
Incidence and Duration of Sick Leave Due to Work-Related Musculoskeletal Disorders in the Accommodation and Food Services Activities Sector in Slovenia: A Nationwide 5-Year Observational Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Data Collection
2.2. Classification of Economic Activities
2.3. Data Analysis and Outcome Measures
3. Results
3.1. Workers in “Accommodation and Food Services Activities”
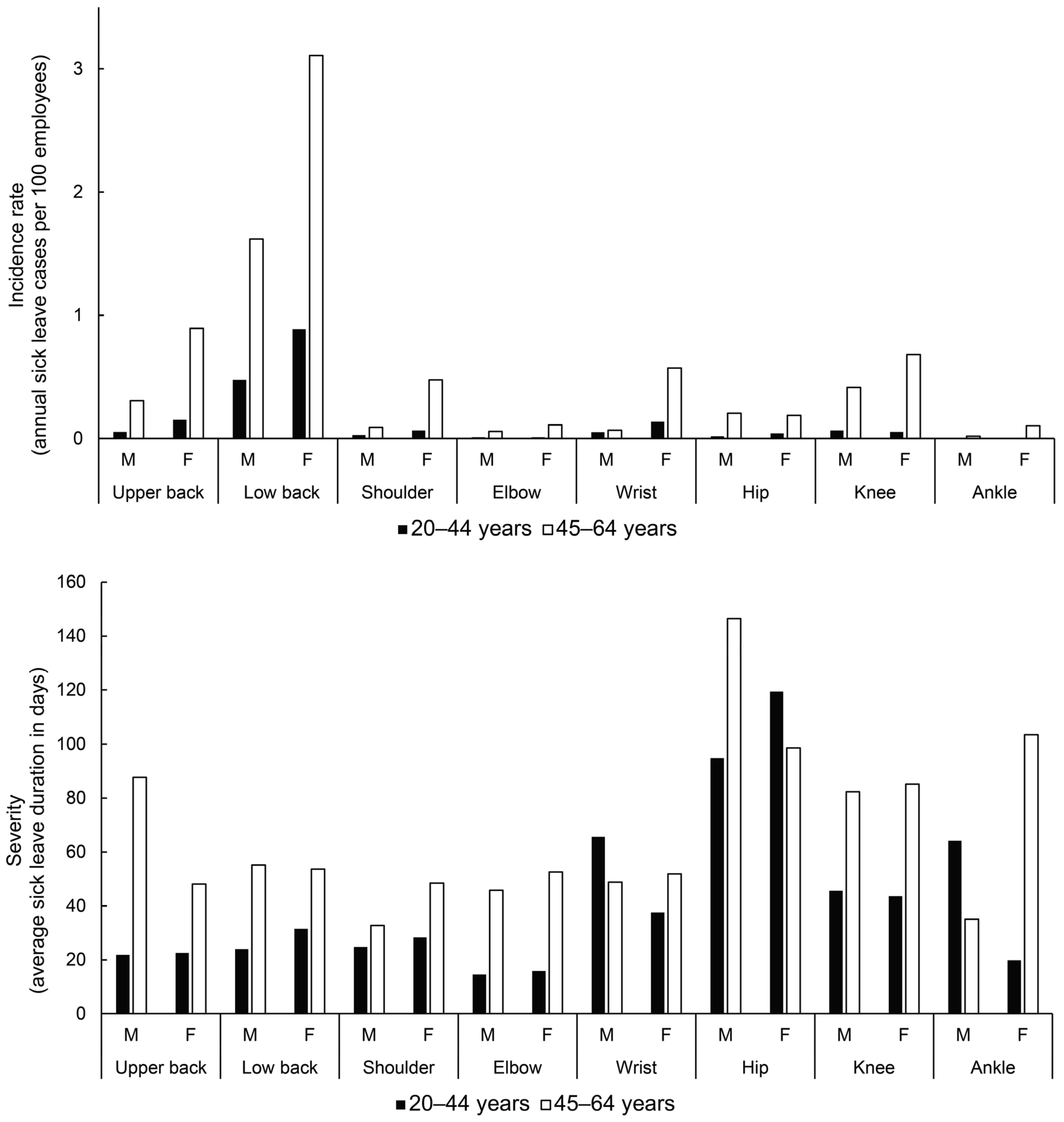
3.2. Sick Leave Incidence and Severity of the Most Common Work-Related Musculoskeletal Disorders in Sector I by Age, Gender and Body Region
3.3. Trends in Sick Leave Due to the Most Common Work-Related Musculoskeletal Disorders in Sector I from 2015 to 2019
3.4. Sick Leave Incidence and Severity of the Most Common Work-Related Musculoskeletal Disorders in Sector I Divisions
4. Discussion
4.1. Body-Site-Specific MSDs
4.2. Gender-Specific MSDs
4.3. Age-Specific MSDs
4.4. Division-Specific MSDs
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Agency for Safety and Health at Work. Work-Related Musculoskeletal Disorders: Prevalence, Costs and Demographics in the EU; EU: Bilbao, Spain, 2019. [Google Scholar]
- Wang, L.; Rosenman, K. Adverse Health Outcomes Among Industrial and Occupational Sectors in Michigan. Prev. Chronic Dis. 2018, 15, 170487. [Google Scholar] [CrossRef] [PubMed]
- Prijon, T. Zdravstveni Absentizem Zaradi z Delom Povezanih Kostno-Mišičnih Obolenj in Duševnih Stresnih Motenj v Sloveniji. Primerjalna Analiza Začasne Nezmožnosti Za Delo v Letih 2015 in 2019 v Okviru Projekta “Promocija Aktivnosti Za Preprečevanje Kostno-Mišičnih; Nacionalni Institut za Javno Zdravje: Ljubljana, Slovenia, 2020. [Google Scholar]
- Republic of Slovenia Statistical Office Persons in Employment by Activity (NACE Rev. 2), 5-Year Age Groups and Sex, Slovenia, Annually. Available online: https://pxweb.stat.si/SiStatData/pxweb/sl/Data/-/0764601S.PX (accessed on 26 January 2023).
- Chyuan, J.Y.A.; Du, C.L.; Yeh, W.Y.; Li, C.Y. Musculoskeletal Disorders in Hotel Restaurant Workers. Occup. Med. 2004, 54, 55–57. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, P.G.; Filiaggi, A.J. Cross-Sectional Investigation of Task Demands and Musculoskeletal Discomfort among Restaurant Wait Staff. Ergonomics 2006, 49, 93–106. [Google Scholar] [CrossRef]
- Peng, C.; Hsieh, H.; Li, M.; Liaw, L.; Wang, C.; Pan, C.; Wu, M. Gender Differences and Site-specific Incident Risks of Musculoskeletal Disorders among 224,506 Workers in the Food and Beverage Service Industry in Taiwan: A 15-year Nationwide Population-Based Cohort Study. J. Occup. Health 2021, 63, e12214. [Google Scholar] [CrossRef]
- Lee, J.W.; Lee, J.J.; Mun, H.J.; Lee, K.-J.; Kim, J.J. The Relationship between Musculoskeletal Symptoms and Work-Related Risk Factors in Hotel Workers. Ann. Occup. Environ. Med. 2013, 25, 20. [Google Scholar] [CrossRef]
