
PTSD and Partial PTSD among First Responders One and Five Years after the Paris Terror Attacks in November 2015
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Recruitment
2.2. Data Collection
2.2.1. Dependent Variable
- Criterion A: Having had a stressful experience. Matching our inclusion criterion, this refers to the November 2015 terrorist attacks during which survey participants responded.
- Criterion B: Intrusion symptoms
- Criterion C: The symptoms of avoidance
- Criterion D: Symptoms of altered cognitions and moods
- Criterion E: Symptoms of altered wakefulness and responsiveness
- Criterion F: Symptoms described by the previous criteria (B to E) that have lasted for more than one month.
2.2.2. Independent Variables
2.3. Statistical Analyses
- Moderate chronicity: partial PTSD in both wave 1 and 2.
- Severe chronicity: PTSD in both wave 1 and 2.
- Delayed onset PTSD: no PTSD in wave 1 and PTSD in wave 2.
- Delayed onset partial PTSD: no PTSD in wave 1 and partial PTSD in wave 2.
- Partial recovery: PTSD in wave 1 and partial PTSD in wave 2.
- Complete recovery: PTSD in wave 1 and no PTSD in wave 2.
- Remission: partial PTSD in wave 1 and no PTSD in wave 2.
- Worsening: partial PTSD in wave 1 and PTSD in wave 2.
- Resistant: no PTSD in wave 1 and in wave 2.
3. Results
3.1. Participation Rate and Inclusion
3.2. Factors Associated to Attrition
3.3. Prevalence of PTSD and Partial PTSD Five Years after the Attacks
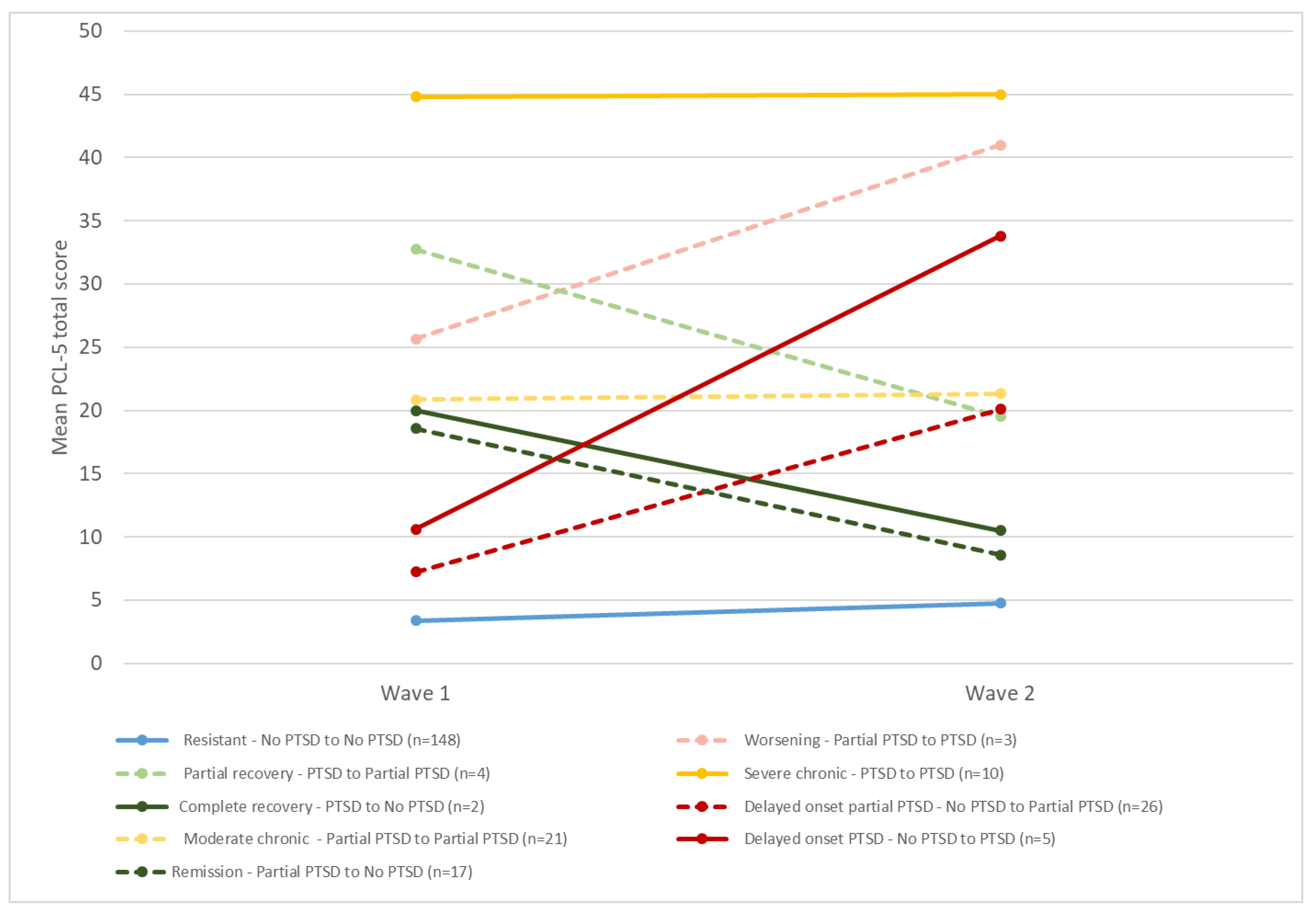
3.4. Evolution of PTSD between the 2 Waves
- at wave 1, 75.2% of participants did not have PTSD, 17.8% had partial PTSD and 7.0% had PTSD;
- at wave 2, 70.2% of participants had no PTSD, 22.1% had partial PTSD and 7.7% had PTSD.
3.5. Factors Associated with PTSD and Partial PTSD Five Years after the Attacks
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Philippe, J.-M.; Brahic, O.; Carli, P.; Tourtier, J.-P.; Riou, B.; Vallet, B. French Ministry of Health’s Response to Paris Attacks of 13 November 2015. Crit. Care Lond. Engl. 2016, 20, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motreff, Y.; Baubet, T.; Pirard, P.; Rabet, G.; Petitclerc, M.; Stene, L.E.; Vuillermoz, C.; Chauvin, P.; Vandentorren, S. Factors Associated with PTSD and Partial PTSD among First Responders Following the Paris Terror Attacks in November 2015. J. Psychiatr. Res. 2020, 121, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, G.A.; Brewin, C.R.; Kaniasty, K.; Greca, A.M.L. Weighing