
Knee Laxity in the Menstrual Cycle after Anterior Cruciate Ligament Reconstruction: A Case Series
 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
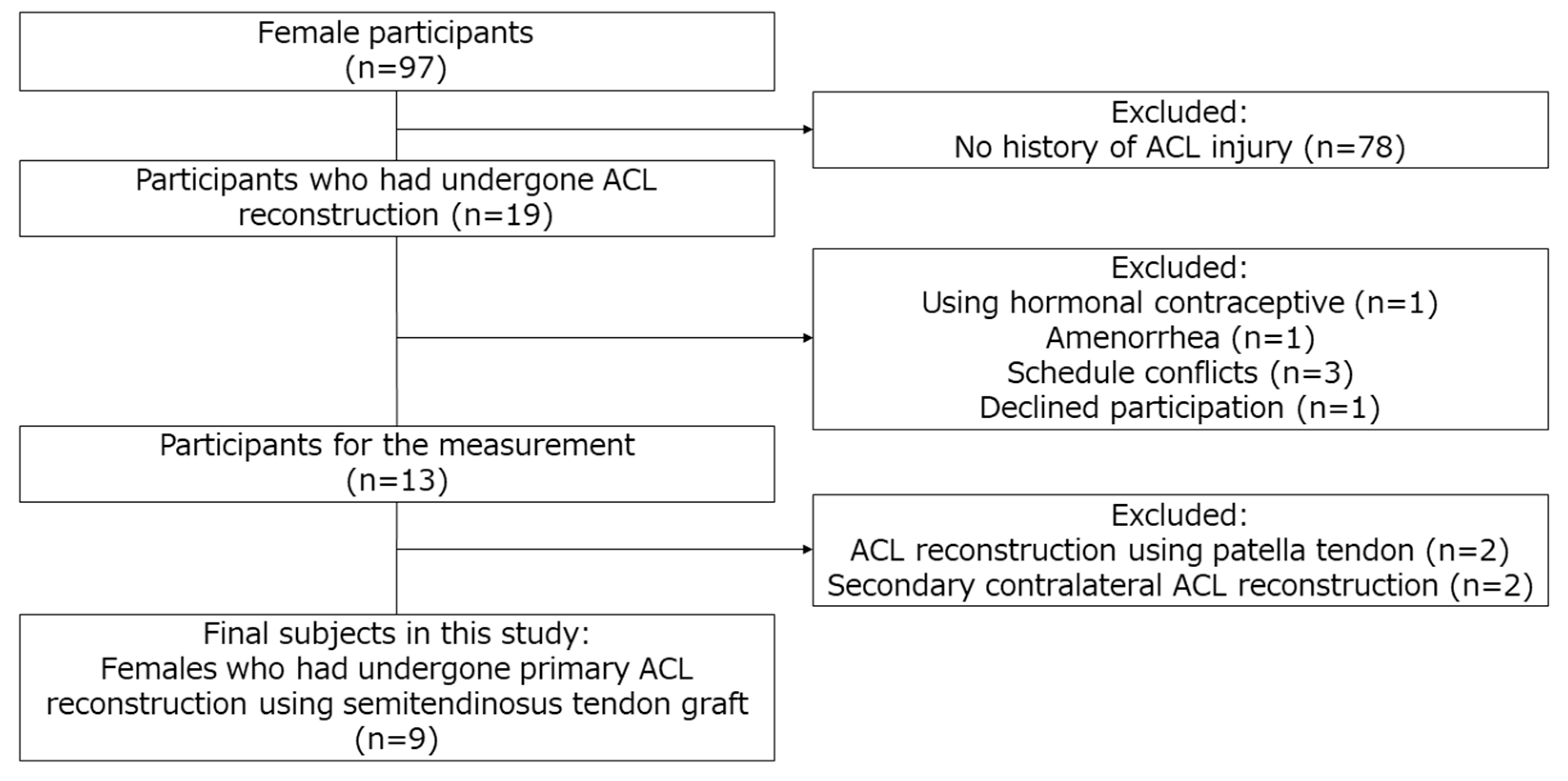
2.1. Subjects
2.2. Recording the Menstrual Cycle
2.3. Timing of Measurement
2.4. Measurement Methods
2.4.1. Estradiol Concentration
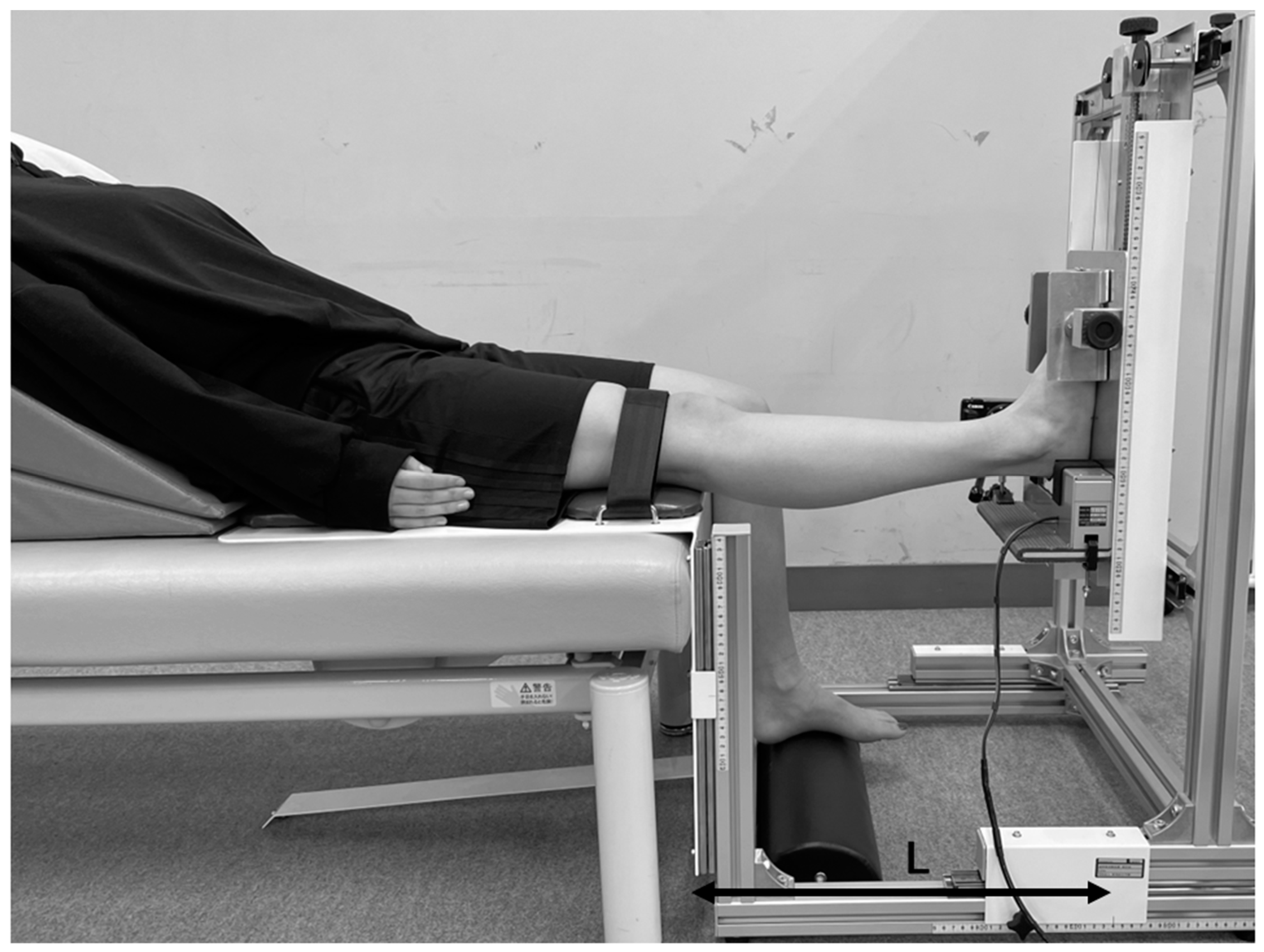
2.4.2. Anterior Knee Laxity
2.4.3. Genu Recurvatum
2.4.4. Muscle Stiffness
2.5. Reliability of Measurements
2.5.1. Test–Retest Reliability
2.5.2. Interrater Reliability
2.6. Statistical Analysis
3. Results
3.1. Comparison of the Early Follicular and Ovulatory Phases
3.2. Comparison of Reconstructed and Contralateral Sides
3.3. Reliability of Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ireland, M.L. The female ACL: Why is it more prone to injury? Orthop. Clin. North Am. 2002, 33, 637–651. [Google Scholar] [CrossRef] [Green Version]
- Arendt, E.A.; Agel, J.; Dick, R. Anterior cruciate ligament injury patterns among collegiate men and women. J. Athl. Train 1999, 34, 86–92. [Google Scholar] [PubMed]
- Somerson, J.S.; Isby, I.J.; Hagen, M.S.; Kweon, C.Y.; Gee, A.O. The menstrual cycle may affect anterior knee laxity and the rate of anterior cruciate ligament rupture: A systematic review and meta-analysis. JBJS Rev. 2019, 7, e2. [Google Scholar] [CrossRef] [PubMed]
- Beynnon, B.D.; Johnson, R.J.; Braun, S.; Sargent, M.; Bernstein, I.M.; Skelly, J.M.; Vacek, P.M. The relationship between menstrual cycle phase and anterior cruciate ligament injury: A case-control study of recreational alpine skiers. Am. J. Sports Med. 2006, 34, 757–764. [Google Scholar] [CrossRef]
