
Impacts of Air Pollution on Health and Cost of Illness in Jakarta, Indonesia
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
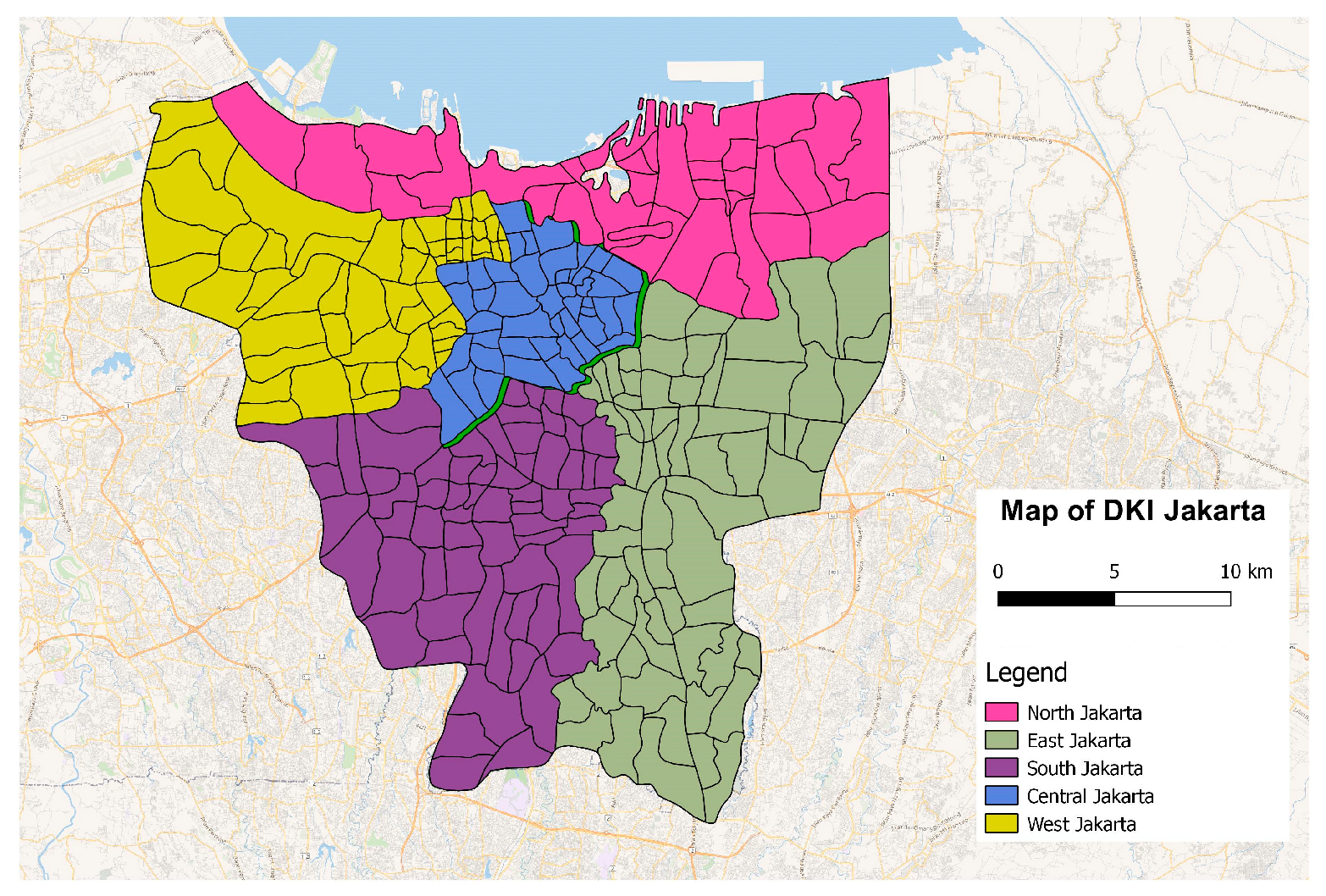
2.1. Study Area
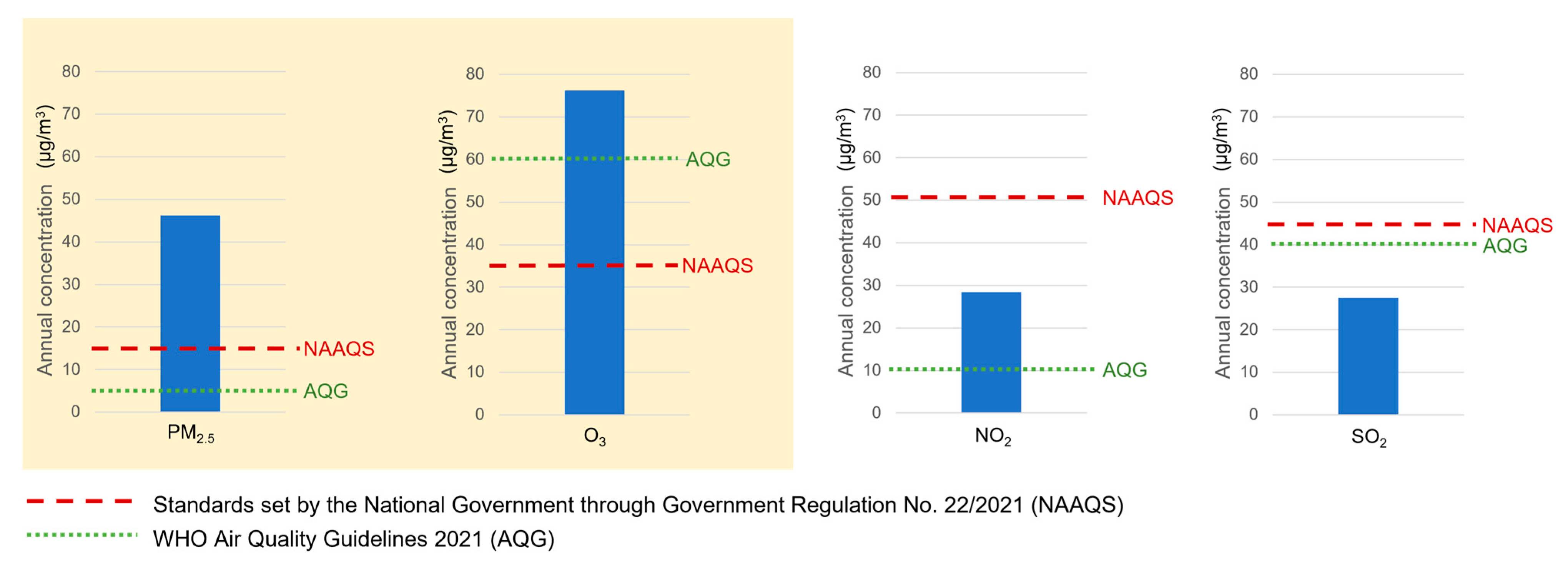
2.2. Exposure Data (PM2.5 and O3 Concentration)
2.3. Health Data
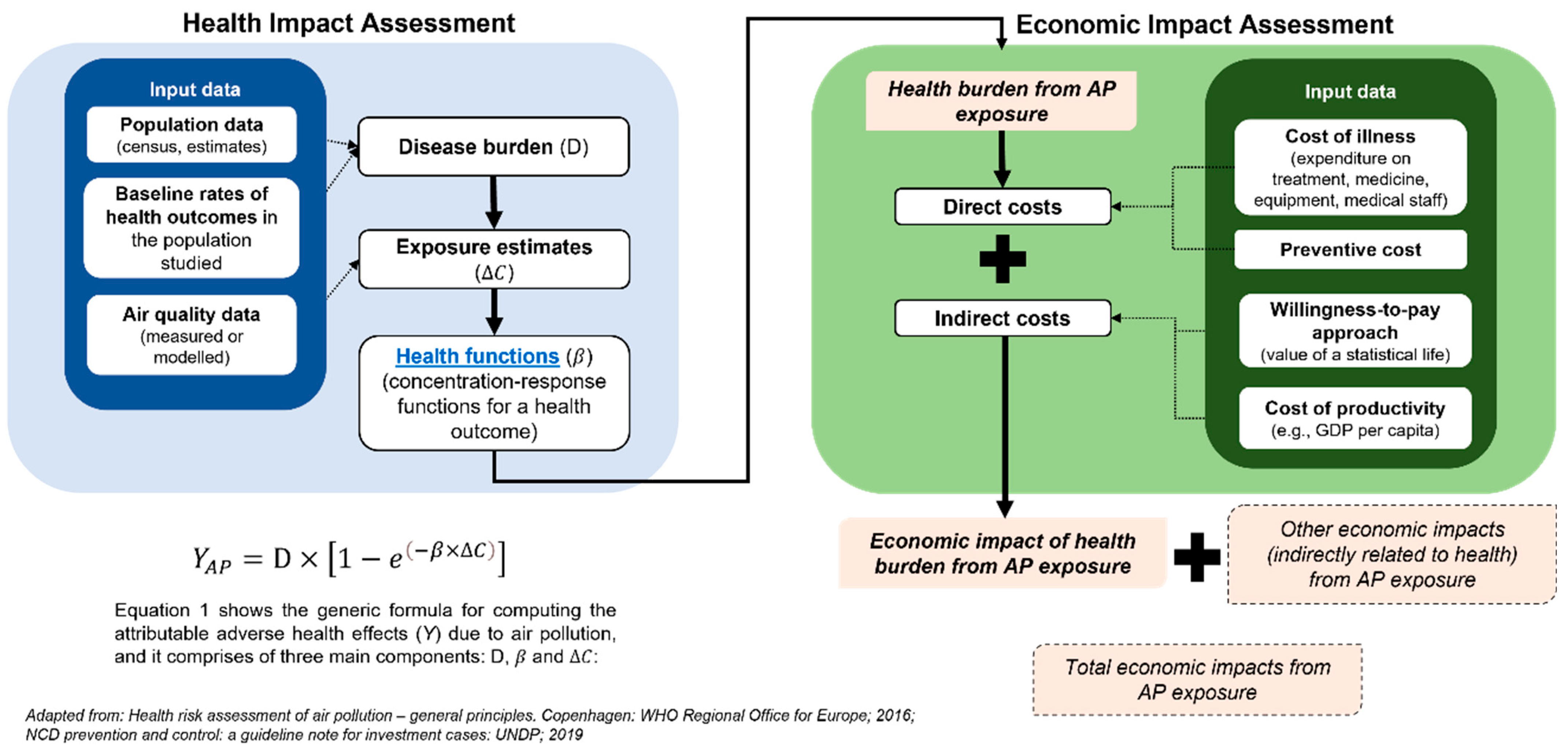
2.4. Estimation of the Health Burdens of Air Pollution
2.4.1. Long-term Impacts of Air Pollution
2.4.2. Short-term Impacts of Air Pollution
2.4.3. Calculating Health Burdens Attributable to Air Pollution
- = Number of health outcomes attributable to air pollution
- = Baseline number of health endpoints over the study period
- = the coefficient as the slope of the log-linear relationship between ambient air pollution concentrations and health outcomes, or the exponentiation of RR
- = baseline PM2.5 concentration (in µg/m3) in a day or in a year (e.g., 2019)
- = counterfactual concentration of pollutants (i.e., 4.2 µg/m3 for PM2.5 and 32.4 ppb for O3), below which no additional health risk is conferred
2.4.4. Estimation of Economic Impacts of Health Burdens Attributable to Air Pollution
2.4.5. Estimating Hospitalization Days
2.4.6. Estimating Inpatient Health Care Cost
2.4.7. Estimating Non-Health Care Cost
2.4.8. Estimating the Value of Statistical Life Year (VSL)
2.4.9. Estimating the Cost of Stunting
3. Results
3.1. Demography and Air Pollution Level in Jakarta
3.2. Health Impacts
3.2.1. Long-Term Impacts of Air Pollution
3.2.2. Short-Term Impacts of Air Pollution
3.2.3. The Economic Cost of Health Impacts from Air Pollution
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Ambient (Outdoor) Air Pollution. Available online: https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 4 October 2021).
