
Therapeutic Adherence of People with Mental Disorders: An Evolutionary Concept Analysis
 , ,
, ,  , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
1.1. Background
1.2. Aim and Research Questions
- What surrogate terms and related concepts are used?
- What attributes, antecedents, and consequences apply to the concept of therapeutic adherence in the mental health context?
2. Materials and Methods
2.1. Study Design
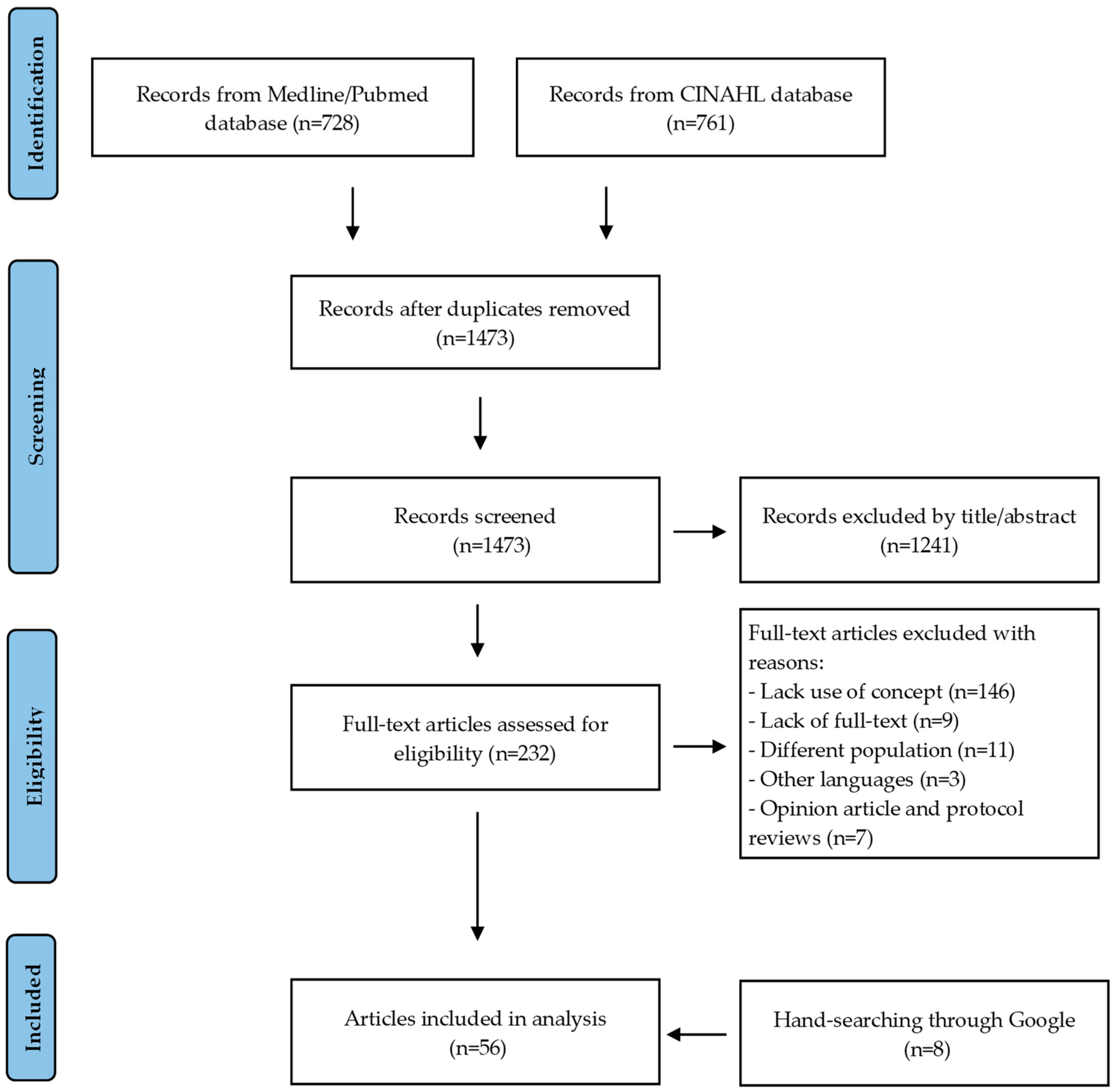
2.2. Literature Search Methods
3. Results
3.1. Concept of Interest, Surrogate Terms, and Related Concepts
3.2. Attributes

{kind=link}
{kind=link}
| Individual Level | Microsystem Level | Meso/Exosystem Level |
|---|---|---|
| Motivation for treatment and readiness to change [34,35,36,37]. Medication literacy combines: (a) Readiness to understand the role of medication, how to use it, and understanding how it works for the patient [34,38]; (b) Knowledge about mental health disorders and understanding how to use medication [3,34,38,39]; (c) Understanding what works personally [38]; (d) Ability to reflect on past experiences with medication, self-medication, and forgetfulness [40]. Illness-Symptom experiences: (a) Tolerance to side effects of medication [41,42]; (b) Symptoms and severity of symptoms [42,43]. Personal resources include: (a) Coping skills [44]; (b) Self-efficacy [36,37,45]; (c) Self-care ability [33,43]; (d) Ability to remember [43]; (e) Ability to establish interpersonal skills [33]. | Quality of the therapeutic alliance [40,45,46,47,48,49,50,51,52]. Shared decision making and negotiation [39,40,46,50,53,54,55,56,57]. Community support contains: (a) Family involvement and social support [39,40,48,51,58]; (b) Patient and family ongoing support [42,48,61]; (c) Mutual support groups [46,59,60]; (d) Peer workers as role models [40]. | Therapy-related factors: (1) Medication plan (a) Type of medication (antipsychotics) [51]; (b) Route of administration/delivery; Alternate oral with injectable medication [40,50,61,62]; (c) Long-acting depot injection reduces nonintentional nonadherence [40,50,63]; (d) Storage of medication-medication packs or dosette boxes [40]/pillboxes [64]. (2) Other Interventions (a) Psychoeducation along with drug treatment [50]; (b) Type of treatment provision (telehealth vs. face-to-face) [52,61]; (c) Use of reminders and electronic prompting [50,62,64]. Organizational-related factors: (a) Availability and flexibility of services (schedules) [48,65]; (b) Person-centered planning and collaborative documentation [66]; (c) Community centers and community groups [40]; (d) Services oriented toward their individual goals [66]; (e) Quality of care and attention to patient care needs based on an individual treatment project [65] and case management [40]; (f) Continuity of care [46,51,62] (g) Control of patients over their treatment [66]; (h) Good discharge planning [49]; (i) Home visits [62]; (j) Multidisciplinary work [65]. |
3.3. Antecedents
3.4. Consequences
3.5. Pragmatic Utility and Empirical Referents
3.6. Exemplar Case Study
3.7. Operational Definition
4. Discussion
4.1. Study Limitations
4.2. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Institute of Health Metrics and Evaluation. Global Health Data Exchange (GHDx). Available online: https://vizhub.healthdata.org/gbd-results/ (accessed on 22 December 2022).
