
Preventive Behaviors and Influencing Factors among Thai Residents in Endemic Areas during the Highest Epidemic Peak of the COVID-19 Outbreak
 and
and
Abstract
:1. Introduction
2. Materials and Methods
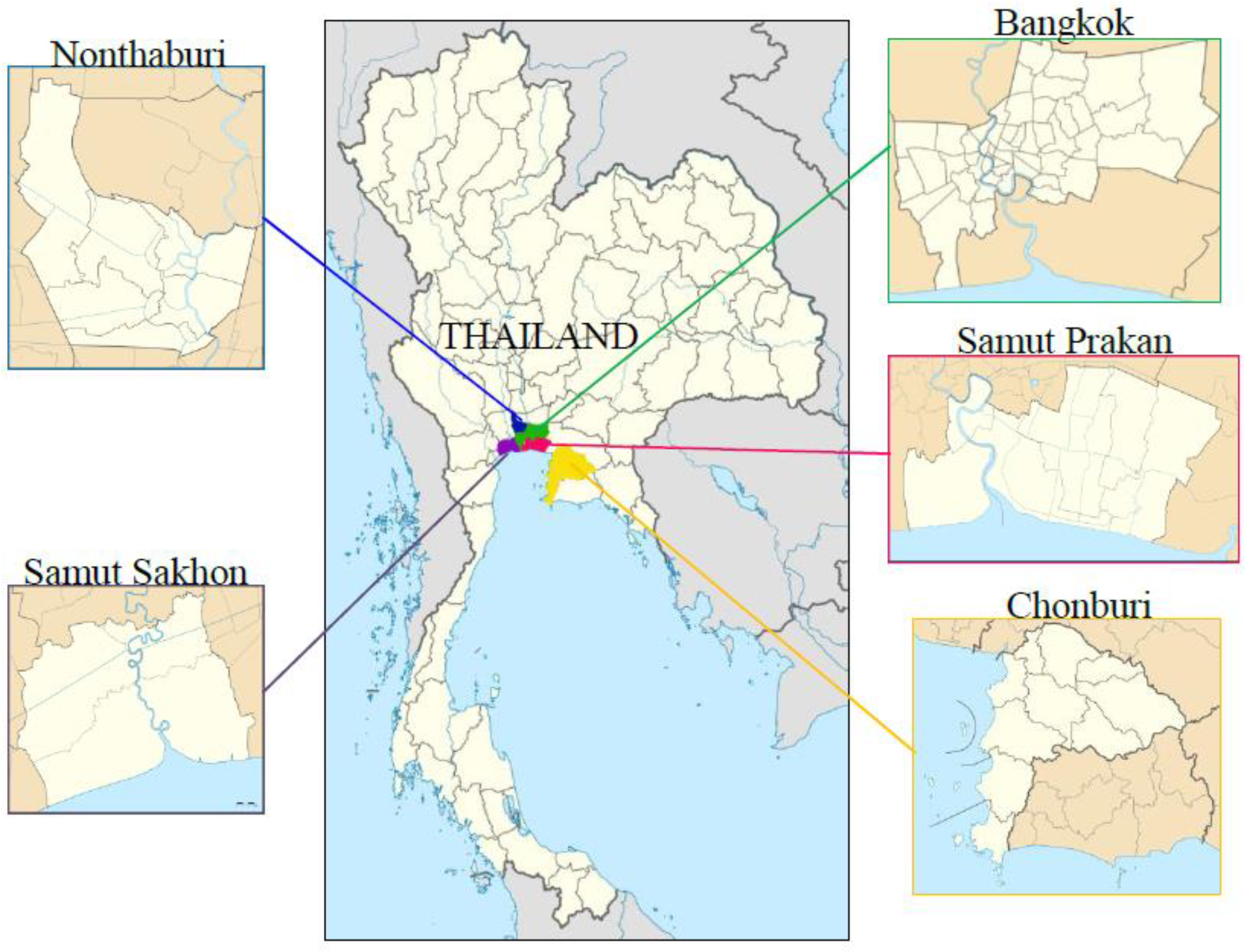
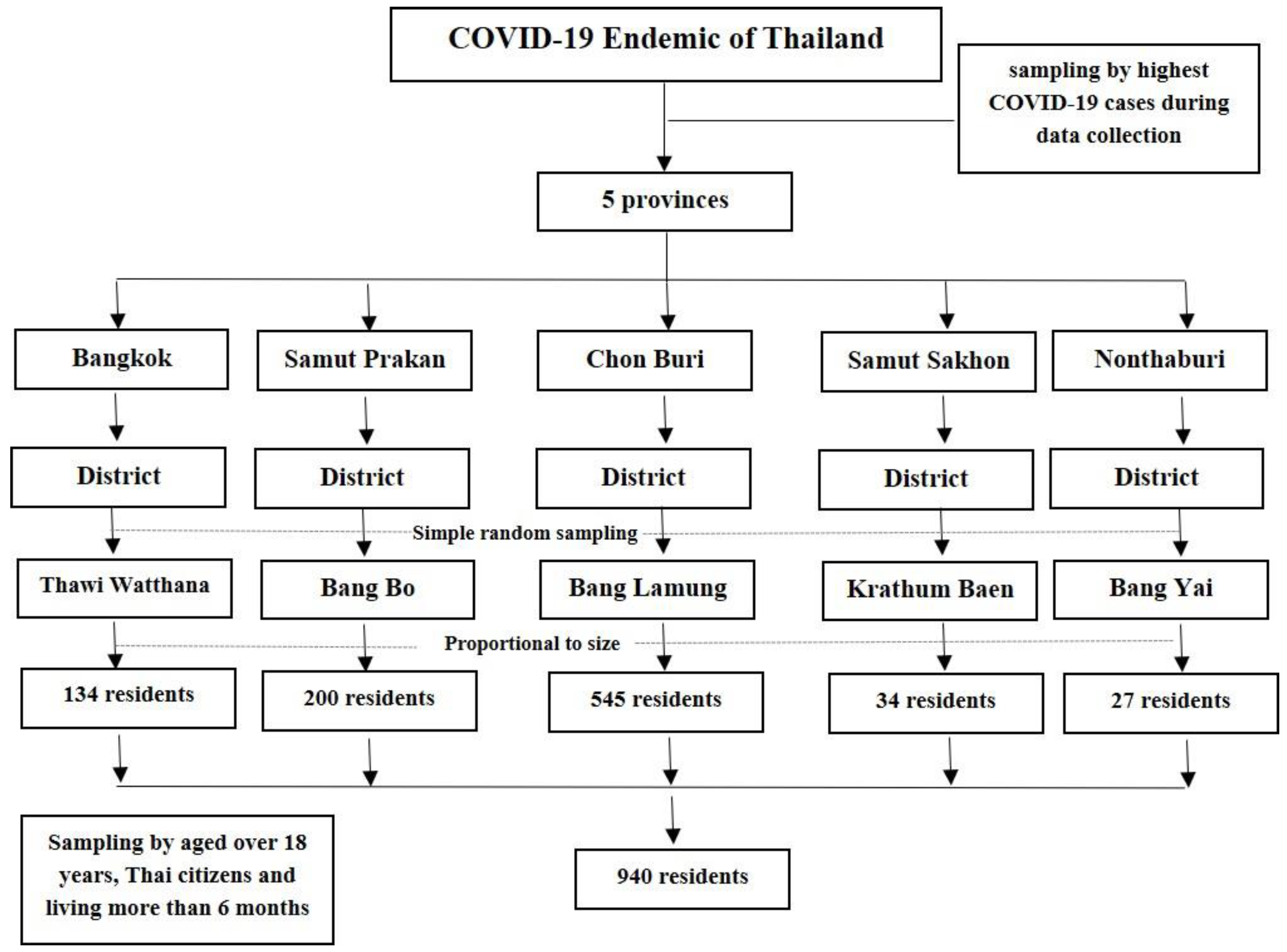
2.1. Study Design and Setting
2.2. Participants
2.3. Measurement
2.4. Data Collection
2.5. Statistical Procedures and Analysis
3. Results
3.1. Sociodemographic Characteristics of Residents
3.2. Knowledge and Attitude Levels on COVID-19 Prevention
3.3. Preventive Behavior Level toward COVID-19
3.4. Association between the Independent and Dependent Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahmed, H.M. Adherence to COVID-19 preventive measures among male medical students, Egypt. J. Egypt. Public Health Assoc. 2022, 97, 8. [Google Scholar] [CrossRef]
- World Health Organization. Statement on the Second Meeting of the International Health Regulations Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV); World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Lakshmi, P.S.; Suresh, M. Factors influencing the epidemiological characteristics of pandemic COVID-19: A TISM approach. Int. J. Healthc. Manag. 2020, 13, 89–98. [Google Scholar] [CrossRef] [Green Version]
- Joshi, A.; Kaur, M.; Kaur, R.; Grover, A.; Nash, D.; El-Mohandes, A. Predictors of COVID-19 vaccine acceptance, intention, and hesitancy: A scoping review. Front. Public Health 2021, 9, 698111. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19: Coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [Green Version]
- CDC: Use Masks to Slow the Spread of COVID-19. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/diy-cloth-facecoverings.html (accessed on 30 March 2022).
