
Effectiveness of Pain Neuroscience Education in Patients with Chronic Musculoskeletal Pain and Central Sensitization: A Systematic Review


Abstract
:1. Introduction
1.1. Background
1.2. Objectives
2. Methods
2.1. Eligibility Criteria
2.1.1. Study Design
2.1.2. Participants
2.1.3. Interventions
2.1.4. Comparisons
2.1.5. Outcome and Outcome Measures
2.2. Search Methods for Inclusion of Studies
Electronic Searches
2.3. Study Selection and Data Extraction
2.4. Inter-Rater Agreement
2.5. Risk of Bias
2.6. Analysis
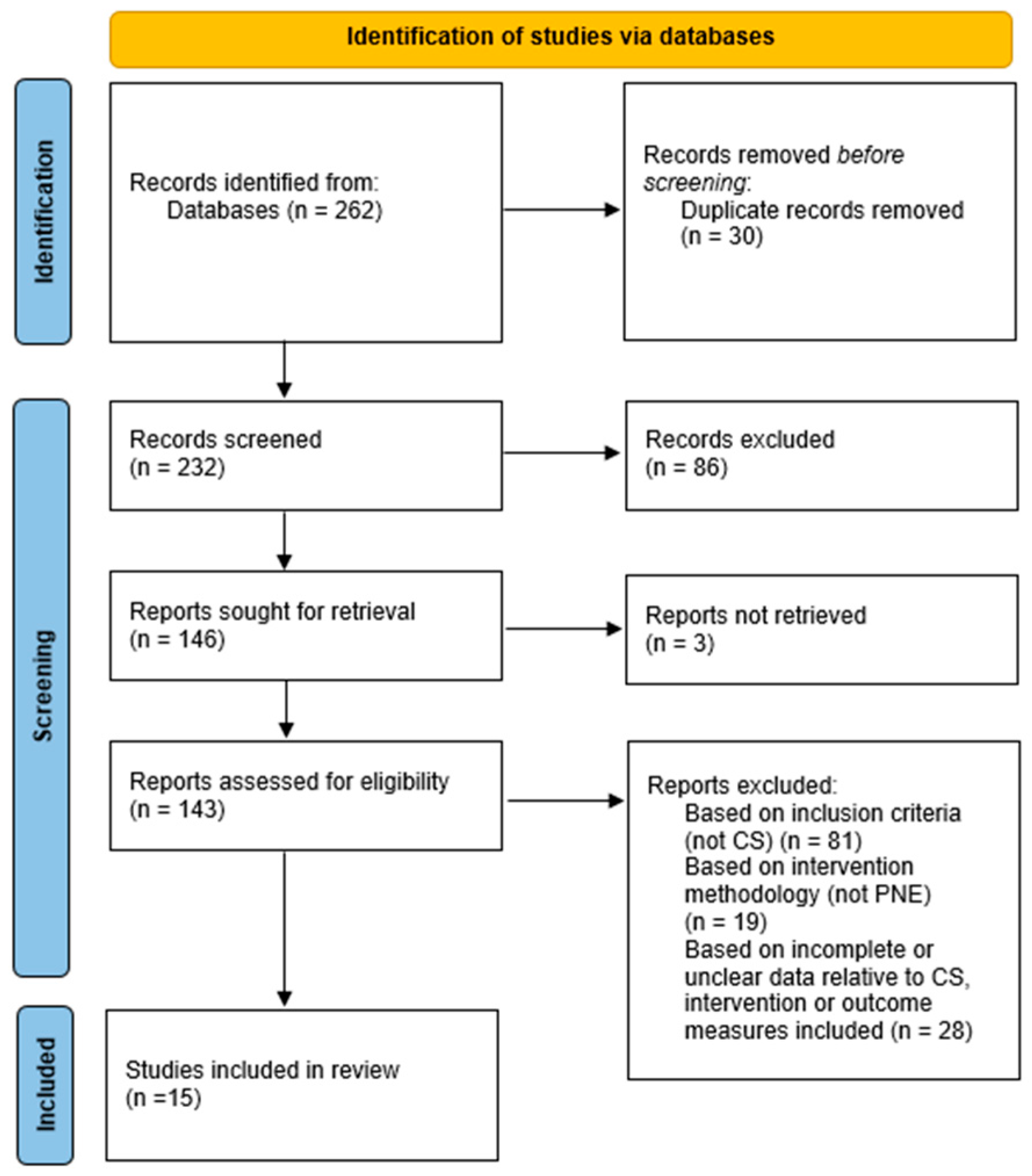
3. Results
3.1. Study Characteristics
3.1.1. Sample
3.1.2. Drop-Out and Lost to Follow-Up
3.1.3. Follow-Ups
3.1.4. Adverse Effects
3.1.5. Type of Participants
3.1.6. Type of Interventions
3.1.7. Type of Control Groups
3.1.8. Type of Outcome and Outcome Measures
3.2. Risk of Bias
3.3. Agreement
3.4. Effects of Interventions
3.4.1. Fibromyalgia
3.4.2. Chronic Spinal Pain (CSP)
3.4.3. CFS
3.4.4. Fibromyalgia and/or CLBP
3.4.5. CLBP
4. Discussion
4.1. Most Effective Strategies for Diagnostic Label
4.1.1. Fibromyalgia
4.1.2. CSP
4.1.3. CFS
4.1.4. Fibromyalgia and/or CLBP
4.1.5. CLBP
4.2. Applicability of Results and Training for Health Professionals
4.3. Consistency
4.4. Strengths and Limitations
5. Conclusions
5.1. Implications for Practice
5.2. Implications for Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Supplementary Data
References
- World Health Organization. Musculoskeletal Health. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions (accessed on 12 August 2022).
- Maselli, F.; Storari, L.; Barbari, V.; Colombi, A.; Turolla, A.; Gianola, S.; Rossettini, G.; Testa, M. Prevalence and incidence of low back pain among runners: A systematic review. BMC Musculoskelet. Disord. 2020, 21, 343. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Chen, M.; Wu, X.; Lin, S.; Tao, C.; Cao, H.; Shao, Z.; Xiao, G. Global, regional and national burden of low back pain 1990–2019: A systematic analysis of the Global Burden of Disease study 2019. J. Orthop. Transl. 2021, 32, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.; March, L.; Zheng, X.; Huang, J.; Wang, X.; Zhao, J.; Blyth, F.M.; Smith, E.; Buchbinder, R.; Hoy, D. Global low back pain prevalence and years lived with disability from 1990 to 2017: Estimates from the Global Burden of Disease Study 2017. Ann. Transl. Med. 2020, 8, 299. [Google Scholar] [CrossRef] [PubMed]
- Bonica, J.J. The Management of Pain, 2nd ed.; Lea & Febiger: Philadelphia, PA, USA, 1990. [Google Scholar]
- Treede, R.D.; Rief, W.; Barke, A.; Aziz, Q.; Bennett, M.I.; Benoliel, R.; Cohen, M.; Evers, S.; Finnerup, N.B.; First, M.B.; et al. A classification of chronic pain for ICD-11. Pain 2015, 156, 1003–1007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merskey, H.; Bogduk, N. Classification of Chronic Pain, 2nd ed.; IASP Task Force on Taxonomy; IASP Press: Seattle, WA, USA, 1994. [Google Scholar]
- Perrot, S.; Cohen, M.; Barke, A.; Korwisi, B.; Rief, W.; Treede, R.D.; IASP Taskforce for the Classification of Chronic Pain. The IASP classification of chronic pain for ICD-11: Chronic secondary musculoskeletal pain. Pain 2019, 160, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Cimmino, M.A.; Ferrone, C.; Cutolo, M. Epidemiology of chronic musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 2011, 25, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Kinney, M.; Seider, J.; Beaty, A.F.; Coughlin, K.; Dyal, M.; Clewley, D. The impact of therapeutic alliance in physical therapy for chronic musculoskeletal pain: A systematic review of the literature. Physiother. Theory Pract. 2020, 36, 886–898. [Google Scholar] [CrossRef]
- McCarberg, B.H.; Nicholson, B.D.; Todd, K.H.; Palmer, T.; Penles, L. The impact of pain on quality of life and the unmet needs of pain management: Results from pain sufferers and physicians participating in an Internet survey. Am. J. Ther. 2008, 15, 312–320. [Google Scholar] [CrossRef]
- Barbari, V.; Storari, L.; Ciuro, A.; Testa, M. Effectiveness of communicative and educative strategies in chronic low back pain patients: A systematic review. Patient Educ. Couns. 2020, 103, 908–929. [Google Scholar] [CrossRef]
- George, S.Z.; Fritz, J.M.; Silfies, S.P.; Schneider, M.J.; Beneciuk, J.M.; Lentz, T.A.; Gilliam, J.R.; Hendren, S.; Norman, K.S. Interventions for the Management of Acute and Chronic Low Back Pain: Revision 2021. J. Orthop. Sports Phys. Ther. 2021, 51, CPG1–CPG60. [Google Scholar] [CrossRef]
- Booth, J.; Moseley, G.L.; Schiltenwolf, M.; Cashin, A.; Davies, M.; Hübscher, M. Exercise for chronic musculoskeletal pain: A biopsychosocial approach. Musculoskelet. Care 2017, 15, 413–421. [Google Scholar] [CrossRef]
- Sharma, L. Osteoarthritis of the Knee. N. Engl. J. Med. 2021, 384, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, N.N.; Candido, K.D.; Vlaeyen, J.W.S.; Van Zundert, J.; Cohen, S.P. Low back pain. Lancet 2021, 398, 78–92. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Qaseem, A.; Snow, V.; Casey, D.; Cross, J.T., Jr.; Shekelle, P.; Owens, D.K.; Clinical Efficacy Assessment Subcommittee of the American College of Physicians; American College of Physicians; American Pain Society Low Back Pain Guidelines Panel. Diagnosis and treatment of low back pain: A joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann. Intern. Med. 2007, 47, 478–491. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Diener, I.; Butler, D.S.; Puentedura, E.J. The effect of neuroscience education on pain, disability, anxiety, and stress in chronic musculoskeletal pain. Arch. Phys. Med. Rehabil. 2011, 92, 2041–2056. [Google Scholar] [CrossRef]
- Louw, A.; Zimney, K.; Puentedura, E.J.; Diener, I. The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Physiother. Theory Pract. 2016, 32, 332–355. [Google Scholar] [CrossRef]
- Wood, L.; Hendrick, P.A. A systematic review and meta-analysis of pain neuroscience education for chronic low back pain: Short-and long-term outcomes of pain and disability. Eur. J. Pain 2019, 23, 234–249. [Google Scholar] [CrossRef]
- Watson, J.A.; Ryan, C.G.; Cooper, L.; Ellington, D.; Whittle, R.; Lavender, M.; Dixon, J.; Atkinson, G.; Cooper, K.; Martin, D.J. Pain Neuroscience Education for Adults With Chronic Musculoskeletal Pain: A Mixed-Methods Systematic Review and Meta-Analysis. J. Pain 2019, 20, 1140.e1–1140.e22. [Google Scholar] [CrossRef]
- Suso-Martí, L.; Cuenca-Martínez, F.; Alba-Quesada, P.; Muñoz-Alarcos, V.; Herranz-Gómez, A.; Varangot-Reille, C.; Domínguez-Navarro, F.; Casaña, J. Effectiveness of Pain Neuroscience Education in Patients with Fibromyalgia: A Systematic Review and Meta-Analysis. Pain Med. 2022, 23, 1837–1850. [Google Scholar] [CrossRef]
- Moseley, G.L. Reconceptualising pain according to modern pain science. Phys. Ther. Rev. 2007, 12, 169–178. [Google Scholar] [CrossRef]
- Nijs, J.; Paul van Wilgen, C.; Van Oosterwijck, J.; van Ittersum, M.; Meeus, M. How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: Practice guidelines. Man. Ther. 2011, 16, 413–418. [Google Scholar] [CrossRef] [Green Version]
- Barbari, V.; Storari, L.; Maselli, F.; Testa, M. Applicability of pain neuroscience education: Where are we now? J. Back Musculoskelet. Rehabil. 2021, 34, 511–520. [Google Scholar] [CrossRef]
- Nijs, J.; Van Houdenhove, B.; Oostendorp, R.A. Recognition of central sensitization in patients with musculoskeletal pain: Application of pain neurophysiology in manual therapy practice. Man. Ther. 2010, 15, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Puentedura, E.J.; Flynn, T. Combining manual therapy with pain neuroscience education in the treatment of chronic low back pain: A narrative review of the literature. Physiother. Theory Pract. 2016, 32, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Nijs, J.; Puentedura, E.J. A clinical perspective on a pain neuroscience education approach to manual therapy. J. Man. Manip. Ther. 2017, 25, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The nuts and bolts of PROSPERO: An international prospective register of systematic reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosek, E.; Cohen, M.; Baron, R.; Gebhart, G.F.; Mico, J.A.; Rice, A.S.C.; Rief, W.; Sluka, A.K. Do we need a third mechanistic descriptor for chronic pain states? Pain 2016, 157, 1382–1386. [Google Scholar] [CrossRef] [PubMed]