the Costs of Disaster: Consequences, Risks, and Resilience in Individuals, Families, and Communities. Psychol. Sci. Public Interest 2010, 11, 1–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonde, J.P.E.; Jensen, J.H.; Smid, G.E.; Flachs, E.M.; Elklit, A.; Mors, O.; Videbech, P. Time Course of Symptoms in Posttraumatic Stress Disorder with Delayed Expression: A Systematic Review. Acta Psychiatr. Scand. 2022, 145, 116–131. [Google Scholar] [CrossRef]
- Hobfoll, S.E.; Palmieri, P.A.; Johnson, R.J.; Canetti-Nisim, D.; Hall, B.J.; Galea, S. Trajectories of Resilience, Resistance, and Distress During Ongoing Terrorism: The Case of Jews and Arabs in Israel. J. Consult. Clin. Psychol. 2009, 77, 138. [Google Scholar] [CrossRef]
- Wesemann, U.; Bühler, A.; Mahnke, M.; Polk, S.; Willmund, G. Longitudinal Mental Health Effects of the 2016 Terrorist Attack in Berlin on Various Occupational Groups of Emergency Service Personnel. Health Secur. 2020, 18, 403–408. [Google Scholar] [CrossRef]
- Kessler, R.C. Posttraumatic Stress Disorder: The Burden to the Individual and to Society. J. Clin. Psychiatry 2000, 61 (Suppl. 5), 14866. [Google Scholar]
- van der Velden, P.G.; Wong, A.; Boshuizen, H.C.; Grievink, L. Persistent Mental Health Disturbances during the 10 Years after a Disaster: Four-Wave Longitudinal Comparative Study. Psychiatry Clin. Neurosci. 2013, 67, 110–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, W.; Figueira, I.; Maurat, A.M.; Bucassio, E.P.; Vieira, I.; Jardim, S.R.; Coutinho, E.S.F.; Mari, J.J.; Mendlowicz, M.V. Partial and Full PTSD in Brazilian Ambulance Workers: Prevalence and Impact on Health and on Quality of Life. J. Trauma. Stress 2007, 20, 637–642. [Google Scholar] [CrossRef]
- Skogstad, L.; Heir, T.; Hauff, E.; Ekeberg, Ø. Post-Traumatic Stress among Rescue Workers after Terror Attacks in Norway. Occup. Med. Oxf. Engl. 2016, 66, 528–535. [Google Scholar] [CrossRef] [Green Version]
- Norris, F.H.; Tracy, M.; Galea, S. Looking for Resilience: Understanding the Longitudinal Trajectories of Responses to Stress. Soc. Sci. Med. 2009, 68, 2190–2198. [Google Scholar] [CrossRef]
- Rigutto, C.; Sapara, A.O.; Agyapong, V.I.O. Anxiety, Depression and Posttraumatic Stress Disorder after Terrorist Attacks: A General Review of the Literature. Behav. Sci. 2021, 11, 140. [Google Scholar] [CrossRef]