- Stasielowicz, L. A continuous time meta-analysis of the relationship between conspiracy beliefs and individual preventive behavior during the COVID-19 pandemic. Sci. Rep. 2022, 12, 11508. [Google Scholar] [CrossRef]
- Paiva, T.O.; Cruz-Martins, N.; Pasion, R.; Almeida, P.R.; Barbosa, F. Boldness personality traits are associated with reduced risk perceptions and adoption of protective behaviors during the first COVID-19 outbreak. Front. Psychol. 2021, 12, 974. [Google Scholar] [CrossRef]
- The Standard Team: Prime Minister Declares State of Emergency Effective 26 March in Response to COVID-19; Maintains There Is No Curfew Yet. Available online: https://thestandard.co/promulgating-the-emergency-decree/ (accessed on 30 March 2022).
- Department of Disease Control Ministry of Public Health: Guidelines for Vaccinating against COVID-19 in an Outbreak Situation in 2021 of Thailand (Thai). Available online: https://ddc.moph.go.th/vaccine-covid19/getFiles/11/1628849610213.pdf (accessed on 30 March 2022).
- Department of Disease Control Ministry of Public Health: COVID-19 Infected Situation (Thai). Available online: https://ddc.moph.go.th/covid19-dashboard/ (accessed on 15 January 2022).
- Coronavirus: Travel Restrictions, Border Shutdowns by Country. Available online: https://www.aljazeera.com/news/2020/6/3/coronavirustravel-restrictions-border-shutdowns-bycountry (accessed on 20 February 2022).
- Karimy, M.; Bastami, F.; Sharifat, R.; Heydarabadi, A.B.; Hatamzadeh, N.; Pakpour, A.H.; Cheraghian, B.; Zamani-Alavijeh, F.; Jasemzadeh, M.; Araban, M. Factors related to preventive COVID-19 behaviors using health belief model among general population: A cross-sectional study in Iran. BMC Public Health 2021, 21, 1934. [Google Scholar] [CrossRef]
- Mahmud, S.; Mohsin, M.; Khan, I.A.; Mian, A.U.; Zaman, M.A. Knowledge, beliefs, attitudes and perceived risk about COVID-19 vaccine and determinants of COVID-19 vaccine acceptance in Bangladesh. PLoS ONE 2021, 16, e0257096. [Google Scholar] [CrossRef]
- Zhong, B.L.; Luo, W.; Li, H.M.; Zhang, Q.Q.; Liu, X.G.; Li, W.T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Biol. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef] [Green Version]
- Ilesanmi, O.; Alele, F.O. Knowledge, attitude and perception of ebola virus disease among secondary school students in Ondo State, Nigeria, October, 2014. PLoS Curr. 2016, 8. [Google Scholar] [CrossRef]
- Lau, J.T.; Kim, J.H.; Tsui, H.; Griffiths, S. Perceptions related to human avian influenza and their associations with anticipated psychological and behavioral responses at the onset of outbreak in the Hong Kong Chinese general population. Am. J. Infect. Control 2007, 35, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Oh, S. Factors associated with preventive behaviors for COVID-19 among adolescents in South Korea. J. Pediatr. Nurs. 2022, 62e, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Ichinose, T. The Impact of the COVID-19 pandemic on the general public in urban and rural areas in Southern Japan. Sustainability 2022, 14, 2277. [Google Scholar] [CrossRef]
- Huang, Q.; Jackson, S.; Derakhshan, S.; Lee, L.; Pham, E.; Jackson, A.; Cutter, S.L. Urban-rural differences in COVID-19 exposures and outcomes in the South: A preliminary analysis of South Carolina. PLoS ONE 2021, 16, e0246548. [Google Scholar] [CrossRef] [PubMed]
- Peters, D.J. Community susceptibility and resiliency to COVID-19 across the rural-urban continuum in the United States. J. Rural Health 2020, 36, 446–456. [Google Scholar] [CrossRef]