- European Agency for Safety and Health at Work. Work-Related Musculoskeletal Disorders—Facts and Figures; EU: Bilbao, Spain, 2020. [Google Scholar]
- European Agency for Safety and Health at Work. Protecting Workers in Hotels, Restaurants and Catering; EU: Bilbao, Spain, 2008. [Google Scholar]
- European Agency for Safety and Health at Work. Musculoskeletal Disorders (MSDs) in HORECA; EU: Bilbao, Spain, 2008. [Google Scholar]
- European Agency for Safety and Health at Work. Musculoskeletal Disorders and Psychosocial Risk Factors in the Workplace—Statistical Analysis of EU-Wide Survey Data; EU: Bilbao, Spain, 2021. [Google Scholar]
- Zerbo Šporin, D.; Kozinc, Ž.; Prijon, T.; Šarabon, N. The Prevalence and Severity of Sick Leave Due to Low Back Disorders among Workers in Slovenia: Analysis of National Data across Gender, Age and Classification of Economic Activities. Int. J. Environ. Res. Public Health 2022, 19, 131. [Google Scholar] [CrossRef]
- Gheribi, E.; Bonadonna, A. An analysis of foodservice and accommodation industry in europe using secondary statistics. J. Posit. Manag. 2019, 9, 55. [Google Scholar] [CrossRef]
- Krause, N.; Scherzer, T.; Rugulies, R. Physical Workload, Work Intensification, and Prevalence of Pain in Low Wage Workers: Results from a Participatory Research Project with Hotel Room Cleaners in Las Vegas. Am. J. Ind. Med. 2005, 48, 326–337. [Google Scholar] [CrossRef]
- Gawde, N.C. A Study of Musculoskeletal Pain among Hotel Employees, India. J. Ecophysiol. Occup. Heal. 2018, 18, 44–51. [Google Scholar] [CrossRef]
- Shiue, H.; Lu, C.; Chen, C.; Shih, T.; Wu, S.; Yang, C.; Yang, Y.; Wu, T. Musculoskeletal Disorder among 52,261 Chinese Restaurant Cooks Cohort: Result from the National Health Insurance Data. J. Occup. Health 2008, 50, 163–168. [Google Scholar] [CrossRef] [Green Version]
- Tegenu, H.; Gebrehiwot, M.; Azanaw, J.; Akalu, T.Y. Self-Reported Work-Related Musculoskeletal Disorders and Associated Factors among Restaurant Workers in Gondar City, Northwest Ethiopia, 2020. J. Environ. Public Health 2021, 2021, 6082506. [Google Scholar] [CrossRef] [PubMed]
- Hubertsson, J.; Englund, M.; Hallgårde, U.; Lidwall, U.; Löfvendahl, S.; Petersson, I.F. Sick Leave Patterns in Common Musculoskeletal Disorders—A Study of Doctor Prescribed Sick Leave. BMC Musculoskelet. Disord. 2014, 15, 176. [Google Scholar] [CrossRef] [PubMed]
- Okunribido, O. Lower Limb MSD: Scoping Work to Help Inform Advice and Research Planning; Health and Safety Excutive: Norwich, UK, 2009. [Google Scholar]
- Park, J.; Kim, Y.; Han, B. Work Sectors with High Risk for Work-Related Musculoskeletal Disorders in Korean Men and Women. Saf. Health Work 2018, 9, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Choobineh, A.; Rajaeefard, A.; Neghab, M. Association between Perceived Demands and Musculoskeletal Disorders among Hospital Nurses of Shiraz University of Medical Sciences: A Questionnaire Survey. Int. J. Occup. Saf. Ergon. 2006, 12, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Le, T.K.; Montejano, L.B.; Cao, Z.; Zhao, Y.; Ang, D. Healthcare Costs Associated with Osteoarthritis in US Patients. Pain Pract. 2012, 12, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.D.; Pill, M.W. A Claims-Based View of Health Care Charges and Utilization for Commercially Insured Patients with Osteoarthritis. Manag. Care 2009, 18, 44–50. [Google Scholar]
