
Determinants and Projections of Minimum Acceptable Diet among Children Aged 6–23 Months: A National and Subnational Inequality Assessment in Bangladesh
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Study Participants
2.3. Outcome Measures
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Prevalence of a MAD
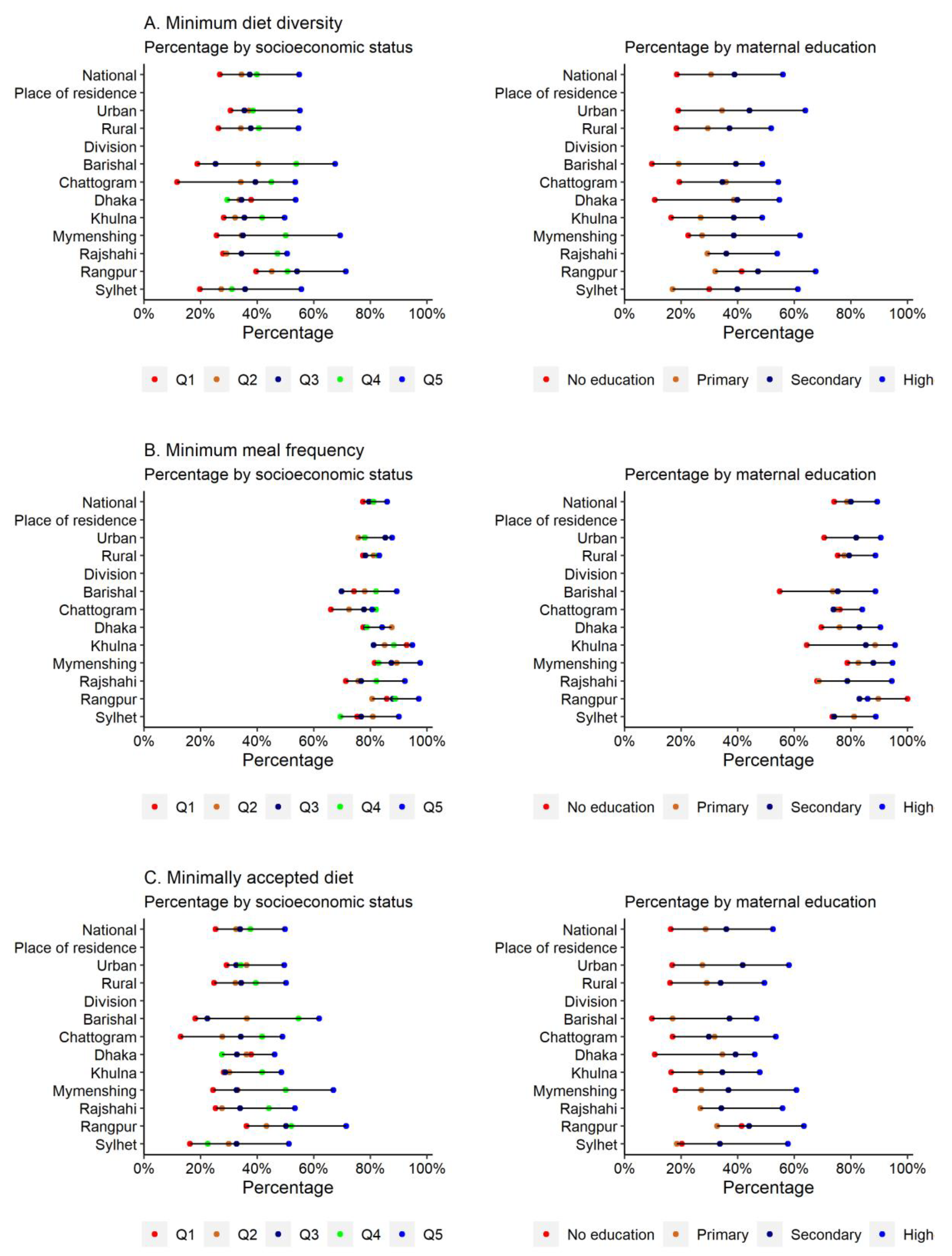
3.3. Absolute Inequality in the MAD
3.4. Relative Inequality in the MAD
3.5. Determinants of a MAD
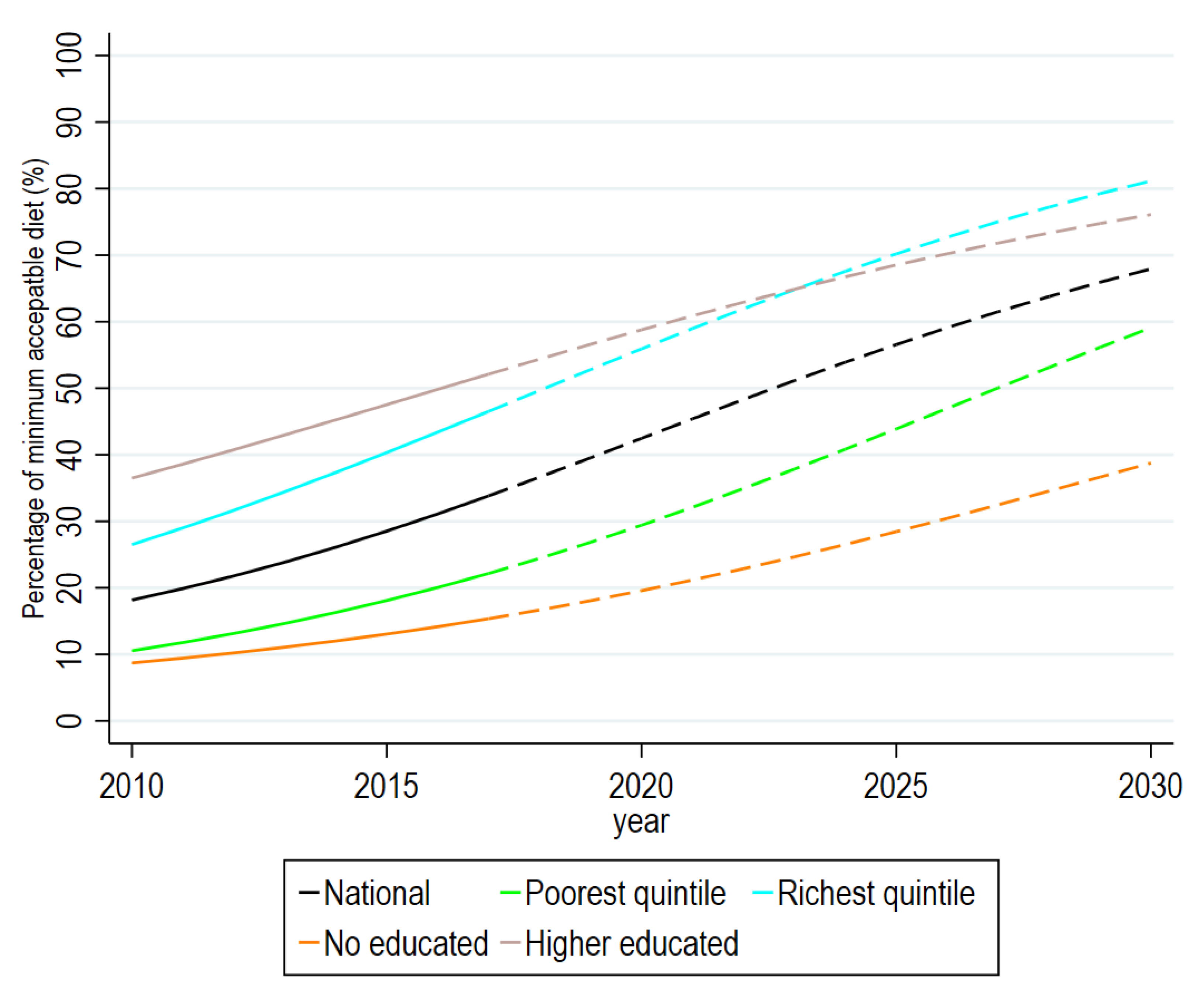
3.6. Trends and Future Directions of the MAD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Infant and Young Child Feeding: Model Chapter for Textbooks for Medical Students and Allied Health Professionals; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Grantham-McGregor, S.; Cheung, Y.B.; Cueto, S.; Glewwe, P.; Richter, L.; Strupp, B.; International Child Development Steering Group. Developmental potential in the first 5 years for children in developing countries. Lancet 2007, 369, 60–70. [Google Scholar] [PubMed] [Green Version]
- Masuke, R.; Msuya, S.E.; Mahande, J.M.; Diarz, E.J.; Stray-Pedersen, B.; Jahanpour, O.; Mgongo, M. Effect of inappropriate complementary feeding practices on the nutritional status of children aged 6–24 months in urban Moshi, Northern Tanzania: Cohort study. PLoS ONE 2021, 16, e0250562. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Children: Reducing Mortality: Fact Sheet; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Ogbo, F.A.; Nguyen, H.; Naz, S.; Agho, K.E.; Page, A. The association between infant and young child feeding practices and diarrhoea in Tanzanian children. Trop. Med. Health 2018, 46, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, G.; Steketee, R.W.; Black, R.E.; Bhutta, Z.A.; Morris, S.S. How many child deaths can we prevent this year? Lancet 2003, 362, 65–71. [Google Scholar] [CrossRef]
- United Nations Children’s Fund (UNICEF). World Health Organization, International Bank for Reconstruction and Development/The World Bank. In Levels and Trends in Child Malnutrition: Key Findings of the 2021 Edition of the Joint Child Malnutrition Estimates; United Nations Children’s Fund: New York, NY, USA, 2021. [Google Scholar]
- Dominguez, G.G.; Neves, P.A.R.; Barros, A.J.; Victora, C.G. Complementary feeding practices in 80 low-and middle-income countries: Prevalence and socioeconomic inequalities in dietary diversity, meal frequency and dietary adequacy. J. Nutr. 2021, 151, 1956–1964. [Google Scholar] [CrossRef]
