-1.pdf (accessed on 29 January 2023).
- Shuter, J.; Hosgood, H.D.; Nardin, S.; Weinberger, A.H. Persons living with HIV who do not smoke cigarettes: A comparison of ex-smokers and never smokers. Tob. Use Insights 2021, 14, 1179173x211053349. [Google Scholar] [CrossRef] [PubMed]
- CDC. Burden of Cigarette Use in the U.S. 2022; August. Available online: https://www.cdc.gov/tobacco/campaign/tips/resources/data/cigarette-smoking-in-united-states.html#anchor_1551996389595 (accessed on 20 January 2023).
- Shuter, J.; Bernstein, S.L. Cigarette smoking is an independent predictor of nonadherence in HIV-infected individuals receiving highly active antiretroviral therapy. Nicotine Tob. Res. 2008, 10, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Tesoriero, J.M.; Gieryic, S.M.; Carrascal, A.; Lavigne, H.E. Smoking among HIV positive New Yorkers: Prevalence, frequency, and opportunities for cessation. AIDS Behav. 2010, 14, 824–835. [Google Scholar] [CrossRef] [PubMed]
- Gervais, A.; O’Loughlin, J.; Dugas, E.; Eisenberg, M.J.; Wellman, R.J.; DiFranza, J.R. A systematic review of randomized controlled trials of youth smoking cessation interventions. Database Abstr. Rev. Eff. (DARE) Qual. Assess. Rev. 2007, 6, ii1–ii2. [Google Scholar]
- Shuter, J.; Morales, D.A.; Considine-Dunn, S.E.; An, L.C.; Stanton, C.A. Feasibility and preliminary efficacy of a web-based smoking cessation intervention for HIV-infected smokers: A randomized controlled trial. J. Acquir. Immune Defic. Syndr. 2014, 67, 59–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, J.D.; Dochney, J.A.; Blazekovic, S.; Leone, F.; Metzger, D.; Frank, I.; Gross, R.; Hole, A.; Mounzer, K.; Siegel, S.; et al. The nature and consequences of cognitive deficits among tobacco smokers with HIV: A comparison to tobacco smokers without HIV. J. Neurovirol. 2017, 23, 550–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heminger, C.L.; Boal, A.L.; Zumer, M.; Abroms, L.C. Text2Quit: An analysis of participant engagement in the mobile smoking cessation program. Am. J. Drug Alcohol Abuse 2016, 42, 450–458. [Google Scholar] [CrossRef]
- Businelle, M.S. The potential of mHealth for tobacco dependence treatment: Domestic and international examples from NCI’s Smokefree.gov initiative. Nicotine Tob. Res. 2014, 16, 1033. [Google Scholar] [CrossRef]