- Pietrzak, R.H.; Feder, A.; Singh, R.; Schechter, C.B.; Bromet, E.J.; Katz, C.L.; Reissman, D.B.; Ozbay, F.; Sharma, V.; Crane, M.; et al. Trajectories of PTSD Risk and Resilience in World Trade Center Responders: An 8-Year Prospective Cohort Study. Psychol. Med. 2014, 44, 205–219. [Google Scholar] [CrossRef]
- Debchoudhury, I.; Welch, A.E.; Fairclough, M.A.; Cone, J.E.; Brackbill, R.M.; Stellman, S.D.; Farfel, M.R. Comparison of Health Outcomes among Affiliated and Lay Disaster Volunteers Enrolled in the World Trade Center Health Registry. Prev. Med. 2011, 53, 359–363. [Google Scholar] [CrossRef] [Green Version]
- Santiago, P.N.; Ursano, R.J.; Gray, C.L.; Pynoos, R.S.; Spiegel, D.; Lewis-Fernandez, R.; Friedman, M.J.; Fullerton, C.S. A Systematic Review of PTSD Prevalence and Trajectories in DSM-5 Defined Trauma Exposed Populations: Intentional and Non-Intentional Traumatic Events. PLoS ONE 2013, 8, e59236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pietrzak, R.H.; Schechter, C.B.; Bromet, E.J.; Katz, C.L.; Reissman, D.B.; Ozbay, F.; Sharma, V.; Crane, M.; Harrison, D.; Herbert, R.; et al. The Burden of Full and Subsyndromal Posttraumatic Stress Disorder among Police Involved in the World Trade Center Rescue and Recovery Effort. J. Psychiatr. Res. 2012, 46, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Brackbill, R.M.; Hadler, J.L.; DiGrande, L.; Ekenga, C.C.; Farfel, M.R.; Friedman, S.; Perlman, S.E.; Stellman, S.D.; Walker, D.J.; Wu, D.; et al. Asthma and Posttraumatic Stress Symptoms 5 to 6 Years Following Exposure to the World Trade Center Terrorist Attack. JAMA 2009, 302, 502–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motreff, Y.; Pirard, P.; Vuillermoz, C.; Rabet, G.; Petitclerc, M.; Stene, L.E.; Baubet, T.; Chauvin, P.; Vandentorren, S. Mental Health Care Utilization by First Responders after Paris Attacks. Occup. Med. Oxf. Engl. 2022, 72, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Pirard, P.; Baubet, T.; Motreff, Y.; Rabet, G.; Marillier, M.; Vandentorren, S.; Vuillermoz, C.; Stene, L.E.; Messiah, A. Use of Mental Health Supports by Civilians Exposed to the November 2015 Terrorist Attacks in Paris. BMC Health Serv. Res. 2020, 20, 959. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Litz, B.T.; Keane, T.M.; Palmieri, P.A.; Marx, B.P.; Schnurr, P.P. The PTSD Checklist for DSM-5 (PCL-5). 2013. Available online: https://www.ptsd.va.gov/ (accessed on 22 July 2022).
