
Beneficial Effects of an Online Mindfulness-Based Intervention on Sleep Quality in Italian Poor Sleepers during the COVID-19 Pandemic: A Randomized Trial
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
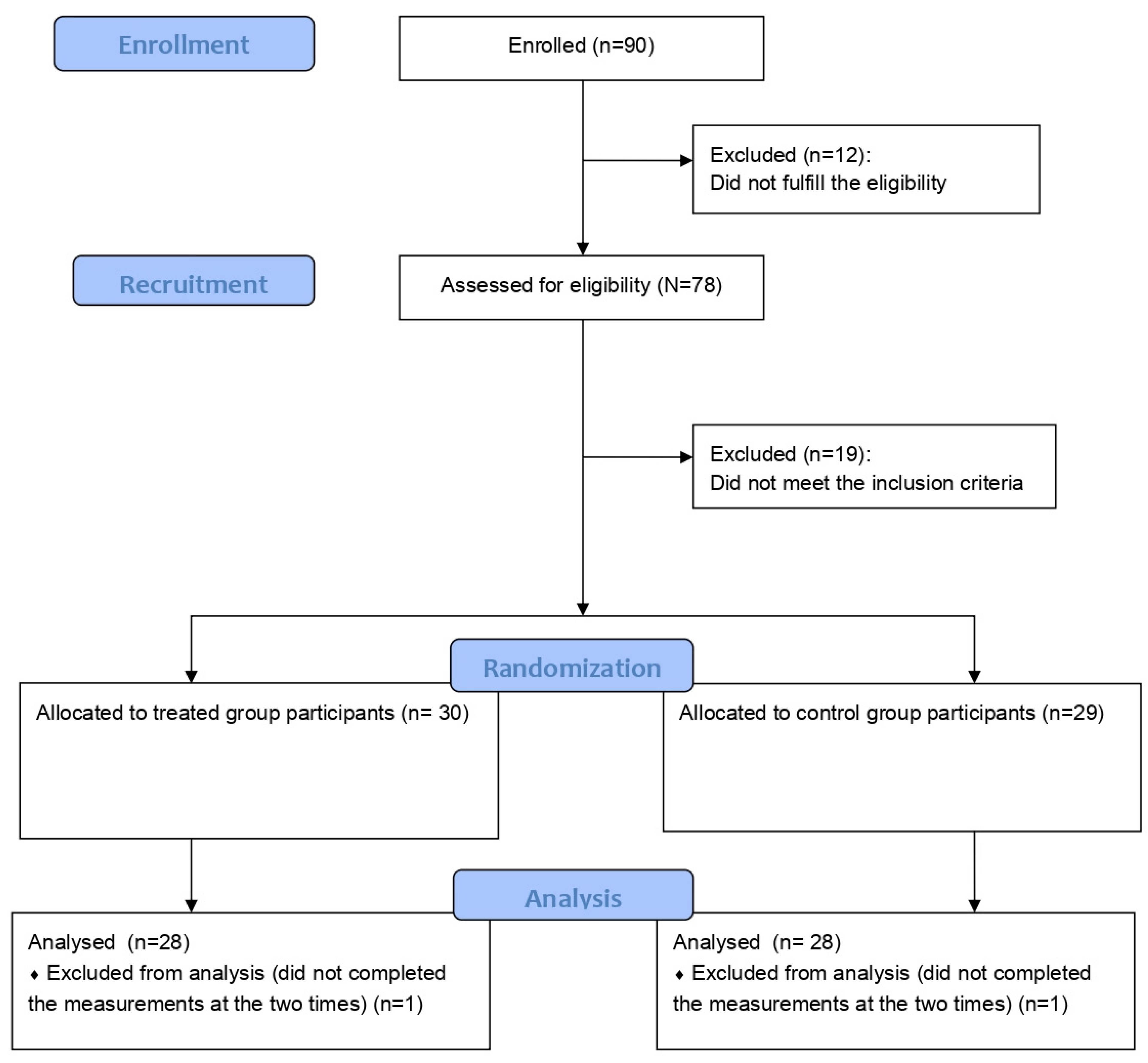
2.1. Participants
2.2. Intervention
2.3. Psychological and Sleep Metrics
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pigeon, W.; Perlis, M.L. Sleep homeostasis in primary insomnia. Sleep Med. Rev. 2006, 10, 247–254. [Google Scholar] [CrossRef]
- Espie, C.A. Insomnia: Conceptual issues in the development, persistence, and treatment of sleep disorder in adults. Annu. Rev. Psychol. 2002, 53, 215–243. [Google Scholar] [CrossRef]
- Terzano, M.G.; Parrino, L.; Cirignotta, F.; Ferini-Strambi, L.; Gigli, G.; Rudelli, G.; Sommacal, S.; Bonnani, E.; Iudice, A.; Bruni, O.; et al. Studio Morfeo: Insomnia in primary care, a survey conducted on the Italian population. Sleep Med. 2004, 5, 67–75. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Smirne, S. Prevalence and consequences of insomnia disorders in the general population of Italy. Sleep Med. 2002, 3, 115–120. [Google Scholar] [CrossRef] [PubMed]
- Varghese, N.E.; Lugo, A.; Ghislandi, S.; Colombo, P.; Pacifici, R.; Gallus, S. Sleep dissatisfaction and insufficient sleep duration in the Italian population. Sci. Rep. 2020, 10, 17943. [Google Scholar] [CrossRef]
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J. Neurol. 2021, 268, 8–15. [Google Scholar] [CrossRef]
- Casagrande, M.; Favieri, F.; Tambelli, R.; Forte, G. The enemy who sealed the world: Effects quarantine due to the COVID-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020, 75, 12–20. [Google Scholar] [CrossRef]
- Brandt, J.; Leong, C. Benzodiazepines and Z-Drugs: An Updated Review of Major Adverse Outcomes Reported on in Epidemiologic Research. Drugs R D 2017, 17, 493–507. [Google Scholar] [CrossRef]
- van Straten, A.; van der Zweerde, T.; Kleiboer, A.; Cuijpers, P.; Morin, C.M.; Lancee, J. Cognitive and behavioral therapies in the treatment of insomnia: A meta-analysis. Sleep Med. Rev. 2018, 38, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Bootzin, R.R.; Epstein, D.R. Understanding and Treating Insomnia. Annu. Rev. Clin. Psychol. 2011, 7, 435–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qaseem, A.; Kansagara, D.; Forciea, M.A.; Cooke, M.; Denberg, T.D.; Barry, M.J.; Boyd, C.; Chow, R.D.; Fitterman, N.; Harris, R.P.; et al. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians. Ann. Intern. Med. 2016, 165, 125–133. [Google Scholar] [CrossRef]
