
Endometrial Injury Upregulates Expression of Receptivity Genes in Women with Implantation Failure
 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
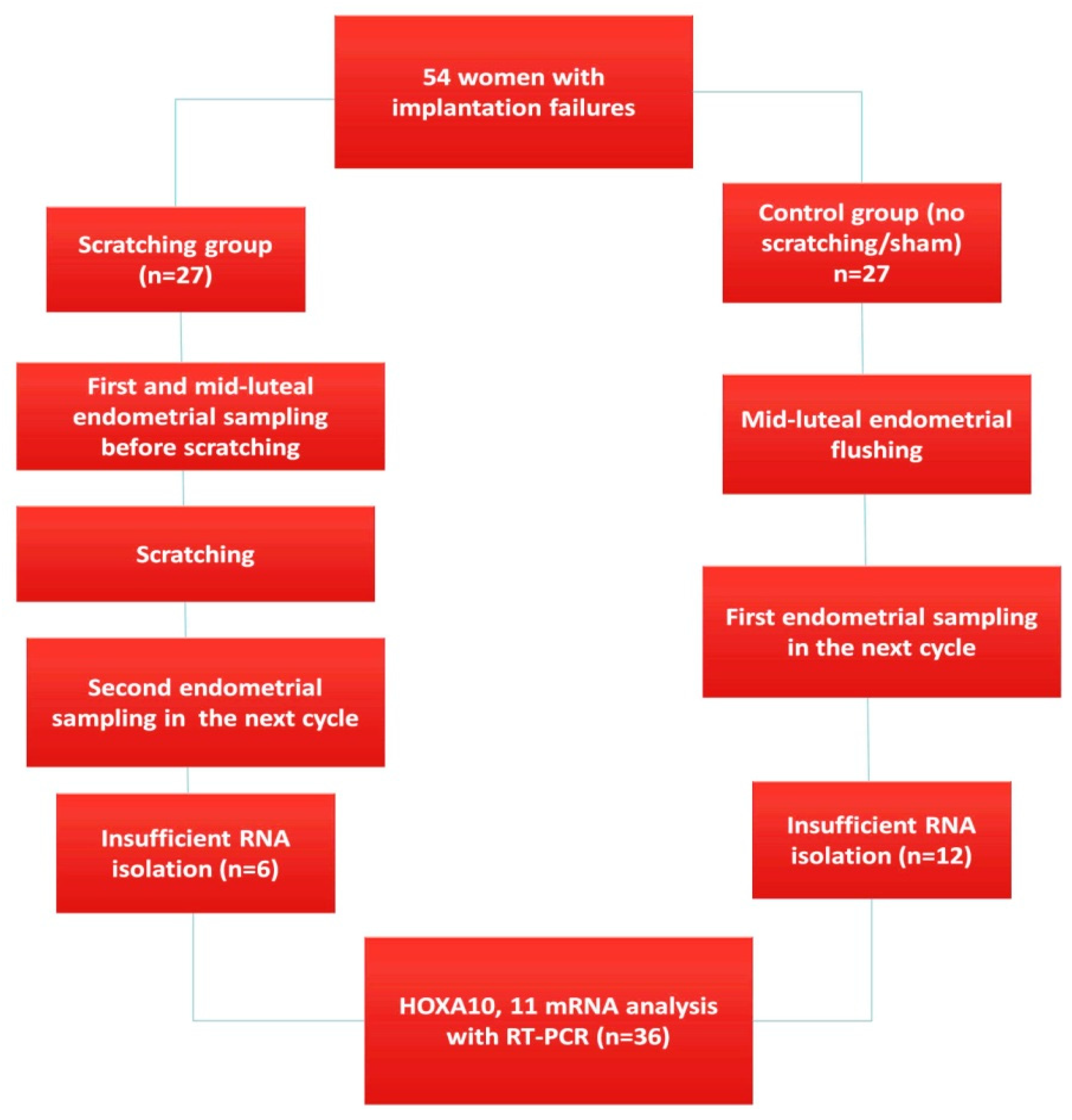
- Study design and participants
- Sample collection before and after endometrial injury/flushing
- RT-PCR
- Sample preparation, RNA isolation, and cDNA synthesis
- Measurement of HOXA10 and HOXA11 mRNA expression
- Measurement of endometrial HOXA10 and HOXA11 protein expressions
- Statistical Analysis
3. Results
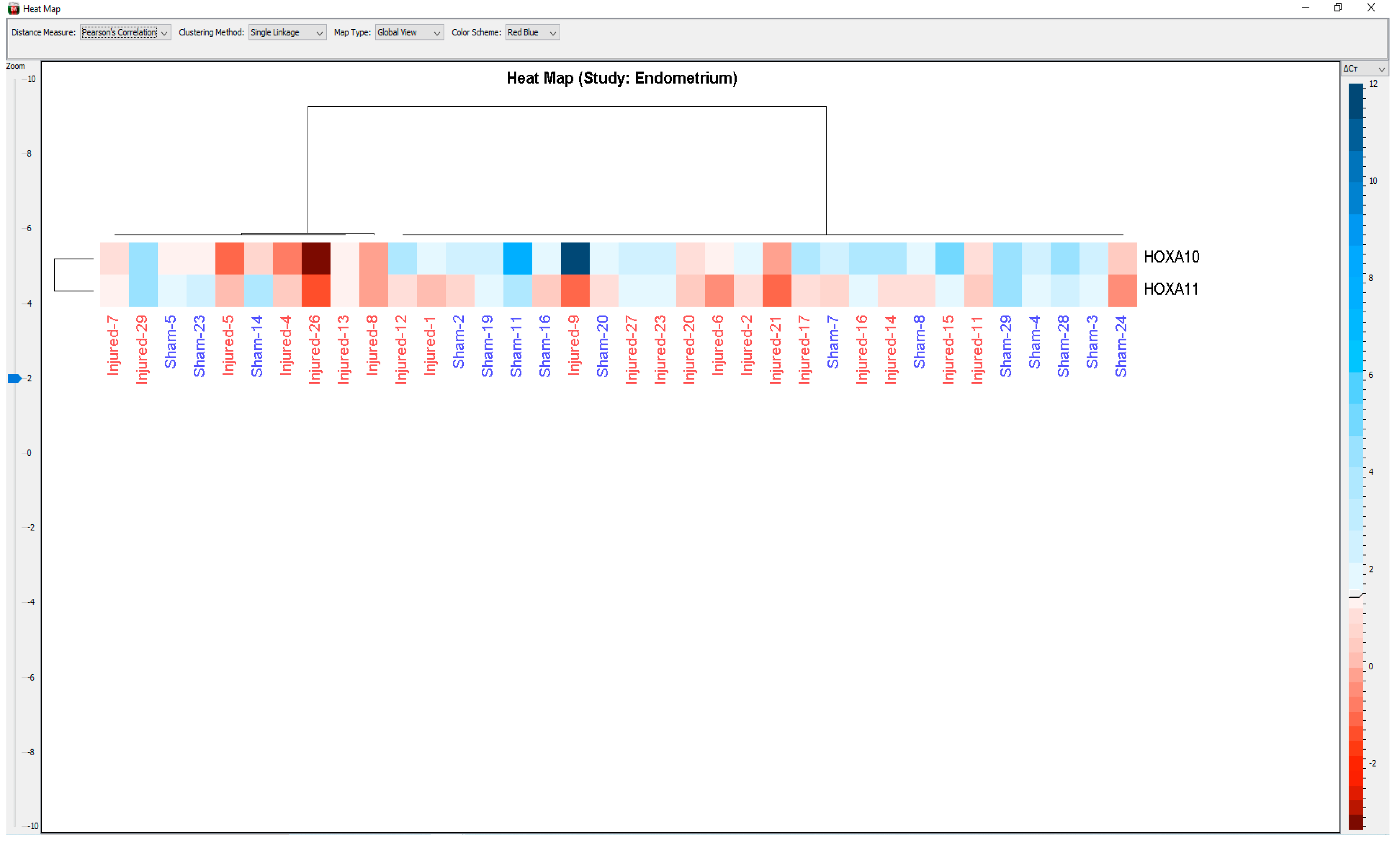
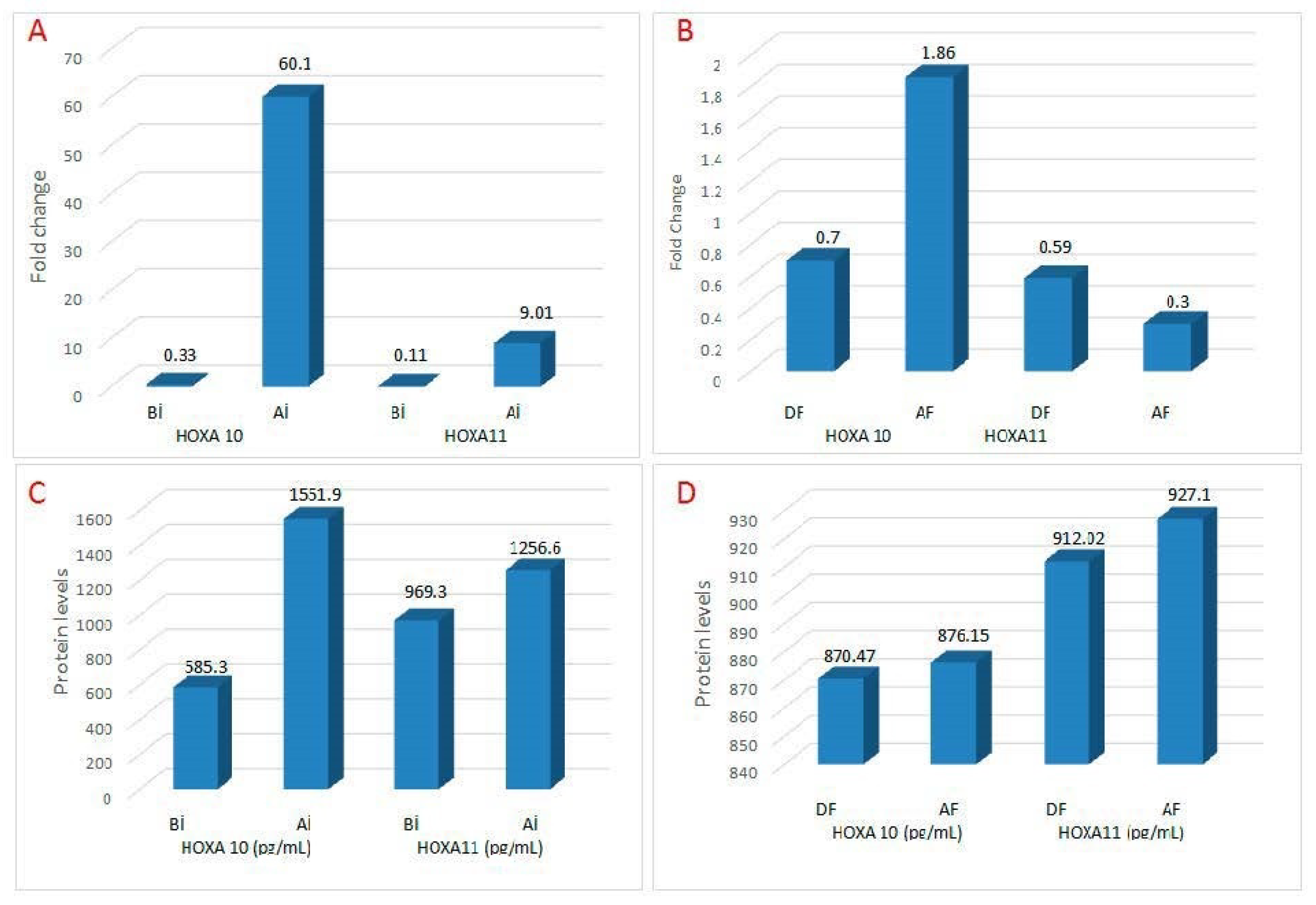
3.1. Pre- and Post-Injury Endometrial HOXA10 and 11 mRNA Levels
3.2. Pre- and Post-Injury Endometrial HOXA10 and HOXA11 Protein Levels
3.3. Fertility Outcome following Injury/Flushing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coughlan, C.; Ledger, W.; Wang, Q.; Liu, F.; Demirol, A.; Gurgan, T.; Cutting, R.; Ong, K.; Sallam, H.; Li, T.C. Recurrent implantation failure: Definition and management. Reprod. Biomed. Online 2014, 28, 14–38. [Google Scholar] [CrossRef] [Green Version]
- Franasiak, J.M.; Alecsandru, D.; Forman, E.J.; Gemmell, L.C.; Goldberg, J.M.; Llarena, N.; Margolis, C.; Laven, J.; Schoenmakers, S.; Seli, E. A review of the pathophysiology of recurrent implantation failure. Fertil. Steril. 2021, 116, 1436–1448. [Google Scholar] [CrossRef]
- Simon, A.; Laufer, N. Assessment and treatment of repeated implantation failure (RIF). J. Assist. Reprod. Genet. 2012, 29, 1227–1239. [Google Scholar] [CrossRef] [Green Version]
- Granot, I.; Dekel, N.; Bechor, E.; Segal, I.; Fieldust, S.; Barash, A. Temporal analysis of connexin43, protein and gene expression, throughout the menstrual cycle in human endometrium. Fertil. Steril. 2000, 73, 381–386. [Google Scholar] [CrossRef]