- Kosek, E.; Clauw, D.; Nijs, J.; Baron, R.; Gilron, I.; Harris, R.E.; Mico, J.A.; Rice, A.S.C.; Sterling, M. Chronic nociplastic pain affecting the musculoskeletal system: Clinical criteria and grading system. Pain 2021, 162, 2629–2634. [Google Scholar] [CrossRef]
- Altman, D.G. Practical Statistics for Medical Research, 1st ed.; Chapman and Hall: London, UK, 1990. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Barrenengoa-Cuadra, M.J.; Muñoa-Capron-Manieux, M.; Fernández-Luco, M.; Angón-Puras, L.Á.; Romón-Gómez, A.J.; Azkuenaga, M.; Etxebarria, A.; Orrantia, G.; Pikaza, A.; Uribe-Etxebarria, L.; et al. Effectiveness of a structured group intervention based on pain neuroscience education for patients with fibromyalgia in primary care: A multicentre randomized open-label controlled trial. Eur. J. Pain 2021, 25, 1137–1149. [Google Scholar] [CrossRef] [PubMed]
- Bodes Pardo, G.; Lluch Girbés, E.; Roussel, N.A.; Gallego Izquierdo, T.; Jiménez Penick, V.; Pecos Martín, D. Pain Neurophysiology Education and Therapeutic Exercise for Patients With Chronic Low Back Pain: A Single-Blind Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2018, 99, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Gül, H.; Erel, S.; Toraman, N.F. Physiotherapy combined with therapeutic neuroscience education versus physiotherapy alone for patients with chronic low back pain: A pilot, randomized-controlled trial. Turk. J. Phys. Med. Rehabil. 2021, 67, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Kohns, D.J.; Urbanik, C.P.; Geisser, M.E.; Schubiner, H.; Lumley, M.A. The Effects of a Pain Psychology and Neuroscience Self-Evaluation Internet Intervention: A Randomized Controlled Trial. Clin. J. Pain 2020, 36, 683–692. [Google Scholar] [CrossRef] [PubMed]
- Malfliet, A.; Kregel, J.; Meeus, M.; Danneels, L.; Cagnie, B.; Roussel, N.; Nijs, J. Patients with Chronic Spinal Pain Benefit from Pain Neuroscience Education Regardless the Self-Reported Signs of Central Sensitization: Secondary Analysis of a Randomized Controlled Multicenter Trial. PM R 2018, 10, 1330–1343.e1. [Google Scholar] [CrossRef] [PubMed]
- Meeus, M.; Nijs, J.; Van Oosterwijck, J.; Van Alsenoy, V.; Truijen, S. Pain physiology education improves pain beliefs in patients with chronic fatigue syndrome compared with pacing and self-management education: A double-blind randomized controlled trial. Arch. Phys. Med. Rehabil. 2010, 91, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Orhan, C.; Lenoir, D.; Favoreel, A.; Van Looveren, E.; Yildiz Kabak, V.; Mukhtar, N.B.; Cagnie, B.; Meeus, M. Culture-sensitive and standard pain neuroscience education improves pain, disability, and pain cognitions in first-generation Turkish migrants with chronic low back pain: A pilot randomized controlled trial. Physiother. Theory Pract. 2021, 37, 633–645. [Google Scholar] [CrossRef]
- Pires, D.; Cruz, E.B.; Caeiro, C. Aquatic exercise and pain neurophysiology education versus aquatic exercise alone for patients with chronic low back pain: A randomized controlled trial. Clin. Rehabil. 2015, 29, 538–547. [Google Scholar] [CrossRef]
- Rabiei, P.; Sheikhi, B.; Letafatkar, A. Comparing Pain Neuroscience Education Followed by Motor Control Exercises With Group-Based Exercises for Chronic Low Back Pain: A Randomized Controlled Trial. Pain Pract. 2021, 21, 333–342. [Google Scholar] [CrossRef]
- Ryan, C.G.; Gray, H.G.; Newton, M.; Granat, M.H. Pain biology education and exercise classes compared to pain biology education alone for individuals with chronic low back pain: A pilot randomised controlled trial. Man. Ther. 2010, 15, 382–387. [Google Scholar] [CrossRef]
- Saracoglu, I.; Arik, M.I.; Afsar, E.; Gokpinar, H.H. The effectiveness of pain neuroscience education combined with manual therapy and home exercise for chronic low back pain: A single-blind randomized controlled trial. Physiother. Theory Pract. 2022, 38, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Serrat, M.; Almirall, M.; Musté, M.; Sanabria-Mazo, J.P.; Feliu-Soler, A.; Méndez-Ulrich, J.L.; Luciano, J.V.; Sanz, A. Effectiveness of a Multicomponent Treatment for Fibromyalgia Based on Pain Neuroscience Education, Exercise Therapy, Psychological Support, and Nature Exposure (NAT-FM): A Pragmatic Randomized Controlled Trial. J. Clin. Med. 2020, 9, 3348. [Google Scholar] [CrossRef]
- Téllez-García, M.; de-la-Llave-Rincón, A.I.; Salom-Moreno, J.; Palacios-Ceña, M.; Ortega-Santiago, R.; Fernández-de-Las-Peñas, C. Neuroscience education in addition to trigger point dry needling for the management of patients with mechanical chronic low back pain: A preliminary clinical trial. J. Bodyw. Mov. Ther. 2015, 19, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Van Ittersum, M.W.; van Wilgen, C.P.; van der Schans, C.P.; Lambrecht, L.; Groothoff, J.W.; Nijs, J. Written pain neuroscience education in fibromyalgia: A multicenter randomized controlled trial. Pain Pract. 2014, 14, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Van Oosterwijck, J.; Meeus, M.; Paul, L.; De Schryver, M.; Pascal, A.; Lambrecht, L.; Nijs, J. Pain physiology education improves health status and endogenous pain inhibition in fibromyalgia: A double-blind randomized controlled trial. Clin. J. Pain 2013, 29, 873–882. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 Criteria for the Classification of Fibromyalgia. Report of the Multicenter Criteria Committee. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Shiri, R.; Coggon, D.; Falah-Hassani, K. Exercise for the Prevention of Low Back Pain: Systematic Review and Meta-Analysis of Controlled Trials. Am. J. Epidemiol. 2018, 187, 1093–1101. [Google Scholar] [CrossRef] [Green Version]
- Gordon, R.; Bloxham, S. A Systematic Review of the Effects of Exercise and Physical Activity on Non-Specific Chronic Low Back Pain. Healthcare 2016, 4, 22. [Google Scholar] [CrossRef] [Green Version]
- Searle, A.; Spink, M.; Ho, A.; Chuter, V. Exercise interventions for the treatment of chronic low back pain: A systematic review and meta-analysis of randomised controlled trials. Clin. Rehabil. 2015, 29, 1155–1167. [Google Scholar] [CrossRef]
- Quentin, C.; Bagheri, R.; Ugbolue, U.C.; Coudeyre, E.; Pélissier, C.; Descatha, A.; Menini, T.; Bouillon-Minois, J.B.; Dutheil, F. Effect of Home Exercise Training in Patients with Nonspecific Low-Back Pain: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8430. [Google Scholar] [CrossRef]
- Maselli, F.; Palladino, M.; Barbari, V.; Storari, L.; Rossettini, G.; Testa, M. The diagnostic value of Red Flags in thoracolumbar pain: A systematic review. Disabil. Rehabil. 2022, 44, 1190–1206. [Google Scholar] [CrossRef]
- Andreoletti, F.; Maselli, F.; Storari, L.; Vongher, A.; Erbesato, M.; Testa, M.; Turolla, A. Screening for Referral of Serious Pathology by Physical Examination Tests in Patients with Back or Chest Pain: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 16418. [Google Scholar] [CrossRef] [PubMed]
- Pennella, D.; Giagio, S.; Maselli, F.; Giovannico, G.; Roncone, A.; Fiorentino, F.; Brindisino, F. Red flags useful to screen for gastrointestinal and hepatic diseases in patients with shoulder pain: A scoping review. Musculoskelet. Care 2022, 20, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Piano, L.; Maselli, F.; Viceconti, A.; Gianola, S.; Ciuro, A. Direct access to physical therapy for the patient with musculoskeletal disorders, a literature review. J. Phys. Ther. Sci. 2017, 29, 1463–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooker, S.P.; Buchner, D.M. Education and training in physical activity research and practice. Prev. Med. 2009, 49, 294–296. [Google Scholar] [CrossRef] [PubMed]