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Results. Available online: http://ghdx.healthdata.org/gbd-results-tool. (accessed on 2 July 2021).
- Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; Abegaz, K.H.; Abolhassani, H.; Aboyans, V.; et al. Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Ministry of Health of Republic of Indonesia. National Health Accounts—Indonesia. 2018. Available online: http://ppjk.kemkes.go.id/download/http-ppjk-kemkes-go-id-download-national-health-accounts-indonesia-tahun-2018/ (accessed on 2 July 2021).
- Institute for Health Metrics and Evaluation. GBD Compare|IHME Viz Hub. Available online: http://vizhub.healthdata.org/gbd-compare (accessed on 28 June 2021).
- World Bank. The Global Health Cost of PM2.5 Air Pollution: A Case for Action Beyond 2021; International Development in Focus; The World Bank: Washington, WA, USA, 2022; ISBN 978-1-4648-1816-5. [Google Scholar]
- World Health Organization. Air Pollution and Child Health: Prescribing Clean Air; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- American Lung Association. Children and Air Pollution. Available online: https://www.lung.org/clean-air/outdoors/who-is-at-risk/children-and-air-pollution (accessed on 10 May 2021).
- Liu, Y.; Xu, J.; Chen, D.; Sun, P.; Ma, X. The Association between Air Pollution and Preterm Birth and Low Birth Weight in Guangdong, China. BMC Public Health 2019, 19, 3. [Google Scholar] [CrossRef] [PubMed]
- Pun, V.C.; Dowling, R.; Mehta, S. Ambient and Household Air Pollution on Early-Life Determinants of Stunting—A Systematic Review and Meta-Analysis. Environ. Sci. Pollut. Res. 2021, 28, 26404–26412. [Google Scholar] [CrossRef] [PubMed]
- Jaafar, H.; Razi, N.A.; Azzeri, A.; Isahak, M.; Dahlui, M. A Systematic Review of Financial Implications of Air Pollution on Health in Asia. Environ. Sci. Pollut. Res. 2018, 25, 30009–30020. [Google Scholar] [CrossRef]
- Hoddinott, J.; Alderman, H.; Behrman, J.R.; Haddad, L.; Horton, S. The Economic Rationale for Investing in Stunting Reduction. Matern. Child Nutr. 2013, 9, 69–82. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Brauer, M.; Cropper, M.L.; Balakrishnan, K.; Mathur, P.; Dey, S.; Turkgulu, B.; Kumar, G.A.; Khare, M.; Beig, G.; et al. Health and Economic Impact of Air Pollution in the States of India: The Global Burden of Disease Study 2019. Lancet Planet Health 2021, 5, e25–e38. [Google Scholar] [CrossRef]
- Lock, K. Health Impact Assessment. BMJ 2000, 320, 1395–1403. [Google Scholar] [CrossRef]
- Brauer, M.; Amann, M.; Burnett, R.T.; Cohen, A.; Dentener, F.; Ezzati, M.; Henderson, S.B.; Krzyzanowski, M.; Martin, R.V.; van Dingenen, R.; et al. Exposure Assessment for Estimation of the Global Burden of Disease Attributable to Outdoor Air Pollution. Environ. Sci. Technol. 2012, 46, 652–660. [Google Scholar] [CrossRef]
- Zhang, X.; Cheng, C.; Zhao, H. A Health Impact and Economic Loss Assessment of O3 and PM2.5 Exposure in China From 2015 to 2020. Geohealth 2022, 6, e2021GH000531. [Google Scholar] [CrossRef]
- U. S. Environmental Protection Agency. Part 50 National Primary and Secondary Ambient Air Quality Standards 2011, 40 CFR 50; U. S. Environmental Protection Agency: Washington, DC, USA, 2011; Volume 2.