- Barash, A.; Dekel, N.; Fieldust, S.; Segal, I.; Schechtman, E.; Granot, I. Local injury to the endometrium doubles the incidence of successful pregnancies in patients undergoing in vitro fertilization. Fertil. Steril. 2003, 6, 1317–1322. [Google Scholar] [CrossRef]
- Gibreel, A.; Badawy, A.; El-Refai, W.; El-Adawi, N. Endometrial scratching to improve pregnancy rate in couples with unexplained subfertility: A randomized controlled trial. J. Obstet. Gynaecol. Res. 2013, 39, 680–684. [Google Scholar] [CrossRef]
- Siristatidis, C.; Kreatsa, M.; Koutlaki, N.; Galazios, G.; Regalities, V.P.; Papantoniou, N. Endometrial injury for RIF patients undergoing IVF/ICSI: A prospective nonrandomized controlled trial. Gynecol. Endocrinol. 2017, 33, 297–300. [Google Scholar] [CrossRef]
- Baum, M.; Yerushalmi, G.M.; Maman, E.; Kedem, A.; Machtinger, R.; Hourvitz, A.; Dor, J. Does local injury to the endometrium before IVF cycle really affect treatment outcome? Results of a randomized placebo-controlled trial. Gynecol. Endocrinol. 2012, 28, 933–936. [Google Scholar] [CrossRef]
- Ersahin, S.S.; Ersahin, A. Endometrial injury concurrent with hysteroscopy increases the expression of Leukemia inhibitory factor: A preliminary study. Reprod. Biol. Endocrinol. 2022, 20, 11. [Google Scholar] [CrossRef]
- Zeyneloglu, H.B.; Onalan, G. Remedies for recurrent implantation failure. Semin. Reprod. Med. 2014, 32, 297–305. [Google Scholar]
- Gnainsky, Y.; Granot, I.; Aldo, P.B.; Barash, A.; Or, Y.; Schechtman, E.; Mor, G.; Dekel, N. Local injury of the endometrium induces an inflammatory response that promotes successful implantation. Fertil. Steril. 2010, 94, 2030–2036. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Li, R.; Wang, R.; Huang, H.X.; Zhong, K. Local injury to the endometrium in controlled ovarian hyperstimulation cycles improves implantation rates. Fertil. Steril. 2008, 89, 1166–1176. [Google Scholar] [CrossRef]