- Coombes, J.S.; Williams, A.; Radford, J. Training health professionals to provide physical activity counselling. Prog. Cardiovasc. Dis. 2021, 64, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Netherway, J.; Smith, B.; Monforte, J. Training Healthcare Professionals on How to Promote Physical Activity in the UK: A Scoping Review of Current Trends and Future Opportunities. Int. J. Environ. Res. Public Health 2021, 18, 6701. [Google Scholar] [CrossRef]
- Siddall, B.; Ram, A.; Jones, M.D.; Booth, J.; Perriman, D.; Summers, S.J. Short-term impact of combining pain neuroscience education with exercise for chronic musculoskeletal pain: A systematic review and meta-analysis. Pain 2022, 163, e20–e30. [Google Scholar] [CrossRef]
- Bülow, K.; Lindberg, K.; Vaegter, H.B.; Juhl, C.B. Effectiveness of Pain Neurophysiology Education on Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Pain Med. 2021, 22, 891–904. [Google Scholar] [CrossRef]


{kind=link}
| General Informations (Author, Years, Study Design, Country) | Partecipants (Characteristics, Number, Age, Gender, Recriument) | Interventions (Number of Participants, Content, Frequency, Duration and Professional in Charge) | Comparisons (Number of Participants, Content, Frequency, Duration and Professional in Charge) | Outcome Measures and Follow-Up | Results (EX: Experimental Group; C: Control Group) |
|---|---|---|---|---|---|
| Barrenengoa-Cuadra et al. [35], in 2021 RCT Spain | Fibromyalgia according to American College of Reumatology criteria (ACR) [50] N = 140 Age: > 18 years Patients recruited from waiting lists at five medical centres in Bilbao, using an electronic database. | Number (N) = 70, Male (M) = 2, Female (F) = 68, Age = 52,3 ± 9,2 1- Pain Neuroscience Education (PNE): 6 weekly lessons lasting 2 h, plus a 7° session as reinforcement after 1 month. The intervention involved the use of audio-visual material to treat concepts related to the neurobiology of pain and movement awareness. The material was also sent by email to patients after each session. Professional in charge: multidisciplinary team composed of 2–3 physiotherapists specialized in educational interventions on fibromyalgic patients 2- Usual care (same as control group) | N = 69, M = 6, F = 63, Age = 51.4 ± 10.2 1- Usual care: In Spain, the usual treatments include use of drugs, the most used are antidepressants, antiepileptics and analgesics. Professional in charge: doctors for prescription of medicines. | Fibromyalgia Impact Questionnaire (FIQ) Brief Pain Inventory (BPI-SF) Health Assessment Questionnaire (HAQ) Hospital Anxiety and Depression Scale (HADS) Pain Catastrophizing Scale (PCS-13) Baseline 1 month 6 months 12 months | FIQ EX: 60.9 ± 15.3 ⟶ 36.5 ± 21.8 ⟶ 38.0 ± 24.2 ⟶ 37.4 ± 24.1 C: 60.1 ± 13.8 ⟶ 60.6 ± 12.8 ⟶ 57.0 ± 14.3 ⟶ 56.7 ± 15.6 p < 0.001 BPI-SF (severity) EX: 5.8 ± 1.7 ⟶ 3.5 ± 1.9 ⟶ 4.0 ± 2.2 ⟶ 3.7 ± 2.2 C: 5.6 ± 1.7 ⟶ 5.7 ± 1.7 ⟶ 5.2 ± 1.9 ⟶ 5.5 ± 1.8 p < 0.05 BPI-SF (interference) EX: 6.6 ± 2.2 ⟶ 3.5 ± 2.7 ⟶ 3.6 ± 2.7 ⟶ 3.5 ± 2.7 C: 6.4 ± 2.2 ⟶ 6.6 ± 2.2 ⟶ 5.7 ± 2.2 ⟶ 5.9 ± 2.3 p < 0.05 HAQ EX: 1.4 ± 0.5 ⟶ 0.6 ± 0.5 ⟶ 0.6 ± 0.5 ⟶ 0.7 ± 0.5 C: 1.3 ± 0.6 ⟶ 1.1 ± 0.6 ⟶ 1.0 ± 0.6 ⟶ 1.1 ± 0.6 p < 0.05 HADS (anxiety) EX: 13.1 ± 3.9 ⟶ 8.4 ± 4.6 ⟶ 8.7 ± 4.9 ⟶ 8.2 ± 4.2 C: 12.3 ± 4.2 ⟶ 11.8 ± 4.3 ⟶ 11.8 ± 4.1 ⟶ 11.9 ± 4.1 p < 0.05 HADS (depression) EX: 9.5 ± 4.4 ⟶ 1.3 ± 0.9 ⟶ 4.9 ± 4.5 ⟶ 5.1 ± 4.9 C: 9.2 ± 4.0 ⟶ 2.4 ± 2.4 ⟶ 9.3 ± 4.5 ⟶ 8.8 ± 4.7 p < 0.05 PCS-13 EX: 26.9 ± 14.6 ⟶ 11.0 ± 11.3 ⟶ 11.6 ± 12.8 ⟶ 10.6 ± 12.3 C: 24.4 ± 13.0 ⟶ 25.5 ± 15.7 ⟶ 23.8 ± 14.2 ⟶ 23.3 ± 15.5 p < 0.05 |
| Bodes et al. [36], in 2018 RCT Spain | CLBP > 6 months (patients with high CSI values at baseline) N = 56 Age: 20–75 Patients recruited through advertisements posted in four clinics and in the University of Alcalà in Madrid | N = 28, M = 6, F = 22, Age = 44.9 ± 9.6 1- PNE: 2 educational sessions of 30–50 min applied on patients divided into groups of 4–6 people. First session: explanation of the concepts underlying the neurophysiology of pain and delivery of a booklet to be read to reinforce the information shared. Second session (after 1 month): in-depth discussion and discussion of the contents of the first session. Professional in charge: physiotherapist expert on PNE. 2- Therapeutic exercise (same as control group) | N = 28, M = 6, F = 22, Age = 49.2 ± 10.5 1- Therapeutic exercise: proposed motor control exercises, stretching and aerobic exercises First session: Explanation of exercises to patients and supervision during execution in order to make them autonomous in following the plan at home. Exercises are done every day for 3 months Second session (after 1 month): control and correction of the exercises assigned in the first session. Professional in charge: physiotherapist experienced in motor control. | Numerical Pain Rating Scale (NPRS) Roland Morris Disability Questionnaire (RMDQ) Pain Catastrophizing Scale (PCS-13) Tampa Scale of Kinesiophobia (TSK-11) Baseline 1 month 3 months | NPRS EX: 7.9 [7.4,8.4] ⟶ 3.9 [3.2,4.6] ⟶ 2.7 [2.0,3.4] C: 7.8 [7.5,8.4] ⟶ 6.0 [5.4,6.6] ⟶ 4.8 [4.1,5.5] p < 0.001 3 months RMDQ EX: 12.0 [11.4,12.6] ⟶ 8.5 [7.8,9.3] ⟶ 6.4 [5.5,7.2] C: 12.6 [12.1,13.1] ⟶ 11.0 [10.3,11.6] ⟶ 9.8 [8.9,10.6] p < 0.001 3 months PCS-13 EX: 34.1 [31.2,37.0] ⟶ 22.2 [18.8,25.6] ⟶ 18.2 [15.4,21.0] C: 32.1 [30.2,34.1] ⟶ 28.7 [26.6,30.8] ⟶ 26.9 [24.8,29.0] p < 0.001 3 months TSK-11 EX: 28.7 [26.1,30.9] ⟶ 20.1 [18.5,21.6] ⟶ 16.1 [15.2,16.9] C: 28.1 [26.0,30.2] ⟶ 26.1 [24.1,28.0] ⟶ 24.1 [22.0,26.1] p < 0.001 3 months |
| Gül et al. [37], in 2021 RCT Turkey | CLBP > 3 months N = 31 M = 5, F = 26 Age: 18–60 Patients recruited from the clinic in Antalya | N = 16, Age: 42.1 ± 10.1 Both groups followed 15 sessions of physiotherapy, 3 each week. 1-TNE: 2 sessions per week, lasting 40 min. Conducting a one-to-one interview in a quiet and illuminated room; the arguments explained in the first session were related to neurophysiological mechanisms and psychosocial factors underlying pain. Images, metaphors, drawings were used and participants were given a brochure to read at home and the physiotherapist asked questions about the contents of the first session as reinforcement. Professional in charge: physiotherapist specialized on the TNE concept, as described by Moseley and Butler. 2- Physiotherapy (same as control group) | N = 15, Age: 42.5 ± 12.0 1- Physiotherapy: includes the use of: Hot-pack (20 min), ultrasound (10 min, intensity of 1,5 watt/cm2, frequency of 1 Mhz), TENS (at the beginning 80 μsec/100 Hz), successive sessions with acupuncture TENS (200 μsec/5 Hz for 20 min). Physiotherapist delivered a written program of exercises after teaching them to all patients. The exercise plan includes isotonic and isometric reinforcement, exercises for trunk muscles, stretching. Compliance was monitored with a diary. Professional in charge: physiotherapist | Visual Analogue Scale (VAS) Tampa Scale of Kinesiophobia (TSK-11) Roland Morris Disability Questionnaire (RMDQ) Baseline 3 weeks | VAS EX: Δ ⟶ −35.9 ± 28.3 C: Δ ⟶ 33.8 ± 29.5 p > 0.05 TSK-11 EX: Δ ⟶ −17.3 ± 12.1 C: Δ ⟶ −2.9 ± 6.4 p = 0.410 RMDQ EX: Δ ⟶ −8.8 ± 5.5 C: Δ ⟶ −5.7 ± 4.4 p > 0.05 |