- Semahegn, A.; Torpey, K.; Manu, A.; Assefa, N.; Tesfaye, G.; Ankomah, A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: A systematic review and meta-analysis. Syst. Rev. 2020, 9, 17. [Google Scholar] [CrossRef] [Green Version]
- Deng, M.; Zhai, S.; Ouyang, X.; Liu, Z.; Ross, B. Factors influencing medication adherence among patients with severe mental disorders from the perspective of mental health professionals. BMC Psychiatry 2022, 22, 22. [Google Scholar] [CrossRef]
- National Council on Patient Information and Education (NCPIE). Enhancing Prescription Medicine Adherence: A National Action Plan; NCPIE: Rockville, MD, USA, 2007. [Google Scholar]
- Sabaté, E. Adherence to Long-Term Therapies: Evidence for Action; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Christensen, A.J. Patient Adherence to Medical Treatment Regimens: Bridging the Gap Between Behavioral Science and Biomedicine; Yale University Press: New Haven, CT, USA; London, UK, 2004. [Google Scholar]
- Chakrabarti, S. What’s in a name? Compliance, adherence and concordance in chronic psychiatric disorders. World J. Psychiatry 2014, 4, 30–36. [Google Scholar] [CrossRef]
- Bissonnette, J.M. Adherence: A concept analysis. J. Adv. Nurs. 2008, 63, 634–643. [Google Scholar] [CrossRef]
- Martin, L.R.; Williams, S.L.; Haskard, K.B.; Dimatteo, M.R. The challenge of patient adherence. Ther. Clin. Risk Manag. 2005, 1, 189–199. [Google Scholar]
- Emilsson, M.; Gustafsson, P.; Öhnström, G.; Marteinsdottir, I. Impact of personality on adherence to and beliefs about ADHD medication, and perceptions of ADHD in adolescents. BMC Psychiatry 2020, 20, 139. [Google Scholar] [CrossRef] [Green Version]
- Ferretti, F.; Goracci, A.; Laurenzi, P.F.; Centola, R.; Crecchi, I.; De Luca, A.; Monzillo, J.; Guidi, O.; Sinigaglia, G.; Gualtieri, G.; et al. Neuroticism and Conscientiousness Moderate the Effect of Oral Medication Beliefs on Adherence of People with Mental Illness during the Pandemic. Brain Sci. 2022, 12, 1315. [Google Scholar] [CrossRef]
- Marrero, R.J.; Fumero, A.; de Miguel, A.; Peñate, W. Psychological factors involved in psychopharmacological medication adherence in mental health patients: A systematic review. Patient Educ. Couns. 2020, 103, 2116–2131. [Google Scholar] [CrossRef]
- Hyvert, S.; Yailian, A.-L.; Haesebaert, J.; Vignot, E.; Chapurlat, R.; Dussart, C.; De Freminville, H.; Janoly-Dumenil, A. Association between health literacy and medication adherence in chronic diseases: A recent systematic review. Int. J. Clin. Pharm. 2022, 45, 38–51. [Google Scholar] [CrossRef]
- Gardner, C.L. Adherence: A concept analysis. Int. J. Nurs. Knowl. 2015, 26, 96–101. [Google Scholar] [CrossRef]
- Tofthagen, R.; Fagerstrøm, L.M. Rodgers’ evolutionary concept analysis-a valid method for developing knowledge in nursing science. Scand. J. Caring Sci. 2010, 24, 21–31. [Google Scholar] [CrossRef]
- Bombard, Y.; Baker, G.R.; Orlando, E.; Fancott, C.; Bhatia, P.; Casalino, S.; Onate, K.; Denis, J.L.; Pomey, M.P. Engaging patients to improve quality of care: A systematic review. Implement. Sci. 2018, 13, 98. [Google Scholar] [CrossRef]
