

Assessment of Patient Treatment and Rehabilitation Processes Using Electromyography Signals and Selected Industry 4.0 Solutions
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials 1. Applicable Treatment and Rehabilitation Processes for a Patient with a Musculoskeletal Injury
2.2. Materials 2. EMG Signal in the Treatment and Rehabilitation of Patients with a Musculoskeletal Condition
- Electroencephalography (EEG);
- Electromyography (EMG);
- Electrooculography (EOG);
- Electrogastrography (EGG).
- Biological signals can be divided according to their source into [11]:
- Bioelectrical (ECG, EEG, EMG);
- Bioimpedance (tissue impedance measurement);
- Bioacoustic (voice, heart sounds);
- Biomagnetic (measurement of the magnetic field generated by internal organs, e.g., the brain, heart, lungs);
- Biomechanical (musculoskeletal diagnosis, mechanical heart rate);
- Bio-optical (e.g., oximetry), other (e.g., spirometry).
- A signal processor connected between the surface myoelectric sensor and the signal transmitter;
- An electrode sensor, a signal amplification circuit connected to the electrode sensor and a signal connected to the signal amplification circuit. The circuit and the signal smoothing circuit are connected to the signal full-wave rectifying circuit;
- The electrode sensor includes a reference electrode, a muscle intermediate electrode and a muscle end electrode;