- Boden, B.P.; Sheehan, F.T.; Torg, J.S.; Hewett, T.E. Noncontact anterior cruciate ligament injuries: Mechanisms and risk factors. J. Am. Acad. Orthop. Surg. 2010, 18, 520–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myer, G.D.; Ford, K.R.; Paterno, M.V.; Nick, T.G.; Hewett, T.E. The effects of generalized joint laxity on risk of anterior cruciate ligament injury in young female athletes. Am. J Sports Med. 2008, 36, 1073–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, L.C.; Denegar, C.R.; Buckley, W.E.; Hertel, J. Factors associated with anterior cruciate ligament injury: History in female athletes. J. Sports Med. Phys. Fitness 2007, 47, 446–454. [Google Scholar]
- Shultz, S.J.; Levine, B.J.; Nguyen, A.D.; Kim, H.; Montgomery, M.M.; Perrin, D.H. A comparison of cyclic variations in anterior knee laxity, genu recurvatum, and general joint laxity across the menstrual cycle. J. Orthop. Res. 2010, 28, 1411–1417. [Google Scholar] [CrossRef] [Green Version]
- Beynnon, B.D.; Bernstein, I.M.; Belisle, A.; Brattbakk, B.; Devanny, P.; Risinger, R.; Durant, D. The effect of estradiol and progesterone on knee and ankle joint laxity. Am. J. Sports Med. 2005, 33, 1298–1304. [Google Scholar] [CrossRef]
- Maruyama, S.; Yamazaki, T.; Sato, Y.; Suzuki, Y.; Shimizu, S.; Ikezu, M.; Kaneko, F.; Matsuzawa, K.; Hirabayashi, R.; Edama, M. Relationship between anterior knee laxity and general joint laxity during the menstrual cycle. Orthop. J. Sports Med. 2021, 9, 2325967121993045. [Google Scholar] [CrossRef]
- Paterno, M.V.; Rauh, M.J.; Schmitt, L.C.; Ford, K.R.; Hewett, T.E. Incidence of contralateral and ipsilateral anterior cruciate ligament (ACL) injury after primary ACL reconstruction and return to sport. Clin. J. Sport Med. 2012, 22, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Amiel, D.; Kleiner, J.B.; Roux, R.D.; Harwood, F.L.; Akeson, W.H. The phenomenon of “ligamentization”: Anterior cruciate ligament reconstruction with autogenous patellar tendon. J. Orthop. Res. 1986, 4, 162–172. [Google Scholar] [CrossRef] [PubMed]