- Kalma, Y.; Granot, I.; Gnainsky, Y.; Or, Y.; Czernobilsky, B.; Dekel, N.; Barash, A. Endometrial biopsy-induced gene modulation: First evidence for the expression of bladder-transmembranal uroplakin Ib in human endometrium. Fertil. Steril. 2009, 91, 1042–1049. [Google Scholar] [CrossRef]
- Du, H.; Taylor, H.S. The Role of Hox Genes in Female Reproductive Tract Development, Adult Function, and Fertility. Cold Spring Harb. Perspect. Med. 2015, 6, a023002. [Google Scholar] [CrossRef] [Green Version]
- Satokata, I.; Benson, G.; Maas, R. Sexually dimorphic sterility phenotypes in Hoxa10-deficient mice. Nature 1995, 374, 460–463. [Google Scholar] [CrossRef]
- Benson, G.V.; Lim, H.; Paria, B.C.; Satokata, I.; Dey, S.K.; Maas, R.L. Mechanisms of reduced fertility in Hoxa-10 mutant mice: Uterine homeosis and loss of maternal Hoxa-10 expression. Development 1996, 122, 2687–2696. [Google Scholar] [CrossRef]
- Polanski, L.T.; Baumgarten, M.N.; Quenby, S.; Brosens, J.; Campbell, B.K.; Raine-Fenning, N.J. What exactly do we mean by 'recurrent implantation failure'? A systematic review and opinion. Reprod. Biomed. Online 2014, 28, 409–423. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Tal, R.; Chao, H.; Liu, M.; Liu, Y. Effect of local endometrial injury in proliferative vs. luteal phase on IVF outcomes in unselected sub fertile women undergoing in vitro fertilization. Reprod. Biol. Endocrinol. 2017, 15, 75. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems; World Health Organization: Geneva, Switzerland, 1993; p. 129. [Google Scholar]
- Ben-Nagi, J.; Miell, J.; Mavrelos, D.; Naftalin, J.; Lee, C.; Jurkovic, D. Endometrial implantation factors in women with submucous uterine fibroids. Reprod. Biomed. Online 2010, 21, 610–615. [Google Scholar] [CrossRef] [Green Version]