- World Health Organization. Health Risks of Air Pollution in Europe–HRAPIE Project. Recommendations for Concentration–Response Functions for Cost–Benefit Analysis of Particulate Matter, Ozone and Nitrogen Dioxide; World Health Organization: Copenhagen, Denmark, 2013. [Google Scholar]
- Heft-Neal, S.; Burney, J.; Bendavid, E.; Burke, M. Robust Relationship between Air Quality and Infant Mortality in Africa. Nature 2018, 559, 254–258. [Google Scholar] [CrossRef]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Particulate Matter Risk Curves; Global Burden of Disease Collaborative Network: Seattle, WA, USA, 2021. [Google Scholar]
- Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019 (GBD 2019) Relative Risks; Global Burden of Disease Collaborative Network: Seattle, WA, USA, 2020. [Google Scholar]
- Ariawan, I.; Sartono, B.; Wahyuningsih, W.; Negara, S.I.; Mawardi, J.; Jaya, C.; Sutara, F.A.; Nugraha, N.S.; Panggabean, P.D.; Purnama, T.S.; et al. BPJS Kesehatan Sample Data Year 2015-2018; Year 2020; BPJS Kesehatan: Jakarta, Indonesia, 2020. [Google Scholar]
- Bank of Indonesia. Foreign Exchange Rates. Available online: https://www.bi.go.id/id/statistik/informasi-kurs/transaksi-bi/default.aspx (accessed on 12 October 2021).
- Sectoral Statistics Portal of DKI Jakarta Province. DKI Jakarta Province Minimum Wage 2015–2020. Available online: https://statistik.jakarta.go.id/tabel/upah-minimum-provinsi-dki-jakarta/ (accessed on 10 September 2021).
- The World Bank. World Bank Open Data. Available online: https://data.worldbank.org/ (accessed on 10 September 2021).
- U.S Department of Transportation. Departmental Guidance on Valuation of a Statistical Life in Economic Analysis. Available online: https://www.transportation.gov/office-policy/transportation-policy/revised-departmental-guidance-on-valuation-of-a-statistical-life-in-economic-analysis (accessed on 10 September 2021).
- Robinson, L.A.; Hammitt, J.K.; O’Keeffe, L. Valuing Mortality Risk Reductions in Global Benefit-Cost Analysis. J. Benefit Cost Anal. 2019, 10, 15–50. [Google Scholar] [CrossRef] [PubMed]
- Statistics Indonesia (Badan Pusat Statistik—BPS). Statistical Terms. Available online: https://www.bps.go.id/istilah/index.html?Istilah_page=4 (accessed on 10 September 2021).
- Statistics Indonesia (Badan Pusat Statistik—BPS). Gross Regional Domestic Product of Regencies/Municipalities in Indonesia 2016–2020; Statistics Indonesia (Badan Pusat Statistik—BPS): Jakarta, Indonesia, 2021.
- Nurhayati-Wolff, H. Annual Inflation Rate of the Healthcare Sector in Indonesia from 2014 to 2020. Available online: https://www.statista.com/statistics/1005580/indonesia-annual-inflation-rate-of-healthcare/#statisticContainer (accessed on 10 September 2021).
- Badan Pusat Statistik Provinsi DKI Jakarta. DKI Jakarta Dalam Angka (DKI Jakarta Province in Figures) 2021; BPS Provinsi DKI Jakarta: Jakarta, Indonesia, 2021.
- Government of Indonesia. Government Regulation No. 22/2021 on Environment Protection and Management. Available online: https://jdih.setkab.go.id//puu/buka_puu/176367/Lampiran_VII_Salinan_PP_Nomor_22_Tahun_2021.pdf (accessed on 4 September 2021).