- Whittaker, R.; McRobbie, H.; Bullen, C.; Rodgers, A.; Gu, Y.; Dobson, R. Mobile phone text messaging and app-based interventions for smoking cessation. Cochrane Database Syst. Rev. 2019, 10, Cd006611. [Google Scholar] [CrossRef]
- Shuter, J.; Kim, R.S.; An, L.C.; Abroms, L.C. Feasibility of a Smartphone-Based Tobacco Treatment for HIV-Infected Smokers. Nicotine Tob. Res. 2020, 22, 398–407. [Google Scholar] [CrossRef]
- Maguire, G.; Chen, H.; Schnall, R.; Xu, W.; Huang, M.-C. Smoking Cessation System for Preemptive Smoking Detection. IEEE Internet Things J. 2022, 9, 3204–3214. [Google Scholar] [CrossRef] [PubMed]
- Stanton, C.A.; Lloyd-Richardson, E.E.; Papandonatos, G.; de Dios, M.; Niaura, R. Mediators of the relationship between nicotine replacement therapy and smoking abstinence among people living with HIV/AIDS. AIDS Educ. Prev. 2009, 21 (Suppl. 3), 65–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.; Zhang, X.; Jiang, H.; Asaeikheybari, G.; Goel, N.; Hooper, M.W.; Huang, M.-C. Are you smoking? Automatic alert system helping people keep away from cigarettes. Smart Health 2018, 9–10, 158–169. [Google Scholar] [CrossRef]
- Hovell, M.F.; Bellettiere, J.; Liles, S.; Nguyen, B.; Berardi, V.; Johnson, C.; Matt, G.; Malone, J.; Boman-Davis, M.C.; E Quintana, P.J.; et al. Randomised controlled trial of real-time feedback and brief coaching to reduce indoor smoking. Tob. Control 2020, 29, 183–190. [Google Scholar] [CrossRef] [PubMed]
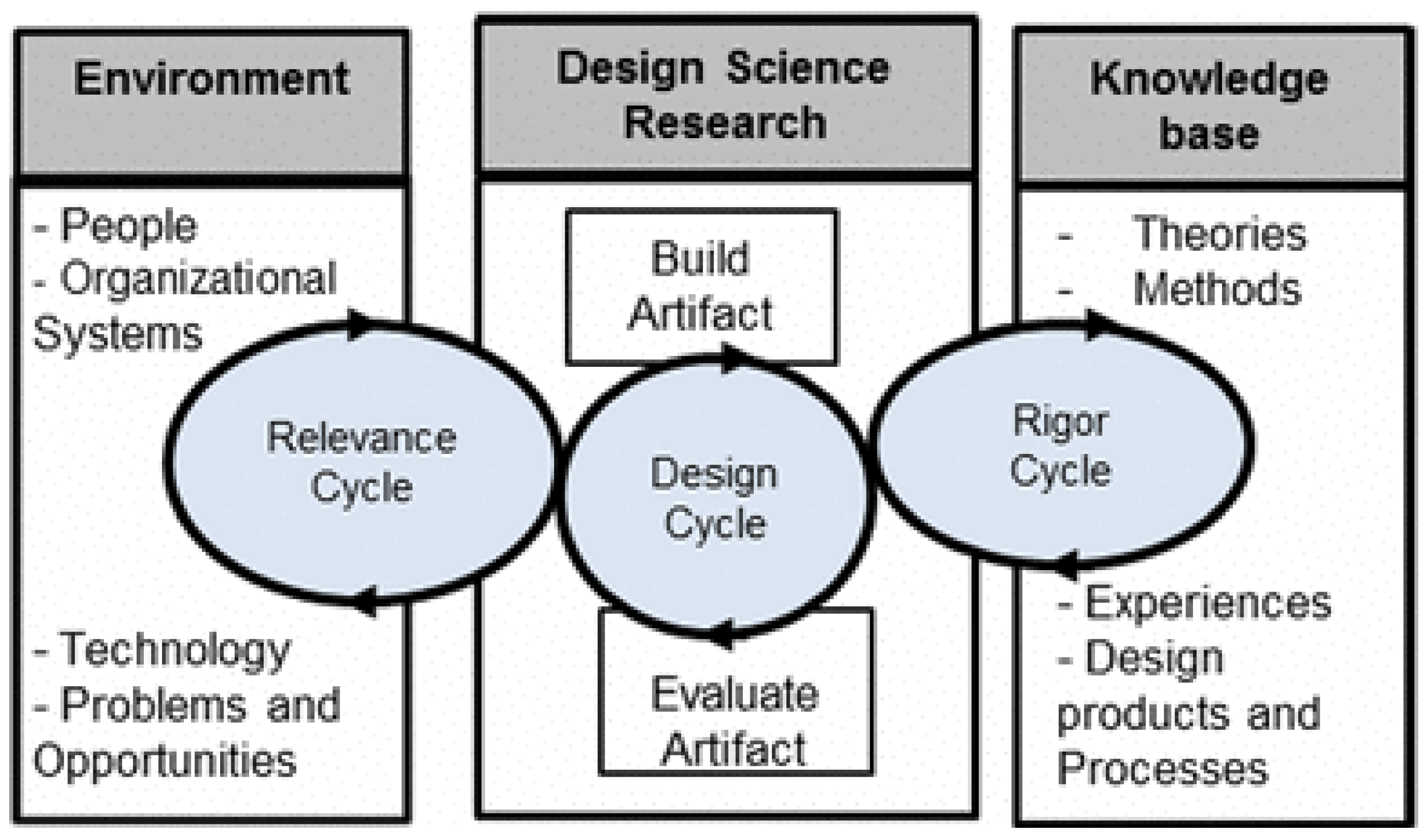
- Hevner, A.R. A three cycle view of design science research. Scand. J. Inf. Syst. 2007, 19, 4. [Google Scholar]
- Schnall, R.; Rojas, M.; Bakken, S.; Brown, W.; Carballo-Dieguez, A.; Carry, M.; Gelaude, D.; Mosley, J.P.; Travers, J. A user-centered model for designing consumer mobile health (mHealth) applications (apps). J. Biomed. Inform. 2016, 60, 243–251. [Google Scholar] [CrossRef]
- Brin, M.; Trujillo, P.; Huang, M.-C.; Cioe, P.; Chen, H.; Xu, W.; Schnall, R. Development and Evaluation of Visualizations of Smoking Data for Integration into the Sense2Quit App for Tobacco Cessation JAMIA. J. Am. Med. Inform. Assoc. Under Review.