- Ashbaugh, A.R.; Houle-Johnson, S.; Herbert, C.; El-Hage, W.; Brunet, A. Psychometric Validation of the English and French Versions of the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5). PLoS ONE 2016, 11, e0161645. [Google Scholar] [CrossRef]
- Bovin, M.J.; Marx, B.P.; Weathers, F.W.; Gallagher, M.W.; Rodriguez, P.; Schnurr, P.P.; Keane, T.M. Psychometric Properties of the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders–Fifth Edition (PCL-5) in Veterans. Psychol. Assess. 2016, 28, 1379–1391. [Google Scholar] [CrossRef]
- Krüger-Gottschalk, A.; Knaevelsrud, C.; Rau, H.; Dyer, A.; Schäfer, I.; Schellong, J.; Ehring, T. The German Version of the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Psychometric Properties and Diagnostic Utility. BMC Psychiatry 2017, 17, 379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLaughlin, K.A.; Koenen, K.C.; Friedman, M.J.; Ruscio, A.M.; Karam, E.G.; Shahly, V.; Stein, D.J.; Hill, E.D.; Petukhova, M.; Alonso, J.; et al. Subthreshold Posttraumatic Stress Disorder in the World Health Organization World Mental Health Surveys. Biol. Psychiatry 2015, 77, 375–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Empereur-bissonnet, P.; Perrine, A.; Pédrono, G.; El Haddad, M.; Zeghnoun, A.; Richard, J.; Blanchard, M.; Saoudi, A.; Motreff, Y.; Morel, P.; et al. Santé Post Incendie 76—Une Étude à l’écoute de Votre Santé. Étude Épidémiologique Par Questionnaire Sur l’incendie Industriel Du 26 Septembre 2019 à Rouen (France); Rapport principal; Santé Publique France: Saint-Maurice, France, 2021; 81p. [Google Scholar]
- Bowler, R.M.; Han, H.; Gocheva, V.; Nakagawa, S.; Alper, H.; DiGrande, L.; Cone, J.E. Gender Differences in Probable Posttraumatic Stress Disorder among Police Responders to the 2001 World Trade Center Terrorist Attack. Am. J. Ind. Med. 2010, 53, 1186–1196. [Google Scholar] [CrossRef]
- Perrin, M.A.; DiGrande, L.; Wheeler, K.; Thorpe, L.; Farfel, M.; Brackbill, R. Differences in PTSD Prevalence and Associated Risk Factors among World Trade Center Disaster Rescue and Recovery Workers. Am. J. Psychiatry 2007, 164, 1385–1394. [Google Scholar] [CrossRef]
- De Stefano, C.; Orri, M.; Agostinucci, J.M.; Zouaghi, H.; Lapostolle, F.; Baubet, T.; Adnet, F. Early Psychological Impact of Paris Terrorist Attacks on Healthcare Emergency Staff: A Cross-Sectional Study. Depress. Anxiety 2018, 35, 275–282. [Google Scholar] [CrossRef]
- Vandentorren, S.; Pirard, P.; Sanna, A.; Aubert, L.; Motreff, Y.; Dantchev, N.; Lesieur, S.; Chauvin, P.; Baubet, T. Healthcare Provision and the Psychological, Somatic and Social Impact on People Involved in the Terror Attacks in January 2015 in Paris: Cohort Study. Br. J. Psychiatry 2018, 212, 207–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuillermoz, C.; Stene, L.E.; Aubert, L.; Motreff, Y.; Pirard, P.; Baubet, T.; Lesieur, S.; Chauvin, P.; Vandentorren, S. Non-Participation and Attrition in a Longitudinal Study of Civilians Exposed to the January 2015 Terrorist Attacks in Paris, France. BMC Med. Res. Methodol. 2020, 20, 63. [Google Scholar] [CrossRef]
- Weisæth, L. Importance of High Response Rates in Traumatic Stress Research. Acta Psychiatr. Scand. 1989, 80, 131–137. [Google Scholar] [CrossRef]
- Stene, L.E.; Dyb, G. Research Participation after Terrorism: An Open Cohort Study of Survivors and Parents after the 2011 Utøya Attack in Norway. BMC Res. Notes 2016, 9, 57. [Google Scholar] [CrossRef] [Green Version]
