
Evaluation of Correlation between Sleep and Psychiatric Disorders in a Population of Night Shift Workers: A Pilot Study

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assessment of Sleep Disorders
2.3. Statistical Analysis
3. Results
3.1. Insomnia Disorders in the General Population
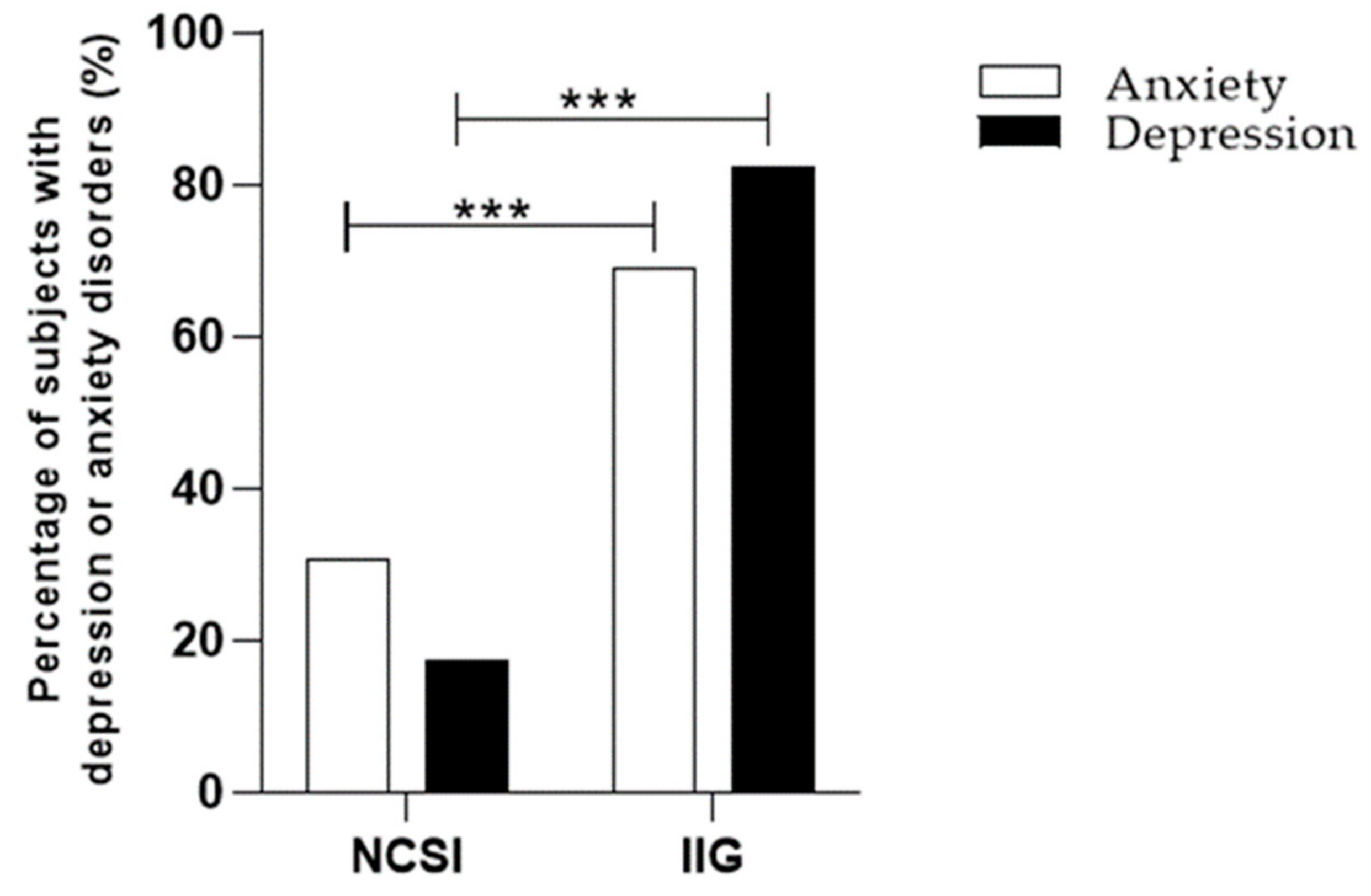
3.2. Association between Sleep Disorders and Psychiatric Disorders
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bhaskar, S.; Hemavathy, D.; Prasad, S. Prevalence of chronic insomnia in adult patients and its correlation with medical comorbidities. J. Family Med. Prim. Care 2016, 5, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Roth, T. Insomnia: Definition, prevalence, etiology, and consequences. J. Clin. Sleep Med. 2007, 3 (Suppl. S5), S7–S10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plescia, F.; Cirrincione, L.; Martorana, D.; Ledda, C.; Rapisarda, V.; Castelli, V.; Martines, F.; Vinnikov, D.; Cannizzaro, E. Alcohol Abuse and Insomnia Disorder: Focus on a Group of Night and Day Workers. Int. J. Environ. Res. Public Health 2021, 18, 13196. [Google Scholar] [CrossRef] [PubMed]
- Plescia, F.; Brancato, A.; Venniro, M.; Maniaci, G.; Cannizzaro, E.; Sutera, F.M.; De Caro, V.; Giannola, L.I.; Cannizzaro, C. Acetaldehyde self-administration by a two-bottle choice paradigm: Consequences on emotional reactivity, spatial learning, and memory. Alcohol 2015, 49, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.N.; Zong, Q.Q.; Yang, Y.; Zhang, L.; Xiang, Y.F.; Ng, C.H.; Chen, L.G.; Xiang, Y.T. Gender Difference in the Prevalence of Insomnia: A Meta-Analysis of Observational Studies. Front. Psychiatry 2020, 11, 577429. [Google Scholar] [CrossRef]
- Miner, B.; Kryger, M.H. Sleep in the Aging Population. Sleep Med. Clin. 2017, 12, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Boivin, D.B. Influence of sleep-wake and circadian rhythm disturbances in psychiatric disorders. J. Psychiatry Neurosci. 2000, 25, 446–458. [Google Scholar]
- Khurshid, K.A. Comorbid Insomnia and Psychiatric Disorders: An Update. Innov. Clin. Neurosci. 2018, 15, 28–32. [Google Scholar]
- Taylor, D.J.; Lichstein, K.L.; Durrence, H.H.; Reidel, B.W.; Bush, A.J. Epidemiology of insomnia, depression, and anxiety. Sleep 2005, 28, 1457–1464. [Google Scholar] [CrossRef]