- Hefti, F.; Müller, W.; Jakob, R.P.; Stäubli, H.U. Evaluation of knee ligament injuries with the IKDC form. Knee Surg. Sports Traumatol. Arthrosc. 1993, 1, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Magnussen, R.A.; Reinke, E.K.; Huston, L.J.; Briskin, I.; Cox, C.L.; Dunn, W.R.; Flanigan, D.C.; Jones, M.H.; Kaeding, C.C.; Matava, M.J.; et al. Neither residual anterior knee laxity up to 6 mm nor a pivot glide predict patient-reported outcome scores or subsequent knee surgery between 2 and 6 years after ACL reconstruction. Am. J. Sports Med. 2021, 49, 2631–2637. [Google Scholar] [CrossRef]
- Shultz, S.J.; Kirk, S.E.; Johnson, M.L.; Sander, T.C.; Perrin, D.H. Relationship between sex hormones and anterior knee laxity across the menstrual cycle. Med. Sci. Sports Exerc. 2004, 36, 1165–1174. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.H.; al-Shaikh, R.; Panossian, V.; Yang, R.S.; Nelson, S.D.; Soleiman, N.; Finerman, G.A.; Lane, J.M. Primary immunolocalization of estrogen and progesterone target cells in the human anterior cruciate ligament. J. Orthop. Res. 1996, 14, 526–533. [Google Scholar] [CrossRef]
- Fede, C.; Albertin, G.; Petrelli, L.; Sfriso, M.M.; Biz, C.; De Caro, R.; Stecco, C. Hormone receptor expression in human fascial tissue. Eur. J. Histochem. 2016, 60, 2710. [Google Scholar] [CrossRef] [Green Version]
- Wiik, A.; Ekman, M.; Morgan, G.; Johansson, O.; Jansson, E.; Esbjörnsson, M. Oestrogen receptor beta is present in both muscle fibres and endothelial cells within human skeletal muscle tissue. Histochem. Cell Biol. 2005, 124, 161–165. [Google Scholar] [CrossRef]