- Nastri, C.O.; Lensen, S.F.; Gibreel, A.; Raine-Fenning, N.; Ferriani, R.A.; Bhattacharya, S.; Martins, W.P. Endometrial injury in women undergoing assisted reproductive techniques. Cochrane Database Syst. Rev. 2015, 3, CD009517. [Google Scholar] [CrossRef] [Green Version]
- Karimzadeh, M.A.; Ayazi Rozbahani, M.; Tabibnejad, N. Endometrial local injury improves the pregnancy rate among recurrent implantation failure patients undergoing in vitro fertilisation/intra cytoplasmic sperm injection: A randomised clinical trial. Aust. N. Z. J. Obstet. Gynaecol. 2009, 49, 677–680. [Google Scholar] [CrossRef]
- Maged, A.M.; Rashwan, H.; Abdel Aziz, S.; Ramadan, W.; Mostafa, W.A.I.; Metwally, A.A.; Katta, M. Randomized controlled trial of the effect of endometrial injury on implantation and clinical pregnancy rates during the first ICSI cycle. Int. J. Gynecol. Obstet. 2018, 2, 211–216. [Google Scholar] [CrossRef]
- Zygula, A.; Szymusik, I.; Grzechocinska, B.; Marianowski, P.; Wielgos, M. Endometrial injury for women with previous in vitro fertilization failure—Does it improve pregnancy rate? Neuroendocrinol. Lett. 2016, 6, 419–426. [Google Scholar]
- Panagiotopoulou, N.; Karavolos, S.; Choudhary, M. Endometrial injury prior to assisted reproductive techniques for recurrent implantation failure: A systematic literature review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 193, 27–33. [Google Scholar] [CrossRef]
- van Hoogenhuijze, N.E.; Kasius, J.C.; Broekmans, F.J.M.; Bosteels, J.; Torrance, H.L. Endometrial scratching prior to IVF; does it help and for whom? A systematic review and meta-analysis. Hum. Reprod. Open 2019, 2019, hoy025. [Google Scholar] [CrossRef] [Green Version]
- Loeb, L. Ueber die experimentelle Erzeugung von Knoten von Deciduage webe in dem Uterus des Meerschweinchensnachstattgefunder copulation. Zbtfür Allg Path Path Anat 1907, 18, 563–565. [Google Scholar]