- Person, B.; Sy, F.; Holton, K.; Govert, B.; Liang, A. National Center for Inectious Diseases/SARS Community Outreach Team. Fear and stigma: The epidemic within the SARS outbreak. Emerg. Infect. Dis. 2004, 10, 358–363. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Historical origins of the health belief model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Becker, M.H. The health belief model and personal health behavior. Health Educ. Monogr. 1974, 2, 324–473. [Google Scholar] [CrossRef]
- Charan, J.; Biswas, T. How to Calculate Sample Size for Different Study Designs in Medical Research? Indian J. Psychol. Med. 2013, 35, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Kamacooko, O.; Kitonsa, J.; Bahemuka, U.M.; Kibengo, F.M.; Wajja, A.; Basajja, V.; Lumala, A.; Kakande, A.; Kafeero, P.; Ssemwanga, E.; et al. Knowledge, attitudes, and practices regarding COVID-19 among healthcare workers in Uganda: A cross-sectional survey. Int. J. Environ. Res. Public Health 2021, 18, 7004. [Google Scholar] [CrossRef]
- Masoud, A.T.; Zaazouee, M.S.; Elsayed, S.M.; Ragab, K.M.; Kamal, E.M.; Alnasser, Y.T.; Assar, A.; Nourelden, A.Z.; Istatiah, L.J.; Abd-Elgawad, M.M.; et al. KAP-COVID GLOBAL: A multinational survey of the levels and determinants of public knowledge, attitudes and practices towards COVID-19. BMJ Open 2021, 11, e043971. [Google Scholar] [CrossRef]
- Park, D.I. Development and validation of a knowledge, attitudes and practices questionnaire on COVID-19 (KAP COVID-19). Int. J. Environ. Res. Public Health 2021, 18, 7493. [Google Scholar] [CrossRef] [PubMed]
- Chokkanchitchai, S. COVID-19 vaccine with “Herd Immunity” in Thailand. J. Prev. Med. Assoc. Thail. 2021, 11, 1. [Google Scholar]
- Potisopha, W.; Saensom, D.; Noonark, C.; Kabkumba, C.; Pearkao, C. Factors impacting COVID-19 preventive behaviors in Thai adults during the initial phase of vaccination. J. Public Health Dev. 2022, 20, 236–248. [Google Scholar]
- Abdelhafiz, A.S.; Mohammed, Z.; Ibrahim, M.E.; Ziady, H.H.; Alorabi, M.; Ayyad, M.; Sultan, E.A. Knowledge, perceptions, and attitude of Egyptians towards the novel coronavirus disease (COVID-19). J. Community Health 2020, 45, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Feroz, A.S.; Ali, N.A.; Feroz, R.; Akber, N.; Meghani, S.N. Exploring community perceptions, attitudes and practices regarding the COVID-19 pandemic in Karachi, Pakistan. BMJ Open 2021, 11, e048359. [Google Scholar] [CrossRef] [PubMed]
- Waewwab, P.; Pan-ngum, W.; Siri, S.; Bhopdhornangkul, B.; Mahikul, W. Knowledge, attitudes, and practices regarding “New Normal” guidelines and quality of life among Thai people during the COVID-19 outbreak: An online cross-sectional survey. Front. Public Health 2022, 10, 914417. [Google Scholar] [CrossRef] [PubMed]
- Kunno, J.; Yubonpunt, P.; Supawattanabodee, B.; Wiriyasirivaj, B.; Sumanasrethakul, C. COVID-19 knowledge, attitudes, and practices among healthcare worker in urban community Bangkok, Thailand. Rocz. Panstw. Zakl. Hig. 2022, 73, 17–26. [Google Scholar] [CrossRef]
- Yodmai, K.; Pechrapa, K.; Kittipichai, W.; Charupoonpol, P.; Suksatan, W. Factors associated with good COVID-19 preventive behaviors among older adults in urban communities in Thailand. J. Prim. Care Community Health 2021, 12, 21501327211036251. [Google Scholar] [CrossRef]
- Rojpaisarnkit, K.; Kaewpan, W.; Pengpid, S.; Peltzer, K. COVID-19 preventive behaviors and influencing factors in the Thai population: A web-based survey. Front. Public Health 2022, 10, 816464. [Google Scholar] [CrossRef]