- National Institute of Population Research and Training (NIPORT); ICF. Bangladesh Demographic and Health Survey 2017–2018; NIPORT: Dhaka, Bangladesh; ICF: Rockville, MD, USA, 2020. [Google Scholar]
- Al-Mamun, M.A.K.M.; Imam, A.; Zaman, S.S.; Khan, A.W.; Reza, M.M. Program Implementation Report 2017 of the 4th Health, Population and Nutrition Sector Program (4th HPNSP): January 2017–June 2022. Program Management & Monitoring Unit (PMMU), Planning Wing, the Ministry of Health and Family Welfare (MOHFW); Government of Bangladesh (GoB): Dhaka, Bangladesh, 2017. [Google Scholar]
- World Health Organization. Global Nutrition Monitoring Framework: Operational Guidance for Tracking Progress in Meeting Targets for 2025; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; United Nations Department of Economic and Social Affairs: New York, NY, USA, 2015. [Google Scholar]
- Sheikh, N.; Akram, R.; Ali, N.; Haque, S.R.; Tisha, S.; Mahumud, R.A.; Sarker, A.R.; Sultana, M. Infant and young child feeding practice, dietary diversity, associated predictors, and child health outcomes in Bangladesh. J. Child Health Care 2020, 24, 260–273. [Google Scholar] [CrossRef]
- Mistry, S.K.; Hossain, M.B.; Irfan, N.M.; Saha, M.; Saberin, S.; Shamim, A.A.; Arora, A. Trends in Complementary Feeding Indicators and Intake from Specific Food Groups among Children Aged 6–23 Months in Bangladesh. Int. J. Environ. Res. Public Health 2022, 19, 550. [Google Scholar] [CrossRef]
- Khanam, M.; Hasan, E. Inequalities in health care utilization for common illnesses among under five children in Bangladesh. BMC Pediatr. 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Raheem, E.; Khan, J.R.; Hossain, M.S. Regional disparities in maternal and child health indicators: Cluster analysis of districts in Bangladesh. PLoS ONE 2019, 14, e0210697. [Google Scholar] [CrossRef]
- Hasan, M.M.; Uddin, J.; Pulok, M.H.; Zaman, N.; Hajizadeh, M. Socioeconomic Inequalities in Child Malnutrition in Bangladesh: Do They Differ by Region? Int. J. Environ. Res. Public Health 2020, 17, 1079. [Google Scholar] [CrossRef]
- Das, S.; Baffour, B.; Richardson, A. Prevalence of child undernutrition measures and their spatio-demographic inequalities in Bangladesh: An application of multilevel Bayesian modelling. BMC Public Health 2022, 22, 1–21. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices: Definitions and Measurement Methods; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Ahmad, A.; Madanijah, S.; Dwiriani, C.M.; Kolopaking, R. Complementary feeding practices and nutritional status of children 6–23 months old: Formative study in Aceh, Indonesia. Nutr. Res. Pract. 2018, 12, 512. [Google Scholar] [CrossRef] [PubMed]