| Kohns et al. [38], in 2020 RCT Michigan (USA) | LBP or Fibromyalgia ≥ 3 months N = 104 Patients recruited from the online registry: University of Michigan Health Research Volunteer Pool (umhealthresearch. org) | N = 51, M = 15, F = 35, Other = 1, Age: 44.35 ± 14.87 A single PPN session lasting 20–25 min, used a 3-min instructional video. Topics: pain, role of the brain in chronic pain, anatomy and physiology of the nervous system, perception of pain. At the end of the video, 5 self-assessment exercises to identify the presence of risk factors for central sensitization pain (compilation of body chart, assessment scales for risk factors, identification of personality traits related to chronic pain, identification of events that may affect chronic pain, Adverse Childhood Experience Scale). After a month and then after 10 months, participants were sent a link to a survey that contained follow-up measures. | N = 53, M = 11, F = 41, Other = 1 Age: 44.34 ± 14.69 Single session of self-assessment of health-related behaviors, lasting 20–25 min, used an educational video. Topics: 4 rules for a healthy lifestyle. at the end of the video 5 exercises to identify the habits of participants regarding: diet, exercise, sleep, hygiene, social relations. After a month and then after 10 months, participants were sent a link to a survey that contained follow-up measures. | Brief Pain Inventory (BPI) Patient-Reported Outcomes Measurement Information System (PROMIS) Pain Stages of Change Questionnaire (PSOCQ) Pain Catastrophizing Scale (PCS-13) Tampa Scale of Kinesiophobia (TSK-11) Satisfaction with Life Scale (SWLS) Baseline 1 month 10 months | BPI (severity) EX: 4.98 ± 1.54 ⟶ 4.03 ± 0.18 ⟶ 4.46 ± 0.23 C: 4.50 ± 1.73 ⟶ 4.60 ± 0.17 ⟶ 4.21 ± 0.23 p = 0.024 1 month p = 0.434 10 months BPI (interference) EX: 4.89 ± 2.44 ⟶ 3.91 ± 0.26 ⟶ 4.36 ± 0.29 C: 4.86 ± 2,64 ⟶ 4.71 ± 0.25 ⟶ 4.58 ± 0.28 p = 0.031 1 month p = 0.601 10 months PROMIS EX: 1.41 ± 0.77 ⟶ 1.34 ± 0.07 ⟶ 1.45 ± 0.08 C: 1.40 ± 0.85 ⟶ 1.47 ± 0.07 ⟶ 1.49 ± 0.08 p = 0.189 1 month p = 0.720 10 months PSOCQ EX: 8.28 ± 2.04 ⟶ 8.87 ± 0.19 ⟶ 8.64 ± 0.24 C: 8.02 ± 1.79 ⟶ 8.09 ± 0.19 ⟶ 8.39 ± 0.23 p = 0.005 1 month p = 0.447 10 months PCS-13 EX: 17.94 ± 10.94 ⟶ 15.44 ± 1.09 ⟶ 14.26 ± 1.03 C: 18.47 ± 12.15 ⟶ 17.61 ± 1.07 ⟶ 14.84 ± 1.01 p = 0.162 1 month p = 0.687 10 months TSK-11 EX: 24.55 ± 7.63 ⟶ 22.55 ± 0.54 ⟶ 23.77 ± 0.56 C: 24.13 ± 5.72 ⟶ 24.28 ± 0.53 ⟶ 24.16 ± 0.55 p = 0.082 1 month p = 0.623 10 months SWLS EX: 16.63 ± 7.08 ⟶ 17.71 ± 0.57 ⟶ 18.36 ± 0.70 C: 17.58 ± 8.43 ⟶ 17.30 ± 0.56 ⟶ 17.73 ± 0.69 p = 0.618 1 month p = 0.524 10 months |
| Malfliet et al. [39], in 2018 RCT Belgium | Chronic Spinal Pain (CSP) > 3 months N = 120 Age: 18–65 Patients recruited from two university medical centers through flyers, advertisements, social media. Patients divided into groups according to CSI levels. | N = 60, divided into: G1 = 24 (high CSI), M = 7, F = 17 Age: 36.58 ± 11.03 G2 = 36 (low CSI), M = 15, F = 21 Age: 40.47 ± 12.49 3 sessions in 2 weeks - First group session (max 6 people) with PNE education, used power point presentation (30–60 min). delivered a brochure to read at home. - Second online session with 3 videos and a final questionnaire. Topic for first and second session: anatomy and physiology of the nervous system, pain, factors influencing pain and central and peripheral sensitization. - Third individual session, 30 min of conversation one-by-one, with attention to the patient’s personal needs and discussion of the contents of previous sessions. Professional in charge: physiotherapist with experience on CSP | N = 60, divided into: G3 = 30 (high CSI) M = 8, F = 22 Age: 40.13 ± 14.91 G4 = 30 (low CSI) M = 17, F = 13 Age: 42.10 ± 11.10 Three sessions in 2 weeks - First group session (max 6 people) with education based on Neck/Back school guidelines, used power point presentation (30–60 min), delivered a brochure to read at home. - Second online session with 3 videos and a final questionnaire. Topics for first and second session: course and mechanical causes of pain, anatomy and physiology of the musculoskeletal apparatus, ergonomics and exercises (omitted information on the nervous system). - Third individual session, 30 min of conversation one-by-one, with attention to the patient’s personal needs and discussion of the contents of previous sessions. Professional in charge: physiotherapist with experience on CSP | Pain Disability Index (PDI) Pain Catastrophizing Scale (PCS-13) Tampa Scale of Kinesiophobia (TSK-17) Revised Illness Perception Questionnaire (IPQ-r) Pain Vigilance Awareness Questionnaire (PVAQ) Baseline 2 weeks (post-education) | PDI EX1: 30.09 ± 2.70 ⟶ 27.65 ± 2.41 C3: 26.03 ± 2.16 ⟶ 28.53 ± 2.11 EX2:16.25 ± 2.16 ⟶ 16.58 ± 1.93 C4: 17.13 ± 2.36 ⟶ 16.93 ± 2.11 p < 0.001 PCS-13 (Rumination) EX1: 8.96 ± 0.79 ⟶ 7.21 ± 0.78 C3: 7.63 ± 0.70 ⟶ 6.67 ± 0.70 EX2: 4.89 ± 0.64 ⟶ 5.33 ± 0.64 C4: 5.37 ± 0.70 ⟶ 4.77 ± 0.70 p < 0.001 PCS-13 (Magnification) EX1: 3.75 ± 0.43 ⟶ 2.83 ± 0.43 C3: 3.23 ± 0.38 ⟶ 2.87 ± 0.39 EX2: 1.58 ± 0.35 ⟶ 2.36 ± 0.35 C4: 2.27 ± 0.38 ⟶ 1.93 ± 0.39 p < 0.001 PCS-13 (Helplessness) EX1: 9.63 ± 0.98 ⟶ 7.96 ± 0.99 C3: 8.73 ± 0.88 ⟶ 7.47 ± 0.88 EX2: 6.19 ± 0.80 ⟶ 5.92 ± 0.80 C4: 6.47 ± 0.88 ⟶ 5.87 ± 0.88 p < 0.001 PCS-13 (total score) EX1: 22.33 ± 1.93 ⟶ 18.00 ± 1.93 C3: 19.60 ± 1.73 ⟶ 17.00 ± 1.72 EX2: 12.37 ± 1.58 ⟶ 13.61 ± 1.57 C4: 14.10 ± 1.73 ⟶ 12.57 ± 1.72 p > 0.05 TSK-17 EX1: 37.00 ± 1.39 ⟶ 32.25 ± 1.43 C3: 37.97 ± 1.24 ⟶ 36.53 ± 1.28 EX2: 32.61 ± 1.13 ⟶ 20.03 ± 1.17 C4: 35.47 ± 1.24 ⟶ 34.93 ± 1.28 p < 0.001 IPQ-r (Acute/Chronic timeline) EX1: 24.63 ± 0.80 ⟶ 20.58 ± 0.93 C3: 23.13 ± 0.71 ⟶ 22.17 ± 0.83 EX2: 23.33 ± 0.65 ⟶ 19.47 ± 0.76 C4: 23.33 ± 0.71 ⟶ 21.00 ± 0.83 IPQ-r (Consequence) EX1: 19.50 ± 0.89 ⟶ 16.96 ± 0.84 C3: 18.00 ± 0.79 ⟶ 17.90 ± 0.75 EX2: 14.53 ± 0.72 ⟶ 12.94 ± 0.69 C4: 15.30 ± 0.79 ⟶ 15.00 ± 0.75 IPQ-r (Personal Control) EX1: 19.33 ± 0.83 ⟶ 22.50 ± 0.63 C3: 19.43 ± 0.74 ⟶ 21.87 ± 0.56 EX2: 20.75 ± 0.67 ⟶ 22.39 ± 0.51 C4: 22.27 ± 0.74 ⟶ 22.43 ± 0.56 IPQ-r (Treatment control) EX1: 16.42 ± 0.56 ⟶ 17.75 ± 0.45 C3: 16.63 ± 0.50 ⟶ 17.07 ± 0.40 EX2: 17.11 ± 0.46 ⟶ 18.03 ± 0.37 C4: 17.83 ± 0.50 ⟶ 18.30 ± 0.40 IPQ-r (Illness Coherence) EX1: 16.88 ± 0.50 ⟶ 18.17 ± 0.52 C3: 15.63 ± 0.45 ⟶ 16.30 ± 0.46 EX2: 17.17 ± 0.41 ⟶ 17.19 ± 0.42 C4: 17.27 ± 0.45 ⟶ 18.07 ± 0.46 IPQ-r (Timeline Cyclical) EX1: 12.83 ± 0.65 ⟶ 14.17 ± 0.67 C3: 12.53 ± 0.58 ⟶ 12.77 ± 0.60 EX2: 13.28 ± 0.53 ⟶ 14.42 ± 0.54 C4: 13.80 ± 0.58 ⟶ 13.13 ± 0.60 IPQ-r (Emotional representations) EX1: 17.21 ± 0.93 ⟶ 17.04 ± 0.95 C3: 15.67 ± 0.83 ⟶ 16.00 ± 0.85 EX2: 13.42 ± 0.76 ⟶ 14.19 ± 0.77 C4: 13.40 ± 0.83 ⟶ 13.93 ± 0.85 p < 0.001 PVAQ EX1: 40.88 ± 2.49 ⟶ 35.38 ± 2.50 C3: 36.10 ± 2.22 ⟶ 34.97 ± 2.23 EX2: 34.25 ± 2.03 ⟶ 32.61 ± 2.04 C4: 35.43 ± 2.22 ⟶ 32.60 ± 2.23 p > 0.05 |
| Meeus et al. [40], in 2010 RCT Belgium | Chronic Fatigue Syndrome (CFS) according to the criteria of: Centers for Disease Control and Prevention for CFS (1994) [51] N = 48 Age: 18–65 Patients recruited from the medical records available at the specialized university clinic in Brussels. | N = 24, M = 2, F = 22 Age: 38.3 ± 10.6 PNE: execution of an educational session based on the contents of the book “Explain Pain” with the help of images and examples. Topics retracted in another individual interactive session. | N = 24, M = 6, F = 18 Age: 42.3 ± 10.2 Education to self-management of ADL. Performing an educational session to promote a balance between rest and activity in patients, in order to avoid exacerbation of symptoms. | Pain Coping Inventory (PCI) Pain Catastrophizing Scale (PCS-13) Tampa Scale of Kinesiophobia (TSK-CFS) Pre-session (Baseline) Post-session | PCI (transforming) EX: 2.48 ± 0.71 ⟶ 2.30 ± 0.64 C: 2.23 ± 0.80 ⟶ 2.09 ± 0.62 p > 0.01 PCI (distraction) EX: 2.22 ± 0.54 ⟶ 2.32 ± 0.62 C: 2.51 ± 0.60 ⟶ 2.41 ± 0.52 p = 0.021 PCI (reducing demands) EX: 2.60 ± 0.59 ⟶ 2.29 ± 0.70 C: 2.71 ± 0.76 ⟶ 2.60 ± 0.85 p > 0.01 PCI (retreating) EX: 2.27 ± 0.80 ⟶ 2.21 ± 0.73 C: 2.53 ± 0.57 ⟶ 2.53 ± 0.57 p > 0.01 PCI (worrying) EX: 2.11 ± 0.41 ⟶ 1.85 ± 0.40 C: 2.09 ± 0.67 ⟶ 2.02 ± 0.67 p = 0.011 PCI (resting) EX: 2.41 ± 0.59 ⟶ 2.15 ± 0.59 C: 2.60 ± 0.64 ⟶ 2.56 ± 0.69 p > 0.01 PCS-13 (helplessness) EX: 8.54 ± 5.39 ⟶ 6.63 ± 4.70 C: 9.96 ± 6.77 ⟶ 9.29 ± 6.93 p > 0.01 PCS-13 (magnification) EX: 2.38 ± 1.93 ⟶ 1.67 ± 1.55 C: 4.00 ± 3.51 ⟶ 3.75 ± 4.19 p > 0.01 PCS-13 (ruminating) EX: 7.29 ± 3.86 ⟶ 5.71 ± 3.46 C: 7.83 ± 4.59 ⟶ 7.67 ± 4.91 p = 0.009 TSK-CFS EX: 39.17 ± 9.52 ⟶ 33.21 ± 6.58 C: 39.71 ± 7.15 ⟶ 37.42 ± 8.15 p > 0.05 |