- Rusch, H.L.; Rosario, M.; Levison, L.M.; Olivera, A.; Livingston, W.S.; Wu, T.; Gill, J.M. The effect of mindfulness meditation on sleep quality: A systematic review and meta-analysis of randomized controlled trials. Ann. N. Y. Acad. Sci. 2019, 1445, 5–16. [Google Scholar] [CrossRef]
- Gong, H.; Ni, C.X.; Liu, Y.Z.; Zhang, Y.; Su, W.J.; Lian, Y.J.; Peng, W.; Jiang, C.L. Mindfulness meditation for insomnia: A meta-analysis of randomized controlled trials. J. Psychosom. Res. 2016, 89, 1–6. [Google Scholar] [CrossRef]
- Chiesa, A.; Fazia, T.; Bernardinelli, L.; Morandi, G. Citation patterns and trends of systematic reviews about mindfulness. Complement. Ther. Clin. Pract. 2017, 28, 26–37. [Google Scholar] [CrossRef]
- Gardi, C.; Fazia, T.; Stringa, B.; Giommi, F. A short Mindfulness retreat can improve biological markers of stress and inflammation. Psychoneuroendocrinology 2022, 135, 105579. [Google Scholar] [CrossRef]
- Schlechta Portella, C.F.; Ghelman, R.; Abdala, V.; Schveitzer, M.C.; Afonso, R.F. Meditation: Evidence Map of Systematic Reviews. Front. Public Health 2021, 9, 742715. [Google Scholar] [CrossRef]
- Winbush, N.Y.; Gross, C.R.; Kreitzer, M.J. The effects of mindfulness-based stress reduction on sleep disturbance: A systematic review. Explore 2007, 3, 585–591. [Google Scholar] [CrossRef]
- Ong, J.C.; Moore, C. What do we really know about mindfulness and sleep health? Curr. Opin. Psychol. 2020, 34, 18–22. [Google Scholar] [CrossRef]
- Ong, J.C.; Ulmer, C.S.; Manber, R. Improving sleep with mindfulness and acceptance: A metacognitive model of insomnia. Behav. Res. Ther. 2012, 50, 651–660. [Google Scholar] [CrossRef]
- Binks, H.; Vincent, G.E.; Gupta, C.; Irwin, C.; Khalesi, S. Effects of Diet on Sleep: A Narrative Review. Nutrients 2020, 12, 936. [Google Scholar] [CrossRef] [Green Version]
- Dashti, H.S.; Scheer, F.A.J.L.; Jacques, P.F.; Lamon-Fava, S.; Ordovás, J.M. Short sleep duration and dietary intake: Epidemiologic evidence, mechanisms, and health implications. Adv. Nutr. 2015, 6, 648–659. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; Taggart, F.M.; Kandala, N.B.; Currie, A.; Peile, E.; Stranges, S.; Miller, M.A. Meta-analysis of short sleep duration and obesity in children and adults. Sleep 2008, 31, 619–626. [Google Scholar] [CrossRef]
- Grandner, M.A.; Jackson, N.; Gerstner, J.R.; Knutson, K.L. Dietary nutrients associated with short and long sleep duration. Data from a nationally representative sample. Appetite 2013, 64, 71–80. [Google Scholar] [CrossRef]
- Stern, J.H.; Grant, A.S.; Thomson, C.A.; Tinker, L.; Hale, L.; Brennan, K.M.; Woods, N.F.; Chen, Z. Short sleep duration is associated with decreased serum leptin, increased energy intake and decreased diet quality in postmenopausal women. Obesity 2014, 22, E55–E61. [Google Scholar] [CrossRef]