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Health Organization: Geneva, Switzerland, 2021; p. 1302. [Google Scholar]
- Syahril, S.; Resosudarmo, B.P.; Tomo, H.S. Study on Air Quality in Jakarta, Indonesia: Future Trends, Health Impacts, Economic Value and Policy Options; ADB, Jakarta: Jakarta, Indonesia, 2002. [Google Scholar]
- Resosudarmo, B.P.; Napitupulu, L. Health and Economic Impact of Air Pollution in Jakarta. Econ. Record 2004, 80, S65–S75. [Google Scholar] [CrossRef]
- Safrudin, A.; Palguna, A.; Adrison, V.; Khoirunurrofik, K.; Haryanto, B.; Krisnawati, L.; Zakaria, M.; Hamonangan, E.; Nurafiatin, L.; Suhud, M.; et al. Cost Benefit Analysis for Fuel Quality and Fuel Economy Initiative in Indonesia; Ministry of Environment Republic of Indonesia: Jakarta, Indonesia, 2013.
- Breathe Easy Jakarta. Factsheet 4: Health Impacts; Breathe Easy Jakarta: Jakarta, Indonesia, 2016. [Google Scholar]
- Roy, R.; Braathen, N.A. The Rising Cost of Ambient Air Pollution Thus Far in the 21st Century: Results from the BRIICS and the OECD Countries. In OECD Environment Working Papers No. 124; OECD: Paris, France, 2017. [Google Scholar] [CrossRef]
- Trautmann, S.; Rehm, J.; Wittchen, H. The Economic Costs of Mental Disorders. EMBO Rep. 2016, 17, 1245–1249. [Google Scholar] [CrossRef] [PubMed]
- Mankiw, N.G. Principles of Economics, 10th ed.; Prentice Hall: Boston, MA, USA, 2011; ISBN 9780538453059. [Google Scholar]
- Bhutta, Z.A.; Ahmed, T.; Black, R.E.; Cousens, S.; Dewey, K.; Giugliani, E.; Haider, B.A.; Kirkwood, B.; Morris, S.S.; Sachdev, H.; et al. What Works? Interventions for Maternal and Child Undernutrition and Survival. Lancet 2008, 371, 417–440. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E. Evidence-Based Interventions for Improvement of Maternal and Child Nutrition: What Can Be Done and at What Cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef]
- Health Canada. Health Impacts of Air Pollution in Canada: Estimates of Premature Deaths and Nonfatal Outcomes—2021 Report; Health Canada: Ottawa, ON, Canada, 2021.
- Mueller, W.; Vardoulakis, S.; Steinle, S.; Loh, M.; Johnston, H.J.; Precha, N.; Kliengchuay, W.; Sahanavin, N.; Nakhapakorn, K.; Sillaparassamee, R.; et al. A Health Impact Assessment of Long-Term Exposure to Particulate Air Pollution in Thailand. Environ. Res. Lett. 2021, 16, 055018. [Google Scholar] [CrossRef]
- Rocha, C.A.; Lima, J.L.R.; Mendonça, K.V.; Marques, E.V.; Zanella, M.E.; Ribeiro, J.P.; Bertoncini, B.V.; Castelo Branco, V.T.F.; Cavalcante, R.M. Health Impact Assessment of Air Pollution in the Metropolitan Region of Fortaleza, Ceará, Brazil. Atmos Environ. 2020, 241, 117751. [Google Scholar] [CrossRef]
- Abe, K.C.; Rodrigues, M.A.; Miraglia, S.G.E.K. Health Impact Assessment of Air Pollution in Lisbon, Portugal. J. Air Waste Manag. Assoc. 2022, 72, 1307–1315. [Google Scholar] [CrossRef]
- Khomenko, S.; Cirach, M.; Pereira-Barboza, E.; Mueller, N.; Barrera-Gómez, J.; Rojas-Rueda, D.; de Hoogh, K.; Hoek, G.; Nieuwenhuijsen, M. Premature Mortality Due to Air Pollution in European Cities: A Health Impact Assessment. Lancet Planet Health 2021, 5, e121–e134. [Google Scholar] [CrossRef]
- Hasnain, A.; Sheng, Y.; Hashmi, M.Z.; Bhatti, U.A.; Hussain, A.; Hameed, M.; Marjan, S.; Bazai, S.U.; Hossain, M.A.; Sahabuddin, M.; et al. Time Series Analysis and Forecasting of Air Pollutants Based on Prophet Forecasting Model in Jiangsu Province, China. Front. Environ. Sci. 2022, 10, 1044. [Google Scholar] [CrossRef]
- Aamir, M.; Li, Z.; Bazai, S.; Wagan, R.A.; Bhatti, U.A.; Nizamani, M.M.; Akram, S. Spatiotemporal Change of Air-Quality Patterns in Hubei Province—A Pre- to Post-COVID-19 Analysis Using Path Analysis and Regression. Atmosphere 2021, 12, 1338. [Google Scholar] [CrossRef]
- DKI Jakarta Provincial Government. Sekitar 87 Persen Masyarakat Dki Jakarta Sudah Memiliki Jaminan Kesehatan di Tahun. 2019. Available online: https://statistik.jakarta.go.id/sekitar-87-persen-masyarakat-dki-jakarta-sudah-memiliki-jaminan-kesehatan-di-tahun-2019/ (accessed on 12 July 2021).