- Humphrey, K.W. Interactions between oestradiol 3, 17 beta and progesterone on the induction and growth of deciduomata in ovariectomized mice. Aust. J. Biol. Sci. 1969, 22, 689–699. [Google Scholar] [CrossRef] [Green Version]
- Hoos, P.C.; Hoffman, L.H. Effect of histamine receptor antagonists and indomethacin on implantation in the rabbit. Biol. Reprod. 1983, 29, 833–840. [Google Scholar] [CrossRef] [Green Version]
- Lensen, S.F.; Armstrong, S.; Gibreel, A.; Nastri, C.O.; Raine-Fenning, N.; Martins, W.P. Endometrial injury in women undergoing in vitro fertilisation (IVF). Cochrane Database Syst. Rev. 2021, 6, CD009517. [Google Scholar]
- Celik, O.; Unlu, C.; Otlu, B.; Celik, N.; Caliskan, E. Laparoscopic endometrioma resection increases peri-implantation endometrial HOXA-10 and HOXA-11 mRNA expression. Fertil. Steril. 2015, 104, 356–365. [Google Scholar] [CrossRef]
- Taylor, H.S. The role of HOX genes in the development and function of the female reproductive tract. Semin. Reprod. Med. 2000, 18, 81–89. [Google Scholar] [CrossRef]
- Lim, H.; Ma, L.; Ma, W.G.; Maas, R.L.; Dey, S.K. Hoxa-10 regulates uterine stromal cell responsiveness to progesterone during implantation and decidualization in the mouse. Mol. Endocrinol. 1999, 13, 1005–1017. [Google Scholar] [CrossRef]
- Li, R.; Wang, R.; Zhou, L. Local injury of the proliferative phase endometrium substantially increases the ER expression in following secretory phase endometrium. Fertil. Steril. 2008, 90, S162–S163. [Google Scholar] [CrossRef]
- Li, R.; Hao, G. Local injury to the endometrium: Its effect on implantation. Curr. Opin. Obstet. Gynecol. 2009, 21, 236–239. [Google Scholar] [CrossRef]
- Ubaldi, F.; Bourgain, C.; Tournaye, H.; Smitz, J.; Van Steirteghem, A.; Devroey, P. Endometrial evaluation by aspiration biopsy on the day of oocyte retrieval in the embryo transfer cycles in patients with serum progesterone rise during the follicular phase. Fertil. Steril. 1997, 67, 521–526. [Google Scholar] [CrossRef]