- Zoom Video Communications, Inc. Global Infrastructure and Security Guide Global Infastructure & Security Guide; Zoom Video Communications, Inc.: San Jose, CA, USA, 2016. [Google Scholar]
- Fazia, T.; Bubbico, F.; Iliakis, I.; Salvato, G.; Berzuini, G.; Bruno, S.; Bernardinelli, L. Short-Term Meditation Training Fosters Mindfulness and Emotion Regulation: A Pilot Study. Front. Psychol. 2020, 11, 2828. [Google Scholar] [CrossRef]
- Fazia, T.; Bubbico, F.; Berzuini, G.; Tezza, L.D.; Cortellini, C.; Bruno, S.; Bernardinelli, L. Mindfulness meditation training in an occupational setting: Effects of a 12-weeks mindfulness-based intervention on wellbeing. Work 2021, 70, 1089–1099. [Google Scholar] [CrossRef]
- Fazia, T.; Bubbico, F.; Salvato, G.; Berzuini, G.; Bruno, S.; Bottini, G.; Bernardinelli, L. Boosting psychological well-being through a social mindfulness-based intervention in the general population. Int. J. Environ. Res. Public Health 2020, 17, 8404. [Google Scholar] [CrossRef]
- Vielhaber, K.; Riemann, D.; Feige, B.; Kuelz, A.; Kirschbaum, C.; Voderholzer, U. Impact of experimentally induced serotonin deficiency by tryptophan depletion on saliva cortisol concentrations. Pharmacopsychiatry 2005, 38, 87–94. [Google Scholar] [CrossRef]
- Thakkar, M.M. Histamine in the regulation of wakefulness. Sleep Med. Rev. 2011, 15, 65–74. [Google Scholar] [CrossRef]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Pinheiro, J.C.; Bates, D.M. Mixed-Effects Models in S and S-PLUS; Springer: Berlin/Heidelberg, Germany, 2000; ISBN 1441903178. [Google Scholar]
- Rice, J.A. Mathematical Statistics and Data Analysis; Cengage Learning: Boston, MA, USA, 2013. [Google Scholar]
- Yekutieli, D.; Benjamini, Y. The control of the false discovery rate in multiple testing under dependency. Ann. Stat. 2001, 29, 1165–1188. [Google Scholar] [CrossRef]
- Rothman, K.J. No adjustments are needed for multiple comparisons. Epidemiology 1990, 1, 43–46. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing; Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Curcio, G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 2013, 34, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Palagini, L.; Ragno, G.; Caccavale, L.; Gronchi, A.; Terzaghi, M.; Mauri, M.; Kyle, S.; Espie, C.A.; Manni, R. Italian validation of the Sleep Condition Indicator: A clinical screening tool to evaluate Insomnia Disorder according to DSM-5 criteria. Int. J. Psychophysiol. 2015, 98, 435–440. [Google Scholar] [CrossRef]
- Gagnon, C.; Bélanger, L.; Ivers, H.; Morin, C.M. Validation of the Insomnia Severity Index in primary care. J. Am. Board Fam. Med. 2013, 26, 701–710. [Google Scholar] [CrossRef]