- Kim, E.; Shepherd, M.E.; Clinton, J.D. The effect of big-city news on rural America during the COVID-19 pandemic. Proc. Natl. Acad. Sci. USA 2020, 117, 22009–22014. [Google Scholar] [CrossRef] [PubMed]
- Shiina, A.; Niitsu, T.; Kobori, O.; Idemoto, K.; Hashimoto, T.; Sasaki, T.; Igarashi, Y.; Shimizu, E.; Nakazato, M.; Hashimoto, K.; et al. Relationship between perception and anxiety about COVID-19 infection and risk behaviors for spreading infection: A national survey in Japan. Brain Behav. Immun. Health 2020, 6, 100101. [Google Scholar] [CrossRef] [PubMed]
- Ohta, R.; Ryu, Y.; Sano, C. Fears related to COVID-19 among rural older people in Japan. Healthcare 2021, 9, 524. [Google Scholar] [CrossRef] [PubMed]
- Doung-ngern, P.; Suphanchaimat, R.; Panjangampatthana, A.; Janekrongtham, C.; Ruampoom, D.; Daochaeng, N.; Eungkanit, N.; Pisitpayat, N.; Srisong, N.; Yasopa, O.; et al. Case-control study of use of personal protective measures and risk for severe acute respiratory syndrome coronavirus 2 infection, Thailand. Emerg. Infect. Dis. 2020, 26, 2607–2616. [Google Scholar] [CrossRef]
- Chen, X.; Chen, H.H. Differences in preventive behaviors of COVID-19 between urban and rural residents: Lessons learned from a cross-sectional study in China. Int. J. Environ. Res. Public Health 2020, 17, 4437. [Google Scholar] [CrossRef]
- Hyun, W.I.; Hee, S.Y.; Ok, S.N. Infection preventive behaviors and its association with perceived threat and perceived social factors during the COVID-19 pandemic in South Korea: 2020 community health survey. BMC Public Health 2022, 22, 1381. [Google Scholar] [CrossRef]
- Al-Wutayd, O.; Mansour, A.E.; Aldosary, A.H.; Hamdan, H.Z.; Al-Batanony, M.A. Handwashing knowledge, attitudes, and practices during the COVID-19 pandemic in Saudi Arabia: A non-representative cross-sectional study. Sci. Rep. 2021, 11, 16769. [Google Scholar] [CrossRef]
- McGarrity, L.A. Socioeconomic status as context for minority stress and health disparities among lesbian, gay, and bisexual individuals. Psychol. Sex Orientat. Gend. Divers. 2014, 1, 383–397. [Google Scholar] [CrossRef]
- Pampel, F.C.; Krueger, P.M.; Denney, J.T. Socioeconomic disparities in health behaviors. Annu. Rev. Sociol. 2010, 36, 349–370. [Google Scholar]
- Pothisa, T.; Ong-Artborirak, P.; Seangpraw, K.; Tonchoy, P.; Kantow, S.; Auttama, N.; Boonyathee, S.; Choowanthanapakorn, M.; Bootsikeaw, S.; Panta, P.; et al. Knowledge of COVID-19 and its relationship with preventive behaviors and vaccination among adults in Northern Thailand’s community. Int. J. Environ. Res. Public Health 2022, 19, 1521. [Google Scholar] [CrossRef]
- Kamate, S.K.; Sharma, S.; Thakar, S.; Srivastava, D.; Sengupta, K.; Hadi, A.J.; Chaudhary, A.; Joshi, R.; Dhanker, K. Assessing knowledge, attitudes and practices of dental practitioners regarding the COVID-19 pandemic: A multinational study. Dent. Med. Probl. 2020, 57, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Al Ahdab, S. A cross-sectional survey of knowledge, attitude and practice (KAP) towards COVID-19 pandemic among the Syrian residents. BMC Public Health 2021, 21, 296. [Google Scholar] [CrossRef] [PubMed]
- Upake, C.; Nanthamongkolchai, S.; Taechaboonsermsak, P.; Yodmai, K.; Suksatan, W. Factors predicting the Coronavirus Disease 2019 preventive behaviors of older adults: A cross-sectional study in Bangkok, Thailand. Int. J. Environ. Res. Public Health 2022, 19, 10361. [Google Scholar] [CrossRef] [PubMed]