| Orhan et al. [41], in 2021 RCT Belgium | CLBP > 3 months N = 29 Age: 18–65 Patients recruited at a private medical centre in Ghent (BE). | N = 15, M = 4, F = 11 Age: 55.0 (47.0–59.0) 2 educational sessions with PNE. approach developed during a study “Delphi modified”(Orhan et al., 2019). The same contents as the control group, but with adaptations based on the culture of the participants or gender. Topics: difference between chronic and acute pain, role of pain, genesis of pain, factors that promote central awareness and treatment strategies. use of verbal information, images, metaphors based on previous research and books including: “Explain Pain” (Butler and Moseley, 2003) and “Pijneducatie: Een Praktische Handleiding voor (Para) medici” (Van Wilgen e Nijs, 2010). Professional in charge: first author instructed by 2 physiotherapists experts in PNE. | N = 14, M = 4 F = 10 Age: 55.0 (45.0–60.2) Two educational sessions with standard PNE (same as the intervention group). Standard content translated into Turkish by 2 independent native Turkish-speaking translators. Topics: difference between chronic and acute pain, role of pain, genesis of pain, factors that promote central awareness and treatment strategies. use of verbal information, images, metaphors based on previous research and books including: “Explain Pain” (Butler and Moseley, 2003) and “Pijneducatie: Een Praktische Handleiding voor (Para) medici” (Van Wilgen e Nijs, 2010). Professional in charge: first author instructed by 2 physiotherapists experts in PNE. | Numerical Rating Scale (NRS) Roland Morris Disability Questionnaire (RMDQ) Pain Beliefs Questionnaire (PBQ) Pain Catastrophizing Scale (PCS-13) Tampa Scale of Kinesiophobia (TSK-17) Baseline 1 weeks 4 weeks | NRS EX: 6.50 ± 1.80 ⟶ 5.80 ± 2.07 ⟶ 5.86 ± 2.35 C: 6.85 ± 2.21 ⟶ 5.85 ± 2.24 ⟶ 6.00 ± 2.48 p > 0.05 RMDQ EX: 16.66 ± 4.32 ⟶ 15.40 ± 4.82 ⟶ 15.60 ± 6.12 C: 16.21 ± 4.62 ⟶ 14.42 ± 5.98 ⟶ 13.07 ± 5.91 p > 0.05 PBQ (organic score) EX: 4.23 ± 0.93 ⟶ 3.67 ± 0.99 ⟶ 3.87 ± 0.65 C: 4.02 ± 0.75 ⟶ 3.64 ± 0.70 ⟶ 3.50 ± 0.92 p > 0.05 PBQ (psychological score) EX: 4.10 ± 1.22 ⟶ 4.86 ± 1.22 ⟶ 4.36 ± 1.14 C: 4.35 ± 0.93 ⟶ 4.51 ± 1.04 ⟶ 4.12 ± 1.07 p > 0.05 PCS-13 EX: 29.40 ± 10.68 ⟶ 25.93 ± 11.21 ⟶ 24.80 ± 11.21 C: 24.14 ± 10.86 ⟶ 19.35 ± 10.77 ⟶ 19.00 ± 11.08 p > 0.05 TSK-17 EX: 45.33 ± 5.17 ⟶ 42.73 ± 5.37 ⟶ 43.26 ± 6.06 C: 43.64 ± 3.65 ⟶ 41.71 ± 3.45 ⟶ 40.50 ± 3.87 p > 0.05 |
| Pires et al. [42], in 2015 RCT Portugal | CLBP > 3 months N = 62 Age: 18–65 Patients recruited from the waiting list of a Portuguese clinic | N = 30, M = 10, F = 20 Age: 50.9 ± 6.2 1. PNE: 2 group session of 90 min each, for educational sessions were used as help metaphors and images shown before the program of the exercise. Topics: neurophysiology of pain, central sensitization, psychosocial factors 2. Aquatic exercise program (same as control) | N = 32, M = 12, F = 20 Age: 51.0 ± 6.3 1. Aquatic exercise program: Group exercises, 2 sessions per week for 6 weeks, each lasting 30–50 min with warm-up, activity, cooling-off. | Visual Analogue Scale (VAS) Quebec Back Pain Disability Scale (QBPDS-PT) Tampa Scale of Kinesiophobia (TSK-13) Baseline 6 weeks 3 months | VAS EX: 43.4 ± 23 ⟶ 20.6 ± 19 ⟶ 18.0 ± 19 C: 42.4 ± 21.2 ⟶ 27.6 ± 17.2 ⟶ 35.8 ± 28 p = 0.14 6 weeks p < 0.05 3 months QBPDS-PT EX: 32.3 ± 14 ⟶ 21.2 ± 15.8 ⟶ 19.2 ± 14.8 C: 28.1 ± 13.6 ⟶ 20.4 ± 12.3 ⟶ 25.9 ± 15.7 p > 0.05 TSK-13 EX: 28.6 ± 6 ⟶ 25.2 ± 4.7 ⟶ 23.2 ± 6.3 C: 29.1 ± 5.6 ⟶ 27.5 ± 6.2 ⟶ 26.5 ± 7.9 p > 0.05 |
| Rabiei et al. [43], in 2021 RCT Iran | CLBP > 3 months N = 73 Age: 30–60 Patients recruited by physiotherapists through leaflets exposed in rehab clinics. | N = 37, M = 16, F = 21 Age: 42.46 ± 9.7 1. PNE: 3 educational sessions, each lasting 30–60 min. Frontal sessions, with the help of diagrams and drawings Professional in charge: Persian native physiotherapist, trained in PNE and MCE programs. 2. MCE, 2 sessions a week for 8 weeks. In the first session, each patient was assessed by the physiotherapist. The training included: sensory-motor control training, proprioception and recruitment (diaphragm, multifidus, transverse abdomen, pelvic floor) in progression. Initially proposed static exercises, then dynamic exercises related to functional activities. Objective: coordination, posture, stability of the spine, encouraging the resumption of activities feared by the patient in daily life. Professional in charge: Persian native physiotherapist, trained in PNE and MCE programs. | N = 36, M = 18, F = 18 Age: 44.19 ± 8.79 1. Group-based exercise (GE) program. Proposed sessions 2 times a week for 8 weeks, each session lasting 60 min (10 min group warm-up, 45 min muscle strengthening exercises, 5 min light exercises). For each exercise: 3 series of 10 repetitions each. The program was modified in relation to patient tolerance. Professional in charge: physiotherapist not involved in the intervention group | Visual Analogue Scale (VAS) Roland Morris Disability Questionnaire (RMDQ) Fear Avoidance Beliefs Questionnaire (FABQ) Pain Self Efficacy Questionnaire (PSEQ) Baseline 8 weeks | VAS EX: 6.45 ± 1.21 ⟶ 3.79 ± 1.02 C: 6.36 ± 1.14 ⟶ 4.91 ± 1.67 p = 0.041 RMDQ EX: 14.6 ± 1.55 ⟶ 7.94 ± 2.17 C: 15.0 ± 2.14 ⟶ 9.50 ± 3.25 p = 0.021 FABQ-W EX: 24.2 ± 10.4 ⟶ 11.5 ± 6.41 C: 21.6 ± 8.02 ⟶ 14.9 ± 6.43 p = 0.819 FABQ-PA EX: 17.2 ± 4.25 ⟶ 8.24 ± 3.72 C: 15.7 ± 5.17 ⟶ 10.2 ± 4.15 p = 0.803 PSEQ EX: 26.6 ± 9.53 ⟶ 43.9 ± 11.6 C: 29.5 ± 10.9 ⟶ 38.9 ± 12.0 p = 0.661 |
| Ryan et al. [44], in 2010 RCT UK | CLBP > 3 months N = 38 Age: 18–65 Patients recruited from 5 different physical therapy departments | N = 18, M = 7, F = 11 Age: 45.2 ± 9.5 1.PNE: a single educational session of 2 h and 30 min on the biology of pain. oral session, with the help of diagrams, drawings and delivery of the book: “The back book” | N = 20, M = 6, F = 14 Age: 45.2 ± 11.9 1.PNE (same as intervention group) 2. Circuit aerobics exercises associated with core stability exercises (“Back to fitness exercise classes”). each session divided into: 10 min warm-up, 20–30 min aerobic phase, 10–15 min cool-down). 6 exercise classes, one class per week for 6 weeks. | Roland Morris Disability Questionnaire (RMDQ) Numerical Rating Scale (NRS) Tampa Scale of Kinesiophobia (TSK-13) Pain Self Efficacy Questionnaire (PSEQ) Baseline 8 weeks 3 months | RMDQ EX: 10.8 ± 5.2 ⟶ 3.3 ± 3.0 ⟶ 4.3 ± 4.2 C: 9.4 ± 4.2 ⟶ 5.6 ± 3.9 ⟶ 6.4 ± 5.1 p > 0.05 NRS EX: 39.3 ± 26.2 ⟶ 8.4 ± 7.5 ⟶ 22.6 ± 30.8 C: 28.1 ± 20.4 ⟶ 23.9 ± 23.3 ⟶ 19.1 ± 18.9 p = 0.025 8 weeks p > 0.05 3 months TSK-13 EX: 28.4 ± 8.2 ⟶ 21.3 ± 6.5 ⟶ 23.7 ± 6.6 C: 25.8 ± 7.4 ⟶ 21.9 ± 8.2 ⟶ 21.5 ± 7.5 p > 0.05 PSEQ EX: 41.9 ± 12.5 ⟶ 55.1 ± 4.7 ⟶ 49.5 ± 9.8 C: 50.0 ± 11.4 ⟶ 48.8 ± 12.2 ⟶ 49.5 ± 13.1 p = 0.024 8 weeks p > 0.05 3 months |
| Saracoglu et al. [45], in 2020 RCT Turkey | CLBP > 6 months N = 69 Age: 18–65 Patients recruited by the physical therapy department of Kutahya University Hospital | The participants were divided into 3 groups. Group 1 ⟶ N = 20, M = 9, F = 12 1. PNE: according to the method recommended by Louw, Nijs and Puentedura (2017). 4 individual educational sessions, one per week, lasting about 40–45 min, after the manual therapy session. Topics: peripheral pain, allodynia, central and peripheral sensitization, hyperalgesia, neuroplasticity, stress, fear, catastrophization, immunological response, how to deal with pain, role of physical exercise and manual therapy. In support, used tools such as: metaphors, presentations, images. Professional in charge: physiotherapist trained at the International Spine and Pain Institute 2. Manual Therapy: same group 2 modes. 3. Home exercise program: same group 2 and group 3 modes. | Group 2 ⟶ N = 19, M = 11, F = 10 Group 3 ⟶ N = 18, M = 10, F = 10 Two control groups: Group 2: 1. Manual therapy: personalized treatment, 2 sessions per week, for 4 weeks, each lasting 30 min. Use different techniques with variable speed, range, direction of force application and patient position. Professional in charge: same experienced physiotherapist of PNE, with University Master and 10 years of experience in manual therapy. 2. Home exercise program, developed by Koumantakis, Watson and Oldham (2005). Objectives: to increase strength and flexibility of the trunk muscles, buttocks, quadriceps and ischiocrural. the program includes: stretching, heating, reinforcement. indication: 10 repetitions, 3 times a day for 4 weeks. Professional in charge: physiotherapist. Group 3: only home exercise program, with the same group 1 and group 2 modes. | Numerical Pain Rating Scale (NPRS) Oswestry Disability Index (ODI) Tampa Scale of Kinesiophobia (TSK-17) Baseline 4 weeks 12 weeks | NPRS G1: 7.29 ± 1.41 ⟶ 3.05 ± 1.50 ⟶ 2.09 ± 1.64 G2: 7.58 ± 1.47 ⟶ 4.42 ± 1.78 ⟶ 4.52 ± 1.84 C: 7.32 ± 1.48 ⟶ 5.89 ± 2.03 ⟶ 5.47 ± 1.95 p (G1 vs. G2) = 0.01 p (G1 vs. G3) < 0.001 ODI G1: 34.45 ± 7.39 ⟶ 22.80 ± 6.77 ⟶ 19.90 ± 5.72 G2: 32.00 ± 6.87 ⟶ 25.00 ± 7.88 ⟶ 25.89 ± 7.37 C: 34.74 ± 8.55 ⟶ 31.77 ± 9.27 ⟶ 32.33 ± 8.49 p (G1 vs. G2) = 0.67 p (G1 vs. G3) < 0.001 TSK-17 G1: 44.35 ± 4.30 ⟶ 35.55 ± 5.75 ⟶ 35.19 ± 3.99 G2: 45.10 ± 4.45 ⟶ 41.63 ± 5.23 ⟶ 42.21 ± 5.04 C: 45.55 ± 4.10 ⟶ 44.94 ± 4.70 ⟶ 44.88 ± 5.10 p (G1 vs. G2) < 0.001 p (G1 vs. G3) < 0.001 |