- Medic, G.; Wille, M.; Hemels, M.E.H. Short- and long-term health consequences of sleep disruption. Nat. Sci. Sleep 2017, 9, 151–161. [Google Scholar] [CrossRef]
- Grandner, M.A. Sleep, Health, and Society. Sleep Med. Clin. 2017, 12, 1–22. [Google Scholar] [CrossRef]
- Favieri, F.; Forte, G.; Tambelli, R.; Casagrande, M. The Italians in the Time of Coronavirus: Psychosocial Aspects of the Unexpected COVID-19 Pandemic. Front. Psychiatry 2021, 12, 551924. [Google Scholar] [CrossRef] [PubMed]
- Gorgoni, M.; Scarpelli, S.; Mangiaruga, A.; Alfonsi, V.; Bonsignore, M.R.; Fanfulla, F.; Ferini-Strambi, L.; Nobili, L.; Plazzi, G.; De Gennaro, L.; et al. Pre-sleep arousal and sleep quality during the COVID-19 lockdown in Italy. Sleep Med. 2021, 88, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Kalmbach, D.A.; Pillai, V.; Arnedt, J.T.; Drake, C.L. Identifying At-Risk Individuals for Insomnia Using the Ford Insomnia Response to Stress Test. Sleep 2016, 39, 449. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Espie, C.A.; Kyle, S.D.; Hames, P.; Gardani, M.; Fleming, L.; Cape, J. The Sleep Condition Indicator: A clinical screening tool to evaluate insomnia disorder. BMJ Open 2014, 4, 4183. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Mastin, D.F.; Bryson, J.; Corwyn, R. Assessment of sleep hygiene using the Sleep Hygiene Index. J. Behav. Med. 2006, 29, 223–227. [Google Scholar] [CrossRef]
- Drake, C.; Richardson, G.; Roehrs, T.; Scofield, H.; Roth, T. Vulnerability to stress-related sleep disturbance and hyperarousal. Sleep 2004, 27, 285–291. [Google Scholar] [CrossRef]
- Coren, S.; Mah, K.B. Prediction of physiological arousability: A validation of the Arousal Predisposition Scale. Behav. Res. Ther. 1993, 31, 215–219. [Google Scholar] [CrossRef]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J. Pers. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef] [PubMed]
- Baer, R.A.; Smith, G.T.; Hopkins, J.; Krietemeyer, J.; Toney, L. Using Self-Report Assessment Methods to Explore Facets of Mindfulness. Assessment 2006, 13, 27–45. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | Mean (SD) Controls | Mean (SD) Treated | p-Value |
|---|---|---|---|
| Age | 53.96 (13.31) | 53.46 (10.04) | 0.87 |
| N (%) controls | N (%) treated | ||
| Sex | |||
| Male | 5 (18%%) | 5 (18%) | 1 |
| Female | 23 (82%) | 23 (82%) | |
| Nationality | |||
| Italian | 26 (93%) | 28 (100%) | 0.49 |
| Non-Italian | 2 (7%) | 0 (0%) | |
| Marital status | |||
| Cohabitant/married | 11 (39%) | 16 (57%) | 0.36 |
| Unmarried/single | 8 (29%) | 4 (14%) | |
| Separated/Divorced | 8 (29%) | 8 (29%) | |
| Widowed | 1 (4%) | 0 (0%) | |
| Number of children | |||
| 0 | 10 (36%) | 11 (39%) | 0.43 |