- Jones, C.L.; Jensen, J.D.; Scherr, C.L.; Brown, N.R.; Christy, K.; Weaver, J. The Health Belief Model as an explanatory framework in communication research: Exploring parallel, serial, and moderated mediation. Health Commun. 2015, 30, 566–576. [Google Scholar] [CrossRef] [Green Version]
- Fogg, B. Persuasive technology: Using computers to change what we think and do. Ubiquity 2002, 2002, 5. [Google Scholar] [CrossRef] [Green Version]
- Schnall, R.; Bakken, S.; Rojas, M.; Travers, J.; Carballo-Dieguez, A. mHealth Technology as a Persuasive Tool for Treatment, Care and Management of Persons Living with HIV. AIDS Behav. 2015, 19 (Suppl. 2), 81–89. [Google Scholar] [CrossRef] [Green Version]
- Sheahan, S.L.; Garrity, T.F. Stress and Tobacco Addiction. J. Am. Acad. Nurse Pract. 1992, 4, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Bray, R.M.; Fairbank, J.A.; Marsden, M.E. Stress and Substance Use Among Military Women and Men. Am. J. Drug Alcohol Abus. 1999, 25, 239–256. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.J.; Das, S.; Young-Wolff, K.C. Smoking, Mental Illness, and Public Health. Annu. Rev. Public Health 2017, 38, 165–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnall, R.; Carcamo, J.; Porras, T.; Huang, M.-C.; Hooper, M.W. Use of the Phase-Based Model of Smoking Treatment to Guide Intervention Development for Persons Living with HIV Who Self-Identify as African American Tobacco Smokers. Int. J. Environ. Res. Public Health 2019, 16, 1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toll, B.A.; O’Malley, S.S.; Katulak, N.A.; Wu, R.; Dubin, J.A.; Latimer, A.; Meandzija, B.; George, T.P.; Jatlow, P.; Cooney, J.L.; et al. Comparing gain- and loss-framed messages for smoking cessation with sustained-release bupropion: A randomized controlled trial. Psychol. Addict. Behav. 2007, 21, 534–544. [Google Scholar] [CrossRef] [Green Version]
- Schnall, R.; Liu, J.; Alvarez, G.; Porras, T.; Ganzhorn, S.; Boerner, S.; Huang, M.-C.; Trujillo, P.; Cioe, P.P. A Smoking Cessation Mobile App for Persons Living with HIV: Preliminary Efficacy and Feasibility Study. JMIR Form Res. 2022, 6, e28626. [Google Scholar] [CrossRef]
- Hill, D.; Chapman, S.; Donovan, R. The return of scare tactics. Tob. Control 1998, 7, 5–8. [Google Scholar] [CrossRef]
- CDC. Basic Statistics|HIV Basics|HIV/AIDS|CDC. 2022. Available online: https://www.cdc.gov/hiv/basics/statistics.html (accessed on 17 January 2023).


