
Impact of Social Isolation Due to COVID-19 on Daily Life Activities and Independence of People over 65: A Cross-Sectional Study
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Outcome Variables
2.4. Intervention
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Envejecimiento y Atención a la Dependencia en Argentina|Publications. Available online: https://publications.iadb.org/publications/spanish/document/Envejecimiento-yaten-cion-a-la-dependencia-en-Argentina.pdf (accessed on 3 July 2022).
- Álvarez, A.Á.; Piédrola, R.M.; Mora, R.M.; Máximo, N.; Bocanegra, B.M.M.; Valverde, M.Á.T.; Rivas, N. Dominio y Proceso. Available online: http://www.terapia-ocupacional.com/aota2010esp.pdf (accessed on 23 June 2022).
- World Health Organization. Clasificación Internacional del Funcionamiento de la Discapacidad y de la Salud: CIF; Organización Mundial de la Salud: Geneva, Switzerland, 2001. [Google Scholar]
- Loredo-Figueroa, M.T.; Gallegos-Torres, R.M.; Xeque-Morales, A.S.; Palomé-Vega, G.; Juárez-Lira, A. Nivel de dependencia, autocuidado y calidad de vida del adulto mayor. Enfermería Univ. 2016, 13, 159–165. [Google Scholar] [CrossRef]
- Aguilar, K. Valoración de autoestima y del desempeño en las actividades básicas e instrumentarías de la vida diaria en los adultos mayores que acuden a consulta externa de Geriatría del Hospital de Agudos Carlos G. Durand. Rev. Argent. Gerontol. Geriatría 2017, 32, 89–97. [Google Scholar]
- Lau, H.; Khosrawipour, V.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salud Confirma el Primer Caso de Coronavirus en el País. Argentina.gob.ar. 2020. Available online: https://www.argentina.gob.ar/noticias/salud-confirma-el-primer-caso-de-coronavirus-en-el-pais (accessed on 3 July 2022).
- COVID-19 Strategy Update—14 April 2020. Available online: https://www.who.int/publications-detail-redirect/covid-19-strategy-update---14-april-2020 (accessed on 3 July 2022).
- Organización Panamericana de la Salud. Orientaciones Para la Aplicación de Medidas de Salud Pública no Farmacológicas en Grupos de Población en Situación de Vulnerabilidad en el Contexto de la COVID-19. 2020. Available online: https://iris.paho.org/handle/10665.2/52955 (accessed on 23 June 2022).
- Ozemek, C.; Lavie, C.J.; Rognmo, Ø. Global physical activity levels—Need for intervention. Prog. Cardiovasc. Dis. 2019, 62, 102–107. [Google Scholar] [CrossRef]
- Chou, C.-H.; Hwang, C.-L.; Wu, Y.-T. Effect of Exercise on Physical Function, Daily Living Activities, and Quality of Life in the Frail Older Adults: A Meta-Analysis. Arch. Phys. Med. Rehabil. 2012, 93, 237–244. [Google Scholar] [CrossRef]
- Singhal, T. A review of coronavirus disease-2019 (COVID-19). Indian J. Pediatr. 2020, 87, 281–286. [Google Scholar] [CrossRef] [Green Version]
- Davies, N.; Frost, R.; Bussey, J.; Hartmann-Boyce, J.; Park, S. Maximising Mobility in Older People When Isolated with COVID-19; Centre for Evidence-Based Medicine: Oxford, UK, 2020. [Google Scholar]
- Morgan, K. Daytime activity and risk factors for late-life insomnia. J. Sleep Res. 2003, 12, 231–238. [Google Scholar] [CrossRef]
- Reyes, P.M.; Gutiérrez, C.M.; Mena, R.P.; Torres, S.J. Efectos del ejercicio físico sobre la calidad del sueño, insomnio y somnolencia diurna en personas mayores. Revisión de la literatura. Rev. Española De Geriatría Y Gerontol. 2020, 55, 42–49. [Google Scholar] [CrossRef]
- Ali, I.; Alharbi, O.M. COVID-19: Disease, management, treatment, and social impact. Sci. Total Environ. 2020, 728, 138861. [Google Scholar] [CrossRef]
- L’Angiocola, P.D.; Monti, M. COVID-19: The critical balance between appropriate governmental restrictions and expected economic, psychological and social consequences in Italy. Are we going in the right direction? Acta Bio Med. Atenei Parm. 2020, 91, 35–38. [Google Scholar] [CrossRef]
- Tran, L.D.; Rice, T.H.; Ong, P.M.; Banerjee, S.; Liou, J.; Ponce, N.A. Impact of gentrification on adult mental health. Health Serv. Res. 2020, 55, 432–444. [Google Scholar] [CrossRef] [Green Version]
- Asociación Médica Mundial. Declaración de Helsinki. 2013. Available online: http://www.anmat.gov.ar/comunicados/HELSINSKI2013.pdf (accessed on 23 June 2022).