| 1 | 6 (21%) | 8 (28%) | |
| 2 | 9 (32%) | 9 (32%) | |
| ≥3 | 3 (11%) | 0 (0%) | |
| Dependent children/family members | |||
| No | 18 (64%) | 18 (64%) | 1 |
| Yes | 10 (36%) | 10 (36%) | |
| Unpaid loans | |||
| No | 21 (75%) | 22 (79%) | 1 |
| Yes | 7 (25%) | 6 (21%) | |
| Education | |||
| Middle school | 1 (4%) | 1 (4%) | 1 |
| High school | 11(39%) | 10 (36%) | |
| Degree | 13 46(%) | 14 (50%) | |
| Post-graduate course (e.g., PhD) | 3 (11%) | 3 (11%) | |
| Job | |||
| Public or private employee | 15 (54%) | 16 (57%) | 0.35 |
| Freelance (e.g., lawyer, doctor etc.) | 4 (14%) | 3 (11%) | |
| Student | 0 (0%) | 1 (4%) | |
| Unemployed or looking for a job | 3 (11%) | 0 (0%) | |
| Housewife | 0 (0%) | 2 (7%) | |
| Retired | 6 (21%) | 6 (21%) | |
| Type of employment agreement | |||
| Undetermined term | 13 (46%) | 15 (54%) | 0.80 |
| Fixed term | 4 (14%) | 2 (7%) | |
| Not applicable | 11 (39%) | 11 (39%) | |
| Employee satisfaction | |||
| No | 12 (43%) | 7 (25%) | 0.26 |
| Yes | 16 (57%) | 21 (75%) | |
| Sport | |||
| No | 5 (18%) | 8 (29%) | 0.53 |
| Yes | 23 (82%) | 20 (71%) | |
| Smoker | |||
| Yes | 4 (14%) | 4 (14%) | 1 |
| No | 24 (86%) | 24 (86%) | |
| Knowledge about meditation | |||
| Clear idea | 19 (68%) | 16 (57%) | 0.40 |
| Vague idea | 8 (29%) | 12 (43%) | |
| Just heard of | 1 (4%) | 0 (0%) | |
| Previous meditation experience | |||
| Yes | 22 (79%) | 24 (86%) | 0.73 |
| No | 6 (21%) | 4 (14%) | |
| Religious | |||
| No | 13 (46%) | 16 (57%) | 0.59 |
| Yes | 15 (54%) | 12 (43%) | |
| Number of books read in a year | |||
| 0–1 | 4 (14%) | 2 (7%) | 0.52 |
| 2–3 | 6 (21%) | 4 (14%) | |
| >3 | 18 (64%) | 22 (79%) | |
| Member of a cultural/sportive association | |||
| No | 20 (71%) | 17 (61%) | 0.57 |
| Yes | 8 (29%) | 11 (39%) | |
| Diet | |||
| Mediterranean | 22 (79%) | 24 (86%) | 0.69 |
| Vegetarian | 2 (7%) | 1 (4%) | |
| Vegan | 3 (11%) | 1 (4%) | |
| Macrobiotic | 1 (4%) | 2 (7%) | |
| Disease/disability | |||
| No | 20 (71%) | 15 (54%) | 0.27 |
| Yes | 8 (29%) | 13 (46%) | |
| Addiction | |||
| No | 27 (96%) | 25 (89%) | 0.61 |
| Yes | 1 (4%) | 3 (11%) | |
| Have you ever gone to a psychologist | |||
| No | 10 (36%) | 11 (39%) | 1 |
| Yes | 18 (64%) | 17 (61%) | |
| Drug for insomnia | |||
| No | 21 (75%) | 17 (61%) | 0.39 |
| Yes | 7 (25%) | 11 (39%) |
| Questionnaire | Mean (SD) Controls t0 | Mean (SD) Treated t0 | Mean (SD) Controls t1 | Mean (SD) Treated t1 | Internal Consistency t0 | Internal Consistency t1 | Effect Size (Hedges’ g) |
|---|---|---|---|---|---|---|---|
| ERQ | |||||||
| Reappraisal | 4.97 (1.09) | 5.09 (1.20) | 5.05 (1.13) | 4.88 (1.26) | 0.89 | 0.91 | −0.31 (small) |
| Suppression | 3.68 (1.05) | 3.39 (1.36) | 3.52 (1.25) | 3.60 (1.04) | 0.70 | 0.61 | 0.32 (small) |