- Shafiq, M.; Elharake, J.A.; Malik, A.A.; McFadden, S.M.; Aguolu, O.G.; Omer, S.B. COVID-19 sources of information, knowledge, and preventive behaviors among the US adult population. J. Public Health Manag. Pract. 2021, 27, 278–284. [Google Scholar] [CrossRef]
- Komwong, D.; Prasanthanakul, J.; Phanasathit, M.; Wongwan, T. Prevalence of mental health problems and associated factors of Thai healthcare workers during the first wave of COVID-19 pandemic. J. Public Health Dev. 2022, 20, 106–119. [Google Scholar] [CrossRef]
- Assavanopakun, P.; Promkutkao, T.; Promkutkeo, S.; Sirikul, W. Perspectives and factors affecting the preventive behavior pertinent to COVID-19 among school employees in Chiang Mai, Thailand: A cross-sectional study. Int. J. Environ. Res. Public Health 2022, 19, 5662. [Google Scholar] [CrossRef]
- Siramaneerat, I. Perceptions, knowledge and self-defense behaviors regarding COVID-19 among employees at Rajamangala University of Technology Thanyaburi, Thailand. J. Health Res. 2020, 36, 794–801. [Google Scholar] [CrossRef]
- Li, X.; Lu, P.; Hu, L.; Huang, T.; Lu, L. Factors associated with mental health results among workers with income losses exposed to COVID-19 in China. Int. J. Environ. Res. Public Health 2020, 17, 5627. [Google Scholar] [CrossRef]
- Mou, T.J.; Afroz, K.A.; Haq, M.A.; Jahan, D.; Ahmad, R.; Islam, T.; Chowdhury, K.; Kumar, S.; Irfan, M.; Islam, M.S.; et al. The effect of socio-demographic factors in health-seeking behaviors among Bangladeshi residents during the first wave of COVID-19. Healthcare 2022, 10, 483. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Categories | Number, (%) |
|---|---|---|
| Gender | Male | 376 (39.7) |
| Female | 570 (60.3) | |
| Age | 18–24 | 100 (10.6) |
| 25–37 | 286 (30.2) | |
| 38–45 | 197 (20.8) | |
| 46–53 | 197 (20.8) | |
| 45+ | 166 (17.5) | |
| Education | Primary school | 206 (21.8) |
| Secondary school | 305 (32.2) | |
| Diploma degree | 182 (19.2) | |
| Bachelor’s degree and above | 253 (26.7) | |
| Marital status | Single/divorced | 424 (44.8) |
| Married | 522 (55.2) | |
| Occupation | Self-employed | 167 (17.7) |
| General employee | 371 (39.2) | |
| Student | 43 (4.5) | |
| Government sector | 88 (9.3) | |
| Private sector | 220 (23.3) | |
| Farmer | 8 (0.8) | |
| None | 49 (5.2) | |
| Income per month | Less than BHT 5000 | 173 (18.3) |
| BHT 5001–10,000 | 308 (32.6) | |
| More than BHT 10,000 | 165 (49.2) | |
| Number of vaccines received | 0 | 91 (9.6) |
| 1 | 24 (2.5) | |
| 2 | 315 (33.3) | |
| 3 | 399 (42.2) | |
| 4 | 177 (12.4) | |
| Have you had a COVID-19 infection before? | Yes | 503 (53.2) |
| No | 443 (46.8) | |
| Source of COVID-19 infection | Do not know | 99 (22.6) |
| Family member | 173 (39.4) | |
| Colleague | 105 (23.9) | |
| High-risk area | 60 (13.7) | |
| Other | 2 (0.5) | |
| Health insurance | Yes | 178 (18.8) |
| No | 768 (81.2) |
| Items and Level | Number | Percentage (%) |
|---|---|---|
| COVID-19 Knowledge Level | ||
| General | ||
| Low | 121 | 12.8 |
| High | 825 | 87.2 |
| Mean 2.72, SD 0.80, Range 1–5 | ||
| Preventive measures | ||
| Low | 329 | 34.8 |
| High | 617 | 65.2 |
| Mean 4.69, SD 0.96, Range 1–6 | ||
| COVID-19 attitude level | ||
| Risk perception | ||
| Poor | 507 | 53.6 |
| Good | 439 | 46.4 |
| Mean 22.60, SD 2.90, Range 16–29 | ||
| Mistrust | ||
| Poor | 666 | 70.4 |
| Good | 280 | 29.6 |
| Mean 21.80, SD 3.16, Range 12–30 | ||
| Items | Yes | |
|---|---|---|
| Number | % | |
| General knowledge | ||
| 1. There is currently a symptomatic treatment cure for COVID-19. | 922 | 97.5 |