- Ley No 25.236. Protección de Los Datos Personales. Ministerio de Justicia y Derechos Humanos. 2000. Available online: http://servicios.infoleg.gob.ar/infolegInternet/anexos/60000-64999/64790/norma.htm (accessed on 23 June 2022).
- Barthel, L. Functional evaluation: The Barthel index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontol. 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Sample Size Calculator by Raosoft, Inc. Available online: http://www.raosoft.com/samplesize.html (accessed on 3 July 2022).
- Fernández-Ballesteros, R.; Sánchez-Izquierdo Alonso, M. Impacto del COVID-19 en personas mayores en España: Algunos resultados y reflexiones. Clínica Y Salud 2020, 31, 165–169. [Google Scholar] [CrossRef]
- Navarro González, E.; Calero García, M.D.; López Pérez-Díaz, Á.; Luna Gómez Ceballos, A.; Torres Carbonell, I.; Calero García, M.J. Nivel de independencia en la vida diaria y plasticidad cognitiva en la vejez. Escr. Psicol. 2008, 2, 74–84. [Google Scholar] [CrossRef]
- Carnero-Pardo, C. Education, dementia and cerebral reserve. Rev. Neurol. 2000, 31, 584–592. [Google Scholar]
- Newsom, J.T.; Schulz, R. Social support as a mediator in the relation between functional status and quality of life in older adults. Psychol. Aging 1996, 11, 34–44. [Google Scholar] [CrossRef]
- Andel, R.; Vigen, C.; Mack, W.J.; Clark, L.J.; Gatz, M. The effect of education and occupational complexity on rate of cognitive decline in Alzheimer’s patients. J. Int. Neuropsychol. Soc. 2006, 12, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Menec, V.H. The Relation Between Everyday Activities and Successful Aging: A 6-Year Longitudinal Study. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2003, 58, S74–S82. [Google Scholar] [CrossRef] [Green Version]
- Van Hooren, S.A.; Valentijn, S.A.; Bosma, H.; Ponds, R.W.; Van Boxtel, M.P.; Jolles, J. Relation between health status and cognitive functioning: A 6-year follow-up of the Maastricht Aging Study. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2005, 60, P57–P60. [Google Scholar] [CrossRef] [Green Version]
- Glei, D.A.; Landau, D.A.; Goldman, N.; Chuang, Y.-L.; Rodríguez, G.; Weinstein, M. Participating in social activities helps preserve cognitive function: An analysis of a longitudinal, population-based study of the elderly. Int. J. Epidemiol. 2005, 34, 864–871. [Google Scholar] [CrossRef]
- Zunzunegui, M.-V.; Alvarado, B.E.; Del Ser, T.; Otero, A. Social Networks, Social Integration, and Social Engagement Determine Cognitive Decline in Community-Dwelling Spanish Older Adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2003, 58, S93–S100. [Google Scholar] [CrossRef] [Green Version]
- Silva, C.A.M.; Orellana, P.A.R.; Nassr, G.N.M. Valoración del estado funcional de adultos mayores con dependencia moderada y severa pertenecientes a un centro de salud familiar. Fisioter. E Pesqui. 2015, 22, 76–83. [Google Scholar]
- da Silva, H.S.; de Oliveira Duarte, Y.A.; de Andrade, F.B.; Cerqueira, A.T.D.A.R.; Santos, J.L.F.; Lebrão, M.L. Correlates of above-average cognitive performance among older adults: The SABE study Fatores de desempenho cognitivo acima da média em idosos: Estudo SABE. Cad Saúde Pública 2014, 30, 1977–1986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Zhang, Y.; Du, S.; Wang, Q.; Xia, H.; Sun, R. Exercise interventions for improving physical function, daily living activi-ties and quality of life in community-dwelling frail older adults: A systematic review and meta-analysis of randomized controlled trials. Geriatr. Nurs. 2020, 41, 261–273. [Google Scholar] [CrossRef]
- Spampinato, G. Las Caídas en Las Personas Mayores y Cómo Prevenirlas. Secretaría Nacional de Niñez, Adolescencia y Familia. Ministerio de Desarrollo Social. Available online: https://www.argentina.gob.ar/sites/default/!les/caidas_en_personas_mayores.pdf (accessed on 23 June 2022).