{kind=link}
| Relevance Focus Groups |
|
| Design Session 1.0: Optimal Features |
| Starter: If you had an app to help you quit smoking, what messages would stop you from smoking a cigarette? (Referring to slides/handout) [see Supplementary File S1] Imagine each of the broad categories as separate screens on a mobile app.
|
| Design Session 2.0: Interface |
| Starter: If you have used an app to improve or monitor your health, what did it look like? If you have not used such an app, what would you expect it to look like? (Referring to slides/handout) [see Supplementary File S1] Imagine each of the broad categories as separate screens on a mobile app.
|
| Code | Excerpts | |
|---|---|---|
| Perceived Barriers | Perceived Benefits | |
| History of smoking (n = 19) | “My barrier is that I have…it’s like the routine that you get when you start smoking…when you’ve been smoking for a long time.”—FG2 Participant “I quit smoking for two years because I had a heart attack, which was from the cigarettes. Last year I started picking it up again.”—FG1 Participant “I started smoking three years ago because I was a part of the in-crowd. Everybody else was doing it, so let me go ahead and try it.”—FG2 Participant “Yes, the urges get so bad and like I really want to stop so bad, but I’ve been doing it for so long now, you know so it’s really hard. I’ve been smoking over twenty years, but you know I just.”—FG4 Participant | “I caught a bad asthma attack and I had to go to the hospital, because I was smoking cigarettes back-to-back. So, I had to go to the hospital, and I was like, you know what? Something’s got to give. Girl, you’ve got to get it together. Like, for real, for real. Do you want to stay alive, or you want to be somewhere else?”—FG3 Participant “What I went through then was horrible. Even my family was scared I was going to die. If you put the HIV with the smoking and you see how I was then, I was like, nah.”—FG2 Participant |
| Triggers (n = 96) | “For me, I get up in the morning, have coffee, I have to have a cigarette. After I eat, I have to have a cigarette. Certain things like that. It’s not just the nicotine, it’s to have something in your mouth; in between your fingers. That’s one of the barriers that I have.”—FG2 Participant “Well, I love to eat, and so you know. But after I eat, I want a cigarette.”—FG4 Participant “For me, I get up in the morning, have coffee, I have to have a cigarette. After I eat, I have to have a cigarette. Certain things like that.”—FG2 Participant “My barriers, number one, starts with my drinking…the alcohol. That’s where it all starts.”—FG2 Participant “Now, for me when I was doing drugs, I had to have cigarettes. When I drink, yeah, I had to have cigarettes, you know.”—FG3 Participant | No quotes |
| Consequences of Quitting (n = 15) | “There’s the good and the bad. For some people you don’t want to smoke cigarettes, eat a piece of candy or something. But then, you get diabetes.”—FG1 Participant “I am just worried about massive weight gain and stuff. That’s what I worry about.”—FG1 Participant “I started smoking, marijuana, because not smoking those cigarettes now. So now I’m smoking marijuana, but I’m smoking more marijuana…”—FG3 Participant | No quotes |
| Motivation to Quit (n = 69) | No quotes | “Ok, I know I smoked, how many pack of cigarettes day, right? You put that $10.00 up in the bank. And you have that other $10.00. And you look at yourself, you’d be like, wow, I saved all of this.”—FG3 Participant “Financially, it’s hurting me, but I am still spending that kind of money. That’s what I am saying. All that money I could be saving towards something else.”—FG2 Participant “I don’t smoke the whole day, but I will have a spray or something, because I don’t like to smell the smoke on me.”—FG3 Participant |
| Messages to Help Quit (n = 181) | “I turn around with the commercials because I hate the commercials. Every time I see a commercial that’s when I smoke because they piss me off…really, really piss me off…those commercials.”—FG2 Participant “The commercials just punish you. They don’t reward you. A lot of people are more receptive from rewards than punishment.”—FG2 Participant “They done had one person with their fingers falling off, I was still smoking.”—FG3 Participant | “For me, I saw cancer. I see those commercials on TV with the guy with the thing is his throat. That’s really scary.”—FG2 Participant “By see past people laying in the hospital bed with cancer or something like that. That would scare me.”—FG2 Participant “And it could just say to you, congratulations, Mr. Such and Such, you completed. You know and then the party confetti. And then a little turtle gets up and do his little dance.”—FG #4 “Or maybe something like that comes on and says, you know find something else to do. You know do some exercising.”—FG3 Participant |