- Bridgeman, J.T.; Zhang, Y.; Donahue, H.; Wade, A.M.; Juliano, P.J. Estrogen receptor expression in posterior tibial tendon dysfunction: A pilot study. Foot Ankle Int. 2010, 31, 1081–1084. [Google Scholar] [CrossRef]
- Yu, W.D.; Liu, S.H.; Hatch, J.D.; Panossian, V.; Finerman, G.A. Effect of estrogen on cellular metabolism of the human anterior cruciate ligament. Clin. Orthop. Relat. Res. 1999, 366, 229–238. [Google Scholar] [CrossRef]
- Marturano, J.E.; Xylas, J.F.; Sridharan, G.V.; Georgakoudi, I.; Kuo, C.K. Lysyl oxidase-mediated collagen crosslinks may be assessed as markers of functional properties of tendon tissue formation. Acta Biomater. 2014, 10, 1370–1379. [Google Scholar] [CrossRef]
- Lee, C.A.; Lee-Barthel, A.; Marquino, L.; Sandoval, N.; Marcotte, G.R.; Baar, K. Estrogen inhibits lysyl oxidase and decreases mechanical function in engineered ligaments. J. Appl. Physiol. 2015, 118, 1250–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Knee Documentation Committee. International Knee Documentation Committee (IKDC) Subjective Knee Form. American Orthopaedic Society for Sports Medicine. 2000. Available online: https://www.sportsmed.org/uploads/main/files/general/IKDC/AOSSM-IKDC-Japanese.pdf (accessed on 16 November 2021).
- Tegner, Y.; Lysholm, J. Rating systems in the evaluation of knee ligament injuries. Clin. Orthop. Relat. Res. 1985, 198, 43–49. [Google Scholar] [CrossRef]
- Saliva Collection and Handling Advice 3rd Edition. 2015. Available online: https://fnkprddata.blob.core.windows.net/domestic/download/pdf/SAL_handbook3.pdf (accessed on 25 November 2022).
