

Iron Deficiency among School-Aged Adolescents in Hong Kong: Prevalence, Predictors, and Effects on Health-Related Quality of Life
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Definitions of ID and IDA
2.3. Factors Associated with Iron Stores
2.4. Functional Outcomes
2.5. Statistical Analysis
3. Results
3.1. Hematological Findings in the Overall Cohort
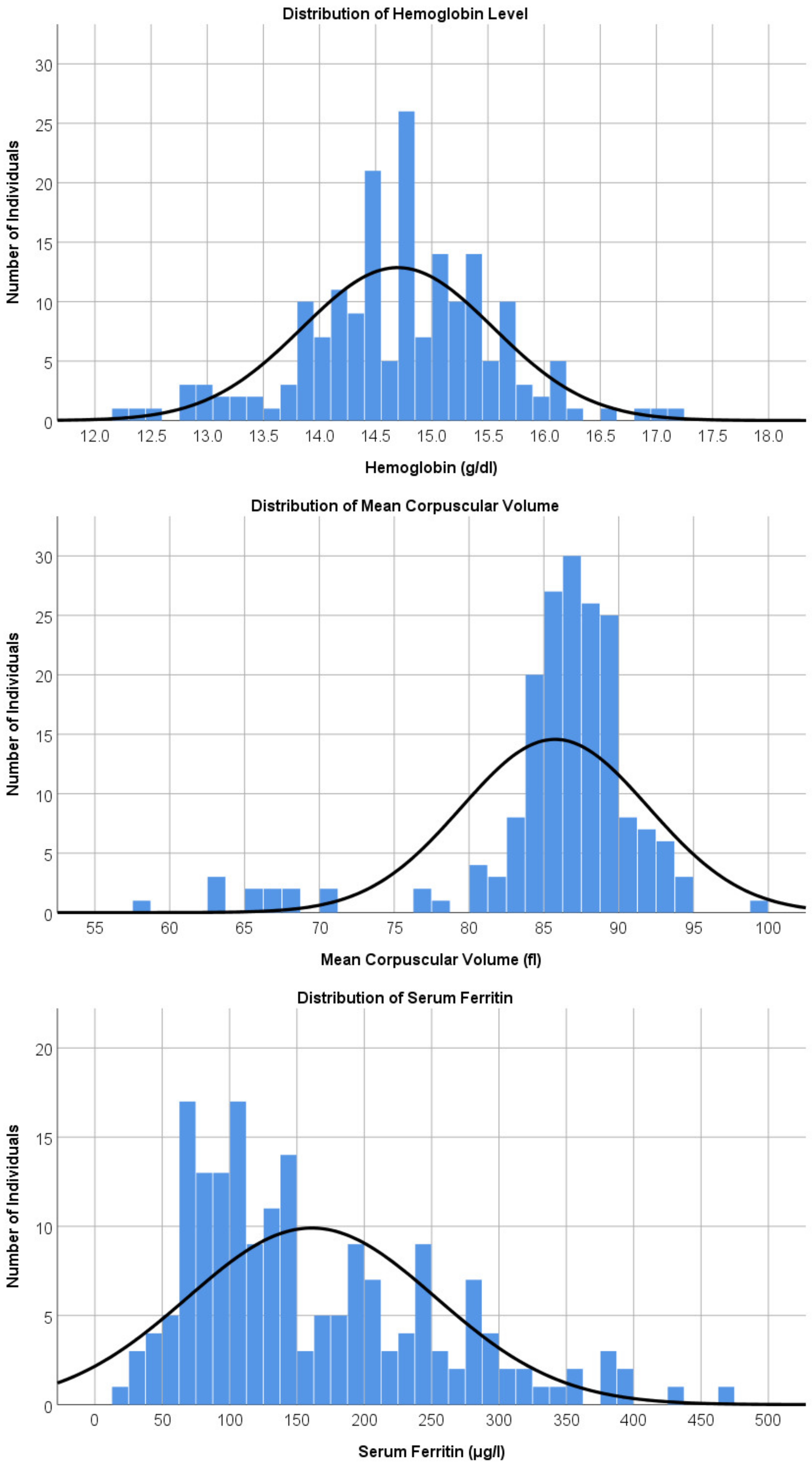
3.2. Hematological Findings in Boys
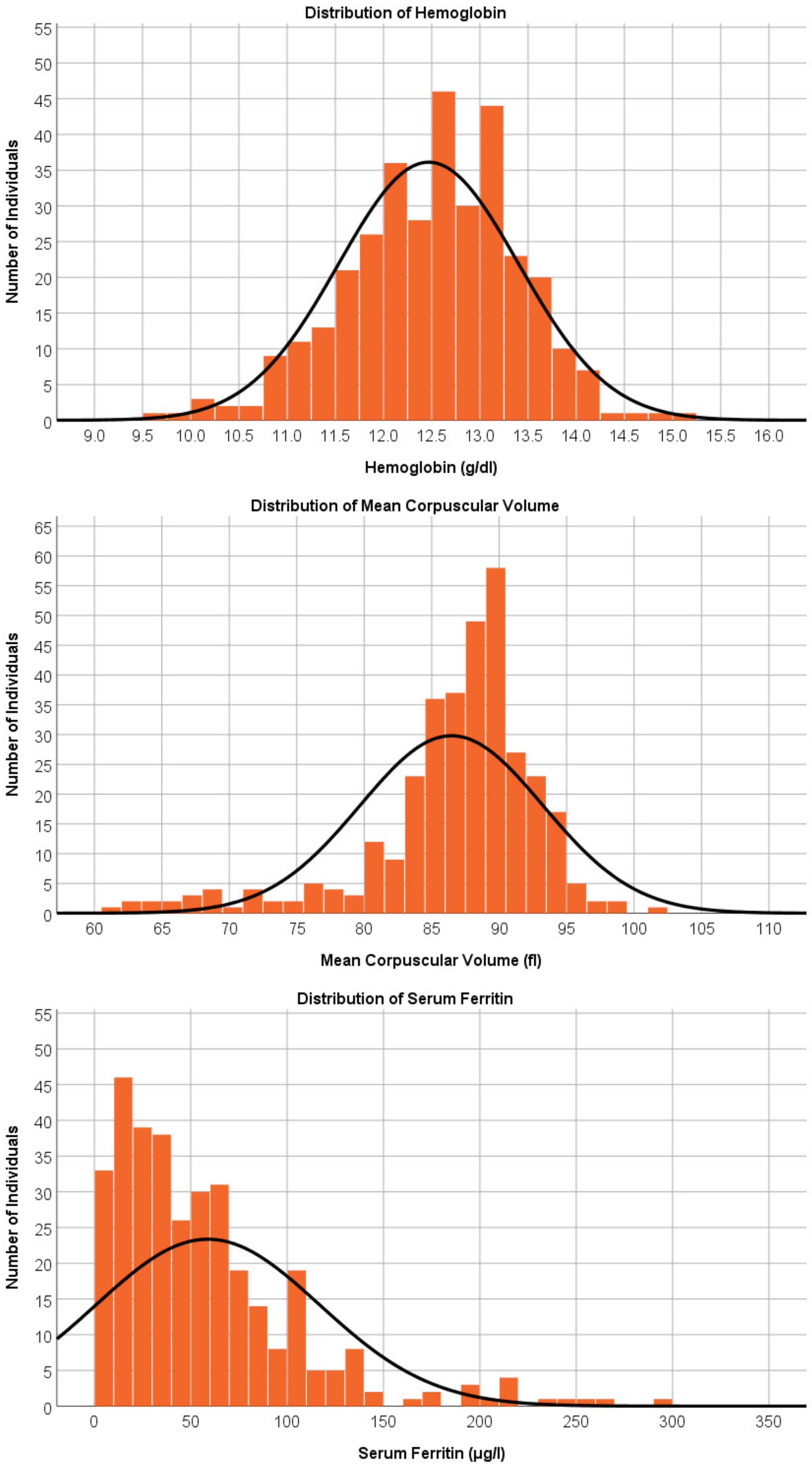
3.3. Hematological Findings in Girls
3.4. Association between Dietary Characteristics and Iron Store
3.5. Association between Weight Status and Iron Store
3.6. Association between Menstrual Characteristics and Iron Store
3.7. Association between Iron Store and HRQoL
3.8. Association between Iron Store and Fatigue