- Coggon, D.; Ntani, G.; Palmer, K.T.; Felli, V.E.; Harari, R.; Barrero, L.H.; Felknor, S.A.; Gimeno, D.; Cattrell, A.; Serra, C.; et al. Disabling Musculoskeletal Pain in Working Populations: Is It the Job, the Person, or the Culture? Pain 2013, 154, 856–863. [Google Scholar] [CrossRef]
- Okunribido, O. Ageing and Work-Related Musculoskeletal Disorders: A Review of the Recent Literature; HSE: Buxton, UK, 2010. [Google Scholar]
- Okunribido, O.O.; Wynn, T.; Lewis, D. Are Older Workers at Greater Risk of Musculoskeletal Disorders in the Workplace than Young Workers?—A Literature Review. Occup. Ergon. 2011, 10, 53–68. [Google Scholar] [CrossRef]
- Postler, A.; Luque Ramos, A.; Goronzy, J.; Günther, K.P.; Lange, T.; Schmitt, J.; Zink, A.; Hoffmann, F. Prevalence and Treatment of Hip and Knee Osteoarthritis in People Aged 60 Years or Older in Germany: An Analysis Based on Health Insurance Claims Data. Clin. Interv. Aging 2018, 13, 2339–2349. [Google Scholar] [CrossRef]
- Ferguson, R.J.; Palmer, A.J.; Taylor, A.; Porter, M.L.; Malchau, H.; Glyn-Jones, S. Hip Replacement. Lancet 2018, 392, 1662–1671. [Google Scholar] [CrossRef]
- Günther, K.P.; Deckert, S.; Lützner, C.; Lange, T.; Schmitt, J.; Postler, A. Total Hip Replacement for Osteoarthritis—Evidence-Based and Patient-Oriented Indications. Dtsch. Arztebl. Int. 2021, 118, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Browne, J.P.; Bastaki, H.; Dawson, J. What Is the Optimal Time Point to Assess Patient-Reported Recovery after Hip and Knee Replacement? A Systematic Review and Analysis of Routinely Reported Outcome Data from the English Patient-Reported Outcome Measures Programme. Health Qual. Life Outcomes 2013, 11, 128. [Google Scholar] [CrossRef] [PubMed]
- Oakman, J.; Neupane, S.; Nygård, C.H. Does Age Matter in Predicting Musculoskeletal Disorder Risk? An Analysis of Workplace Predictors over 4 Years. Int. Arch. Occup. Environ. Health 2016, 89, 1127–1136. [Google Scholar] [CrossRef] [PubMed]
- Chim, J. Ergonomics Workload Analysis for the Prevention of Musculoskeletal Disorders in Food Services in the Health Sector. In Proceedings of the 42nd Annual Conference on Human Factors & Ergonomics Society of Australia (HFESA 2006), Sydney, NSW, Australia, 20–22 November 2006; pp. 197–205. [Google Scholar]
- Ariyanto, J.; Palutturi, S.; Russeng, S.S.; Birawida, A.; Warsinggih, W.; Rosyanti, L. Control of the Risk of Musculoskeletal Disorders in the Food Industry: Systematic Review. Ann. Rom. Soc. Cell Biol. 2021, 25, 4254–4261. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Body Region | Included Musculoskeletal Disorders |