- Khan, J.R.; Awan, N.; Sheikh, M.T. A Multilevel and Spatial Analysis of the Infant and Young Child Feeding Practices and Associated Factors among the Under-2 Aged Children in Bangladesh. Child Care Pract. 2019, 28, 178–195. [Google Scholar] [CrossRef]
- Mya, K.S.; Kyaw, A.T.; Tun, T. Feeding practices and nutritional status of children age 6–23 months in Myanmar: A secondary analysis of the 2015-16 Demographic and Health Survey. PLoS ONE 2019, 14, e0209044. [Google Scholar] [CrossRef] [PubMed]
- Na, M.; Aguayo, V.M.; Arimond, M.; Mustaphi, P.; Stewart, C.P. Predictors of complementary feeding practices in Afghanistan: Analysis of the 2015 Demographic and Health Survey. Matern. Child Nutr. 2018, 14, e12696. [Google Scholar] [CrossRef] [PubMed]
- Rutstein, S.; Johnson, K. The DHS Wealth Index. DHS Comparative Reports No. 6; ORC Macro: Calverton, MD, USA, 2004. [Google Scholar]
- National Institute of Population Research and Training (NIPORT); Mitra and Associates; ICF International. Bangladesh Demographic and Health Survey 2011; NIPORT, Mitra and Associates: Dhaka, Bangladesh; ICF International: Calverton, MD, USA, 2013. [Google Scholar]
- Senarath, U.; Dibley, M.J. Complementary feeding practices in South Asia: Analyses of recent national survey data by the South Asia Infant Feeding Research Network. Matern. Child Nutr. 2012, 8, 5–10. [Google Scholar] [CrossRef]
- Prveen, S.S.S.; Khan, M.N.I.; Islam, S.N. Food security and food consumption pattern among poor people of Sylhet division. Int. J. Adv. Res. Biol. Sci. 2021, 8(4), 19–27. [Google Scholar]
- Nath, S.R.K.M.; Ahmed, K.S.; Roy, G.; Hossain, A.; Alam, S.M.N.; Chowdhury, F.K.; Mahbub, A. Education Watch 2009-10. Exploring low performance in education: The case of Sylhet Division; Campaign for Popular Education (CAMPE): Dhaka, Bangladesh, 2011. [Google Scholar]
- Sen, B.; Ahmed, M.; Yunus, M.; Ali, Z. Regional Inequality in Bangladesh in the 2000s: Re-Visiting the East-West Divide Debate; Bangladesh Institute of Development Studies: Dhaka, Bangladesh, 2014. [Google Scholar]
- Mia, M.N.; Rahman, M.S.; Roy, P.K. Sociodemographic and geographical inequalities in under-and overnutrition among children and mothers in Bangladesh: A spatial modelling approach to a nationally representative survey. Public Health Nutr. 2018, 21, 2471–2481. [Google Scholar] [CrossRef] [Green Version]