| Serrat et al. [46], in 2020 RCT Spain | Fibromyalgia according to American College of Reumatology criteria (ACR) [38] N = 169 Age: ≥18 Patients recruited at the university hospital in Val d’Hebron (UHVH) by a specialized physiotherapist. | N = 84, M = 2, F = 82 Age: 54.12 ± 8.62 1. NAT-FM: 2-h session per week for 12 weeks. Outdoor sessions, different approaches were used: - PNE: (20 min) reconceptualization of pain, anatomy and neurophysiology of the nervous system, modulation of pain, influencing factors, types of pain, neuromatrix theory, neuroplasticity. - Therapeutic exercise and activities in nature: (40 min) hiking, yoga, nordic walking, photography, Shirin yoku. - Cognitive behavioral therapy (CBT): (20 min) - Mindfulness Training (MT): (20 min) 2. TAU: same as control group Professional in charge: physiotherapist, sports psychologist and technician of the CSSU of the Val d’Hebron university hospital, prepared to conduct this treatment, supported by a patient with fibromyalgia who brought his testimony in groups to motivate participants in compliance, after successfully completing the program FIBROWALK | N = 85, M = 0, F = 85 Age: 53.15 ± 9.06 1.TAU: 2-h session per week for 12 weeks. Includes: basic disease education, aerobic exercises, personalized pharmacological treatment. integration of the FIBROWALK protocol. | Fibromyalgia Impact Questionnaire (FIQ) Visual Analogue Scale (VAS) Hospital Anxiety and Depression Scale (HADS) Short Form Health Survey 36 (SF-36) Rosenberg Self-Esteem Scale (RSES) Tampa Scale of Kinesiophobia (TSK-11) Pain Catastrophizing Scale (PCS-13) Baseline 6 weeks 12 weeks | FIQR EX: 73.07 ± 13.79 ⟶ 58.78 ± 18.70 ⟶ 50.69 ± 18.05 C: 73.21 ± 14.72 ⟶ 69.68 ± 13.36 ⟶ 69.18 ± 17.88 p < 0.001 VAS pain EX: 7.74 ± 1.52 ⟶ 6.78 ± 1.99 ⟶ 5.60 ± 1.98 C: 7.80 ± 1.61 ⟶ 7.52 ± 1.59 ⟶ 7.47 ± 1.79 p = 0.003 6 weeks p < 0.001 12 weeks VAS fatigue EX: 7.61 ± 1.89 ⟶ 5.98 ± 2.10 ⟶ 5.58 ± 2.00 C: 7.76 ± 1.91 ⟶ 7.32 ± 2.09 ⟶ 7.08 ± 2.34 p = 0.002 6 weeks p < 0.001 12 weeks HADS-A EX: 13.95 ± 3.80 ⟶ 11.03 ± 4.25 ⟶ 10.16 ± 4.19 C: 13.13 ± 4.22 ⟶ 12.35 ± 4.07 ⟶ 12.68 ± 4.63 p < 0.001 HADS-D EX: 11.27 ± 3.71 ⟶ 9.66 ± 4.47 ⟶ 8.18 ± 4.42 C: 11.49 ± 4.64 ⟶ 11.22 ± 5.02 ⟶ 11.67 ± 5.18 p = 0.027 6 weeks p < 0.001 12 weeks SF-36 EX: 27.03 ± 18.85 ⟶ 35.09 ± 20.47 ⟶ 43.42 ± 20.92 C: 26.04 ± 18.11 ⟶ 28.24 ± 17.38 ⟶ 25.07 ± 15.86 p = 0.017 6 weeks p < 0.001 12 weeks RSES EX: 16.03 ± 3.36 ⟶ 16.60 ± 2.70 ⟶ 16.53 ± 2.25 C: 15.41 ± 3.57 ⟶ 15.48 ± 2.57 ⟶ 16.25 ± 3.45 p > 0.05 TSK-11 EX: 29.23 ± 7.40 ⟶ 21.36 ± 6.83 ⟶ 17.95 ± 4.97 C: 29.92 ± 7.58 ⟶ 25.59 ± 6.46 ⟶ 28 ± 7.44 p < 0.001 PCS-13 EX: 27.04 ± 11.33 ⟶ 17.83 ± 9.56 ⟶ 13.53 ± 8.87 C: 27.72 ± 12.65 ⟶ 26.72 ± 13.25 ⟶ 27.49 ± 13.35 p < 0.001 |
| Téllez-Garcia et al. [47], in 2015 RCT Spain | Non-specific CLBP ≥ 3 months N= 12 Age: 18–65 Patients with non-specific LBP recruited had gone to the doctor to request physiotherapy sessions | N = 6, M = 2, F = 4 Age: 36 ± 5 1. Dry needling (same as control group) 2. PNE: 2 individual educational sessions, one to one lasting 30 min each, once a week immediately after the 2° and 3° sessions of Dry needling. Topics: neurophysiology of pain, beliefs about pain. Used power point material based on the book “Explain Pain” by Butler and Moseley (2003) and other material to read at home. | N = 6, M = 2, F = 4 Age: 37 ± 13 Three dry needling sessions, once a week. run on active trigger point (gluteus medius, quadratus lumborum) with fast-in and fast-out techniques by Hong. Professional in charge: clinical expert | Numerical Pain Rating Scale (NPRS) Oswestry Disability Index (ODI) - Roland Morris Disability Questionnaire (RMDQ) Tampa Scale of Kinesiophobia (TSK-17) Baseline 4 weeks | NPRS EX: 5.0 ± 2.1 ⟶ 0.8 ± 1.0 C: 4.8 ± 3.1 ⟶ 1.2 ± 1.1 p > 0.05 ODI EX: 24.2 ± 9.7 ⟶ 4.7 ± 3.2 C: 30.0 ± 14.8 ⟶ 6.0 ± 5.1 p > 0.05 RMDQ EX: 10.3 ± 3.4 ⟶ 1.0 ± 1.1 C: 8.3 ± 1.2 ⟶ 2.2 ± 2.2 ± 0.8 p > 0.05 TSK-17 EX: 41.5 ± 6.2 ⟶ 23.8 ± 2.9 C: 43.3 ± 5.9 ⟶ 38.3 ± 5.1 p = 0.008 MCID > 8 |
| Van Ittersum et al. [48], in 2014 RCT Belgium | Fibromyalgia according to American College of Reumatology criteria (ACR) [38] N = 105 Age: 18–65 Patients recruited from two centers specialized in chronic pain and cfs, in Belgium | N = 53, M = 6%, F = 94% Age: 47.6 ± 9.1 For both groups, a period of 6 weeks was considered for reading, learning and applying the contents of the brochures. To the intervention group proposed education through PNE with delivery of a 15 page brochure containing images and written information about: neurophysiology of pain, anatomy and physiology of the nervous system, based on the book “Explain Pain” by Butler and Moseley (2003). After 2 weeks, the physiotherapist called the patients to make sure they understood the contents of the brochure and answered any questions. | N = 52, M = 8%, F = 92% Age: 45.8 ± 9.8 To the control group, proposed a brochure of 15 pages containing relaxation exercises and instructions to perform them independently at home. Explanation of the relationship between pain and physical and psychological factors (Loeser model). Patients could choose one or more exercises on the 3 techniques proposed (Jacobson’s progressive muscle relaxation method, visualization method derived from meditation techniques, autogenous training described by Schultz). After 2 weeks, the physiotherapist called the patients same as intervention group. | Fibromyalgia Impact Questionnaire (FIQ) Revised Illlness Perception Questionnaire (IPQ-R_FM) Pain Catastrophizing Scale (PCS) Baseline 6 weeks 6 months | FIQ EX: 70.0 ± 14.8 ⟶ 69.3 ± 15.4 ⟶ 67.4 ± 15.5 C: 66.6 ± 14.8 ⟶ 65.1 ± 15.2 ⟶ 67.1 ± 15.1 p > 0.05 IPQ-R FM: IPQ-r (Acute/Chronic timeline) EX: 17.4 ± 2.8 ⟶ 18.0 ± 3.0 ⟶ 21.0 ± 5.0 C: 17.6 ± 2.3 ⟶ 18.5 ± 3.0 ⟶ 23.4 ± 4.5 IPQ-r (Timeline Cyclical) EX: 14.7 ± 3.9 ⟶ 14.3v3.7 ⟶ 14.8 ± 3.3 C: 14.1 ± 3.4 ⟶ 14.7 ± 3.5 ⟶ 14.3 ± 3.3 IPQ-r (Consequence) EX: 20.3 ± 3.9 ⟶ 20.4 ± 3.6 ⟶ 22.2 ± 3.7 C: 20.4 ± 3.5 ⟶ 21.0 ± 3.4 ⟶ 23.4 ± 3.9 IPQ-r (Personal Control) EX: 16.0 ± 3.4 ⟶ 16.9 ± 3.3 ⟶ 16.4 ± 3.9 C: 16.8 ± 2.2 ⟶ 15.2 ± 2.6 ⟶ 17.7 ± 3.7 IPQ-r (Treatment control) EX: 15.4 ± 2.4 ⟶ 15.1 ± 2.4 ⟶ 14.8 ± 3.1 C: 15.3 ± 2.1 ⟶ 15.2 ± 2.6 ⟶ 14.9 ± 3.1 IPQ-r (Emotional representations) EX: 16.6 ± 4.6 ⟶ 16.5 ± 5.0 ⟶ 17.1 ± 5.2 C: 15.1 ± 4.3 ⟶ 15.0 ± 4.0 ⟶ 16.1 ± 4.7 IPQ-r (Illness Coherence) EX 15.6 ± 4.0 ⟶ 15.1 ± 3.9 ⟶ 15.7 ± 3.3: C: 15.8 ± 3.6 ⟶ 15.4 ± 3.7 ⟶ 15.4 ± 3.3 IPQ-r (Psychologica attribution) EX: 17.7 ± 5.3 ⟶ 18.1 ± 5.3 ⟶ 17.8 ± 5.3 C: 17.0 ± 5.8 ⟶ 18.2 ± 5.1 ⟶ 17.4 ± 5.7 IPQ-r (Risk factor attribution) EX: 14.6 ± 4.0 ⟶ 15.1 ± 4.0 ⟶ 14.9 ± 4.2 C: 14.2 ± 4.0 ⟶ 14.9 ± 4.3 ⟶ 15.0 ± 4.1 IPQ-r (Immune attribution) EX: 8.7 ± 2.1 ⟶ 8.7 ± 1.9 ⟶ 8.7 ± 2.2 C: 8.5 ± 2.8 ⟶ 8.5 ± 2.6 ⟶ 8.8 ± 2.2 IPQ-r (Accident/chance) EX: 5.5 ± 1.8 ⟶ 5.3 ± 1.7 ⟶ 5.5 ± 1.6 C: 5.2 ± 2.0 ⟶ 5.3 ± 2.2 ⟶ 5.7 ± 2.0 IPQ-r (FM-specific attribution) EX: 23.4 ± 5.0 ⟶ 23.9 ± 4.5 ⟶ 23.5 ± 4.3 C: 23.5 ± 4.5 ⟶ 23.8 ± 4.5 ⟶ 23.6 ± 4.9 p > 0.05 PCS EX: 24.0 ± 11.9 ⟶ 24.1 ± 12.8 ⟶ 24.3 ± 13.4 C: 23.0 ± 12.1 ⟶ 21.7 ± 12.0 ⟶ 22.3 ± 12.8 p > 0.05 |