| Quitting Strategies (n = 39) | No quotes | “You have to have somebody to check you, for real. That’s the only way. They keep bugging you until you stop.”—FG1 Participant “Tell me, ok, if you do this, I’m going to work with you on this. Or I’m going to help you with this. Or, matter of fact, I will go with you to the meeting; how about that?”—FG3 Participant “I’ll smoke a half a cigarette and then leave the rest and smoke the other half later, which helps me to cut down a lot.”—FG1 Participant |
| Mental Health (n = 31) | “You wake up and try to have a positive outlook, and then something just brings your day down…I need a cigarette.”—FG1 Participant “Mental health issues…if you’re going through like anxiety, depression. Probably loneliness. You need something to cope. So, I would say that is one, too.”—FG3 Participant “Yeah, stress is the number one thing, that you start smoking. Because if you can’t get nobody on the phone, like stressed out, and you normally…go to, but like my mom (inaudible) person. I said you know, since she’s gone now, right? I go to a cigarette.”—FG5 Participant | No quotes |
| Code | Excerpts | |
|---|---|---|
| Perceived Barriers | Perceived Benefits | |
| Social actor (n = 55) | “I don’t think we should share information.”—DS2 Participant “I might be jumping the gun, but you need a moderator because people like to go there when they got nothing to do with the group…”—DS2 Participant “Because you’ve always got a couple of knuckleheads that’s going to want to, you know. Because a lot of these groups, I’ve noticed that—especially Facebook groups, the person that—they have a moderator. Everyone just can’t get on and say anything they want. So, a moderator would be helpful.”—DS2 Participant | “Like he said, someone in the same…identifying with you. That’s what I was saying; somebody giving you real information and based on their experience or something. That would be great.”—DS1 Participant “You know, to look at. Somebody that’s maybe a success story. Hi. I’ve been smoke-free for something like that. Just a greeting. And you can meet some of my peers that have also been clean for a few minutes. And we can share some, you know, information and get you started.”—DS2 Participant “The apps need to have a place where you could maybe look for sponsors, if they been thinking about sponsors.”—DS2 Participant “If I am in a chat room, I would like to see you or at least see a picture of you to know who I am talking to…or a video would be ultimate.”—DS1 Participant “I’d rather live, you know, because that shows a lot of your expressions and, you know, when you’re saying something to me.”—DS2 Participant |
| Tool: Imagery (n = 68) | “That negative stuff…I don’t want to see that lady with that hole talking. That was terrible.”—DS1 Participant | “Yeah. I think colors are important. Certain colors kind of put my mood in different ways. Like she was saying, it’s the sky and sky blue. You know, I like those type of colors. They seem to make people’s attitudes a little milder than some other colors.”—DS2 Participant “I would say something maybe like sky color. Like when I’m doing something outdoors.”—DS2 Participant “They want to quit smoking. So, they want something bright and cheery.”—DS2 Participant “I would say my kids because I don’t smoke around them.”—DS1 Participant “Positive message sent…something like that. Like, they’d send something positive to me…positive message…you can do it; send you pictures of someone how has stopped smoking.”—DS1 Participant “Showing the benefits to my health. That would help. Showing positive pitches.”—DS1 Participant “Healthy person with a big heart beating blood.”—DS2 Participant “What’s you’re saving on and the bank is getting bigger and bigger. You actually see the money grow.”—DS1 Participant “I like the piggy bank. Yeah. You saved all that.”—DS2 Participant |