{kind=link}
{kind=link}
{kind=link}
| Health Endpoints | Age | RR (95% CI) |
|---|---|---|
| Infant Mortality, all-cause | 1–12 months | 1.09 (1.04, 1.14) [19] |
| Stunting | <5 years old | 1.19 (1.10, 1.29) 1 [10] |
| Low Birth Weight at term | At birth | 1.18 (1.06, 1.33) [9] |
| Preterm Birth | At birth | 1.007 (1.005, 1.08) [9] |
| Total Hospitalizations | Age | RR (95% CI) |
|---|---|---|
| For PM2.5 | ||
| Due to Cardiovascular diseases Due to Respiratory diseases | All ages All ages | 1.0091 (1.0017, 1.0166) [18] 1.0019 (0.9982, 1.0402) [18] |
| For O3 | ||
| Due to Cardiovascular diseases | 65+ | 1.0089 (1.0050, 1.0127) [18] |
| Due to Respiratory diseases | 65+ | 1.0044 (1.0007, 1.0083) [18] |
| No | Assumption | Amount |
|---|---|---|
| 1 | Exchange Rate USD 2019 (rounded) [23] | IDR 14,000 |
| 2 | Jakarta Monthly Minimum Wage 2019 [24] | USD 281.50 |
| 3 | GNI Indonesia Per Capita 2019 (current) [25] | USD 4051.78 |
| 4 | GNI United States Per Capita 2019 (current) [25] | USD 66,061 |
| 5 | VSL (value of statistical life) United States 2019 [26] | USD 10,900,000 |
| 6 | VSL Indonesia 2019 (adjusted) [27] | USD 284,184.25 |
| 7 | Income Elasticity [27] | 1.5 |
| 8 | Purchasing Power Parity (USD–IDN) [25] | IDR 4.75 |
| 9 | Productive Age [28] | 15–64 |
| 10 | Productive Years | 49 Years |
| 11 | GDP Jakarta 2019 (In Billion USD) [29] | USD 131.64 |
| 12 | Healthcare Inflation (2014–2019) [12] | 5.71% (2014); 5.32% (2015); 3.92% (2016); 2.9% (2017); 3.14% (2018); 3.46% (2019) |
| 13 14 15 16 17 | Low Birth Weight * Cost Preterm Birth * Cost Stunting *^ Cost Hospital Admission for CVD * Cost Hospital Admission for RESP * Cost | USD 1513.03 USD 1136.17 USD 128.26 USD 1313.83 USD 638.98 |
| Characteristics | Jakarta Province * | Central Jakarta | North Jakarta | West Jakarta | South Jakarta | East Jakarta |
|---|---|---|---|---|---|---|
| Total Area (km2) | 664 | 52.4 | 140 | 124.4 | 154.3 | 182.7 |
| Number of Population | 10,557,810 | 928,109 | 1,812,915 | 2,589,933 | 2,264,699 | 2,937,859 |
| Population Density (per km2) | 15,900 | 17,719 | 12,950 | 20,813 | 14,675 | 16,080 |
| Poverty Line (IDR/capita/month) | 667,260 | 625,177 | 549,506 | 517,646 | 729,256 | 539,510 |
| Number of Poor People (% within the municipality) a | 365,550 (3.5%) | 34,130(3.7%) | 91,090 (5.0%) | 84,020 (3.2%) | 61,760 (2.7%) | 91,610 (3.1%) |
| GRDP per capita (in USD) | 19,056.71 | 53,886.57 | 20,592.21 | 12,976.36 | 20,267.86 | 11,880.43 |