- Maruyama, S.; Sekine, C.; Shagawa, M.; Yokota, H.; Hirabayashi, R.; Togashi, R.; Yamada, Y.; Hamano, R.; Ito, A.; Sato, D.; et al. Menstrual cycle changes joint laxity in females-differences between eumenorrhea and oligomenorrhea. J. Clin. Med. 2022, 11, 3222. [Google Scholar] [CrossRef] [PubMed]
- Fröhlich-Zwahlen, A.K.; Casartelli, N.C.; Item-Glatthorn, J.F.; Maffiuletti, N.A. Validity of resting myotonometric assessment of lower extremity muscles in chronic stroke patients with limited hypertonia: A preliminary study. J. Electromyogr. Kinesiol. 2014, 24, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Myoton, A.S. MyotonPRO Digital Palpation Device User Manual. 2022. Available online: https://www.myoton.com/UserFiles/Updates/MyotonPRO_User_Manual.pdf (accessed on 1 November 2022).
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Kerby, D.S. The Simple Difference Formula: An Approach to Teaching Nonparametric Correlation. Compr. Psychol. 2014, 3, 11. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1998. [Google Scholar]
- Mayr, H.O.; Stoehr, A.; Herberger, K.T.; Haasters, F.; Bernstein, A.; Schmal, H.; Prall, W.C. Histomorphological alterations of human anterior cruciate ligament grafts during mid-term and long-term remodeling. Orthop. Surg. 2021, 13, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.Y.; Liu, X.; Smith, C.L.; Zhang, X.; Hsu, H.C.; Wang, D.Y.; Luo, Z.P. The combined regulation of estrogen and cyclic tension on fibroblast biosynthesis derived from anterior cruciate ligament. Matrix Biol. 2004, 23, 323–329. [Google Scholar] [CrossRef]
- Park, S.K.; Stefanyshyn, D.J.; Loitz-Ramage, B.; Hart, D.A.; Ronsky, J.L. Changing hormone levels during the menstrual cycle affect knee laxity and stiffness in healthy female subjects. Am. J. Sports Med. 2009, 37, 588–598. [Google Scholar] [CrossRef]
- Schmitz, R.J.; Shultz, S.J. Anterior knee stiffness changes in laxity “responders” versus “nonresponders” across the menstrual cycle. J. Athl. Train 2013, 48, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Sajovic, M.; Stropnik, D.; Skaza, K. Long-term comparison of semitendinosus and gracilis tendon versus patellar tendon autografts for anterior cruciate ligament reconstruction: A 17-year follow-up of a randomized controlled trial. Am. J. Sports Med. 2018, 46, 1800–1808. [Google Scholar] [CrossRef] [PubMed]
- Ramesh, R.; Von Arx, O.; Azzopardi, T.; Schranz, P.J. The risk of anterior cruciate ligament rupture with generalised joint laxity. J. Bone Joint Surg. Br. 2005, 87, 800–803. [Google Scholar] [CrossRef]
- Robertson, G.A.; Coleman, S.G.; Keating, J.F. Knee stiffness following anterior cruciate ligament reconstruction: The incidence and associated factors of knee stiffness following anterior cruciate ligament reconstruction. Knee 2009, 16, 245–247. [Google Scholar] [CrossRef]
- Sung, E.S.; Kim, J.H. The difference effect of estrogen on muscle tone of medial and lateral thigh muscle during ovulation. J. Exerc. Rehabil. 2018, 14, 419–423. [Google Scholar] [CrossRef] [PubMed]