- Meudal, J.; Vandentorren, S.; Simeoni, L.; Denis, C. French Red Cross Volunteer Rescue Workers: Psychological Characteristics and Healthcare Support after the January 2015 Terrorist Attacks in Paris. J. Nerv. Ment. Dis. 2020, 208, 413–417. [Google Scholar] [CrossRef]
- Berninger, A.; Webber, M.P.; Niles, J.K.; Gustave, J.; Lee, R.; Cohen, H.W.; Kelly, K.; Corrigan, M.; Prezant, D.J. Longitudinal Study of Probable Post-Traumatic Stress Disorder in Firefighters Exposed to the World Trade Center Disaster. Am. J. Ind. Med. 2010, 53, 1177–1185. [Google Scholar] [CrossRef]
- Bowler, R.M.; Harris, M.; Li, J.; Gocheva, V.; Stellman, S.D.; Wilson, K.; Alper, H.; Schwarzer, R.; Cone, J.E. Longitudinal Mental Health Impact among Police Responders to the 9/11 Terrorist Attack. Am. J. Ind. Med. 2012, 55, 297–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feder, A.; Mota, N.; Salim, R.; Rodriguez, J.; Singh, R.; Schaffer, J.; Schechter, C.B.; Cancelmo, L.M.; Bromet, E.J.; Katz, C.L.; et al. Risk, Coping and PTSD Symptom Trajectories in World Trade Center Responders. J. Psychiatr. Res. 2016, 82, 68–79. [Google Scholar] [CrossRef]
- Maslow, C.B.; Caramanica, K.; Welch, A.E.; Stellman, S.D.; Brackbill, R.M.; Farfel, M.R. Trajectories of Scores on a Screening Instrument for PTSD among World Trade Center Rescue, Recovery, and Clean-Up Workers. J. Trauma. Stress 2015, 28, 198–205. [Google Scholar] [CrossRef]
- Sareen, J. Posttraumatic Stress Disorder in Adults: Impact, Comorbidity, Risk Factors, and Treatment. Can. J. Psychiatry Rev. Can. Psychiatr. 2014, 59, 460–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, N.; Checkoway, H.; Kriebel, D. Bias in Occupational Epidemiology Studies. Occup. Environ. Med. 2007, 64, 562–568. [Google Scholar] [CrossRef] [Green Version]
- Schlenger, W.E.; Silver, R.C. Web-Based Methods in Terrorism and Disaster Research. J. Trauma. Stress 2006, 19, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.S.; Lane, M.; Olfson, M.; Pincus, H.A.; Wells, K.B.; Kessler, R.C. Twelve-Month Use of Mental Health Services in the United States: Results from the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 629–640. [Google Scholar] [CrossRef] [Green Version]
- Bentz, L.; Vandentorren, S.; Fabre, R.; Bride, J.; Pirard, P.; Doulet, N.; Baubet, T.; Motreff, Y.; Pradier, C. Mental Health Impact among Hospital Staff in the Aftermath of the Nice 2016 Terror Attack: The ECHOS de Nice Study. BMC Public Health 2021, 21, 1372. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| PTSD | Partial PTSD | |||||
|---|---|---|---|---|---|---|
| n | % | 95% CI | n | % | 95% CI | |
| Firefighters | 18 | 9.6 | 5.4–13.8 | 38 | 20.2 | 14.6–25.9 |
| Healthcare professionals | 8 | 7.4 | 2.4–12.3 | 16 | 14.8 | 8.1–21.5 |
| Affiliated volunteers | 4 | 5.5 | 0.3–10.7 | 20 | 27.4 | 17.2–37.6 |
| Police officers | 7 | 11.9 | 3.6–20.1 | 20 | 33.9 | 21.8–46.0 |
| Total | 37 | 8.6 | 6.0–11.3 | 94 | 22.0 | 18.0–25.9 |
| Trajectory | n | % |
|---|---|---|
| Resistant (No PTSD → No PTSD) | 158 | 61.2 |
| Complete recovery (PTSD → No PTSD) | 3 | - |
| Remission (Partial PTSD → No PTSD) | 20 | 7.7 |
| Partial recovery (PTSD → Partial PTSD) | 4 | - |
| Delayed onset PTSD (No PTSD → PTSD) | 6 | 2.3 |
| Delayed onset partial PTSD (No PTSD → Partial PTSD) | 30 | 11.6 |
| Worsening (Partial PTSD → PTSD) | 3 | - |
| Moderate chronic (Partial PTSD → Partial PTSD) | 23 | 8.9 |
| Severe chronic (PTSD → PTSD) | 11 | 4.3 |
| Total | 258 | 100.0 |
| PTSD | Partial PTSD | |||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Gender | ||||
| Male | 1.00 | - | 1.00 | - |
| Female | 0.75 | 0.21–2.68 | 1.15 | 0.53–2.48 |