- Franzen, P.L.; Buysse, D.J. Sleep disturbances and depression: Risk relationships for subsequent depression and therapeutic implications. Dialogues Clin. Neurosci. 2008, 10, 473–481. [Google Scholar] [CrossRef]
- Turek, F.W. From circadian rhythms to clock genes in depression. Int. Clin. Psychopharmacol. 2007, 22 (Suppl. S2), S1–S8. [Google Scholar] [CrossRef]
- Li, J.; Covassin, N.; Bock, J.M.; Mohamed, E.A.; Pappoppula, L.P.; Shafi, C.; Lopez-Jimenez, F.; Somers, V.K. Excessive Daytime Sleepiness and Cardiovascular Mortality in US Adults: A NHANES 2005-2008 Follow-Up Study. Nat. Sci. Sleep 2021, 13, 1049–1059. [Google Scholar] [CrossRef]
- Olszowka, M.; Held, C.; Hadziosmanovic, N.; Denchev, S.; Manolis, A.; Wallentin, L.; White, H.D.; Stewart, R.A.H.; Hagström, E.; STABILITY Investigators. Excessive daytime sleepiness, morning tiredness and major adverse cardiovascular events in patients with chronic coronary syndrome. J. Int. Med. 2021, 290, 392–403. [Google Scholar] [CrossRef]
- Taylor, D.J.; Mallory, L.J.; Lichstein, K.L.; Durrence, H.H.; Riedel, B.W.; Bush, A.J. Comorbidity of chronic insomnia with medical problems. Sleep 2007, 30, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Foley, D.; Ancoli-Israel, S.; Britz, P.; Walsh, J. Sleep disorders and chronic disease in older adults: Results from the 2003 National Sleep Foundation Sleep in America Survey. J. Psychosom. Res. 2004, 56, 497–502. [Google Scholar] [CrossRef]
- Ballacchino, A.; Salvago, P.; Cannizzaro, E.; Costanzo, R.; Di Marzo, M.; Ferrara, S.; Mattina, E.L.; Messina, G.; Mucia, M.; Mule, L.; et al. Association between sleep-disordered breathing and hearing disorders: Clinical observation in Sicilian patients. ActaMed. Mediterr. 2015, 31, 607–614. [Google Scholar]
- Pace, A.; Iannella, G.; Rossetti, V.; Visconti, I.C.; Gulotta, G.; Cavaliere, C.; De Vito, A.; Maniaci, A.; Cocuzza, S.; Magliulo, G.; et al. Diagnosis of Obstructive Sleep Apnea in Patients with Allergic and Non-Allergic Rhinitis. Medicine 2020, 56, 454. [Google Scholar] [CrossRef]
- C171—Convention on Night Work, No. 171. International Labour Organisation (ILO): Geneva, Switzerland, 1990.