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reiner, R.C., Jr.; Olsen, H.E.; Ikeda, C.T.; Echko, M.M.; Ballestreros, K.E.; Manguerra, H.; Martopullo, I.; Millear, A.; Shields, C.; Smith, A.; et al. Diseases, Injuries, and Risk Factors in Child and Adolescent Health, 1990 to 2017: Findings from the Global Burden of Diseases, Injuries, and Risk Factors 2017 Study. JAMA Pediatr. 2019, 173, e190337. [Google Scholar] [PubMed] [Green Version]
- Kyu, H.H.; Pinho, C.; Wagner, J.A.; Brown, J.C.; Bertozzi-Villa, A.; Charlson, F.J.; Coffeng, L.E.; Dandona, L.; Erskine, H.E.; Ferrari, A.J.; et al. Global and National Burden of Diseases and Injuries Among Children and Adolescents Between 1990 and 2013: Findings from the Global Burden of Disease 2013 Study. JAMA Pediatr. 2016, 170, 267–287. [Google Scholar] [PubMed] [Green Version]
- Wang, J.Y.; Hu, P.J.; Luo, D.M.; Dong, B.; Ma, Y.; Dai, J.; Song, Y.; Ma, J.; Lau, P.W.C. Reducing Anemia Among School-Aged Children in China by Eliminating the Geographic Disparity and Ameliorating Stunting: Evidence from a National Survey. Front. Pediatr. 2020, 8, 193. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Huo, J.; Chen, D.; Man, Q.; Tang, Y.; Zhang, J.; Huang, J. Iron Status Among Children Aged 6−17 Years by Serum Ferritin—China, 2016−2017. China CDC Wkly. 2021, 3, 221–225. [Google Scholar] [CrossRef]
- Regional Office for South-East Asia, World Health Organization. Prevention of Iron Deficiency Anaemia in Adolescents. 2011. Available online: https://apps.who.int/iris/handle/10665/205656 (accessed on 29 December 2022).
- Camaschella, C.; Weiss, G. Regulation of Iron Balance; UpToDate: Waltham, MA, USA, 2022; Available online: https://medilib.ir/uptodate/show/7105 (accessed on 29 December 2022).