- Miller, M.J.; Ambrose, D.M. The Problem of Missed Mental Healthcare Appointments. Clin. Schizophr. Relat. Psychoses 2019, 12, 177–184. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, P.; Balasundaram, S.; Sankaran, A.; Chandrasekaran, V.; Sarkar, S.; Choudhury, S. Factors associated with medication non-adherence among patients with severe mental disorder—A cross-sectional study in a tertiary care centre. Explor. Res. Clin. Soc. Pharm. 2022, 7, 100178. [Google Scholar] [CrossRef]
- Lieslehto, J.; Tiihonen, J.; Lähteenvuo, M.; Tanskanen, A.; Taipale, H. Primary Nonadherence to Antipsychotic Treatment Among Persons with Schizophrenia. Schizophr. Bull. 2022, 48, 655–663. [Google Scholar] [CrossRef]
- Kwame, A.; Petrucka, P.M. A literature-based study of patient-centered care and communication in nurse-patient interactions: Barriers, facilitators, and the way forward. BMC Nurs. 2021, 20, 158. [Google Scholar] [CrossRef]
- Adams, C.E.; Gringart, E.; Strobel, N.A. Explaining adults’ mental health help-seeking through the lens of the theory of planned behavior: A scoping review. Syst. Rev. 2022, 11, 160. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Lazaro, C.I.; García-González, J.M.; Adams, D.P.; Fernandez-Lazaro, D.; Mielgo-Ayuso, J.; Caballero-Garcia, A.; Racionero, F.M.; Córdova, A.; Miron-Canelo, J.A. Adherence to treatment and related factors among patients with chronic conditions in primary care: A cross-sectional study. BMC Fam. Pract. 2019, 20, 132. [Google Scholar] [CrossRef]
- Berben, L.; Dobbels, F.; Engberg, S.; Hill, M.N.; De Geest, S. An ecological perspective on medication adherence. West. J. Nurs. Res. 2012, 34, 635–653. [Google Scholar] [CrossRef]
- Eriksson, M.; Ghazinour, M.; Hammarström, A. Different uses of Bronfenbrenner’s ecological theory in public mental health research: What is their value for guiding public mental health policy and practice? Soc. Theory Health 2018, 16, 414–433. [Google Scholar] [CrossRef] [Green Version]
- Rodgers, B.L.; Knafl, K.A. Concept Development in Nursing: Foundations, Techniques and Applications, 2nd ed.; Saunders: Philadelphia, PA, USA, 2000. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Balkrishnan, R. The importance of medication adherence in improving chronic-disease related outcomes: What we know and what we need to further know. Med. Care 2005, 43, 517–520. [Google Scholar] [CrossRef]
- Grady, P.A.; Gough, L.L. Self-management: A comprehensive approach to management of chronic conditions. Am. J. Public Health 2014, 104, e25–e31. [Google Scholar] [CrossRef]
- Royal Pharmaceutical Society of Great Britain; Marinker, M. From Compliance to Concordance: Achieving Shared Goals in Medicine Taking; Royal Pharmaceutical Society, in Partnership with Merck Sharp & Dohme: London, UK, 1997. [Google Scholar]
- Løvsletten, M.; Lossius Husum, T.; Haug, E.; Granerud, A. Cooperation in the mental health treatment of patients with outpatient commitment. SAGE Open Med. 2020, 8, 2050312120926410. [Google Scholar] [CrossRef]
- Substance Abuse and Mental Health Services Administration. From Action to Maintenance: Stabilizing Change. In Enhancing Motivation for Change in Substance Use Disorder Treatment: Updated 2019. Substance Abuse and Mental Health Services Administration; Substance Abuse and Mental Health Services Administration: Rockville, MD, USA, 2019; pp. 109–124. [Google Scholar]