| Van Oosterwjck et al. [49], in 2013 RCT Belgium | Fibromyalgia according to American College of Reumatology criteria (ACR) [38] N = 30 Age: 18–65 Patients recruited from private practices of internal medicine. | N = 15, M = 3, F = 12 Age: 45.8 ± 9.5 2 educational sessions of PNE lasting 30 min once a week, were proposed to the intervention group. The 1° oral session, the second by telephone call. Topics: neurophysiology of pain, nervous system plasticity, central sensitization, with reference to the book “Explain Pain” by Butler and Moseley (2003). As a support use power-point presentations, images, metaphors, examples. At the end of the first session, a booklet is given to read at home as a reinforcement. | N = 15, M = 1, F = 14 Age: 45.9 ± 11.5 2 individual educational sessions of pain self-management, lasting 30 min once a week, were proposed to the control group. The first oral session, the second by telephone call. Topics: self-management techniques for pain and symptoms. At the end of the 1° session, a booklet is given to read at home as a reinforcement. | Fibromyalgia Impact Questionnaire (FIQ) Short Form Health Survey 36 (SF-36) Pain Coping Inventory (PCI) Pain Catastrophizing Scale (PCS) Pain Vigilance and Awareness (PVAQ) Tampa Scale of Kinesiophobia (TSK-17) Baseline 2 weeks 3 months | FIQ EX: 38.7 ± 10.7 ⟶ 34.9 ± 10.1 ⟶ 36.5 ± 9.9 C: 59.4 ± 12.9 ⟶ 58.7 ± 15.4 ⟶ 60.1 ± 10.5 p > 0.05 SF-36 “physical functioning” EX: 47.7 ± 22.7 ⟶ 51.0 ± 21.6 ⟶ 53.7 ± 21.8 C: 49.7 ± 17.9 ⟶ 45.7 ± 17.1 ⟶ 45.3 ± 12.3 p = 0.046 SF-36 “role limitations due to physical pain” EX: 18.3 ± 34.7 ⟶ 25.0 ± 35.4 ⟶ 28.3 ± 35.2 C: 13.3 ± 22.9 ⟶ 5.0 ± 10.4 ⟶ 15.0 ± 26.4 p > 0.05 SF-36 “bodily pain” EX: 37.1 ± 19.2 ⟶ 45.8 ± 25.8 ⟶ 42.5 ± 19.9 C: 40.3 ± 15.8 ⟶ 49.2 ± 20.2 ⟶ 52.4 ± 21.5 p > 0.05 SF-36 “general health perceptions” EX: 24.7 ± 10.6 ⟶ 32.8 ± 15.5 ⟶ 37.7 ± 15.5 C: 31.47 ± 12.8 ⟶ 33.3 ± 14.0 ⟶ 28.6 ± 12.8 p < 0.001 SF-36 “vitality” EX: 36.3 ± 17.8 ⟶ 35.7 ± 18.5 ⟶ 40.0 ± 21.0 C: 42.2 ± 14.3 ⟶ 38.5 ± 13.1 ⟶ 35.3 ± 13.7 p = 0.047 SF-36 “social functioning” EX: 63.1 ± 21.5 ⟶ 63.8 ± 27.0 ⟶ 58.1 ± 27.4 C: 48.4 ± 17.2 ⟶ 54.9 ± 20.2 ⟶ 61.2 ± 15.9 p > 0.05 SF-36 “role limitations due to emotional problems” EX: 71.1 ± 45.2 ⟶ 60.5 ± 43.1 ⟶ 59.9 ± 47.5 C: 42.2 ± 14.3 ⟶ 38.5 ± 13.1 ⟶ 35.3 ± 13.7 p > 0.05 SF-36 “mental health” EX: 60.8 ± 17.3 ⟶ 61.9 ± 22.4 ⟶ 66.7 ± 17.5 C: 62.0 ± 19.5 ⟶ 60.1 ± 20.8 ⟶ 48.5 ± 18.3 p < 0.001 PCI “transformation” EX: 2.1 ± 0.5 ⟶ 1.8 ± 0.6 ⟶ 1.9 ± 0.6 C: 1.7 ± 0.6 ⟶ 1.9 ± 0.7 ⟶ 1.9 ± 0.7 p > 0.05 PCI “distraction” EX: 2.2 ± 0.6 ⟶ 2.1 ± 0.8 ⟶ 2.1 ± 0.8 C: 2.1 ± 0.6 ⟶ 1.9 ± 0.6 ⟶ 2.0 ± 0.7 p > 0.05 PCI “reducing demands” EX: 2.2 ± 0.6 ⟶ 2.3 ± 0.8 ⟶ 2.2 ± 0.9 C: 2.0 ± 0.8 ⟶ 2.0 ± 0.9 ⟶ 2.1 ± 0.8 p > 0.05 PCI “worrying” EX: 1.7 ± 0.6 ⟶ 1.5 ± 0.5 ⟶ 1.5 ± 0.5 C: 1.7 ± 0.6 ⟶ 1.7 ± 0.7 ⟶ 1.6 ± 0.5 p > 0.05 PCI “retreating” EX: 1.7 ± 0.7 ⟶ 1.6 ± 0.6 ⟶ 1.7 ± 0.6 C: 1.9 ± 0.6 ⟶ 1.9 ± 0.7 ⟶ 1.8 ± 0.6 p > 0.05 PCI “resting” EX: 2.1 ± 0.4 ⟶ 1.9 ± 0.6 ⟶ 2.0 ± 0.8 C: 1.9 ± 0.7 ⟶ 1.9 ± 0.7 ⟶ 2.1 ± 0.6 p > 0.05 PCS “helplessness” EX: 9.5 ± 5.3 ⟶ 6.7 ± 6.0 ⟶ 6.7 ± 5.8 C: 11.1 ± 5.8 ⟶ 10.5 ± 5.6 ⟶ 9.6 ± 5.5 p > 0.05 PCS “magnification” EX: 2.8 ± 2.4 ⟶ 2.2 ± 2.5 ⟶ 1.7 ± 2.1 C: 3.0 ± 2.5 ⟶ 3.2 ± 2.1 ⟶ 3.3 ± 2.7 p > 0.05 PCS “rumination” EX: 7.1 ± 5.0 ⟶ 6.1 ± 3.8 ⟶ 5.1 ± 4.2 C: 7.7 ± 2.7 ⟶ 7.5 ± 3.3 ⟶ 7.5 ± 4.0 p > 0.05 PCS total EX: 19.5 ± 11.8 ⟶ 14.9 ± 11.6 ⟶ 13.3 ± 11.6 C: 21.9 ± 9.9 ⟶ 20.5 ± 10.2 ⟶ 20.4 ± 12.3 p > 0.05 PVAQ EX: 35.3 ± 14.5 ⟶ 34.4 ± 11.7 ⟶ 32.2 ± 13.7 C: 39.7 ± 12.6 ⟶ 42.6 ± 17.1 ⟶ 40.3 ± 14.4 p > 0.05 TSK-17 EX: 38.7 ± 10.7 ⟶ 34.9 ± 10.1 ⟶ 36.5 ± 9.9 C: 40.7 ± 8.4 ⟶ 39.8 ± 7.1 ⟶ 39.9 ± 8.2 p > 0.05 |
| Study | Drop-Outs | Lost to Follow-Up | ||||
|---|---|---|---|---|---|---|
| Experimental Group | Control Group | Experimental Group | Control Group | |||
| Barrenengoa-Cuadra et al. [35], in 2021 | 0 | 1 at baseline | 2 at 12 months | 2 at 12 months | ||
| Bodes et al. [36], in 2018 | 0 | 0 | 0 | 0 | ||
| Gül et al. [37], in 2021 | 0 | 0 | 0 | 0 | ||
| Kohns et al. [38], in 2020 | 0 | 0 | 10 at 10 months | 6 at 10 months | ||
| Malfliet et al. [39], in 2018 | 0 | 0 | 5 at 2 weeks | 4 at 2 weeks | ||
| Meeus et al. [40], in 2010 | 2 at 30 min | 0 | 0 | 0 | ||
| Orhan et al. [41], in 2021 | 4 at 1 week | 4 at 1 week | 0 | 0 | ||
| Pires et al. [42], in 2015 | 1 at 6 weeks | 5 at 6 weeks | 0 | 1 at 3 months | ||
| Rabiei et al. [43], in 2021 | 3 | 4 | 0 | 0 | ||
| Ryan et al. [44], in 2010 | 2 at 8 weeks | 2 at 8 weeks | 3 at 3 months | 4 at 3 months | ||
| Saracoglu et al. [45], in 2020 | 0 | 0 | 3 at 12 weeks | 4 at 12 weeks | 5 at 12 weeks | |
| Serrat et al. [46], in 2020 | 0 | 0 | 10 at 12 weeks | 0 | ||
| Téllez-Garcia et al. [47], in 2015 | 0 | 0 | 0 | 0 | ||
| Van Ittersum et al. [48], in 2014 | 32 at 6 weeks of follow-up | 14 at 6 months of follow-up | ||||
| Van Oosterwjck et al. [49], in 2013 | 0 | 0 | 3 at 3 months | 1 at 3 months | ||
| Outcome Measures | Study in Which Outcome Measures Have Been Addressed |
|---|---|
| BPI—Brief Pain Inventory | Barrenengoa-Cuadra et al. (2021) [35], Kohns et al. (2020) [38] |
| FABQ—Fear Avoidance Beliefs Questionnaire | Rabiei et al. (2021) [43] |
| FIQ—Fibromyalgia Impact Questionnaire | Barrenengoa-Cuadra et al. (2021) [35], Van Ittersum et al. (2014) [48], Van Oosterwjck et al. (2013) [49] |
| FIQR—Fibromyalgia Impact Questionnaire | Serrat et al. (2020) [46] |
| HADS—Hospital Anxiety and Depression Scale | Barrenengoa-Cuadra et al. (2021) [35], Serrat et al. (2020) [46] |
| HAQ—Health Assessment Questionnaire | Barrenengoa-Cuadra et al. (2021) [35] |
| IPQ–r Illness Perception Questionnaire | Malfliet et al. (2018) [39] |
| IPQ-R FM—Revised Illness Perception Questionnaire | Van Ittersum et al. (2014) [48] |
| NPRS—Numerical Pain Rating Scale | Bodes et al. (2018) [36], Saracoglu et al. (2020) [45], Téllez-Garcia et al. (2015) [47] |
| NRS—Numerical Rating Scale | Orhan et al. (2021) [41], Ryan et al. (2010) [44] |
| ODI—Oswestry Disability Index | Saracoglu et al. (2020) [45], Téllez-Garcia et al. (2015) [47] |
| PBQ—Personality Belief Questionnaire | Orhan et al. (2021) [41] |
| PCI—Pain Coping Inventory | Meeus et al. (2010) [40], Van Oosterwjck et al. (2013) [49] |
| PCS—Pain Catastrophizing Scale | Barrenengoa-Cuadra et al. (2021) [35], Bodes et al. (2018) [36], Kohns et al. (2020) [38], Malfliet et al. (2018) [39], Meeus et al. (2010) [40], Orhan et al. (2021) [41], Serrat et al. (2020) [46], Van Ittersum et al. (2014) [48], Van Oosterwjck et al. (2013) [49] |
| PDI—Pain Disability Index | Malfliet et al. (2018) [39] |
| PROMIS—Patient-Reported Outcomes Measurement Information System | Kohns et al. (2020) [38] |
| PSEQ—Pain Self-Efficacy Questionnaire | Rabiei et al. (2021) [43], Ryan et al. (2010) [44] |
| PSOCQ—Pain Stages of Change Questionnaire | Kohns et al. (2020) [38] |
| PVAQ—Pain Vigilance and Awareness Questionnaire | Malfliet et al. (2018) [39], Van Oosterwjck et al. (2013) [36] |
| QBPDS-PT—Quebec Back Pain Disability Scale | Pires et al. (2015) [42] |
| RMDQ Roland-Morris Disability Questionnaire | Bodes et al. (2018) [36], Gül et al. (2021) [37], Orhan et al. (2021) [41]; Rabiei et al. (2021) [43], Ryan et al. (2010) [44], Téllez-Garcia et al. (2015) [47] |
| RSES—Rosenberg Self-Esteem Scale | Serrat et al. (2020) [46] |
| SF-36—Short Form Health Survey | Serrat et al. (2020) [46], Van Oosterwjck et al. (2013) [49] |
| SWLS—Satisfaction With Life Scale | Kohns et al. (2020) [38] |
| TSK/TSK-CFS—Tampa Scale of Kinesiophobia | Bodes et al. (2018) [36], Gül et al. (2021) [37], Kohns et al. (2020) [38], Malfliet et al. (2018) [39], Meeus et al. (2010) [40], Orhan et al. (2021) [41], Pires et al. (2015) [42], Ryan et al. (2010) [44], Saracoglu et al. (2020) [45], Serrat et al. (2020) [46], Téllez-Garcia et al. (2015) [47], Van Oosterwjck et al. (2013) [49] |
| VAS—Visual Analogue Scale | Gül et al. (2021) [37], Pires et al. (2015) [42], Rabiei et al. (2021) [43], Serrat et al. (2020) [46] |
| Random Sequence Generation (Selection Bias) | Allocation Concealment (Selection Bias) | Blinding of Participants and Personnel (Performance Bias) | Blinding of Outcome Data (Attrition Bias) | Incomplete Outcome Data (Attrition Bias) | Selective Reporting (Reporting Bias) | Other Bias | |
|---|---|---|---|---|---|---|---|