- The signal processor contains an A/D converter and a digital signal processor, and the A/D converter is connected to the connector of the digital signal processor;
- A remote monitor coupled to the renderer and configured to receive feedback from the renderer.
2.3. Materials 3. Industry 4.0 Tools in the New Treatment and Rehabilitation Processes for Patients with a Musculoskeletal Injury
- Identifying patients who could benefit from the potential good effects of the drugs being tested;
- Qualifying patients for medical treatment and rehabilitation based on the urgency of needs;
- Monitoring the progress of treatment and rehabilitation.
2.4. Methods. Research Methodology for Evaluating the Treatment and Rehabilitation Processes for a Patient with a Musculoskeletal Injury
- The analysis of the medical records of the patients to classify them for the study and to clarify the possible course of treatment and rehabilitation processes for the patients with a selected disease entity;
- Diagnostic survey, technique: questionnaire, research tool: survey questionnaire completed face-to-face by an interviewer.
- Wilden et al. (2016), who suggested measuring risks [36].
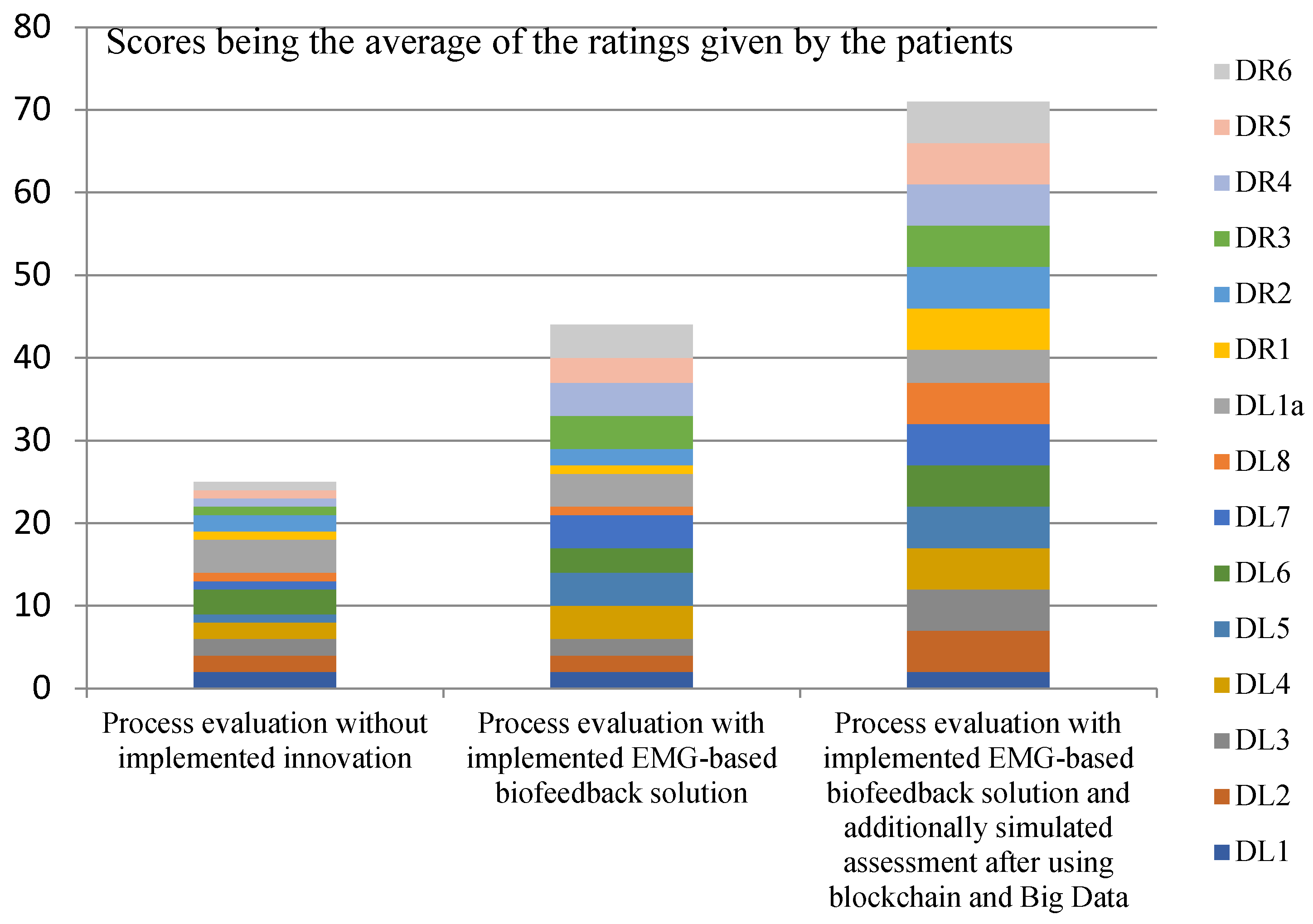
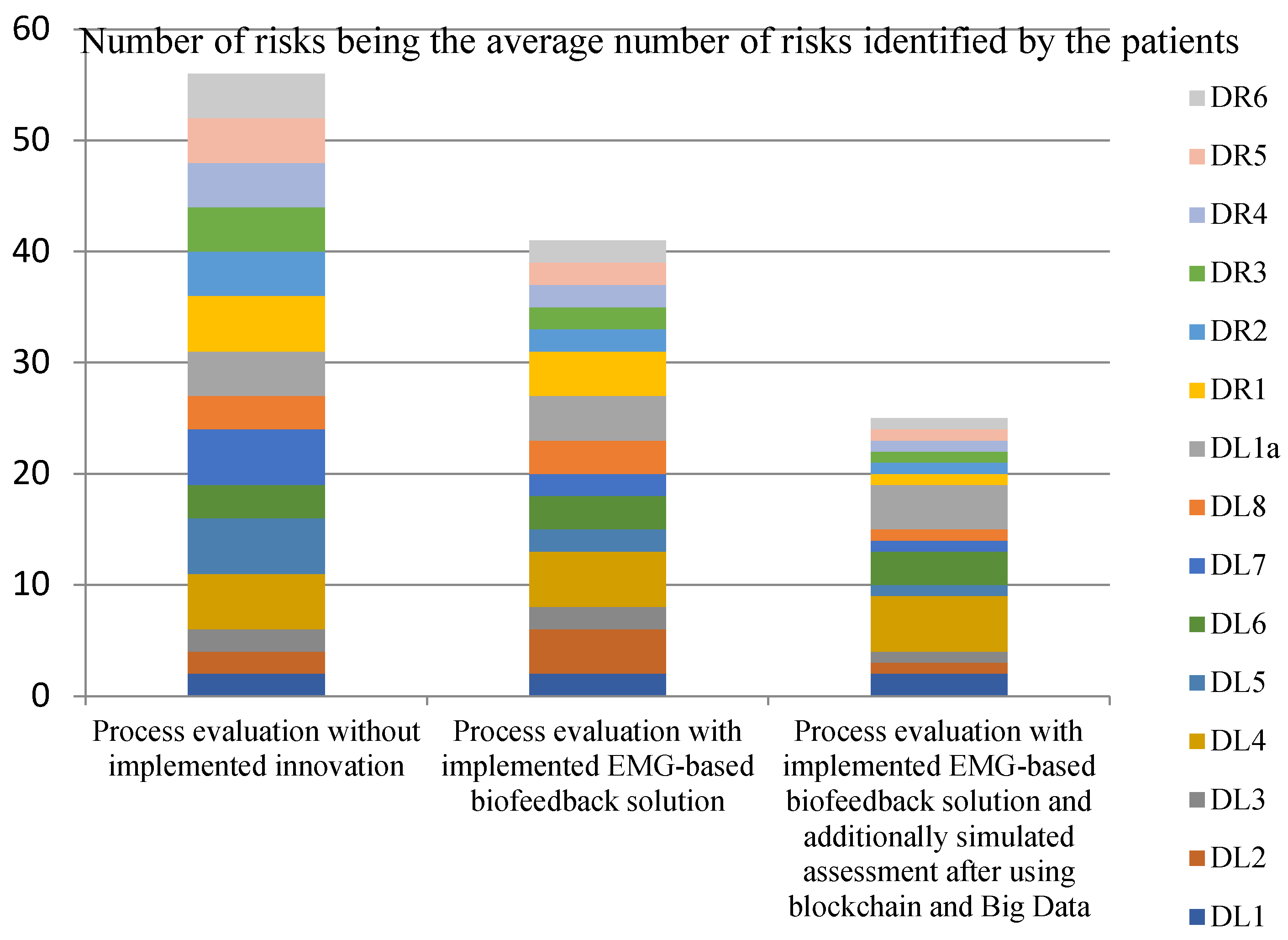
3. Results
- Efficiency (measures: the costs incurred by the insurer and the patient in the treatment and rehabilitation processes, and the number of risks affecting the efficiency of the processes);
- Effectiveness (measures: creation of values for the patient’s physical and mental health, and number of risks that also affect the patient’s health).
4. Discussion
- Diagnostic problems in patients with co-morbidities or diseases acquired during treatment of the underlying injury (e.g., neurological diseases, cardiovascular diseases).
- Doubts/discussions regarding the diagnosis of the interdisciplinary case conference.
- Doubts/discussions regarding the use of preoperative rehabilitation.
- Delegation of tasks/problems with designating medical or rehabilitation staff.
- Patient doubts about the treatment given/lack of full internal patient involvement.
- Long, uncoordinated postoperative recovery period/overdue rehabilitation appointments.
- Necessity of repeating diagnostic evaluation and return to the treatment process.
- Error in choosing a rehabilitation facility that does not specialise in treating the condition.
- Lack of progress in recovery at the health facility chosen by patient/poor atmosphere/lack of empathy.
- Strain during rehabilitation.
- Unexpected/unwanted emotional problems in social, occupational and psychological rehabilitation.
- Willingness to change the rehabilitation facility during the project.
- Numerous changes in the composition of consulting physicians who monitor the results of treatment and rehabilitation.
- In rehabilitation, scheduled hours and appointments reimbursed by the insurer were overrun.
- Unclear, restrictive attitude towards the patient/lack of standardisation of patient management.