- Khowailed, I.A.; Lee, Y.; Lee, H. Assessing the differences in muscle stiffness measured with shear wave elastography and myotonometer during the menstrual cycle in young women. Clin. Physiol. Funct. Imaging 2022, 42, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Puranda, J.L.; Silva, D.F.D.; Edwards, C.M.; Nagpal, T.S.; Souza, S.S.; Semeniuk, K.; Adamo, K.B. Association between reproductive health factors and musculoskeletal injuries in female Canadian Armed Forces members. J. Womens Health 2022, 0647. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Height (cm) | 160.4 ± 5.7 |
| Weight (kg) | 55.3 ± 5.0 |
| BMI | 21.5 ± 1.5 |
| Age (year) | 20.4 ± 1.5 |
| Age at injury (year) | 15.3 ± 1.76 |
| Time from injury to surgery (month) | 2.7 ± 1.5 |
| IKDC subjective evaluation score | 91.1 ± 7.0 |
| Tegner Activity Scale before surgery | 6.7 ± 0.9 |
| Tegner Activity Scale after surgery | 6.1 ± 1.1 |
| Early Follicular Phase | Ovulatory Phase | p | r | |
|---|---|---|---|---|
| E2 concentration (pg/mm) | 1.2 [0.9–1.6] | 1.5 [1.1–1.8] | 0.374 | 0.333 |
| AKL side-to-side difference (mm) | 3.3 [2.9–4.4] | 3.5 [1.0–4.0] | 0.051 | 0.733 |
| Reconstructed Side | Contralateral Side | |||||||
|---|---|---|---|---|---|---|---|---|
| Early Follicular | Ovulatory | p | r | Early Follicular | Ovulatory | p | r | |
| AKL (mm) | 9.4 [7.3–9.7] | 8.3 [5.9–9.3] | 0.044 * | 0.756 | 5.3 [4.7–6.9] | 4.8 [4.4–7.5] | 0.515 | 0.244 |
| GR (°) | 7.7 [5.6–9.1] | 7.5 [6.4–9.9] | 0.086 | 0.644 | 9.7 [7.1–12.0] | 10.2 [7.9–12.0] | 0.173 | 0.511 |
| ST stiffness (N/m) | 194.0 [173.5–226.8] | 196.7 [181.3–228.8] | 0.213 | 0.467 | 191.0 [169.0–238.1] | 199.7 [166.1–225.5] | 0.953 | 0.022 |
| BF stiffness (N/m) | 188.8 [178.3–222.6] | 203.7 [191.3–224.3] | 0.086 | 0.644 | 192.0 [186.4–229.5] | 210.5 [183.9–232.9] | 0.514 | 0.244 |
| Early Follicular Phase | Ovulatory Phase | |||||||
|---|---|---|---|---|---|---|---|---|
| Reconstructed | Contralateral | p | r | Reconstructed | Contralateral | p | r | |
| AKL (mm) | 9.4 [7.3–9.7] | 5.3 [4.7–6.9] | 0.008 * | 1.000 | 8.3 [5.9–9.3] | 4.8 [4.4–7.5] | 0.021 * | 0.867 |
| GR (°) | 7.7 [5.6–9.1] | 9.7 [7.1–12.0] | 0.021 * | 0.867 | 7.5 [6.4–9.9] | 10.2 [7.9–12.0] | 0.028 * | 0.822 |
| ST stiffness (N/m) | 194.0 [173.5–226.8] | 191.0 [169.0–238.1] | 0.514 | 0.244 | 196.7 [181.3–228.8] | 199.7 [166.1–225.5] | 0.594 | 0.200 |
| BF stiffness (N/m) | 188.8 [178.3–222.6] | 192.0 [186.4–229.5] | 0.341 | 0.356 | 203.7 [191.3–224.3] | 210.5 [183.9–232.9] | 0.594 | 0.200 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shagawa, M.; Maruyama, S.; Sekine, C.; Yokota, H.; Hirabayashi, R.; Togashi, R.; Yamada, Y.; Osanami, H.; Sato, D.; Edama, M. Knee Laxity in the Menstrual Cycle after Anterior Cruciate Ligament Reconstruction: A Case Series. Int. J. Environ. Res. Public Health 2023, 20, 2277. https://doi.org/10.3390/ijerph20032277
Shagawa M, Maruyama S, Sekine C, Yokota H, Hirabayashi R, Togashi R, Yamada Y, Osanami H, Sato D, Edama M. Knee Laxity in the Menstrual Cycle after Anterior Cruciate Ligament Reconstruction: A Case Series. International Journal of Environmental Research and Public Health. 2023; 20(3):2277. https://doi.org/10.3390/ijerph20032277
Chicago/Turabian StyleShagawa, Mayuu, Sae Maruyama, Chie Sekine, Hirotake Yokota, Ryo Hirabayashi, Ryoya Togashi, Yuki Yamada, Haruki Osanami, Daisuke Sato, and Mutsuaki Edama. 2023. "Knee Laxity in the Menstrual Cycle after Anterior Cruciate Ligament Reconstruction: A Case Series" International Journal of Environmental Research and Public Health 20, no. 3: 2277. https://doi.org/10.3390/ijerph20032277