- Instituto Nacional de Estadística y Censos. Encuesta Nacional Sobre Calidad de Vida de Adultos Mayores 2012, 1st ed.; Instituto Nacional de Estadística y Censos—INDEC: Buenos Aires, Argentina, 2014; E-Book.
- Capozzo, R.; Zoccolella, S.; Frisullo, M.; Barone, R.; Dell’Abate, M.; Barulli, M.; Musio, M.; Accogli, M.; Logroscino, G. Telemedicine for Delivery of Care in Frontotemporal Lobar Degeneration During COVID-19 Pandemic: Results from Southern Italy. J. Alzheimer’s Dis. 2020, 76, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Emerson, K. Coping with being cooped up: Social distancing during COVID-19 among 60+ in the United States. Rev. Panam. Salud. Publica 2020, 44, e81. [Google Scholar] [CrossRef]
- Wong, S.Y.S.; Zhang, D.; Sit, R.W.S.; Yip, B.H.K.; Chung, R.Y.-N.; Wong, C.K.M.; Chan, D.C.C.; Sun, W.; Kwok, K.O.; Mercer, S.W. Impact of COVID-19 on loneliness, mental health, and health service utilisation: A prospective cohort study of older adults with multimorbidity in primary care. Br. J. Gen. Pract. 2020, 70, e817–e824. [Google Scholar] [CrossRef] [PubMed]
- Antunes, R.; Frontini, R.; Amaro, N.; Salvador, R.; Matos, R.; Morouço, P.; Rebelo-Gonçalves, R. Exploring Lifestyle Habits, Physical Activity, Anxiety and Basic Psychological Needs in a Sample of Portuguese Adults during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 4360. [Google Scholar] [CrossRef]
- Hartley, S.; Colas des Francs, C.; Aussert, F.; Martinot, C.; Dagneaux, S.; Londe, V.; Waldron, L.; Royant-Parola, S. The effects of quarantine for SARS-CoV-2 on sleep: An online survey. Encephale 2020, 46, S53–S59. [Google Scholar] [CrossRef]
- Barros, M.B.A.; Lima, M.G.; Malta, D.C.; Szwarcwald, C.L.; Azevedo, R.C.S.; Romero, D.; de Souza Júnior, P.R.B.; Azevedo, L.O.; Machado, Í.E.; Damacena, G.N.; et al. Report on sadness/depression, nervous-ness/anxiety and sleep problems in the Brazilian adult population during the COVID-19 pandemic. Epidemiol. Serv. Saude 2020, 29, e2020427. [Google Scholar] [CrossRef] [PubMed]