- Rajaratnam, S.M.; Arendt, J. Health in a 24-h society. Lancet 2001, 358, 999–1005. [Google Scholar] [CrossRef]
- Cannizzaro, E.; Cirrincione, L.; Mazzucco, W.; Scorciapino, A.; Catalano, C.; Ramaci, T.; Ledda, C.; Plescia, F. Night-Time Shift Work and Related Stress Responses: A study of security guards. Int. J. Environ. Res. Public Health 2020, 17, 562. [Google Scholar] [CrossRef] [Green Version]
- Angarita, G.A.; Emadi, N.; Hodges, S.; Morgan, P.T. Sleep abnormalities associated with alcohol, cannabis, cocaine, and opioid use: A comprehensive review. Addict. Sci. Clin. Pract. 2016, 11, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramaci, T.; Barattucci, M.; Vella, F.; Senia, P.; Cannizzaro, E.; Scorciapino, A.; Ledda, C.; De Giorgio, A.; Rapisarda, V. Straining at Work and Its Relationship with Personality Profiles and Individual Consequences in Healthcare Workers (HCWs). Int. J. Environ. Res. Public Health 2020, 17, 610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Puttonen, S.; Härmä, M.; Hublin, C. Shift work and cardiovascular disease—Pathways from circadian stress to morbidity. Scand. J. Work Env. Health 2010, 36, 96–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastille-Denis, E.; Lemyre, A.; Pappathomas, A.; Roy, M.; Vallières, A. Are cognitive variables that maintain insomnia also involved in shift work disorder? Sleep Health 2020, 6, 399–406. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Harvey, A.G.; Tang, N.K. (Mis)perception of sleep in insomnia: A puzzle and a resolution. Psychol. Bull. 2012, 138, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Seo, J.E.; Pace-Schott, M.R.; Milad, H.; Song, A. Germain The association of insomnia with anxiety disorders and depression: Exploration of the direction of risk. Biol Psychiatr.: Cognit Neurosci. Neuroimag. 2021, 6, 299–309. [Google Scholar]
- Gujar, N.; Yoo, S.S.; Hu, M.P. Walker Sleep deprivation amplifies reactivity of brain reward networks, biasing the appraisal of positive emotional experiences. J. Neurosci. 2011, 31, 4466–4474. [Google Scholar] [CrossRef] [Green Version]
- Simon, E.B.; Oren, N.; Sharon, H.; Kirschner, A.; Goldway, N.; Okon-Singer, H.; Tauman, R.; Deweese, M.M.; Keil, A.; Hendler, T. Losing Neutrality: The Neural Basis of Impaired Emotional Control without Sleep. J. Neurosci. 2015, 35, 13194–13205. [Google Scholar] [CrossRef] [Green Version]
- Yoo, S.S.; Gujar, N.; Hu, P.; Jolesz, F.A.; Walker, M.P. The human emotional brain without sleep-a prefrontal amygdala disconnect. Curr. Biol. 2007, 17, R877–R878. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, J.; Ding, F.; Nedergaard, M. Distinct functional states of astrocytes during sleep and wakefulness: Is norepinephrine the master regulator? Curr. Sleep Med. Rep. 2015, 1, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Pace-Schott, E.F.; Germain, A.; Milad, M.R. Sleep and REM sleep disturbance in the pathophysiology of PTSD: The role of extinction memory. Biol. Mood. Anxiety Disord. 2015, 5, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Straus, L.D.; Acheson, D.T.; Risbrough, V.B.; Drummond, S.P.A. Sleep Deprivation Disrupts Recall of Conditioned Fear Extinction. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2017, 2, 123–129. [Google Scholar] [CrossRef] [Green Version]
- Straus, L.D.; Drummond, S.P.A.; Risbrough, V.B.; Norman, S.B. Sleep Disruption, Safety Learning, and Fear Extinction in Humans: Implications for Posttraumatic Stress Disorder. Curr. Top Behav. Neurosci. 2018, 38, 193–205. [Google Scholar] [CrossRef]