- Incomplete access to critical information regarding payments by the insurer.
- Relapse of the formally cured disease.
- Problems with e-rehabilitation devices, their lack/lack of funding, problems with the communication interface.
- Lack of staff to remotely monitor the convalescent’s progress.
- Transparency/standardisation of data on rehabilitation services, assessment of rehabilitation and post-rehabilitation effectiveness, assessment of rehabilitation facilities, assessments of individual rehabilitation services.
- The effortfulness associated with the need to describe the cases of rehabilitation patients, the time delays involved, the high error rate, the high labour costs, the lack of standardisation of the documents prepared.
- Privacy, which is more difficult to provide in a rehabilitation facility. Original documents are available to numerous staff members.
5. Conclusions
- Universality—assuming that everyone has the right to rehabilitation, regardless of diagnosis, age or prognosis;
- Earliness—starting rehabilitation at the earliest possible stage, from the first day in hospital;
- Comprehensiveness—comprehensive coordinated actions carried out by a team of specialists, targeting all levels of the person’s life and responding to his/her individual needs;
- Continuity—the systematic provision of rehabilitation interventions and continuing them for as long as a given person needs them.
- Prepare for situation assessment;
- Collect data and information;
- Conduct assessment in the country;
- Write, revise and finalise report, disseminate and communicate findings;
- Prepare for strategic planning;
- Consult, revise, finalise and complete costing of plan;
- Identify priorities and produce first draft of plan;
- Endorse and disseminate the strategic plan;
- Develop monitoring framework with indicators, baselines and targets;
- Establish evaluation and review processes;
- Establish a recurring implementation “plan, do, evaluate” cycle;
- Increase capacity of rehabilitation leadership and governance (Figure 1).
- Focusing on patients by keeping detailed records of their health status;
- Digitising treatment and rehabilitation information.
- Online medical and rehabilitation appointment scheduling, etc.;
- Reducing data storage costs;
- Storing and sharing data that increasingly contribute to the efficiency of treatment and rehabilitation processes [28];
- Reducing costs for individual patients, which is particularly important for patients with reduced mobility or who live far from health centres [12].
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kujawa, J. Comprehensive rehabilitation after total hip and knee arthroplasty. Eur. J. Phys. Rehabil. Med. 2016, 52, 741–752. [Google Scholar]
- Xu, Y.Y.; Li, S.L.; Ma, C.M. A big data of rehabilitation process management based on block chain. IOP Conference Series: Earth and Environmental Science. In Proceedings of the 2020 International Conference on Advances in Biological Science and Technology, Sanya, China, 28–30 October 2020; Volume 707. [Google Scholar] [CrossRef]
- Yen, J.M.; Lim, J.H. A Clinical Perspective on Bespoke Sensing Mechanisms for Remote Monitoring and Rehabilitation of Neurological Diseases: Scoping Review. Sensors 2023, 23, 536. [Google Scholar] [CrossRef] [PubMed]
- Nawari, O.N.; Shriraam, R. Blockchain and the built environment: Potentials and limitations. J. Build. Eng. 2019, 25, 100832. [Google Scholar] [CrossRef]
- Krawiecki, Z.; Jędrych, B. Computer measurement station with rld system for electromyographic signal acquisition, Poznan University of Technology. Acad. J. 2019, 100, 51–61. [Google Scholar]