| First responder category | ||||
| Firefighters | 1.00 | - | 1.00 | - |
| Affiliated volunteers | 0.27 | 0.05–1.38 | 1.75 | 0.73–4.16 |
| Police officers | 2.19 | 0.44–10.79 | 2.44 | 0.88–6.70 |
| Health professionals | 1.24 | 0.24–6.46 | 1.60 | 0.53–4.83 |
| Intervention category (exposure) | ||||
| 1- The evening of 13 November and at unsecured crime scenes * | 3.59 | 0.99–13.02 | 3.56 | 1.55–8.16 |
| 2- On the evening of 13 November and at secure or remote crime scenes ** | 1.00 | - | 1.00 | - |
| 3- Only during the 3 weeks following the attacks | 0.42 | 0.07–2.36 | 0.99 | 0.38–2.58 |
| Educational level | ||||
| Graduate or post-graduate degree | 1.00 | - | 1.00 | - |
| High school diploma | 0.62 | 0.18–2.06 | 1.10 | 0.48–2.49 |
| No high school diploma | 0.19 | 0.03–1.15 | 0.74 | 0.26–2.14 |
| Social isolation | ||||
| No | 1.00 | - | 1.00 | - |
| Yes | 3.14 | 0.93–10.6 | 2.27 | 0.93–5.53 |
| Traumatic events prior to the 2015 attacks | ||||
| No | 1.00 | - | 1.00 | - |
| Yes and intentional | 1.05 | 0.25–4.42 | 2.40 | 1.05–5.47 |
| Yes and not intentional | 1.16 | 0.38–3.55 | 1.85 | 0.93–3.66 |
| History of anti-depressant consumption | ||||
| No | 1.00 | - | 1.00 | - |
| Yes | 1.33 | 0.15–11.58 | 0.69 | 0.19–2.51 |
| Raising awareness of psychological risks in the context of professional activity through specific training | ||||
| 25 years | ||||
| Before and after the attacks | 1.00 | - | 1.00 | - |
| Before or after the attacks | 0.83 | 0.13–5.46 | 0.66 | 0.18–2.41 |
| Neither before nor after the attacks | 0.48 | 0.03–6.75 | 0.23 | 0.04–1.28 |
| 35 years | ||||
| Before and after the attacks | 1.00 | - | 1.00 | - |
| Before or after the attacks | 1.97 | 0.65–5.97 | 1.26 | 0.58–2.77 |
| Neither before nor after the attacks | 1.41 | 0.31–6.45 | 1.05 | 0.37–2.96 |
| 45 years | ||||
| Before and after the attacks | 1.00 | - | 1.00 | - |
| Before or after the attacks | 4.68 | 1.11–19.69 | 2.43 | 1.12–5.27 |
| Neither before nor after the attacks | 4.17 | 0.57–30.38 | 4.77 | 1.92–11.86 |
| Concern about the COVID-19 epidemic (scale of 0 to 10) | ||||
| 0–3 | 1.00 | - | 1.00 | - |
| 3–7 | 1.67 | 0.51–5.48 | 1.06 | 0.55–2.07 |
| 7–10 | 6.40 | 1.66–24.76 | 1.52 | 0.62–3.70 |
| Number of somatic problems present after the attacks of 13 November 2015 | 2.01 | 1.55–2.61 | 1.18 | 0.99–1.39 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prioux, C.; Marillier, M.; Vuillermoz, C.; Vandentorren, S.; Rabet, G.; Petitclerc, M.; Baubet, T.; Stene, L.E.; Pirard, P.; Motreff, Y. PTSD and Partial PTSD among First Responders One and Five Years after the Paris Terror Attacks in November 2015. Int. J. Environ. Res. Public Health 2023, 20, 4160. https://doi.org/10.3390/ijerph20054160
Prioux C, Marillier M, Vuillermoz C, Vandentorren S, Rabet G, Petitclerc M, Baubet T, Stene LE, Pirard P, Motreff Y. PTSD and Partial PTSD among First Responders One and Five Years after the Paris Terror Attacks in November 2015. International Journal of Environmental Research and Public Health. 2023; 20(5):4160. https://doi.org/10.3390/ijerph20054160
Chicago/Turabian StylePrioux, Clémentine, Maude Marillier, Cécile Vuillermoz, Stéphanie Vandentorren, Gabrielle Rabet, Matthieu Petitclerc, Thierry Baubet, Lise Eilin Stene, Philippe Pirard, and Yvon Motreff. 2023. "PTSD and Partial PTSD among First Responders One and Five Years after the Paris Terror Attacks in November 2015" International Journal of Environmental Research and Public Health 20, no. 5: 4160. https://doi.org/10.3390/ijerph20054160