- Munson, M.R.; Jaccard, J.; Moore, K.L.; Rodwin, A.H.; Shimizu, R.; Cole, A.R.; Scott, L.D.; Narendorf, S.C.; Davis, M.; Gilmer, T.; et al. Impact of a brief intervention to improve engagement in a recovery program for young adults with serious mental illness. Schizophr. Res. 2022, 250, 104–111. [Google Scholar] [CrossRef]
- Xiao, J.; Mi, W.; Li, L.; Shi, Y.; Zhang, H. High relapse rate and poor medication adherence in the Chinese population with schizophrenia: Results from an observational survey in the People’s Republic of China. Neuropsychiatr. Dis. Treat. 2015, 11, 1161–1167. [Google Scholar] [CrossRef] [Green Version]
- Cruz, L.P.; Vedana, K.G.; Mercedes, B.P.; Miasso, A.I. Difficulties related to medication therapy for anxiety disorder. Rev. Eletr. Enferm. 2016, 18, e1155. [Google Scholar] [CrossRef] [Green Version]
- Gibson, B.; Butler, J.; Zirkle, M.; Hammond, K.; Weir, C. Foraging for Information in the EHR: The Search for Adherence Related Information by Mental Health Clinicians. AMIA Annu. Symp. Proc. 2017, 2016, 600–608. [Google Scholar]
- Kukla, M.; Salyers, M.P.; Lysaker, P.H. Levels of patient activation among adults with schizophrenia: Associations with hope, symptoms, medication adherence, and recovery attitudes. J. Nerv. Ment. Dis. 2013, 201, 339–344. [Google Scholar] [CrossRef]
- Magura, S.; Mateu, P.F.; Rosenblum, A.; Matusow, H.; Fong, C. Risk factors for medication non-adherence among psychiatric patients with substance misuse histories. Ment. Health Subst. Use 2014, 7, 381–390. [Google Scholar] [CrossRef] [Green Version]
- Inder, M.; Lacey, C.; Crowe, M. Participation in decision-making about medication: A qualitative analysis of medication adherence. Int. J. Ment. Health Nurs. 2019, 28, 181–189. [Google Scholar] [CrossRef]
- Lin, Y.Y.; Yen, W.J.; Hou, W.L.; Liao, W.C.; Lin, M.L. Mental Health Nurses’ Tacit Knowledge of Strategies for Improving Medication Adherence for Schizophrenia: A Qualitative Study. Healthcare 2022, 10, 492. [Google Scholar] [CrossRef]
- Clifford, L.M.; Crabb, S.J.; Turnbull, D.R.; Hahn, L.A.; Galletly, C.A. A qualitative study of medication adherence amongst people with schizophrenia. Arch. Psychiatr. Nurs. 2020, 34, 194–199. [Google Scholar] [CrossRef]
- Rosen, C.S.; Azevedo, K.J.; Tiet, Q.Q.; Greene, C.J.; Wood, A.E.; Calhoun, P.; Bowe, T.; Capehart, B.P.; Crawford, E.F.; Greenbaum, M.A.; et al. An RCT of Effects of Telephone Care Management on Treatment Adherence and Clinical Outcomes Among Veterans With PTSD. Psychiatr. Serv. 2017, 68, 151–158. [Google Scholar] [CrossRef]
- Nyanyiwa, S.; Peters, K.; Murphy, G. A scoping review: Treatment attitudes and adherence for adults with schizophrenia. J. Clin. Nurs. 2022, 31, 3060–3075. [Google Scholar] [CrossRef]
- Mukattash, T.L.; Alzoubi, K.H.; Abu El-Rub, E.; Jarab, A.S.; Al-Azzam, S.I.; Khdour, M.; Shara, M.; Al Hamarneh, Y.N. Prevalence of non-adherence among psychiatric patients in Jordan, a cross-sectional study. Int. J. Pharm. Pract. 2016, 24, 217–221. [Google Scholar] [CrossRef]
- White, D.A.; McGuire, A.B.; Luther, L.; Anderson, A.I.; Phalen, P.; McGrew, J.H. Consumer factors predicting level of treatment response to illness management and recovery. Psychiatr. Rehabil. J. 2017, 40, 344–353. [Google Scholar] [CrossRef]