| FFMQ | |||||||
| All Items | 3.26 (0.52) | 3.18 (0.51) | 3.25 (0.44) | 3.30 (0.41) | 0.93 | 0.88 | 0.50 (medium) |
| Observing | 3.41 (0.84) | 3.49 (0.68) | 3.37 (0.79) | 3.49 (0.67) | 0.85 | 0.83 | 0.07 (negligible) |
| Describing | 3.59 (0.81) | 3.50 (0.77) | 3.57 (0.73) | 3.64 (0.75) | 0.92 | 0.91 | 0.42 (small) |
| Acting with awareness | 3.22 (0.78) | 3.01 (0.73) | 3.27 (0.77) | 3.15 (0.63) | 0.91 | 0.88 | 0.17 (negligible) |
| Non-judging of inner experience | 3.18 (0.92) | 3.18 (0.88) | 3.22 (0.79) | 3.28 (0.84) | 0.93 | 0.91 | 0.09 (negligible) |
| Non-reactivity to inner experience | 2.83 (0.65) | 2.68 (0.59) | 2.73 (0.73) | 2.88 (0.58) | 0.81 | 0.83 | 0.66 (medium) |
| PSQI | |||||||
| All Items | 11.61 (3.71) | 10.64(3.03) | 9.86 (3.97) | 6.96 (3.18) | 0.60 | 0.70 | −0.67 (medium) |
| Subjective sleep quality (Component 1) | 1.86 (0.65) | 1.82 (0.72) | 1.75 (0.58) | 1.18 (0.47) | −0.89 (large) | ||
| Sleep latency (Component 2) | 2.14 (1.04) | 1.46 (0.79) | 1.50 (1.14) | 1.04 (0.79) | 0.27 (small) | ||
| Sleep duration (Component 3) | 1.79 (0.83) | 1.96 (0.69) | 1.61 (0.99) | 1.25 (0.89) | −0.74 (medium) | ||
| Sleep efficiency (Component 4) | 1.46 (1.26) | 1.29 (0.98) | 1.54 (1.35) | 0.82 (1.06) | −0.45 (small) | ||
| Sleep disturbance (Component 5) | 1.64 (0.68) | 1.57 (0.50) | 1.50 (0.64) | 1.18 (0.48) | −0.40 (small) | ||
| Use of sleep medication (Component 6) | 1.29 (1.18) | 1.32 (1.36) | 0.71 (1.08) | 0.86 (1.27) | 0.11 (negligible) | ||
| Daytime dysfunction (Component 7) | 1.43 (0.63) | 1.21 (0.63) | 1.25 (0.64) | 0.64 (0.56) | −0.57 (medium) | ||
| APS | |||||||
| All Items | 38.96 (6.24) | 37.57 (6.62) | 39.00 (7.59) | 38.39 (6.05) | 0.85 | 0.86 | 0.17 (negligible) |
| SCI | |||||||
| All Items | 13.39 (6.78) | 13.82 (5.68) | 16.46 (5.56) | 20.28 (5.01) | 0.81 | 0.78 | 0.66 (medium) |
| FIRST | |||||||
| All Items | 22.03 (6.86) | 23.07 (5.45) | 22.71 (6.51) | 23.21 (6.12) | 0.90 | 0.89 | −0.12 (negligible) |
| ISI | |||||||
| All Items | 11.75 (4.35) | 11.64 (4.33) | 11.32 (5.00) | 7.71 (3.89) | 0.82 | 0.83 | −0.78 (medium) |
| SHI | |||||||
| All Items | 29.61 (5.76) | 28.11 (4.72) | 28.57 (5.80) | 26.61 (5.29) | 0.61 | 0.64 | −0.12 (negligible) |
| Questionnaire | β Time*Group [95%CI] | Standardized β Time*Group [95%CI] | Unadjusted p-Value | Adjusted p-Value |
|---|---|---|---|---|
| ERQ | ||||
| Reappraisal | −0.29 [−0.90; 0.36] | −0.13 [−0.35; 0.09] | 0.34 | 0.51 |
| Suppression | 0.37 [−0.25; 0.98] | 0.16 [−0.11; 0.42] | 0.24 | 0.42 |
| FFMQ | ||||
| All Items | 0.12 [−0.01; 0.26] | 0.13 [−0.01; 0.27] | 0.06 | 0.16 |
| Observing | 0.03 [−0.22; 0.29] | 0.02 [−0.15; 0.20] | 0.78 | 0.78 |