- Fang, C.; He, B.; Wang, Y.; Cao, J.; Gao, S. EMG-Centered Multisensory Based Technologies for Pattern Recognition in Rehabilitation: State of the Art and Challenges. Biosensors 2020, 10, 85. [Google Scholar] [CrossRef]
- Hong, Y.; Wang, B.; Lin, W.; Jin, L.; Liu, S.; Luo, X.; Pan, J.; Wang, W.; Yang, Z. Highly anisotropic and flexible piezoceramic kirigami for preventing joint disorders. Sci. Adv. 2021, 7, eabf0795. [Google Scholar] [CrossRef]
- Kim, J.; Campbell, A.S.; de Ávila, B.E.-F.; Wang, J. Wearable biosensors for healthcare monitoring. Nat. Biotechnol. 2019, 37, 389–406. [Google Scholar] [CrossRef]
- Hutting, N.; Caneiro, J.; Ong’Wen, O.M.; Miciak, M.; Roberts, L. Patient-centered care in musculoskeletal practice: Key elements to support clinicians to focus on the person. Musculoskelet. Sci. Pract. 2022, 57, 102434. [Google Scholar] [CrossRef]
- Frigo, G.; Crenna, P. Multichannel SEMG in clinical gait analysis: A review and state-of-the-art. Clin. Biomech. 2009, 24, 236–245. [Google Scholar] [CrossRef]
- Pereira, A.; Folgado, D.; Nunes, F.; Almeida, J.; Sousa, I. Using inertial sensors to evaluate exercise correctness inelectromyography-based home rehabilitation systems. In Proceedings of the 2019 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Istanbul, Turkey, 26–28 June 2019. [Google Scholar]
- Giggins, O.M.; Persson, U.M.; Caulfield, B. Biofeedback in rehabilitation. J. Neuroeng. Rehabil. 2013, 10, 60. [Google Scholar] [CrossRef] [Green Version]
- Giggins, O.M.; Sweeney, K.T.; Caulfield, B. Rehabilitation exercise assessment using inertial sensors: A cross-sectional analytical study. J. Neuroeng. Rehabil. 2014, 11, 158. [Google Scholar] [CrossRef] [Green Version]
- Rhim, H.; Lee, J.; Lee, S.; Jeon, J.; Kim, G.; Lee, K.; Jang, K.-M. Supervised Rehabilitation May Lead to Better Outcome than Home-Based Rehabilitation Up to 1 Year after Anterior Cruciate Ligament Reconstruction. Medicina 2020, 57, 19. [Google Scholar] [CrossRef]
- Ross, S.E.; Linens, S.W.; Wright, C.J.; Arnold, B.L. Balance assessments for predicting functional ankle instability and stable ankles. Gait Posture 2011, 34, 539–542. [Google Scholar] [CrossRef]
- Hibbs, A.; Thompson, K.; French, D.; Hodgson, D.; Spears, I. Peak and average rectified EMG measures: Which method of data reduction should be used for assessing core training exercise? J. Electromyogr. Kinesiol. 2011, 21, 102–111. [Google Scholar] [CrossRef]
- Reaz, M.B.I.; Hussain, M.S.; Mohd-Yasin, F. Techniques of EMG signal analysis: Detection, processing, classification and applications. Biol. Proced. Online 2006, 8, 11–35. [Google Scholar] [CrossRef] [Green Version]
- Clancy, E.A.; Bertolina, M.V.; Merletti, R.; Farina, D. Time- and frequency-domain monitoring of the myoelectric signal during a long-duration, cyclic, force-varying, fatiguing hand-grip task. J. Electromyogr. Kinesiol. 2008, 18, 789–797. [Google Scholar] [CrossRef]
- Payton, C.J.; Bartlett, R.M. Biomechanical Evaluation of Movement in Sport and Exercise: The British Association of Sport and Exercise Sciences Guide; Routledge: New York, NY, USA, 2008; pp. 77–103. [Google Scholar]
- Phinyomark, A.; Thongpanja, S.; Hu, H.; Phukpattaranont, P.; Limsakul, C. The Usefulness of Mean and Median Frequencies in Electromyography Analysis, Computational Intelligence in Electromyography Analysis—A Perspective on Current Applications and Future Challenges; Ganesh, R.N., Ed.; IntechOpen: London, UK, 2012. [Google Scholar]
- Van Gestel, L.; Wambacq, H.; Aertbeliën, E.; Meyns, P.; Bruyninckx, H.; Bar-On, L.; Molenaers, G.; De Cock, P.; Desloovere, K. To what extent is mean EMG frequency during gait a reflection of functional muscle strength in children with cerebral palsy? Res. Dev. Disabil. 2012, 33, 916–923. [Google Scholar] [CrossRef]