- Xu, C.; Xie, H.; Zhou, Z.; Govindasamy, A.; Mao, R.; Chan, Y.H. Advanced practice nurses led clinic in a psychiatric hospital: An outcome evaluation in Singapore. Arch. Psychiatr. Nurs. 2020, 34, 129–133. [Google Scholar] [CrossRef]
- del Barrio, L.R.; Cyr, C.; Benisty, L.; Richard, P.O. Gaining Autonomy & Medication Management (GAM): New perspectives on well-being, quality of life and psychiatric medication. Cien. Saude Colet. 2013, 18, 2879–2887. [Google Scholar] [CrossRef] [Green Version]
- Salomon, C.; Hamilton, B. “All roads lead to medication?” Qualitative responses from an Australian first-person survey of antipsychotic discontinuation. Psychiatr. Rehabil. J. 2013, 36, 160–165. [Google Scholar] [CrossRef]
- Mazzaia, M.C.; Souza, M.A. Adesão ao tratamento no transtorno afetivo bipolar-percepção do usuário e do profissional de saúde. Rev. Port. Enferm. Saúde Mental. 2017, 17, 34–42. [Google Scholar] [CrossRef]
- Sibeko, G.; Temmingh, H.; Mall, S.; Williams-Ashman, P.; Thornicroft, G.; Susser, E.S.; Lund, C.; Stein, D.J.; Milligan, P.D. Improving adherence in mental health service users with severe mental illness in South Africa: A pilot randomized controlled trial of a treatment partner and text message intervention vs. treatment as usual. BMC Res. Notes 2017, 10, 584. [Google Scholar] [CrossRef] [Green Version]
- Jawad, I.; Watson, S.; Haddad, P.M.; Talbot, P.S.; McAllister-Williams, R.H. Medication nonadherence in bipolar disorder: A narrative review. Ther. Adv. Psychopharmacol. 2018, 8, 349–363. [Google Scholar] [CrossRef] [Green Version]
- Tham, X.C.; Xie, H.; Chng, C.M.L.; Seah, X.Y.; Lopez, V.; Klainin-Yobas, P. Exploring predictors of medication adherence among inpatients with schizophrenia in Singapore’s mental health settings: A non-experimental study. Arch. Psychiatr. Nurs. 2018, 32, 536–548. [Google Scholar] [CrossRef]
- Dixon, L.B.; Holoshitz, Y.; Nossel, I.R. Treatment engagement of individuals experiencing mental illness: Review and update. World Psychiatry 2016, 15, 13–20. [Google Scholar] [CrossRef] [Green Version]
- Mahone, I.H.; Maphis, C.F.; Snow, D.E. Effective Strategies for Nurses Empowering Clients with Schizophrenia: Medication Use as a Tool in Recovery. Issues Ment. Health Nurs. 2016, 37, 372–379. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, L.L.; Campos, R.T. Narratives of users of mental health services in an experiment with autonomous management of medication. Cad. Saude Publica 2017, 33, e00166216. [Google Scholar] [CrossRef] [Green Version]
- Finnerty, M.T.; Layman, D.M.; Chen, Q.; Leckman-Westin, E.; Bermeo, N.; Ng-Mak, D.S.; Rajagopalan, K.; Hoagwood, K.E. Use of a Web-Based Shared Decision-Making Program: Impact on Ongoing Treatment Engagement and Antipsychotic Adherence. Psychiatr. Serv. 2018, 69, 1215–1221. [Google Scholar] [CrossRef] [Green Version]
- Fiorillo, A.R.; Barlati, S.; Bellomo, A.; Corrivetti, G.; Nicolò, G.M.; Sampogna, G.; Stanga, V.; Veltro, F.; Maina, G.; Vita, A. The role of shared decision-making in improving adherence to pharmacological treatments in patients with schizophrenia: A clinical review. Ann. Gen. Psychiatry 2020, 19, 43. [Google Scholar] [CrossRef]