- Camaschella, C.; Girelli, D. The changing landscape of iron deficiency. Mol. Asp. Med. 2020, 75, 100861. [Google Scholar] [CrossRef] [PubMed]
- Camaschella, C.; Nai, A.; Silvestri, L. Iron metabolism and iron disorders revisited in the hepcidin era. Haematologica 2020, 105, 260–272. [Google Scholar] [CrossRef] [Green Version]
- Hare, D.J.; Cardoso, B.R.; Szymlek-Gay, E.A.; Biggs, B.A. Neurological effects of iron supplementation in infancy: Finding the balance between health and harm in iron-replete infants. Lancet Child Adolesc Health 2018, 2, 144–156. [Google Scholar] [CrossRef]
- Camaschella, C. Iron deficiency. Blood 2019, 133, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Dosman, C.; Witmans, M.; Zwaigenbaum, L. Iron′s role in paediatric restless legs syndrome—A review. Paediatr. Child Health 2012, 17, 193–197. [Google Scholar] [CrossRef] [Green Version]
- Ji, X.; Cui, N.; Liu, J. Neurocognitive Function Is Associated with Serum Iron Status in Early Adolescents. Biol. Res. Nurs. 2017, 19, 269–277. [Google Scholar] [CrossRef]
- Yokoi, K.; Konomi, A. Iron deficiency without anaemia is a potential cause of fatigue: Meta-analyses of randomised controlled trials and cross-sectional studies. Br. J. Nutr. 2017, 117, 1422–1431. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Bourgeois, T.; Klima, J.; Berlan, E.D.; Fischer, A.N.; O’Brien, S.H. Iron deficiency and fatigue in adolescent females with heavy menstrual bleeding. Haemophilia 2013, 19, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.K.; Wong, H.K.; Hong, J.; Leung, J.N.; Tsoi, W.C.; Lin, C.K. A study of the predonation hemoglobin and iron status among Hong Kong Chinese blood donors. Transfusion 2013, 53, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Samson, K.L.I.; Fischer, J.A.J.; Roche, M.L. Iron Status, Anemia, and Iron Interventions and Their Associations with Cognitive and Academic Performance in Adolescents: A Systematic Review. Nutrients 2022, 14, 224. [Google Scholar] [CrossRef]
- WHO Guideline on Use of Ferritin Concentrations to Assess Iron Status in Individuals and Populations; World Health Organization: Geneva, Switzerland, 2020.
- WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. Vitamin and Mineral Nutrition Information System; World Health Organization: Geneva, Switzerland, 2011; Available online: http://www.who.int/vmnis/indicators/haemoglobin.pdf (accessed on 29 December 2022).
- Lau, Y.L.; Chan, L.C.; Chan, Y.Y.; Ha, S.Y.; Yeung, C.Y.; Waye, J.S.; Chui, D.H. Prevalence and genotypes of alpha- and beta-thalassemia carriers in Hong Kong—Implications for population screening. N. Engl. J. Med. 1997, 336, 1298–1301. [Google Scholar] [CrossRef] [Green Version]
- Student Health Service, Department of Health, The Government of the Hong Kong Special Administrative Region. Iron Deficiency Anaemia. Available online: https://www.studenthealth.gov.hk/english/health/health_ophp/health_ophp_ane.html (accessed on 20 July 2022).
- Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion. Growth Charts. Available online: https://www.cdc.gov/growthcharts/index.htm (accessed on 29 December 2022).
- Hao, Y.; Tian, Q.; Lu, Y.; Chai, Y.; Rao, S. Psychometric properties of the Chinese version of the Pediatric Quality of Life Inventory™ 4.0 generic core scales. Qual. Life Res. 2010, 19, 1229–1233. [Google Scholar] [CrossRef]