| Barrenengoa-Cuadra et al. [35], in 2021 | LOW RISK | LOW RISK | HIGH RISK | HIGH RISK | LOW RISK | HIGH RISK | LOW RISK |
| Bodes et al. [36], in 2018 | LOW RISK | LOW RISK | HIGH RISK | HIGH RISK | LOW RISK | HIGH RISK | LOW RISK |
| Gül et al. [37], in 2021 | LOW RISK | UNCLEAR RISK | HIGH RISK | HIGH RISK | UNCLEAR RISK | UNCLEAR RISK | UNCLEAR RISK |
| Kohns et al. [38], in 2020 | LOW RISK | LOW RISK | HIGH RISK | UNCLEAR RISK | LOW RISK | LOW RISK | UNCLEAR RISK |
| Malfliet et al. [39], in 2018 | LOW RISK | LOW RISK | HIGH RISK | LOW RISK | UNCLEAR RISK | LOW RISK | UNCLEAR RISK |
| Meeus et al. [40], in 2010 | LOW RISK | LOW RISK | HIGH RISK | LOW RISK | LOW RISK | LOW RISK | UNCLEAR RISK |
| Orhan et al. [41], in 2021 | LOW RISK | UNCLEAR RISK | HIGH RISK | UNCLEAR RISK | LOW RISK | LOW RISK | UNCLEAR RISK |
| Pires et al. [42], in 2015 | LOW RISK | LOW RISK | HIGH RISK | LOW RISK | LOW RISK | LOW RISK | UNCLEAR RISK |
| Rabiei et al. [43], in 2021 | LOW RISK | LOW RISK | HIGH RISK | LOW RISK | LOW RISK | LOW RISK | UNCLEAR RISK |
| Ryan et al. [44], in 2010 | LOW RISK | LOW RISK | HIGH RISK | HIGH RISK | LOW RISK | LOW RISK | HIGH RISK |
| Saracoglu et al. [45], in 2020 | LOW RISK | LOW RISK | HIGH RISK | LOW RISK | LOW RISK | LOW RISK | UNCLEAR RISK |
| Serrat et al. [46], in 2020 | LOW RISK | LOW RISK | HIGH RISK | UNCLEAR RISK | UNCLEAR RISK | LOW RISK | HIGH RISK |
| Téllez-Garcia et al. [47], in 2015 | LOW RISK | LOW RISK | HIGH RISK | LOW RISK | LOW RISK | LOW RISK | HIGH RISK |
| Van Ittersum et al. [48], in 2014 | LOW RISK | LOW RISK | HIGH RISK | LOW RISK | LOW RISK | LOW RISK | UNCLEAR RISK |
| Van Oosterwjck et al. [49], in 2013 | LOW RISK | LOW RISK | HIGH RISK | HIGH RISK | LOW RISK | LOW RISK | UNCLEAR RISK |
| Agreement for Full-Text Selection | Evaluator 1 (B.L.) | Total | ||
|---|---|---|---|---|
| Positive Evaluation | Negative Evaluation | |||
| Evaluator 2 (V.B.) | Positive evaluation | 10 | 3 | 13 |
| Negative evaluation | 4 | 47 | 51 | |
| Total | 14 | 50 | 64 | |
| RCT | Experimental Intervention | ← | No Difference between Groups | Control Intervention | Outcome |
|---|---|---|---|---|---|
| Barrenengoa-Cuadra et al. [35], in 2021 FU: 1 month, 6 months, 12 months | PNE + Usual treatment | FIQ All follow-ups (p < 0.001) PCS BPI-Severity BPI-Interference HAQ HADS-A HADS-D All follow-ups (p < 0.05) | Usual treatment | FIQ BPI-SF HAQ HADS PCS-13 | |
| Bodes et al. [36], in 2018 FU: 1 month 3 months | PNE + Therapeutic exercise | NPRS 3 months (p < 0.001) TSK-11 1 month (p < 0.05) 3 months (p < 0.001) PCS-13 1 month (p < 0.05) 3 months (p < 0.001) RMDQ 3 months (p < 0.001) | Therapeutic exercise | NPRS RMDQ PCS-13 TSK-11 | |
| Gül et al. [37], in 2021 FU: 3 weeks | PNE + Physiotherapy | VAS 3 weeks (p > 0.05) TSK-17 3 weeks (p = 0.410) RMDQ 3 weeks (p > 0.05) | Physiotherapy | VAS TSK-17 RMDQ | |
| Kohns et al. [38], in 2020 FU: 1 month 10 months | PNE | BPI (severità) 1 month (p = 0.024) BPI (interferenza) 1 month (p = 0.031) PSCOQ 1 month (p < 0.05) | BPI (interference and severity) 10 months (p > 0.05) PROMIS Both follow-ups (p > 0.05) PSCOQ 10 months (p > 0.05) PCS-13 Both follow-ups (p > 0.05) TSK-11 Both follow-ups (p > 0.05) SWLS Both follow-up (p > 0.05) | Health Behavior Control | BPI PROMIS PSOCQ PCS-13 TSK-11 SWLS |
| Malfliet et al. [39], in 2018 FU: 2 weeks | PNE | PDI 2 weeks (p < 0.001) PCS 2 weeks (rumination, helplessness, magnification) (p < 0.001) TSK-17 2 weeks (p < 0.001) IPQr 2 weeks (from p < 0.001 to p = −0.01) | PVAQ 2 weeks (p > 0.05) | Neck/Back school education | PDI PCS TSK-17 IPQr PVAQ |
| Meeus et al. [40], in 2010 FU: Post-session | PNE | PCS (ruminating) Post-session (p = 0.009) PCI (distraction) Post-sessione (p = 0.021) PCI (worrying) Post-session (p = 0.011) | PCS (magnification and helplessness), Post-session (p > 0.01) PCI (transforming, reducing demands, retreating, resting) Post-session (p > 0.01) TSK-CFS Post-session (p > 0.01) | Pacing and self-management education | PCI PCS-13 TSK-CFS |
| Orhan et al. [41], in 2021 FU: 1 weeks 4 weeks | PNE “culture-sensitive” | Both follow-ups: NRS (p > 0.05) RMDQ (p > 0.05) PBQ (p > 0.05) PCS-13 (p > 0.05) TSK-17 (p > 0.05) | PNE standard | NRS RMDQ PBQ PCS TSK-17 | |
| Pires et al. [42], in 2015 FU: 6 weeks 3 months | PNE + Aquatic exercises | VAS 3 months (p < 0.05) | TSK-13 (p > 0.05) Both follow-ups QBPDS-PT 6 weeks (p = 0.83) and 3 months (p = 0.09) VAS 6 weeks (p = 0.14) | Aquatic exercises | VAS QBPDS-PT TSK-13 |
| Rabiei et al. [43], in 2021 FU: 8 weeks | PNE + Motor control exercise | VAS 8 weeks (p = 0.041) RMDQ 8 weeks (p = 0.021) | FABQ 8 weeks (p > 0.05) PSEQ 8 weeks (p > 0.05) | Group-based exercise | VAS RMDQ FABQ-W FABQ-PA PSEQ |
| Ryan et al. [44], in 2010 FU: 8 weeks 3 months | PNE | NRS 8 weeks (p = 0.025) PSEQ 8 weeks (p = 0.024) | TSK-13 Both follow-ups (p > 0.05) RMDQ Both follow-ups (p > 0.05) NRS 3 months (p > 0.05) PSEQ 3 months (p > 0.05) | PNE + Aerobic exercise | NRS RMDQ TSK-13 PSEQ-10 |
| Saracoglu et al. [45], in 2020 FU: 4 weeks 12 weeks | Group 1: PNE + Manual therapy + Home exercise | NPRS Both follow-ups: Group 1 vs. G. 3 (p < 0.001) ODI Both follow-ups: Group 1 vs. G. 3 (p < 0.001) TSK-17 Both follow-ups: Group 1 vs. G. 2 (p < 0.001) Group 1 vs. G.3 (p < 0.001) | NPRS Both follow-ups: Group 1 vs. G. 2 (p = 0.01) ODI Both follow-ups: Group 1 vs. G.2 (p = 0.67) | Gruppo 2: Manual therapy + Home exercise Gruppo 3: Home exercise | NPRS ODI TSK-17 |
| Serrat et al. [46], in 2020 FU: 6 weeks 12 weeks | Treatment as usual (TAU) + NAT-FM (PNE, Therapeutic exercise, activities in nature, Cognitive Behavioral Therapy (CBT), Mindfulness training) | FIQR Both follow-ups: (p < 0.001) VAS pain 6 weeks (p = 0.003), 12 weeks (p < 0.001) VAS fatigue 6 weeks (p = 0.002), 12 weeks (p < 0.001) HADS-A Both follow-ups: (p < 0.001) HADS-D 6 weeks (p = 0.027), 12 weeks (p < 0.001) SF-36 6 weeks (p = 0.017) and 12 weeks (p < 0.001) TSK-11 Both follow-ups: (p < 0.001) PCS Both follow-ups: (p > 0.001) | RSES Both follow-ups: (p > 0.05) | Treatment as usual (TAU) | FIQR VAS (pain) VAS (fatigue) HADS-A HADS-D SF-36 TSK-17 PCS RSES |
| Téllez-Garcia et al. [47], in 2015 FU: 4 weeks | PNE + Dry Needling | TSK-17 4 weeks (p = 0.008) MCID > 8 | RMDQ 4 weeks (p = 0.111) ODI 4 weeks (p = 0.542) NPRS 4 weeks (p = 0.801) | Dry Needling | NPRS ODI RMDQ TSK-17 |
| Van Ittersum et al. [48], in 2014 FU: 6 weeks 6 months | PNE | PCS Both follow-ups: (p > 0.05) FIQ (p > 0.05) for both follow-ups IPQ-R FM (p > 0.05) for both follow-ups | Relaxation Education (RE) | FIQ IPQ-FM PCS | |
| Van Oosterwjck et al. [49], in 2013 FU: 2 weeks 3 months | PNE | SF-36 “physical functioning” (p = 0.046) “general health perceptions” (p < 0.001) “vitality” (p = 0.047) “mental health” (p < 0.001) | FIQ 2 weeks (p > 0.05) 3 months (p = 0.079) PCS Both follow-ups (rumination) (p = 0.219), (magnification) (p = 0.109), (helplessness) (p = 0.265) and total (p = 0.158) TSK Both follow-ups (p = 0.360) PVAQ 2 weeks (p > 0.05) 3 months (p = 0.279) PCI (all subdomains) Both follow-ups (p > 0.05) SF-36 (other subdomains) (p > 0.05) | Education about pacing self-management techniques. | FIQ PCI PCS PVAQ TSK-17 SF-36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lepri, B.; Romani, D.; Storari, L.; Barbari, V. Effectiveness of Pain Neuroscience Education in Patients with Chronic Musculoskeletal Pain and Central Sensitization: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 4098. https://doi.org/10.3390/ijerph20054098
Lepri B, Romani D, Storari L, Barbari V. Effectiveness of Pain Neuroscience Education in Patients with Chronic Musculoskeletal Pain and Central Sensitization: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(5):4098. https://doi.org/10.3390/ijerph20054098
Chicago/Turabian StyleLepri, Beatrice, Daniele Romani, Lorenzo Storari, and Valerio Barbari. 2023. "Effectiveness of Pain Neuroscience Education in Patients with Chronic Musculoskeletal Pain and Central Sensitization: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 5: 4098. https://doi.org/10.3390/ijerph20054098