- Bhatta, S.D.; Rahman, T.; Rahman, M.; Sharma, U.; Adams, L. The Landscape of Early Childhood Education in Bangladesh; Report No: AUS0001357; World Bank: Washington, DC, 2020. [Google Scholar]
- Food Planning Monitoring Unit. Bangladesh National Food Policy Plan of Action (2008–2015); Ministry of Food and Disaster Management: Dhaka, Bangladesh, 2016. [Google Scholar]
- General Economics Division. National Strategy for Accelerated Poverty Reduction II; General Economics Division, Planning Commission, Government of the People’s Republic of Bangladesh: Dhaka, Bangladesh, 2009. [Google Scholar]
- International Monetary Fund. Bangladesh: Poverty Reduction Strategy Paper. IMF Staff Country Reports, 2013; International Monetary Fund, Asia Pacific. Dept.: Washington DC, USA, 2013. [Google Scholar]
- Jalal, C.S.; Frongillo, E.A. Effect of poverty reduction program on nutritional status of the extreme poor in Bangladesh. Food Nutr. Bull. 2013, 34, 402–411. [Google Scholar] [CrossRef] [Green Version]
- Pulok, M.H.; Uddin, J.; Enemark, U.; Hossin, M.Z. Socioeconomic inequality in maternal healthcare: An analysis of regional variation in Bangladesh. Health Place 2018, 52, 205–214. [Google Scholar] [CrossRef]
- Kazal, M.M.H.; Rahman, S.; Hossain, M.Z. Poverty Profiles and Coping Strategies of the Haor (Ox-bow Lake) Households in Bangladesh. J. Poverty Alleviation Int. Dev. 2017, 8, 167–191. [Google Scholar]
- Hossain, D.M. Socio-economic situation of the Indigenous people in the Chittagong Hill Tracts (CHT) of Bangladesh. Middle East J. Bus. 2013, 8, 22–30. [Google Scholar] [CrossRef]
- Kazal, M.M.H.; Villinueva, C.C.; Hossain, M.Z.; Das, T.K. Food Security Strategies of the People Living in Haor Areas: Status and Prospects; American International University: Dhaka, Bangladesh, 2010. [Google Scholar]
- Farzana, F.D.; Choudhury, N.; Haque, M.A.; Ali, M.; Raihan, M.J.; Ahmed, S.T.; Rahman, S.S.; Siddiqua, T.J.; Naz, F.; Faruque, A.S.G.; et al. Type of terrain and infant and young child feeding practices: Cross-sectional study findings on children below 2 years of age from northern Bangladesh. BMJ Open 2022, 12, e056593. [Google Scholar] [CrossRef] [PubMed]
- Senarath, U.; Agho, K.E.; Akram, D.E.S.; Godakandage, S.S.; Hazir, T.; Jayawickrama, H.; Joshi, N.; Kabir, I.; Khanam, M.; Patel, A.; et al. Comparisons of complementary feeding indicators and associated factors in children aged 6–23 months across five South Asian countries. Matern. Child Nutr. 2012, 8, 89–106. [Google Scholar] [CrossRef] [PubMed]