- Ye, Q.; Liu, K.; Wang, J.; Bu, X.; Zhao, L. Reliability and validity of the Chinese version of the PedsQL Multidimensional Fatigue Scale in children with acute leukemia. Int. J. Nurs. Sci. 2016, 3, 146–152. [Google Scholar] [CrossRef] [Green Version]
- Fanelli, S.; Walls, C.; Taylor, C. Skipping breakfast is associated with nutrient gaps and poorer diet quality among adults in the United States. Proc. Nutr. Soc. 2021, 80, E48. [Google Scholar] [CrossRef]
- Deshmukh-Taskar, P.R.; Radcliffe, J.D.; Liu, Y.; Nicklas, T.A. Do breakfast skipping and breakfast type affect energy intake, nutrient intake, nutrient adequacy, and diet quality in young adults? NHANES 1999–2002. J. Am. Coll. Nutr. 2010, 29, 407–418. [Google Scholar] [CrossRef] [PubMed]
- Giménez-Legarre, N.; Miguel-Berges, M.L.; Flores-Barrantes, P.; Santaliestra-Pasías, A.M.; Moreno, L.A. Breakfast Characteristics and Its Association with Daily Micronutrients Intake in Children and Adolescents—A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 3201. [Google Scholar] [CrossRef] [PubMed]
- Beck, K.L.; Conlon, C.A.; Kruger, R.; Coad, J. Dietary determinants of and possible solutions to iron deficiency for young women living in industrialized countries: A review. Nutrients 2014, 6, 3747–3776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansur, M.A.; Indriasari, R.; Jafar, N. Body image and weight-control behaviors among adolescent girls with low-mid socioeconomic background. Enfermería Clínica 2020, 30, 285–289. [Google Scholar] [CrossRef]
- Ohara, K.; Kato, Y.; Mase, T.; Kouda, K.; Miyawaki, C.; Fujita, Y.; Okita, Y.; Nakamura, H. Eating behavior and perception of body shape in Japanese university students. Eat Weight. Disord 2014, 19, 461–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noh, J.-W.; Kwon, Y.D.; Yang, Y.; Cheon, J.; Kim, J. Relationship between body image and weight status in east Asian countries: Comparison between South Korea and Taiwan. BMC Public Health 2018, 18, 814. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Jimenez, M.C.; Moreno, G.; Wright, I.; Shih, P.-C.; Vaquero, M.P.; Remacha, A.F. Iron Deficiency in Menstruating Adult Women: Much More than Anemia. Women’s Health Rep. 2020, 1, 26–35. [Google Scholar] [CrossRef] [Green Version]
- Pande, S.; Ranjan, R.; Kratasyuk, V.A. Is Body Mass Index a potential biomarker for anemia in obese adolescents? J. Nutr. Intermed. Metab. 2019, 15, 1–2. [Google Scholar] [CrossRef]
- Pinhas-Hamiel, O.; Newfield, R.S.; Koren, I.; Agmon, A.; Lilos, P.; Phillip, M. Greater prevalence of iron deficiency in overweight and obese children and adolescents. Int. J. Obes. Relat. Metab. Disord 2003, 27, 416–418. [Google Scholar] [CrossRef]
- Spencer, B.R.; Fox, M.P.; Wise, L.A.; Cable, R.G.; Mast, A.E. Iron status and self-reported fatigue in blood donors. Transfusion 2021, 61, 124–133. [Google Scholar] [CrossRef]
- Halterman, J.S.; Kaczorowski, J.M.; Aligne, C.A.; Auinger, P.; Szilagyi, P.G. Iron deficiency and cognitive achievement among school-aged children and adolescents in the United States. Pediatrics 2001, 107, 1381–1386. [Google Scholar] [CrossRef] [Green Version]