- Clinton, J.M.; Davis, C.J.; Zielinski, M.R.; Jewett, K.A.; Krueger, J.M. Biochemical regulation of sleep and sleep biomarkers. J. Clin. Sleep Med. 2011, 7 (Suppl. S5), S38–S42. [Google Scholar] [CrossRef] [Green Version]
- Richtand, N.R. McNamara Serotonin and dopamine interactions in psychosis prevention. Prog. Brain Res. 2008, 172, 141–153. [Google Scholar]
- Benarroch, E.E. Locus coeruleus. Cell Tissue Res. 2018, 373, 221–232. [Google Scholar] [CrossRef]
- Wafford, K.A.; Ebert, B. Emerging anti-insomnia drugs: Tackling sleeplessness and the quality of wake time. Nat. Rev. Drug Discov. 2008, 7, 530–540. [Google Scholar] [CrossRef]
- Benarroch, E.E. The locus ceruleus norepinephrine system: Functional organisation and potential clinical significance. Neurology 2009, 73, 1699–1704. [Google Scholar] [CrossRef]
- Bremner, J.D.; Krystal, J.H.; Southwick, S.M.; Charney, D.S. Noradrenergic mechanisms in stress and anxiety: I. Preclinical studies. Synapse 1996, 23, 28–38. [Google Scholar] [CrossRef]
- Bremner, J.D.; Krystal, J.H.; Southwick, S.M.; Charney, D.S. Noradrenergic mechanisms in stress and anxiety: II. Clinical studies. Synapse 1996, 23, 39–51. [Google Scholar] [CrossRef]
- Albert, P.R.; Benkelfat, C.; Descarries, L. The neurobiology of depression--revisiting the serotonin hypothesis. I. Cellular and molecular mechanisms. Philos. Trans. R. Soc. Lond B. Biol. Sci. 2012, 367, 2378–2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahar, I.; Bambico, F.R.; Mechawar, N.; Nobrega, J.N. Stress, serotonin, and hippocampal neurogenesis in relation to depression and antidepressant effects. Neurosci. Biobehav. Rev. 2014, 38, 173–192. [Google Scholar] [CrossRef] [PubMed]
- Daut, R.A.; Fonken, L.K. Circadian regulation of depression: A role for serotonin. Front. Neuroendocrinol. 2019, 54, 100746. [Google Scholar] [CrossRef] [PubMed]
- Denoyer, M.; Sallanon, M.; Kitahama, K.; Aubert, C.; Jouvet, M. Reversibility of para-chlorophenylalanine-induced insomnia by intrahypothalamic microinjection of L-5-hydroxytryptophan. Neuroscience 1989, 28, 83–94. [Google Scholar] [CrossRef]
- Sangare, A.; Dubourget, R.; Geoffroy, H.; Gallopin, T.; Rancillac, A. Serotonin differentially modulates excitatory and inhibitory synaptic inputs to putative sleep-promoting neurons of the ventrolateral preoptic nucleus. Neuropharmacology 2016, 109, 29–40. [Google Scholar] [CrossRef]
- Bunney, B.G.; Li, J.Z.; Walsh, D.M.; Stein, R.; Vawter, M.P.; Cartagena, P.; Barchas, J.D.; Schatzberg, A.F.; Myers, R.M.; Watson, S.J.; et al. Circadian dysregulation of clock genes: Clues to rapid treatments in major depressive disorder. Mol. Psychiatry 2015, 20, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Bedrosian, T.A.; Nelson, R.J. Timing of light exposure affects mood and brain circuits. Transl. Psychiatry 2017, 7, e1017. [Google Scholar] [CrossRef] [Green Version]
- Buoli, M.; Grassi, S.; Caldiroli, A.; Carnevali, G.S.; Mucci, F.; Iodice, S.; Cantone, L.; Pergoli, L.; Bollati, V. Is there a link between air pollution and mental disorders? Environ. Int. 2018, 118, 154–168. [Google Scholar] [CrossRef]
- Glass, J.D.; Randolph, W.W.; Ferreira, S.A.; Rea, M.A.; Hauser, U.E.; Blank, J.L.; De Vries, M.J. Diurnal variation in 5-hydroxyindole-acetic acid output in the suprachiasmatic region of the Siberian hamster assessed by in vivo microdialysis: Evidence for nocturnal activation of serotonin release. Neuroendocrinology 1992, 56, 582–590. [Google Scholar] [CrossRef]
- Ushijima, K.; Sakaguchi, H.; Sato, Y.; To, H.; Koyanagi, S.; Higuchi, S.; Ohdo, S. Chronopharmacological study of antidepressants in forced swimming test of mice. J. Pharmacol. Exp. Ther. 2005, 315, 764–770. [Google Scholar] [CrossRef] [Green Version]