- Korkmaz, N.C.; Kirdi, N.; Temucin, C.M.; Armutlu, K.; Yakut, Y.; Karabudak, R. Improvement of muscle strength and fatigue with high voltage pulsed galvanic stimulation in multiple sclerosis patients—A non-randomized controlled trial. J. Pak. Med. Assoc. 2011, 61, 736. [Google Scholar]
- Olumide, M.; Danda, R.; Moses, G. Security through block vault in a blockchain enabled federated cloud framework. Appl. Netw. Sci. 2020, 5, 16. [Google Scholar] [CrossRef] [Green Version]
- Mitsutake, S.; Ishizaki, T.; Tsuchiya-Ito, R.; Uda, K.; Teramoto, C.; Shimizu, S.; Ito, H. Associations of Hospital Discharge Services with Potentially Avoidable Readmissions within 30 Days among Older Adults after Rehabilitation in Acute Care Hospitals in Tokyo, Japan. Arch. Phys. Med. Rehabil. 2020, 101, 832–840. [Google Scholar] [CrossRef] [Green Version]
- Alexander, B.; Shlomi, D.; Tal, H. Self-stabilizing Byzantine Consensus for Blockchain: (Brief Announcement). In Cyber Security Cryptography and Machine Learning; Springer: Berlin/Heidelberg, Germany, 2019; pp. 106–110. [Google Scholar] [CrossRef]
- Ottenbacher, K.J.; Graham, J.E.; Fisher, S.R. Data Science in Physical Medicine and Rehabilitation: Opportunities and Challenges. Phys. Med. Rehabil. Clin. N. Am. 2019, 30, 459–571. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Meng, L.; Zhou, H.; Xue, G. A Blockchain-Based Medical Data Sharing Mechanism with Attribute-Based Access Control and Privacy Protection, Privacy Protection and Incentive for AI-Driven IoT. Wirel. Commun. Mob. Comput. 2021, 2021, 6685762. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, A.; Xie, X.; Ye, X. Secure-aware and privacy-preserving electronic health record searching in cloud environment. Int. J. Commun. Syst. 2019, 32, e3925. [Google Scholar] [CrossRef]
- Meng, L.; Hong, X.; Chen, Y.; Ding, Y.; Zhang, C. K-Anonymous Privacy Preserving Scheme Based on Bilinear Pairings over Medical Data. In Proceedings of the International Conference on Wireless Algorithms, Systems, and Applications, Qingdao, China, 13–15 September 2020; Springer: Berlin/Heidelberg, Germany; pp. 381–393. [Google Scholar] [CrossRef]
- Gutenbrunner, C. White Book on Physical and Rehabilitation Medicine in Europe. Eur. Med. 2006, 42, 44. [Google Scholar]
- Wee, H.M.; Wu, S. The Lean supply chain and its impact on the cost and quality of the product: A case study on the motor car. Supply Chain Manag. Int. J. 2009, 14, 335–341. [Google Scholar] [CrossRef]
- Van Echtelt, F.E.A.; Wynstra, F.; van Weele, A.J.; Duysters, G. Managing Supplier Involvement in New Product Development: A Multiple-Case Study. J. Prod. Innov. Manag. 2008, 25, 180–201. [Google Scholar] [CrossRef] [Green Version]
- Eisenhardt, K.M.; Martin, J.A. Dynamic capabilities: What are they? Strateg. Manag. J. 2000, 21, 1105–1121. [Google Scholar] [CrossRef]
- Behrouzi, F.; Wong, K.Y. Research on supply chain performance measures in SMEs in the automotive industry. In Proceedings of the International IEEE Conference Devoted to Industrial Engineering and Engineering Management, Singapore, 6–9 December 2011. [Google Scholar]
- Wilden, R.; Gudergan, S.P. The impact of dynamic capabilities on operational marketing and technological capabilities: Investigating the role of environmental turbulence. J. Acad. Mark. Sci. 2016, 43, 181–199. [Google Scholar] [CrossRef]
- Gunasekaran, A.; Williams, H.; McGaughey, R. A system for measuring and calculating results in a new company. Technovation 2005, 25, 523–533. [Google Scholar] [CrossRef]
- Sundaresan, P.; Lunesu, L.G. A system and Method for Generating a Recovery Key and Managing Credentials Using a Blockchain Smart Contract. U.S. Patent 2,019,036,692, 1 June 2017. Available online: https://patents.google.com/patent/WO2019082100A1/en (accessed on 17 February 2023).