- Celik, O.; Acet, M.; Kucuk, T.; Haberal, E.T.; Acet, T.; Bozkurt, M.; Sahin, L.; Verit, F.F.; Caliskan, E. Surgery for Benign Gynecological Disorders Improve Endometrium Receptivity. Reprod. Sci. 2017, 24, 174–192. [Google Scholar] [CrossRef]
- Daftary, G.S.; Kayisli, U.; Seli, E.; Bukulmez, O.; Arici, A.; Taylor, H.S. Salpingectomy increases peri-implantation endometrial HOXA10 expression in women with hydrosalpinx. Fertil. Steril. 2007, 87, 367–372. [Google Scholar] [CrossRef]
- Senturk, S.; Celik, O.; Dalkilic, S.; Hatirnaz, S.; Celik, N.; Unlu, C.; Otlu, B. Laparoscopic Ovarian Drilling Improves Endometrial Homeobox Gene Expression in PCOS. Reprod. Sci. 2020, 27, 675–680. [Google Scholar] [CrossRef]
- Piccinni, M.P.; Beloni, L.; Livi, C.; Maggi, E.; Scarselli, G.; Romagnani, S. Defective production of both leukemia inhibitory factor and type 2 T-helper cytokines by decidual T cells in unexplained recurrent abortions. Nat. Med. 1998, 4, 1020. [Google Scholar] [CrossRef]
- Senturk, L.M.; Arici, A. Leukemia inhibitory factor in human reproduction. Am. J. Reprod. Immunol. 1998, 39, 144–151. [Google Scholar] [CrossRef]
- De La Cruz, C.C.; Der-Avakian, A.; Spyropoulos, D.D.; Tieu, D.D.; Carpenter, E.M. Targeted disruption of Hoxd9 and Hoxd10 alters locomotor behavior, vertebral identity, and peripheral nervous system development. Dev. Biol. 1999, 216, 595–610. [Google Scholar] [CrossRef] [Green Version]
- Celik, O.; Celik, N.; Zan, E.; Dalkilic, S.; Saglam, A.; Yurci, A.; Senturk, S.; Sahin, E.; Sahin, M.E. Genome-wide expression analysis of endometrium before and after endometrioma surgery. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 253, 141–147. [Google Scholar] [CrossRef]