- Scott, S.P.; De Souza, M.J.; Koehler, K.; Murray-Kolb, L.E. Combined Iron Deficiency and Low Aerobic Fitness Doubly Burden Academic Performance among Women Attending University. J. Nutr. 2017, 147, 104–109. [Google Scholar] [CrossRef] [Green Version]
- Chyu, E.P.Y.; Chen, J.K. The Correlates of Academic Stress in Hong Kong. Int. J. Environ. Res. Public Health 2022, 19, 4009. [Google Scholar] [CrossRef] [PubMed]
- Pule, P.I.; Rachaba, B.; Magafu, M.G.; Habte, D. Factors associated with intention to donate blood: Sociodemographic and past experience variables. J. Blood Transfus. 2014, 2014, 571678. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | All (n = 523) n (%) | Male (n = 183) n (%) | Female (n = 340) n (%) |
|---|---|---|---|
| Age [mean SD] | 17.55 [1.05] | 17.47 [1.02] | 17.59 [1.06] |
| 16–16.9 years | 185 (35.4) | 69 (37.7) | 116 (34.1) |
| 17–17.9 years | 182 (34.8) | 64 (35.0) | 118 (34.7) |
| 18–18.9 years | 85 (16.2) | 27 (14.7) | 58 (17.1) |
| 19–19.9 years | 71 (13.6) | 23 (12.6) | 48 (14.1) |
| Weight status | |||
| Underweight (≤10th percentile) | 66 (12.6) | 28 (15.3) | 38 (11.2) |
| Normal (10 to <85th percentile) | 386 (73.8) | 117 (63.9) | 269 (79.1) |
| Overweight (from ≥85th to <95th percentile) | 43 (8.2) | 17 (9.3) | 26 (7.6) |
| Obese (≥95th percentile) | 28 (5.4) | 21 (11.5) | 7 (2.1) |
| Menstrual characteristics (Female) | |||
| Age menarche [mean SD] years | - | - | 12.17 [1.42] |
| Duration of flow [mean SD] days | - | - | 5.90 [2.96] |
| Menstrual cycle [mean SD] days | - | - | 32.00 [14.31] |
| Highest amount of sanitary products used on the heaviest day [mean SD] | - | - | 3.98 [1.41] |
| Average bleeding per cycle | |||
| Very little bleeding | - | - | 1 (0.3) |
| Low bleeding | - | - | 21 (6.2) |
| Moderate bleeding | - | - | 266 (78.7) |
| Heavy bleeding | - | - | 46 (13.6) |
| Very heavy bleeding | - | - | 4 (1.2) |
| Dietary characteristics | |||
| Regular habit of skipping ≥ 1 meal | 189 (36.3) | 51 (28.4) | 138 (40.6) |
| Skip breakfast | 149 (28.5) | 45 (24.6) | 104 (30.7) |
| Skip lunch | 29 (5.6) | 7 (3.8) | 22 (6.5) |
| Skip dinner | 41 (7.9) | 6 (3.3) | 35 (10.3) |
| Dietary iron score # [mean SD] | 97.78 [16.10] | 99.00 [16.44] | 97.13 [15.90] |
| All (n = 523) n (%) | Male (n = 183) n (%) | Female (n = 340) n (%) | |
|---|---|---|---|
| Iron deficiency (WHO definition) # | 58 (11.1) | 0 | 58 (17.1) |
| Iron deficiency anemia (WHO definition) ^ | 37 (7.1) | 0 | 37 (10.9) |
| Iron deficiency anemia (Local definition) * | 23 (4.4) | 0 | 23 (6.8) |
| Descriptive Data | Multivariable Analysis | ||
|---|---|---|---|
| Dietary Characteristics | Serum Ferritin Level Median (IQR) μg/L | Estimate (Standard Error) | p # |
| Regular habit of skipping ≥ 1 meal | |||
| Yes (n = 189, 36.3%) | 54.5 (23.1–105.0) | −35.2 (14.7) | 0.017 |
| No (n = 334, 63.7%) | 73.9 (39.2–136.2) | Reference group | |
| Regular habit of skipping breakfast | |||
| Yes (n = 149, 28.5%) | 56.1 (28.0–109.0) | −36.8 (15.6) | 0.019 |
| No (n = 374, 71.5%) | 73.0 (36.9–133.1) | Reference group | |
| Regular habit of skipping lunch | |||
| Yes (n = 29, 5.5%) | 37.8 (16.0–63.2) | −77.3 (30.5) | 0.011 |
| No (n = 495, 94.5%) | 71.2 (35.2–129.9) | Reference group | |
| Regular habit of skipping dinner | |||