- Eliacin, J.; Carter, J.M.; Bass, E.B.; Flanagan, M.E.; Salyers, M.P.; McGuire, A.L. Implementation and staff understanding of shared decision-making in the context of recovery-oriented care across US Veterans Health Administration (VHA) inpatient mental healthcare units: A mixed-methods evaluation. BMJ Open 2022, 12, e057300. [Google Scholar] [CrossRef]
- Krutis, S.D. Medication Adherence, Social Support, and Recovery: Perspectives of Individuals with Schizophrenia Spectrum Disorders and Their Families. Ph.D. Dissertation, Towson University, Towson, MD, USA, 2012. [Google Scholar]
- Alston, M.A.; Bennett, C.F.; Rochani, H.D. Treatment Adherence in Youth with First-Episode Psychosis: Impact of Family Support and Telehealth Delivery. Issues Ment. Health Nurs. 2019, 40, 951–956. [Google Scholar] [CrossRef]
- Boardman, G.H.; McCann, T.V.; Kerr, D. A peer support programme for enhancing adherence to oral antipsychotic medication in consumers with schizophrenia. J. Adv. Nurs. 2014, 70, 2293–2302. [Google Scholar] [CrossRef]
- Orsi, J.A.; Malinowski, F.R.; Kagan, S.; Weingarten, R.; Villares, C.C.; Bressan, R.A.; de Oliveira, W.F.; Andrade, M.C.; Gadelha, A. Evaluation of Ongoing Participation of People with Schizophrenia in a Mutual Support Group as a Complementary Intervention to Outpatient Psychiatric Treatment. Psychiatr. Q. 2021, 92, 1283–1296. [Google Scholar] [CrossRef]
- Velligan, D.; Mintz, J.; Maples, N.; Li, X.; Gajewski, S.; Carr, H.; Sierra, C. A randomized trial comparing in person and electronic interventions for improving adherence to oral medications in schizophrenia. Schizophr. Bull. 2013, 39, 999–1007. [Google Scholar] [CrossRef]
- Popp, B.S.; Manea, M.M.; Moraru, M.O. Treatment adherence and social functioning in patients diagnosed with schizophrenia and treated with antipsychotic depot medication. Clujul Med. 2014, 87, 109–112. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, N.J.; Gandhi, S.; Baruah, A.K. Effectiveness of specific intervention on treatment adherence of persons with mental illness: A pilot study. Indian J. Psychiatry 2015, 57, 403–406. [Google Scholar] [CrossRef]
- Malvezzi, C.D.; Gerhardinger, H.C.; Santos, L.F.; Toledo, V.P.; Garcia, A.P. Adherence to treatment by the staff of a mental health service: An exploratory study. Online Braz. J. Nurs. 2016, 15, 177–187. [Google Scholar] [CrossRef]
- Stanhope, V.; Ingoglia, C.; Schmelter, B.; Marcus, S.C. Impact of person-centered planning and collaborative documentation on treatment adherence. Psychiatr. Serv. 2013, 64, 76–79. [Google Scholar] [CrossRef]
- Offord, S.; Lin, J.; Mirski, D.; Wong, B. Impact of early nonadherence to oral antipsychotics on clinical and economic outcomes among patients with schizophrenia. Adv. Ther. 2013, 30, 286–297. [Google Scholar] [CrossRef]
- Timlin, U.; Hakko, H.; Heino, R.; Kyngäs, H. A systematic narrative review of the literature: Adherence to pharmacological and nonpharmacological treatments among adolescents with mental disorders. J. Clin. Nurs. 2014, 23, 3321–3334. [Google Scholar] [CrossRef]
- Salas, J.; Scherrer, J.F.; Tuerk, P.; van den Berk-Clark, C.; Chard, K.M.; Schneider, F.D.; Schnurr, P.P.; Friedman, M.J.; Norman, S.B.; Cohen, B.E.; et al. Large posttraumatic stress disorder improvement and antidepressant medication adherence. J. Affect. Disord. 2020, 260, 119–123. [Google Scholar] [CrossRef]