- Górnicka, M.; Drywień, M.E.; Zielinska, M.A.; Hamułka, J. Dietary and Lifestyle Changes During COVID-19 and the Subsequent Lockdowns among Polish Adults: A Cross-Sectional Online Survey PLifeCOVID-19 Study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef] [PubMed]
- Kwegyir Tsiboe, A. Describing the experiences of older persons with visual impairments during COVID-19 in rural Ghana. J. Adult Prot. 2020, 22, 371–383. [Google Scholar] [CrossRef]
- Heid, A.R.; Cartwright, F.; Wilson-Genderson, M.; Pruchno, R. Challenges Experienced by Older People During the Initial Months of the COVID-19 Pandemic. Gerontologist 2020, 61, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Eghtesadi, M. Breaking Social Isolation Amidst COVID-19: A Viewpoint on Improving Access to Technology in Long-Term Care Facilities. J. Am. Geriatr. Soc. 2020, 68, 949–950. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Barthel | p-Value | Lawton/Brody | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| AF | % | Means | SD | Means | SD | ||||
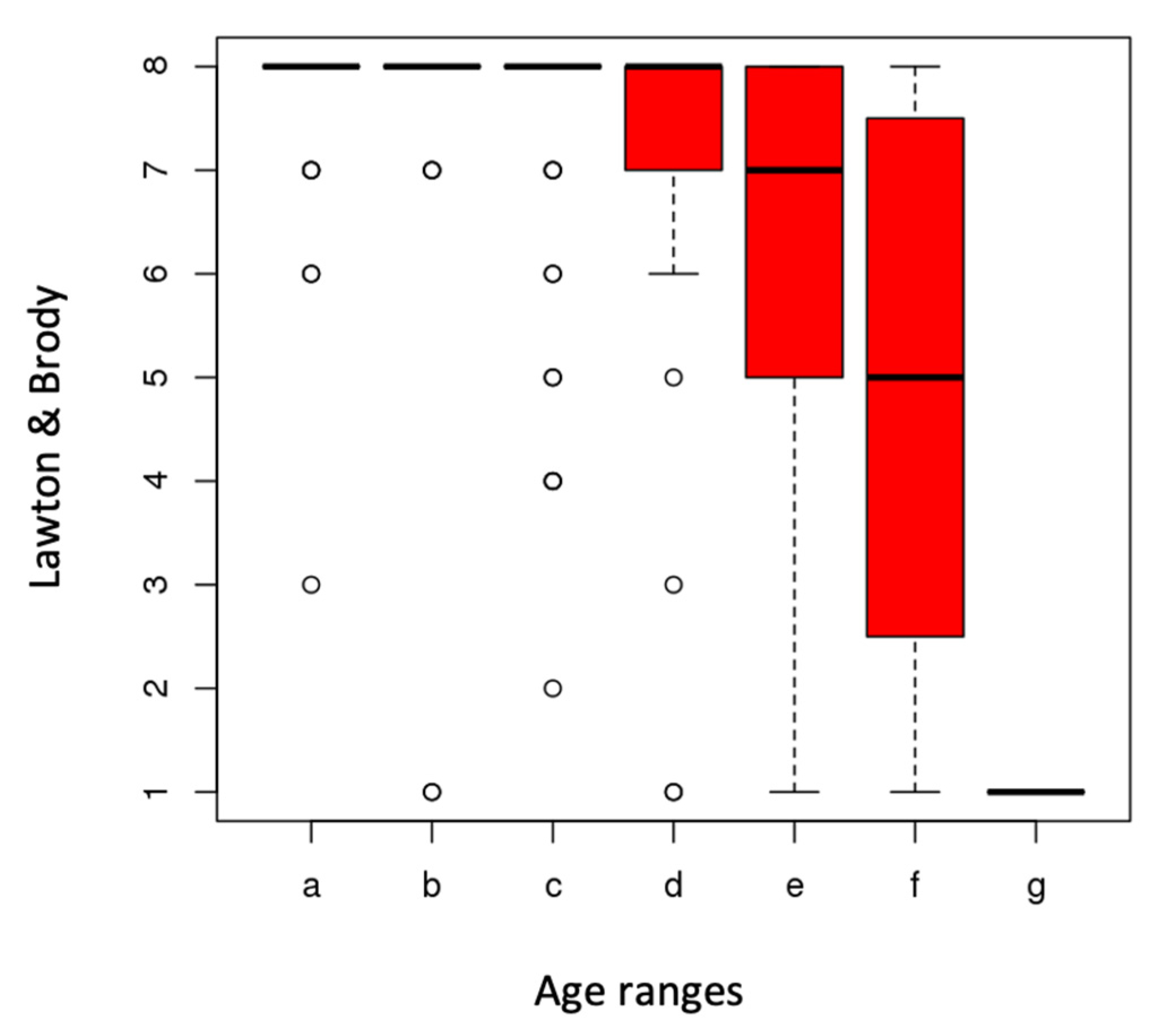
| Age (range) | 0.01 | 0.001 | |||||||
| 65–69 (a) | 38 | 20 | 98.42 | 4.81 | 7.68 | 0.93 | |||
| 70–74 (b) | 40 | 21 | 95.63 | 15.53 | 7.58 | 1.55 | |||
| 75–89 (c) | 52 | 27 | 95.96 | 11.25 | 7.4 | 1.36 | |||
| 80–84 (d) | 40 | 21 | 95.38 | 9.96 | 7.15 | 1.78 | |||
| 85–89 (e) | 15 | 8 | 88.33 | 19.88 | 6.07 | 2.76 | |||
| 90–94 (f) | 7 | 4 | 91.43 | 11.8 | 4.86 | 3.02 | |||
| 95–99 (g) | 1 | 1 | 60 | N/A | 1 | N/A | |||
| Sex | 0.81 | 0.31 | |||||||
| Female | 121 | 63 | 95.83 | 10.27 | 7.21 | 1.79 | |||
| Male | 72 | 37 | 94.44 | 15.33 | 7.22 | 1.81 | |||
| Education | 0.21 | 0.23 | |||||||
| Incomplete primary | 1 | 1 | 95 | N/A | 7 | N/A | |||
| Complete primary | 9 | 5 | 85.56 | 23.38 | 5.89 | 3.06 | |||
| Incomplete secondary | 9 | 5 | 94.44 | 11.3 | 7 | 2.35 | |||
| Complete secondary | 77 | 40 | 95.84 | 11.4 | 7.04 | 1.94 | |||
| Incomplete tertiary | 2 | 1 | 100 | 0 | 8 | 0 | |||
| Complete tertiary | 34 | 18 | 96.91 | 5.51 | 7.62 | 0.89 | |||
| Incomplete university | 13 | 7 | 85.77 | 26.91 | 6.62 | 2.6 | |||