- Katariya, K.O.; Bates, G.W.; Robinson, R.D.; Arthur, N.J.; Propst, A.M. Does the timing of mock embryo transfer affect in vitro fertilization implantation and pregnancy rates? Fertil. Steril. 2007, 88, 1462–1464. [Google Scholar] [CrossRef]
- Borkar, A.; Shah, A.; Gudi, A.; Homburg, R. Outcome of mock embryo transfer before the first IVF cycle: A randomized control trial. Int. J. Reprod. Biomed. 2020, 18, 951–960. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Endometrial Scratching (n = 27) | Non-Scratching (n = 27) | p * | ||||
|---|---|---|---|---|---|---|
| Age (yrs) | 28.3 ± 5.22 | 27.9 ± 4.20 | 0.26 | |||
| BMI (kg/m2) | 22.9 ± 1.53 | 23.7 ± 4.13 | 0.32 | |||
| Infertility duration (yrs) | 3.76 ± 1.40 | 3.89 ± 1.02 | 0.09 | |||
| Failed IVF/ICSI trial | 2.79 ± 1.50 | 2.87 ± 1.90 | 0.43 | |||
| Before scratching | After scratching | p | During flushing | After flushing | p | |
| Endometrial thickness (mm) | 8.66 ± 2.76 | 10.9 ± 2.30 | 0.01 | 8.59 ± 1.99 | 9.02 ± 2.60 | 0.36 |
| LH (mIU/mL) | 4.97 ± 1.90 | 5.13 ± 1.07 | 0.69 | 4.87 ± 1.20 | 4.98 ± 1.87 | 0.20 |
| FSH (mIU/mL) | 5.43 ± 1.08 | 5.32 ± 1.23 | 0.51 | 5.39 ± 1.10 | 5.40 ± 1541 | 0.64 |
| Estradiol (pg/mL) | 37.9 ± 6.40 | 39.4 ± 4.80 | 0.74 | 39.7 ± 6.70 | 38.3 ± 7.44 | 0.51 |
| AFC | 10.2 ± 4.22 | 10.9 ± 3.21 | 0.36 | 9.20 ± 3.40 | 8.76 ± 2.40 | 0.56 |
| Genes | Groups | Average ΔCt | Average 2−ΔCt | Fold Change * | p-Values ** | Regulation |
|---|---|---|---|---|---|---|
| Scratching group (n = 21) *** | ||||||
| a-Before injury | 7.66 | 0.0010 | 0.33 | 0.51 | Down |
| b-After injury | 6.03 | 0.0350 | 60.1 | 0.01 | Up | |
| c-Before injury | 5.70 | 0.0044 | 0.11 | 0.30 | Down |
| d-After injury | 4.30 | 0.0600 | 9.01 | 0.02 | Up | |
| Non-scratching group (n = 15) *** | ||||||
| a-During flushing | 8.50 | 0.0303 | 0.70 | 0.22 | Down |
| b-After flushing | 7.01 | 0.0245 | 1.86 | 0.40 | Up | |
| c-During flushing | 4.05 | 0.0003 | 0.59 | 0.24 | Down |
| d-After flushing | 4.20 | 0.0350 | 0.30 | 0.39 | Down | |