- Zadrapova, M.; Mrázková, E.; Janura, M.; Strycek, M.; Cerny, M. Influence of Rehabilitation Aid with Biofeedback on the Rehabilitation Process during Remote Home-Based Rehabilitation. Int. J. Environ. Res. Public Health 2022, 19, 9069. [Google Scholar] [CrossRef]
- Correia, F.D.; Nogueira, A.; Magalhães, I.; Guimarães, J.; Moreira, M.; Barradas, I.; Teixeira, L.; Tulha, J.; Seabra, R.; Lains, J.; et al. Home-based Rehabilitation with A Novel Digital Biofeedback System versus Conventional In-person Rehabilitation after Total Knee Replacement: A feasibility study. Sci. Rep. 2018, 8, 11299. [Google Scholar] [CrossRef] [Green Version]
- Fletcher, J.; Bartolucci, S. Computer-Implemented System and Method Providing a Decentralized Protocol for the Recovery of Cryptographic Assets. U.S. Patent 11,356,263, 20 December 2018. Available online: https://patents.justia.com/patent/11356263 (accessed on 17 February 2023).
- Domdouzis, K.; Lake, P.; Crowther, P. Distributed Databases. In Concise Guide to Databases. Undergraduate Topics in Computer Science; Springer: Cham, Switzerland, 2021. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Steps of Treatment and Rehabilitation Processes | Description of the Activity Performed during the Process Step |
|---|---|
| DL1: | Exploratory diagnosis and identification of specialists for consultation |
| DL2: | Case conference with a rehabilitation specialist |
| DL3: | Observation and preparation of the patient for surgery, including communicating treatment and management procedures and performance standards (core staff and medical psychologist) |
| DL4: | Hospitalisation—osteosynthesis |
| DL5: | Monitoring of treatment progress (sometimes using e-rehabilitation); return to DL1 if necessary |
| DL6: | Syndesmotic screw removal surgery |
| DL7: | Monitoring of treatment progress (sometimes using e-rehabilitation); return to DL1 or termination of the treatment process if necessary |
| DL8: | Completion of treatment and payment of benefits based on documents collected during the treatment process |
| DR1: | Scheduling appointments and recommendation of medical rehabilitation providers |
| DR2: | Monitoring of the medical rehabilitation progress (post-rehabilitation diagnostic evaluation including the use of e-rehabilitation devices) (return to DR1 if necessary) |
| DR3: | If necessary, scheduling appointments and recommendation of providers of social, occupational and psychological rehabilitation services |
| DR4: | Monitoring the progress of social and occupational rehabilitation |
| DL1a | Resumption of treatment/Hospitalisation—procedure to remove internal fixations |
| DR5 | Monitoring of the medical rehabilitation progress (post-rehabilitation diagnostic evaluation including use of e-rehabilitation devices) (return to DL1a if necessary) |
| DR6 | Completion of rehabilitation, health impairment price and compensation of benefits paid based on documents collected during the rehabilitation process. |
| Next Process Step | Duration of Step | Costs Incurred by the Insurer or the Patient (Own Costs Could Be Reimbursed by the Insurer) | Added Value Created | Number of Identified Risks | Activity Support Tools | |
|---|---|---|---|---|---|---|
| Value for Patient Physical Health Points 1–5 1—Lowest Score 5—Highest Score | Value for Patient Mental Health Points 1–5 1—Lowest Score 5—Highest Score | |||||
| DL1: | - | - | - | |||
| DL2: | - | - | - | |||
| DL3 | ||||||
| DL4 | ||||||
| DL5 | ||||||
| DL6 | ||||||
| DL7 | ||||||
| DL8 | ||||||
| DL1a | ||||||
| DR1 | ||||||
| DR2 | ||||||
| DR3 | ||||||
| DR4 | ||||||
| DR5 | ||||||
| DR6 | ||||||