- Kirk, M.N.; Zubek, D. Adherence challenges and long-acting injectable antipsychotic treatment in patients with schizophrenia. J. Psychosoc. Nurs. Ment. Health Serv. 2013, 51, 13–18. [Google Scholar] [CrossRef]
- Gültekin, A.; Kavak Budak, F. Does Spiritual Well-Being Affect Medication Adherence in Individuals Diagnosed with Mental Illness in Turkey? J. Relig. Health 2022, 61, 64–78. [Google Scholar] [CrossRef]
- Buchman-Wildbaum, T.; Váradi, E.; Schmelowszky, Á.; Griffiths, M.D.; Demetrovics, Z.; Urbán, R. Targeting the problem of treatment non-adherence among mentally ill patients: The impact of loss, grief and stigma. Psychiatry Res. 2020, 290, 113140. [Google Scholar] [CrossRef]
- Hernandez, M.; Barrio, C. Families and medication use and adherence among Latinos with schizophrenia. J. Ment. Health 2017, 26, 14–20. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, S.; Pavalur, R.; Thanapal, S.; Parathasarathy, N.B.; Desai, G.; Bhola, P.; Philip, M.; Chaturvedi, S.K. Medication Adherence, Work Performance and Self-Esteem among Psychiatric Patients Attending Psychosocial Rehabilitation Services at Bangalore, India. Indian J. Psychol. Med. 2014, 36, 392–396. [Google Scholar] [CrossRef] [Green Version]
- Corrigan, P.W.; Angell, B.; Davidson, L.T.; Marcus, S.C.; Salzer, M.S.; Kottsieper, P.; Larson, J.E.; Mahoney, C.A.; O’Connell, M.J.; Stanhope, V.L. From adherence to self-determination: Evolution of a treatment paradigm for people with serious mental illnesses. Psychiatr. Serv. 2012, 63, 169–173. [Google Scholar] [CrossRef]
- Gault, I.; Gallagher, A.; Chambers, M. Perspectives on medicine adherence in service users and carers with experience of legally sanctioned detention and medication: A qualitative study. Patient Prefer. Adherence 2013, 7, 787–799. [Google Scholar] [CrossRef] [Green Version]
- Monterroso, L.; Pierdevara, L.; Joaquim, N. Avaliação da adesão regime terapêutico dos utentes seguidos na consulta externa de psiquiatria do centro hospitalar barlavento algarvio. Rev. Port. Enferm. Saúde Ment. 2012, 7, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Bolkan, C.R.; Bonner, L.M.; Campbell, D.G.; Lanto, A.B.; Zivin, K.B.; Chaney, E.F.; Rubenstein, L.V. Family involvement, medication adherence, and depression outcomes among patients in veterans affairs primary care. Psychiatr. Serv. 2013, 64, 472–478. [Google Scholar] [CrossRef]
- Lam, W.Y.; Fresco, P. Medication Adherence Measures: An Overview. BioMed Res. Int. 2015, 2015, 217047. [Google Scholar] [CrossRef] [Green Version]
- Berntsen, G.R.; Yaron, S.; Chetty, M.; Canfield, C.F.; Ako-Egbe, L.; Phan, P.H.; Curran, C.P.; Castro, I.A. Person-centered care (PCC): The people’s perspective. Int. J. Qual. Health Care 2021, 33, ii23–ii26. [Google Scholar] [CrossRef]
- Miller, E.; Stanhope, V.; Restrepo-Toro, M.; Tondora, J. Person-centered planning in mental health: A transatlantic collaboration to tackle implementation barriers. Am. J. Psychiatr. Rehabil. 2017, 20, 251–267. [Google Scholar] [CrossRef] [Green Version]
- Poitras, M.E.; Maltais, M.E.; Bestard-Denommé, L.; Stewart, M.; Fortin, M. What are the effective elements in patient-centered and multimorbidity care? A scoping review. BMC Health Serv. Res. 2018, 18, 446. [Google Scholar] [CrossRef] [Green Version]