| Yes (n = 41, 7.8%) | 45.8 (17.8–86.8) | −11.4 (26.4) | 0.66 |
| No (n = 482, 92.2%) | 71.2 (35.2–128.2) | Reference group | |
| Dietary iron score * | - | 0.74 (0.43) | 0.091 |
| Weight Status | Serum Ferritin Level Median (IQR) μg/L | Estimate (Standard Error) | p # |
| Underweight (n = 66, 12.6%) | 72.0 (32.0–145.9) | 4.9 (21.1) | 0.81 |
| Overweight/obese (n = 71, 13.6%) | 106.8 (40.9–235.8) | 82.8 (20.8) | <0.0001 |
| Normal weight (n = 386, 73.8%) | 64.9 (31.1–109.9) | Reference group | |
| Menstrual Characteristics (Girls only) | Serum Ferritin Level Median (IQR) μg/L | Estimate (Standard Error) | p^ |
| Bleeding severity | |||
| Heavy/very heavy bleeding (n = 50, 14.7%) | 34.0 (20.0–56.0) | −40.8 (20.2) | 0.043 |
| From very little to moderate bleeding (n = 288, 84.7%) | 45.8 (20.9–77.4) | Reference group | |
| Average amount of sanitary products on the heaviest day of the cycle * | - | −13.7 (5.1) | 0.0072 |
| Physical | Emotion | Social | School | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Est. | SE | p | Est. | SE | p | Est. | SE | p | Est. | SE | p | |
| Serum ferritin (per 10 μg/L) | 0.78 | 0.27 | 0.0047 | 0.41 | 0.42 | 0.32 | 0.036 | 0.32 | 0.91 | 0.81 | 0.40 | 0.045 |
| Habit of skipping meals | ||||||||||||
| Yes | −3.47 | 1.10 | 0.0017 | −3.69 | 1.65 | 0.026 | −1.24 | 1.33 | 0.35 | −3.85 | 1.73 | 0.027 |
| No | Ref | Ref | Ref | Ref | ||||||||
| Dietary iron score | 0.10 | 0.032 | 0.0014 | 0.036 | 0.049 | 0.46 | 0.032 | 0.039 | 0.41 | 0.13 | 0.051 | 0.010 |
| General Fatigue | Sleep Fatigue | Cognitive Fatigue | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Est. | SE | p | Est. | SE | p | Est. | SE | p | |
| Serum ferritin (per 10 μg/L) | 0.92 | 0.38 | 0.016 | 0.10 | 0.42 | 0.81 | −0.14 | 0.34 | 0.66 |
| Habit of skipping meals | |||||||||
| Yes | −2.58 | 1.55 | 0.097 | −4.04 | 1.39 | 0.0038 | −4.04 | 1.39 | 0.82 |
| No | Ref | Ref | Ref | ||||||
| Dietary iron score | 0.06 | 0.04 | 0.17 | 0.02 | 0.04 | 0.56 | 0.09 | 0.05 | 0.061 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheung, Y.T.; Chan, D.F.Y.; Lee, C.K.; Tsoi, W.C.; Lau, C.W.; Leung, J.N.S.; So, J.C.C.; Wong, C.L.P.; Tsang, S.T.Y.; Chu, Y.Y.L.; et al. Iron Deficiency among School-Aged Adolescents in Hong Kong: Prevalence, Predictors, and Effects on Health-Related Quality of Life. Int. J. Environ. Res. Public Health 2023, 20, 2578. https://doi.org/10.3390/ijerph20032578
Cheung YT, Chan DFY, Lee CK, Tsoi WC, Lau CW, Leung JNS, So JCC, Wong CLP, Tsang STY, Chu YYL, et al. Iron Deficiency among School-Aged Adolescents in Hong Kong: Prevalence, Predictors, and Effects on Health-Related Quality of Life. International Journal of Environmental Research and Public Health. 2023; 20(3):2578. https://doi.org/10.3390/ijerph20032578
Chicago/Turabian StyleCheung, Yin Ting, Dorothy Fung Ying Chan, Cheuk Kwong Lee, Wai Chiu Tsoi, Ching Wa Lau, Jennifer Ngar Sze Leung, Jason Chi Chiu So, Chris Lei Po Wong, Stella Tsui Ying Tsang, Yvonne Yuen Ling Chu, and et al. 2023. "Iron Deficiency among School-Aged Adolescents in Hong Kong: Prevalence, Predictors, and Effects on Health-Related Quality of Life" International Journal of Environmental Research and Public Health 20, no. 3: 2578. https://doi.org/10.3390/ijerph20032578