| Land-use Characteristic | Mixed | Governmental Center | Industrial & Port | Industrial (small-scale) | Residential | Industrial |
| Health Outcomes | Total burden | Air Pollution Attributable Indicators | |
|---|---|---|---|
| Number of Cases | Rate | ||
| PM2.5 (annual mean: 52 µg/m3) | |||
| Adverse outcomes in children (2019) | |||
| Infant Deaths | 986 | 327 | 2 per 1000 births |
| Stunting | 11,211 | 6153 | 7 per 1000 children under 5 |
| Low Birth Weight | 1269 | 680 | 5 per 1000 births |
| Preterm Births | 1919 | 62 | 4 per 10,000 births |
| Mortality (2019) * | 23,430 ^ | 9692 | 88 per 100,000 population |
| O3 (annual daily max 8 h average: 274 µg/m3) | |||
| Mortality due to COPD (2019) * | 3635 | 310 | 5 per 100,000 aged 25+ |
| Hospitalizations | Disease Cause | |
|---|---|---|
| Cardiovascular | Respiratory | |
| PM2.5 | ||
| Total Hospitalizations | 150,272 | 108,560 |
| PM2.5 Attributable Indicators | ||
| Number of Cases | 3043 | 455 |
| Rate (per 100,000 population) | 28 | 4 |
| O3 * | ||
| Total Hospitalizations | 37,039 | 12,147 |
| O3 Attributable Indicators | ||
| Number of Cases | 1357 | 182 |
| Rate (per 100,000 population *) | 282 | 38 |
| Adverse Health Outcomes in Children | Mortality | Hospitalizations | |||
|---|---|---|---|---|---|
| Infant Deaths | Stunting | Adverse Birth Outcomes * | |||
| Health Burden | 327 | 6153 | 742 | 10,002 | 5037 |
| Economic Cost | 92.93 | 0.79 | 1.10 | 2842.41 | 6.19 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Syuhada, G.; Akbar, A.; Hardiawan, D.; Pun, V.; Darmawan, A.; Heryati, S.H.A.; Siregar, A.Y.M.; Kusuma, R.R.; Driejana, R.; Ingole, V.; et al. Impacts of Air Pollution on Health and Cost of Illness in Jakarta, Indonesia. Int. J. Environ. Res. Public Health 2023, 20, 2916. https://doi.org/10.3390/ijerph20042916
Syuhada G, Akbar A, Hardiawan D, Pun V, Darmawan A, Heryati SHA, Siregar AYM, Kusuma RR, Driejana R, Ingole V, et al. Impacts of Air Pollution on Health and Cost of Illness in Jakarta, Indonesia. International Journal of Environmental Research and Public Health. 2023; 20(4):2916. https://doi.org/10.3390/ijerph20042916
Chicago/Turabian StyleSyuhada, Ginanjar, Adhadian Akbar, Donny Hardiawan, Vivian Pun, Adi Darmawan, Sri Hayyu Alynda Heryati, Adiatma Yudistira Manogar Siregar, Ririn Radiawati Kusuma, Raden Driejana, Vijendra Ingole, and et al. 2023. "Impacts of Air Pollution on Health and Cost of Illness in Jakarta, Indonesia" International Journal of Environmental Research and Public Health 20, no. 4: 2916. https://doi.org/10.3390/ijerph20042916