- Ushijima, K.; Koyanagi, S.; Sato, Y.; Ogata, T.; Matsunaga, N.; Fujimura, A.; Ohdo, S. Role of activating transcription factor-4 in 24-h rhythm of serotonin transporter expression in the mouse midbrain. Mol. Pharmacol. 2012, 82, 264–270. [Google Scholar] [CrossRef]
- Butler, A.C.; Chapman, J.E.; Forman, E.M.; Beck, A.T. The empirical status of cognitive-behavioral therapy: A review of meta-analyses. Clin. Psychol. Rev. 2006, 26, 17–31. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, M.B.; Cimino, C.R.; Benitez, A.; Brown, C.L.; Gibbons, L.E.; Kennison, R.F.; Shirk, S.D.; Atri, A.; Robitaille, A.; Macdonald, S.W.; et al. Cognitively Stimulating Activities: Effects on Cognition across Four Studies with up to 21 Years of Longitudinal Data. J. Aging Res. 2012, 2012, 461592. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| A | ||||
|---|---|---|---|---|
| n° | % | Insomnia Severity Index Mean | 95% CI | |
| EVIL | 222 | 100 | 5.955 | 5.212–6.698 |
| No clinically significant insomnia | 163 | 73.42 | 3.08 | 2.747–3.413 |
| Subthreshold insomnia | 35 | 15.77 | 10.74 | 10.13–11.35 |
| Moderate insomnia | 19 | 8.56 | 17.37 | 16.43–18.31 |
| Severe insomnia | 5 | 2.25 | 22.80 | 21.76–23.84 |
| B | ||||
| n° | % | Insomnia Severity Index Mean | 95% CI | |
| FEMALE | 191 | 100 | 6.984 | 6.099–7.869 |
| No clinically significant insomnia | 129 | 67.54 | 3.287 | 2.894–3.680 |
| Subthreshold insomnia | 32 | 16.75 | 11.06 | 10.43–11.70 |
| Moderate insomnia | 24 | 12.57 | 17.38 | 16.56–18.19 |
| Severe insomnia | 6 | 3.14 | 23.17 | 21.49–24.85 |
| No Psychiatric Disorder | Anxiety | Depression | |
|---|---|---|---|
| Total Sample Size (n = 413) | n° (%) | n° (%) | n° (%) |
| No clinically significant Insomnia (n = 292) | 275 (94.18) | 13 (4.45) | 4 (1.37) |
| Insomnia in general (n = 121) | 73 (60.33) | 29 (23.97) | 19 (15.70) |
| Subthreshold insomnia (n = 67) | 49 (73.13) | 11 (16,42) | 7 (10.44) |
| Moderate insomnia (n = 43) | 20 (46.51) | 14 (32.56) | 9 (20.93) |
| Severe insomnia (n = 11) | 4 (36.36) | 4 (36.36) | 3 (27.27) |
| Anxiety | Depression | |||
|---|---|---|---|---|
| Odds Ratio | 95% CI | Odds Ratio | 95% CI | |
| Insomnia in general | 8.404 | 4.11–16.73 | 17.89 | 5.966–49.42 |
| Subthreshold insomnia | 4.749 | 2.086–11.43 | 9.821 | 2.946–30.58 |
| Moderate insomnia | 14.81 | 5.905–34.08 | 30.94 | 8.287–94.46 |
| Severe insomnia | 21.15 | 5.485–76.92 | 51.56 | 9.687–304.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirrincione, L.; Plescia, F.; Malta, G.; Campagna, M.; Lecca, L.I.; Skerjanc, A.; Carena, E.; Baylon, V.; Theodoridou, K.; Fruscione, S.; et al. Evaluation of Correlation between Sleep and Psychiatric Disorders in a Population of Night Shift Workers: A Pilot Study. Int. J. Environ. Res. Public Health 2023, 20, 3756. https://doi.org/10.3390/ijerph20043756
Cirrincione L, Plescia F, Malta G, Campagna M, Lecca LI, Skerjanc A, Carena E, Baylon V, Theodoridou K, Fruscione S, et al. Evaluation of Correlation between Sleep and Psychiatric Disorders in a Population of Night Shift Workers: A Pilot Study. International Journal of Environmental Research and Public Health. 2023; 20(4):3756. https://doi.org/10.3390/ijerph20043756
Chicago/Turabian StyleCirrincione, Luigi, Fulvio Plescia, Ginevra Malta, Marcello Campagna, Luigi Isaia Lecca, Alenka Skerjanc, Elisa Carena, Vincenzo Baylon, Kelly Theodoridou, Santo Fruscione, and et al. 2023. "Evaluation of Correlation between Sleep and Psychiatric Disorders in a Population of Night Shift Workers: A Pilot Study" International Journal of Environmental Research and Public Health 20, no. 4: 3756. https://doi.org/10.3390/ijerph20043756