| Tool: Customization (n = 28) | No quotes | “I am leaning a little more towards my own message because I only know what excites me. Nobody knows what really gets me going deep down for me…all of us. A lot of things that affect us we don’t bring up for a myriad of reasons…embarrassment; forgetfulness. If I can customize it and I know I am going to be the only one that sees this.”—DS1 Participant “Yeah. So, you would be able to personalize the notifications. Like for me, it would be a picture of my niece, my girlfriend, if I had one.”—DS2 Participant “Personalization, yeah. Customizing it to your, you know, your age group and your culture and your area…”—DS2 Participant “I put down here show what I can buy when I stop. If you stop for ten years, you can buy a car. If you stop for five years, you can buy a dress…if you stop a month, you can buy this new dress. Actually, show the price of the cigarette against the price of the dress…wow, if I stop for that amount of time, I can get those shoes. Peaked me a little bit.”—DS1 Participant |
| Medium (n = 81) | “(In other apps) I get notifications I don’t want”—DS1 Participant “I really don’t have much to say on that, only because all of these notifications are annoying the hell out of me now.”—DS2 Participant | “I think that’s (group chat) a good idea for an app, you know, that you can actually bring someone else in.”—DS2 Participant “And it gives me a goal…I saved $20 this week; maybe I could do $30 next week. Just something to keep you…that would interest me a little, probably…something to do. Maybe I could save a couple more dollars this week.”—DS1 Participant “Like the educational game. You answer the questions correctly, you get to go to next level. It’s pretty cool. I would do that. If you answer the questions correctly, you go on to the next level. If you keep asking the questions correctly, you’ll get to the end eventually and win.”—DS1 Participant “Games in general that you could pick—because I know some people, just having a game would be enough, any game. Some people, just to take they mind off it. I’m kind of like that.”—DS2 Participant “I like what you said about a bell that notifies you. Maybe they have meetings…let you know when there is a meeting. Notification letting you know there is a meeting, like a smoke cessation meeting.”—DS1 Participant “Yeah. I’d like the notifications to come through because you know, I don’t go to—I’m not like that—I’m not going through my phone to see the dating site, get my emails, my (inaudible). That is why I do like to hear the ping.”—DS2 Participant |
| “As I’ve been saying before, I think education is important. The more we know about HIV, the more we know about smoking, and I think that would be helpful. I am stealing your idea. I’ve got medical facts, but you write education…more than medical facts, it’s education about a lot of things.”—DS1 Participant “I’ve got to say, I’m going there looking for something to help me stop smoking, so, just the benefits and I can click on that and see what the benefits are.”—DS2 Participant “I would like an app that would help point you to information; people to talk to; that would have a list of people you can call and who would be helpful and talking you down from a cigarette, maybe.”—DS1 Participant | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schnall, R.; Trujillo, P.; Alvarez, G.; Michaels, C.L.; Brin, M.; Huang, M.-C.; Chen, H.; Xu, W.; Cioe, P.A. Theoretically Guided Iterative Design of the Sense2Quit App for Tobacco Cessation in Persons Living with HIV. Int. J. Environ. Res. Public Health 2023, 20, 4219. https://doi.org/10.3390/ijerph20054219
Schnall R, Trujillo P, Alvarez G, Michaels CL, Brin M, Huang M-C, Chen H, Xu W, Cioe PA. Theoretically Guided Iterative Design of the Sense2Quit App for Tobacco Cessation in Persons Living with HIV. International Journal of Environmental Research and Public Health. 2023; 20(5):4219. https://doi.org/10.3390/ijerph20054219
Chicago/Turabian StyleSchnall, Rebecca, Paul Trujillo, Gabriella Alvarez, Claudia L. Michaels, Maeve Brin, Ming-Chun Huang, Huan Chen, Wenyao Xu, and Patricia A. Cioe. 2023. "Theoretically Guided Iterative Design of the Sense2Quit App for Tobacco Cessation in Persons Living with HIV" International Journal of Environmental Research and Public Health 20, no. 5: 4219. https://doi.org/10.3390/ijerph20054219