| Total | Sum of money | Total points | Total points | Sum of risks | ||
| Process Step | Process Stakeholders’ Activities after Blockchain Application | Products of Various Steps of the Process after Blockchain and Big Data Implementation | ||
|---|---|---|---|---|
| Authentication centre | Health facilities as:
| Patient | ||
| DL1 | Archiving of documents | Preparation of documents | Acceptance of document availability Receipt of information | Determining the extent of treatment needs |
| DL2 | as above | as above | as above | Determining the extent of treatment needs and preoperative rehabilitation needs/inclusion of preoperative rehabilitation |
| DL3 | as above | as above | as above | Information provided by the patient on the hardship they have to endure to recover |
| DL4 | as above | as above | as above | Information to prepare the physician performing the procedure. Carrying out necessary treatment procedures |
| DL5 | as above | as above | as above | Coordinating follow-up visits based on the results of the patient’s remote devices that monitor patient health status. Setting necessary follow-up appointments and subsequent diagnostic measures |
| DL6 | as above | as above | as above | Information to prepare the physician performing the procedure. Carrying out necessary treatment procedures |
| DL7 | as above | as above | as above | Setting therapy appointments and rehabilitation therapy plan, online support of the patient in performing exercises |
| DL8 | as above | as above | as above | Comprehensive information for the insurer on the patient’s health status. Payment of benefit without patient involvement |
| DL1a | as above | as above | as above | Information to prepare the physician performing the procedure. Carrying out necessary treatment procedures |
| DR1 | as above | as above | as above | Suggesting alternative subproviders of medical rehabilitation services |
| DR2 | as above | as above | as above | Ongoing provision of information on health status and recovery progress, involvement of the patient in the self-rehabilitation process |
| DR3 | as above | as above | as above | Suggesting alternative subproviders of social, occupational and psychological rehabilitation services |
| DR4 | as above | as above | as above | Ongoing provision of information on health status and recovery progress, involvement of the patient in the self-rehabilitation process |
| DR5 | as above | as above | as above | Setting therapy appointments and rehabilitation therapy plan, online support of the patient in performing exercises |
| DR6 | as above | as above | as above | Comprehensive information for the insurer on the patient’s health status. Payment of benefit without patient involvement |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stawiarska, E.; Stawiarski, M. Assessment of Patient Treatment and Rehabilitation Processes Using Electromyography Signals and Selected Industry 4.0 Solutions. Int. J. Environ. Res. Public Health 2023, 20, 3754. https://doi.org/10.3390/ijerph20043754
Stawiarska E, Stawiarski M. Assessment of Patient Treatment and Rehabilitation Processes Using Electromyography Signals and Selected Industry 4.0 Solutions. International Journal of Environmental Research and Public Health. 2023; 20(4):3754. https://doi.org/10.3390/ijerph20043754
Chicago/Turabian StyleStawiarska, Ewa, and Maciej Stawiarski. 2023. "Assessment of Patient Treatment and Rehabilitation Processes Using Electromyography Signals and Selected Industry 4.0 Solutions" International Journal of Environmental Research and Public Health 20, no. 4: 3754. https://doi.org/10.3390/ijerph20043754