| Describing | 0.16 [−0.04; 0.37] | 0.11 [−0.03; 0.25] | 0.11 | 0.23 |
| Acting with awareness | 0.08 [−0.17; 0.34] | 0.06 [−0.12; 0.24] | 0.51 | 0.68 |
| Non-judging of inner experience | 0.07 [−0.30; 0.44] | 0.04 [−0.18; 0.26] | 0.72 | 0.76 |
| Non-reactivity to inner experience | 0.29 [0.06; 0.52] | 0.23 [0.04; 0.41] | 0.01 | 0.04 |
| PSQI | ||||
| All Items | −1.93 [−3.43; −0.42] | −0.25 [−0.45; −0.05] | 0.01 | 0.04 |
| Subjective sleep quality | −0.53 [−0.85; −0.22] | −0.40 [−0.64; −0.16] | 0.001 | 0.02 |
| Sleep latency | 0.21 [−0.21; 0.63] | 0.11 [−0.10; 0.31] | 0.31 | 0.50 |
| Sleep duration | −0.54 [−0.92; −0.15] | −0.30 [−0.52; −0.09] | 0.007 | 0.04 |
| Sleep efficiency | −0.54 [−1.16; 0.09] | −0.23 [−0.49; 0.04] | 0.09 | 0.21 |
| Sleep disturbance | −0.25 [−0.58; 0.08] | −0.21 [−0.48; 0.06] | 0.13 | 0.25 |
| Use of sleep medication | 0.11 [−0.39; 0.60] | 0.04 [−0.16; 0.24] | 0.66 | 0.73 |
| Daytime dysfunction | −0.39 [−0.76; −0.03] | −0.29 [−0.56; −0.02] | 0.03 | 0.09 |
| APS | ||||
| All Items | 0.79 [−1.68; 3.25] | 0.06 [−0.13; 0.25] | 0.52 | 0.68 |
| SCI | ||||
| All Items | 3.39 [0.66; 6.13] | 0.27 [0.05; 0.49] | 0.02 | 0.07 |
| FIRST | ||||
| All Items | −0.54 [−2.97; 1.90] | −0.04 [−0.24; 0.15] | 0.66 | 0.73 |
| ISI | ||||
| All Items | −3.50 [−5.86; −1.14] | −0.38 [−0.63; −0.12] | 0.004 | 0.04 |
| SHI | ||||
| All Items | −0.46 [−2.44; 1.52] | −0.04 [−0.23; 0.14] | 0.64 | 0.73 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fazia, T.; Bubbico, F.; Nova, A.; Bruno, S.; Iozzi, D.; Calgan, B.; Caimi, G.; Terzaghi, M.; Manni, R.; Bernardinelli, L. Beneficial Effects of an Online Mindfulness-Based Intervention on Sleep Quality in Italian Poor Sleepers during the COVID-19 Pandemic: A Randomized Trial. Int. J. Environ. Res. Public Health 2023, 20, 2724. https://doi.org/10.3390/ijerph20032724
Fazia T, Bubbico F, Nova A, Bruno S, Iozzi D, Calgan B, Caimi G, Terzaghi M, Manni R, Bernardinelli L. Beneficial Effects of an Online Mindfulness-Based Intervention on Sleep Quality in Italian Poor Sleepers during the COVID-19 Pandemic: A Randomized Trial. International Journal of Environmental Research and Public Health. 2023; 20(3):2724. https://doi.org/10.3390/ijerph20032724
Chicago/Turabian StyleFazia, Teresa, Francesco Bubbico, Andrea Nova, Salvatore Bruno, Davide Iozzi, Beril Calgan, Giancarlo Caimi, Michele Terzaghi, Raffaele Manni, and Luisa Bernardinelli. 2023. "Beneficial Effects of an Online Mindfulness-Based Intervention on Sleep Quality in Italian Poor Sleepers during the COVID-19 Pandemic: A Randomized Trial" International Journal of Environmental Research and Public Health 20, no. 3: 2724. https://doi.org/10.3390/ijerph20032724