- Boardman, J.M.; Dave, S.B. Person-centred care and psychiatry: Some key perspectives. BJPsych. Int. 2020, 17, 65–68. [Google Scholar] [CrossRef]
- Tomaselli, G.; Buttigieg, S.C.; Rosano, A.; Cassar, M.; Grima, G. Person-Centered Care from a Relational Ethics Perspective for the Delivery of High Quality and Safe Healthcare: A Scoping Review. Front. Public Health 2020, 8, 44. [Google Scholar] [CrossRef] [Green Version]
- Vera San Juan, N.; Gronholm, P.C.; Heslin, M.; Lawrence, V.; Bain, M.; Okuma, A.; Evans-Lacko, S. Recovery from Severe Mental Health Problems: A Systematic Review of Service User and Informal Caregiver Perspectives. Front. Psychiatry 2021, 12, 712026. [Google Scholar] [CrossRef]
- Piat, M.; Wainwright, M.; Sofouli, E.; Vachon, B.; Deslauriers, T.; Préfontaine, C.; Frati, F. Factors influencing the implementation of mental health recovery into services: A systematic mixed studies review. Syst. Rev. 2021, 10, 134. [Google Scholar] [CrossRef]
- Hardcastle, S.J.; Hancox, J.; Hattar, A.; Maxwell-Smith, C.; Thøgersen-Ntoumani, C.; Hagger, M.S. Motivating the unmotivated: How can health behavior be changed in those unwilling to change? Front. Psychol. 2015, 6, 835. [Google Scholar] [CrossRef] [Green Version]
- Laranjeira, C.; Querido, A. Hope and Optimism as an Opportunity to Improve the “Positive Mental Health” Demand. Front. Psychol. 2022, 13, 827320. [Google Scholar] [CrossRef]
- McAllister, S.; Robert, G.; Tsianakas, V.; McCrae, N. Conceptualising nurse-patient therapeutic engagement on acute mental health wards: An integrative review. Int. J. Nurs. Stud. 2019, 93, 106–118. [Google Scholar] [CrossRef]
- Hartley, S.; Raphael, J.; Lovell, K.; Berry, K. Effective nurse-patient relationships in mental health care: A systematic review of interventions to improve the therapeutic alliance. Int. J. Nurs. Stud. 2020, 102, 103490. [Google Scholar] [CrossRef]
- Cutler, R.L.; Fernandez-Llimos, F.; Frommer, M.; Benrimoj, C.; Garcia-Cardenas, V. Economic impact of medication non-adherence by disease groups: A systematic review. BMJ Open 2018, 8, e016982. [Google Scholar] [CrossRef] [Green Version]
- Byrne, S.; Solomon Hart, P. The Boomerang Effect A Synthesis of Findings and a Preliminary Theoretical Framework. Ann. Int. Commun. Assoc. 2009, 33, 3–37. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laranjeira, C.; Carvalho, D.; Valentim, O.; Moutinho, L.; Morgado, T.; Tomás, C.; Gomes, J.; Querido, A. Therapeutic Adherence of People with Mental Disorders: An Evolutionary Concept Analysis. Int. J. Environ. Res. Public Health 2023, 20, 3869. https://doi.org/10.3390/ijerph20053869
Laranjeira C, Carvalho D, Valentim O, Moutinho L, Morgado T, Tomás C, Gomes J, Querido A. Therapeutic Adherence of People with Mental Disorders: An Evolutionary Concept Analysis. International Journal of Environmental Research and Public Health. 2023; 20(5):3869. https://doi.org/10.3390/ijerph20053869
Chicago/Turabian StyleLaranjeira, Carlos, Daniel Carvalho, Olga Valentim, Lídia Moutinho, Tânia Morgado, Catarina Tomás, João Gomes, and Ana Querido. 2023. "Therapeutic Adherence of People with Mental Disorders: An Evolutionary Concept Analysis" International Journal of Environmental Research and Public Health 20, no. 5: 3869. https://doi.org/10.3390/ijerph20053869