|---|---|
| Upper back | cervical disk disorders (M50.0–M50.9), cervicocranial syndrome (M53.0), cervicobrachial syndrome (M53.1), cervicalgia (M54.2) |
| Low back | other intervertebral disk disorders (M51.0–M51.9), sciatica (M54.3), lumbago with sciatica (M54.4), low back pain (M54.5) |
| Shoulder | adhesive capsulitis of shoulder (M75.0), rotator cuff tear or rupture, not specified as traumatic (M75.1), bicipital tendinitis (M75.2), calcific tendinitis of shoulder (M75.3), impingement syndrome of shoulder (M75.4), bursitis of shoulder (M75.5), other shoulder lesions (M75.8), shoulder lesion, unspecified (M75.9) |
| Elbow | medial epicondylitis (M77.0), lateral epicondylitis (M77.1), olecranon bursitis (M70.2), other bursitis of elbow (M70.3) |
| Hand and wrist | osteoarthritis of first carpometacarpal joint (M18.0–M18.9), radial styloid tenosynovitis (de Quervain) (M65.4), crepitant synovitis of hand and wrist (M70.0), peri arthritis of wrist (M77.2), carpal tunnel syndrome (G56.0) |
| Hip | osteoarthritis of hip (M16.0–M16.9), other articular cartilage disorders of hip (M24.15) |
| Knee | osteoarthritis of knee (M17.0–M17.9), internal derangement of knee (M23.0–23.9), prepatellar bursitis (M70.4), other bursitis of knee (M70.5), synovial cyst of popliteal space (Baker) (M71.2) |
| Ankle | primary osteoarthritis of ankle and food (M19.07), secondary osteoarthritis of ankle and (M19.27), other and unspecified osteoarthritis (M19.) |
| Divisions | 20–44 Years | 45–65 Years | ||||
|---|---|---|---|---|---|---|
| M | F | Total | M | F | Total | |
| Accommodation | 2604 | 3750 | 6354 | 1557 | 3140 | 4697 |
| Food and beverage service activities | 7968 | 10,163 | 18,131 | 3270 | 5476 | 8746 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zerbo Šporin, D.; Kozinc, Ž.; Prijon, T.; Šarabon, N. Incidence and Duration of Sick Leave Due to Work-Related Musculoskeletal Disorders in the Accommodation and Food Services Activities Sector in Slovenia: A Nationwide 5-Year Observational Study. Int. J. Environ. Res. Public Health 2023, 20, 3133. https://doi.org/10.3390/ijerph20043133
Zerbo Šporin D, Kozinc Ž, Prijon T, Šarabon N. Incidence and Duration of Sick Leave Due to Work-Related Musculoskeletal Disorders in the Accommodation and Food Services Activities Sector in Slovenia: A Nationwide 5-Year Observational Study. International Journal of Environmental Research and Public Health. 2023; 20(4):3133. https://doi.org/10.3390/ijerph20043133
Chicago/Turabian StyleZerbo Šporin, Dorjana, Žiga Kozinc, Ticijana Prijon, and Nejc Šarabon. 2023. "Incidence and Duration of Sick Leave Due to Work-Related Musculoskeletal Disorders in the Accommodation and Food Services Activities Sector in Slovenia: A Nationwide 5-Year Observational Study" International Journal of Environmental Research and Public Health 20, no. 4: 3133. https://doi.org/10.3390/ijerph20043133