| 2. All persons with COVID-19 will develop severe disease. | 117 | 12.4 |
| 3. Persons with COVID-19 can transmit the virus to others. | 815 | 86.2 |
| 4. It is not necessary for children to take measures to prevent infection by COVID-19. | 130 | 13.7 |
| 5. The bat consumption is the risk of COVID-19 infection. | 595 | 62.9 |
| Preventive measures | ||
| 6. Wearing facemasks can prevent one from acquiring infection by the COVID-19 virus. | 883 | 93.7 |
| 7. To prevent infection by COVID-19, individuals should avoid going to crowded places and avoid using public transport | 683 | 72.2 |
| 8. Not touching face can be reduced the infection of COVID-19. | 699 | 73.9 |
| 9. Isolating people infected with COVID-19 is an effective way to reduce the spread of the virus. | 928 | 98.1 |
| 10. Vaccination can be reduced the severity if infected with COVID-19. | 872 | 92.2 |
| 11. Two complete vaccinations are sufficient to prevent infection with COVID-19. | 377 | 39.9 |
| Items | Strongly Disagree n (%) | Disagree n (%) | Not Sure n (%) | Agree n (%) | Strongly Agree n (%) |
|---|---|---|---|---|---|
| Risk perception | |||||
| 1. I believe that I am low risk of COVID-19 infection. | 77 (8.1) | 179 (18.2) | 465 (49.2) | 149 (15.8) | 76 (8.0) |
| 2. I believe that I am low symptom if I infected COVID-19. | 22 (2.3) | 185 (19.6) | 611 (64.6) | 111 (11.7) | 17 (1.8) |
| 3. The mask wearing can be reduced the risk of COVID-19 infection. | 3 (0.3) | 4 (0.4) | 33 (3.5) | 436 (46.1) | 470 (49.7) |
| 4. The hand washing cannot be reduced the risk of COVID-19 infection. | 249 (26.3) | 241 (25.5) | 78 (8.2) | 249 (26.3) | 129 (13.6) |
| 5. The social distancing in the public area can be reduced the risk of COVID-19 infection. | 1 (0.1) | 8 (0.8) | 36 (3.8) | 474 (50.1) | 427 (45.1) |
| Mistrust issues | |||||
| 6. I am not concerned after knowing the number of COVID-19 case. | 104 (11.0) | 308 (32.6) | 155 (16.4) | 239 (25.3) | 140 (14.8) |
| 7. People who have been infected with COVID-19 should not be condemned by society. | 30 (3.2) | 28 (3.0) | 52 (5.5) | 242 (25.6) | 594 (62.8) |
| 8. When the government measures are announced, I will strictly follow. | 9 (1.0) | 10 (1.1) | 69 (7.3) | 363 (38.4) | 498 (52.3) |
| 9. Vaccination is very important. | 3 (0.3) | 7 (0.7) | 87 (9.2) | 358 (37.8) | 491 (51.9) |
| 10. The emergence of the COVID-19 is a fake | 330 (34.9) | 331 (32.9) | 210 (22.2) | 49 (5.2) | 46 (4.9) |
| 11. The COVID-19 outbreak is an attempt to reduce the world’s population. | 288 (30.4) | 222 (23.5) | 224 (23.7) | 145 (15.3) | 67 (7.1) |
| 12. People who spreads COVID-19 to others should be punished according to the law. | 61 (6.4) | 200 (21.1) | 215 (22.7) | 203 (21.5) | 267 (28.2) |
| Items | Never n (%) | Rarely n (%) | Sometimes n (%) | Mostly n (%) | Always n (%) |
|---|---|---|---|---|---|
| 1. Wearing facial masks in public areas | 0 (0) | 3 (0.3) | 8 (0.8) | 198 (20.4) | 742 (78.4) |
| 2. Keeping social distance in public areas | 0 (0) | 29 (3.1) | 64 (6.8) | 259 (27.4) | 594 (62.8) |
| 3. Washing hands frequently and using soap or hand sanitizer in the public area | 2 (0.2) | 14 (1.5) | 44 (4.7) | 288 (30.4) | 598 (63.2) |
| 4. Changing clothes before entering the house | 8 (0.8) | 62 (6.6) | 184 (19.5) | 243 (25.7) | 449 (47.5) |
| 5. Studying new information on COVID-19 prevention | 16 (1.7) | 112 (11.8) | 206 (21.8) | 278 (29.4) | 334 (35.3) |
| 6. Taking vitamin C frequently | 82 (8.7) | 147 (15.5) | 341 (36.0) | 208 (22.0) | 168 (17.8) |
| 7. Reducing travel to public areas | 13 (1.4) | 168 (17.8) | 279 (29.5) | 251 (26.5) | 235 (24.8) |