| Complete university | 48 | 25 | 97.71 | 6.52 | 7.63 | 1.2 | |||
| Previous | 0.35 | 0.03 | |||||||
| occupation | Administrative | 32 | 17 | 95.16 | 14.56 | 7.34 | 1.47 | ||
| Housewife | 30 | 15 | 90.5 | 17.49 | 6.1 | 2.8 | |||
| Trade | 39 | 20 | 95.9 | 7.94 | 7.49 | 1.43 | |||
| Teacher | 31 | 16 | 97.58 | 4.81 | 7.52 | 1.15 | |||
| Professional | 44 | 23 | 97.73 | 6.69 | 7.61 | 1.24 | |||
| Religious | 1 | 1 | 100 | N/A | 8 | N/A | |||
| Technician | 16 | 8 | 91.88 | 22.57 | 6.63 | 2.36 | |||
| Number of people | |||||||||
| at home | 0.17 | <<0.001 | |||||||
| 1 | 46 | 24 | 97.61 | 4.56 | 7.72 | 0.72 | |||
| 2 | 117 | 61 | 97.09 | 6.7 | 7.45 | 1.42 | |||
| 3 | 20 | 10 | 84.5 | 26.3 | 5.3 | 3.13 | |||
| 4 | 8 | 4 | 81.88 | 28.53 | 5.63 | 2.92 | |||
| 5 | 1 | 1 | 100 | N/A | 6 | N/A | |||
| 8 | 1 | 1 | 100 | N/A | 8 | N/A | |||
| Difficulty | AF | % |
|---|---|---|
| Shopping | 43 | 22 |
| Food preparation | 28 | 15 |
| Laundry | 24 | 12 |
| Housekeeping | 20 | 10 |
| Mode of transportation | 15 | 8 |
| Responsibility for own medications | 12 | 6 |
| Ability to handle finances | 11 | 6 |
| Ability to use telephone | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frutos, M.L.; Cruzado, D.P.; Lunsford, D.; Orza, S.G.; Cantero-Téllez, R. Impact of Social Isolation Due to COVID-19 on Daily Life Activities and Independence of People over 65: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 4177. https://doi.org/10.3390/ijerph20054177
Frutos ML, Cruzado DP, Lunsford D, Orza SG, Cantero-Téllez R. Impact of Social Isolation Due to COVID-19 on Daily Life Activities and Independence of People over 65: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2023; 20(5):4177. https://doi.org/10.3390/ijerph20054177
Chicago/Turabian StyleFrutos, María Laura, David Pérez Cruzado, Dianna Lunsford, Santiago García Orza, and Raquel Cantero-Téllez. 2023. "Impact of Social Isolation Due to COVID-19 on Daily Life Activities and Independence of People over 65: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 20, no. 5: 4177. https://doi.org/10.3390/ijerph20054177