| 1a vs. 3a | 0.33 vs. 0.70 | 0.08 | ||||
| 1b vs. 3b | 60.1 vs. 1.86 | 0.01 | ||||
| 2c vs. 4c | 0.11 vs. 0.59 | 0.65 | ||||
| 2d vs. 4d | 9.01 vs. 0.30 | 0.03 | ||||
| 1b vs. 2d | 60.1 vs. 9.01 | 0.01 | ||||
| Homeobox Genes | Groups | Protein Levels * | p-Values ** |
|---|---|---|---|
| Scratching (n = 27) | |||
| HOXA10 (pg/mL) | Before injury | 585.3 ± 241.6 | <0.001 |
| After injury | 1551.9 ± 304.8 | ||
| HOXA11 (pg/mL) | Before injury | 969.3 ± 226.3 | <0.003 |
| After injury | 1256.6 ± 121.1 | ||
| Non-scratching (n = 27) | |||
| HOXA10 (pg/mL) | During flushing | 870.4 ± 221.2 | >0.05 |
| After flushing | 876.1 ± 231.0 | ||
| HOXA11 (pg/mL) | During flushing | 912.0 ± 149.6 | >0.05 |
| After flushing | 927.1 ± 51.30 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Celik, O.; Yurci, A.; Ersahin, A.; Gungor, N.D.; Celik, N.; Ozcil, M.D.; Dogan, S.; Dalkilic, S.; Dalkilic, L.; Ulug, U.; et al. Endometrial Injury Upregulates Expression of Receptivity Genes in Women with Implantation Failure. Int. J. Environ. Res. Public Health 2023, 20, 3942. https://doi.org/10.3390/ijerph20053942
Celik O, Yurci A, Ersahin A, Gungor ND, Celik N, Ozcil MD, Dogan S, Dalkilic S, Dalkilic L, Ulug U, et al. Endometrial Injury Upregulates Expression of Receptivity Genes in Women with Implantation Failure. International Journal of Environmental Research and Public Health. 2023; 20(5):3942. https://doi.org/10.3390/ijerph20053942
Chicago/Turabian StyleCelik, Onder, Arzu Yurci, Aynur Ersahin, Nur D. Gungor, Nilufer Celik, Mustafa D. Ozcil, Serdar Dogan, Semih Dalkilic, Lutfiye Dalkilic, Ulun Ulug, and et al. 2023. "Endometrial Injury Upregulates Expression of Receptivity Genes in Women with Implantation Failure" International Journal of Environmental Research and Public Health 20, no. 5: 3942. https://doi.org/10.3390/ijerph20053942