| 8. Focusing on working from home and online meetings | 198 (20.9) | 162 (17.1) | 136 (14.4) | 182 (19.2) | 268 (28.3) |
| 9. Reducing face, nose, and eye contact | 14 (1.5) | 30 (3.2) | 150 (15.9) | 343 (36.3) | 409 (43.2) |
| 10. Following all preventive behaviors above by how much | 2 (0.2) | 27 (2.9) | 78 (8.2) | 368 (38.9) | 471 (49.8) |
| Variable | Level of Preventive Behavior | CORa (95% CI)c | p-Value | AORb (95% CI)c | p-Value | |
|---|---|---|---|---|---|---|
| Poor (%) | Good (%) | |||||
| Gender | ||||||
| Male | 32.7 | 67.3 | 1 | |||
| Female | 36.0 | 70.0 | 1.13 (0.85–1.50) | 0.378 | ||
| Age | ||||||
| 18–24 | 23.0 | 77.0 | 3.04 (1.74–5.30) | <0.001 | 2.97 (1.68–5.25) | <0.001 |
| 25–37 | 29.0 | 71.0 | 2.22 (1.49–3.30) | <0.001 | 2.11 (1.39–3.21) | <0.001 |
| 38–45 | 27.9 | 72.1 | 2.34 (1.51–3.62) | <0.001 | 2.04 (1.30–3.21) | 0.002 |
| 46–53 | 27.4 | 72.6 | 2.40 (1.55–3.72) | <0.001 | 2.04 (1.30–3.21) | <0.001 |
| 54+ | 47.6 | 52.4 | 1 | 1 | ||
| Education | ||||||
| Primary school | 35.4 | 64.6 | 1 | |||
| Secondary school | 35.1 | 64.9 | 1.10 (0.72–1.47) | 0.934 | ||
| Diploma degree | 26.9 | 73.1 | 1.49 (0.96–2.30) | 0.074 | ||
| Bachelor’s degree and above | 25.7 | 74.3 | 1.58 (1.06–2.34) | 0.024 | ||
| Marital status | ||||||
| Single/divorced | 30.0 | 70.0 | 1.10 (0.83–1.45) | 0.500 | ||
| Married | 32.0 | 68.0 | 1 | |||
| Income | ||||||
| <10,000 | 35.3 | 64.7 | 1 | 1 | ||
| >10,000 | 27.7 | 73.3 | 1.50 (1.13–1.98) | 0.024 | 1.38 (1.03–1.86) | 0.031 |
| Vaccines received | ||||||
| 0 | 27.5 | 72.5 | 1 | |||
| 1–2 | 30.4 | 69.6 | 0.86 (0.51–1.14) | 0.590 | ||
| 3 | 34.8 | 65.2 | 0.70 (0.42–1.17) | 0.180 | ||
| 4 | 23.1 | 76.9 | 1.26 (0.67–2.37) | 0.468 | ||
| COVID-19 infection | ||||||
| Yes | 33.0 | 67.0 | 0.84 (0.64–1.11) | 0.241 | ||
| No | 29.4 | 70.6 | 1 | |||
| Insurance | ||||||
| Yes | 28.1 | 79.1 | 1.19 (0.83–1.70) | 0.339 | ||
| No | 31.8 | 68.2 | 1 | |||
| COVID-19 Knowledge | ||||||
| General | ||||||
| Low | 32.1 | 67.9 | 1 | 1 | ||
| High | 24.0 | 79.0 | 2.37 (1.71–3.02) | <0.001 | 2.21 (1.64–2.96) | <0.001 |
| Preventive measures | ||||||
| Low | 42.9 | 57.1 | 1 | 1 | ||
| High | 24.8 | 75.2 | 1.50 (0.96–2.33) | 0.072 | 1.52 (0.96–2.40) | 0.096 |
| COVID-19 attitude | ||||||
| Risk perception | ||||||
| Poor | 33.5 | 66.5 | 1 | |||
| Good | 28.2 | 71.8 | 1.28 (0.97–1.69) | 0.080 | ||
| Mistrust | ||||||
| Poor | 29.7 | 70.3 | 1 | |||
| Good | 34.3 | 65.7 | 0.81 (0.60–1.09) | 0.080 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ounsaneha, W.; Laosee, O.; Suksaroj, T.T.; Rattanapan, C. Preventive Behaviors and Influencing Factors among Thai Residents in Endemic Areas during the Highest Epidemic Peak of the COVID-19 Outbreak. Int. J. Environ. Res. Public Health 2023, 20, 2525. https://doi.org/10.3390/ijerph20032525
Ounsaneha W, Laosee O, Suksaroj TT, Rattanapan C. Preventive Behaviors and Influencing Factors among Thai Residents in Endemic Areas during the Highest Epidemic Peak of the COVID-19 Outbreak. International Journal of Environmental Research and Public Health. 2023; 20(3):2525. https://doi.org/10.3390/ijerph20032525
Chicago/Turabian StyleOunsaneha, Weerawat, Orapin Laosee, Thunwadee Tachapattaworakul Suksaroj, and Cheerawit Rattanapan. 2023. "Preventive Behaviors and Influencing Factors among Thai Residents in Endemic Areas during the Highest Epidemic Peak of the COVID-19 Outbreak" International Journal of Environmental Research and Public Health 20, no. 3: 2525. https://doi.org/10.3390/ijerph20032525