- Zia-Us-Sabur, A.; Ahmed, M. Multiple providers and access to primary education: The case of Bangladesh. Prospects 2010, 40, 393–415. [Google Scholar] [CrossRef]
- Oxfam, G.B. 9.Girls’ Education in South Asia, Education and Gender Equality Series, Programme Insights; Education and Gender Equality Series; Oxford Committee for Famine Relief (Oxfam): Oxford, UK, 2006. [Google Scholar]
- Ogbo, F.A.; Agho, K.; Ogeleka, P.; Woolfenden, S.; Page, A.; Eastwood, J.; Global Child Health Research Interest Group. Infant feeding practices and diarrhoea in sub-Saharan African countries with high diarrhoea mortality. PLoS ONE 2017, 12, e0171792. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, K.; Page, A.; Arora, A.; Ogbo, F.; Global Maternal and Child Health Research collaboration (GloMACH). Associations between infant and young child feeding practices and acute respiratory infection and diarrhoea in Ethiopia: A propensity score matching approach. PLoS ONE 2020, 15, e0230978. [Google Scholar] [CrossRef] [Green Version]
- Gelli, A.; Margolies, A.; Santacroce, M.; Roschnik, N.; Twalibu, A.; Katundu, M.; Moestue, H.; Alderman, H.; Ruel, M. Using a Community-Based Early Childhood Development Center as a Platform to Promote Production and Consumption Diversity Increases Children’s Dietary Intake and Reduces Stunting in Malawi: A Cluster-Randomized Trial. J. Nutr. 2018, 148, 1587–1597. [Google Scholar] [CrossRef] [Green Version]
- Sanghvi, T.; Martin, L.; Hajeebhoy, N.; Abrha, T.H.; Abebe, Y.; Haque, R.; Tran, H.T.T.; Roy, S. Strengthening systems to support mothers in infant and young child feeding at scale. Food Nutr. Bull. 2013, 34, S156–S168. [Google Scholar] [CrossRef]
- Keats, E.C.; Das, J.K.; Salam, R.A.; Lassi, Z.S.; Imdad, A.; Black, R.E.; Bhutta, Z.A. Effective interventions to address maternal and child malnutrition: An update of the evidence. Lancet Child Adolesc Health 2021, 5, 367–384. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | N (%) | Percentage (95% Confidence Intervals) | ||
|---|---|---|---|---|
| Minimum Diet Diversity | Minimum Meal Frequency | Minimally Accepted Diet | ||
| Child characteristics | ||||
| Age group (months) | ||||
| 6–11 | 800 (33.0) | 22.7 (20.0–25.7) | 73.0 (69.8–75.9) | 21.7 (19.0–24.7) |
| 12–17 | 847 (34.9) | 45.2 (41.9–48.6) | 84.0 (81.4–86.3) | 42.7 (39.4–46.1) |
| 18–23 | 780 (32.1) | 47.0 (43.6–50.5) | 85.8 (83.1–88.0) | 42.4 (39.0–45.9) |
| Sex | ||||
| Boys | 1254 (51.7) | 38.2 (35.6–40.9) | 81.0 (78.7–83.1) | 35.3 (32.7–38.0) |
| Girls | 1173 (48.3) | 38.6 (35.8–41.4) | 80.9 (78.5–83.0) | 36.1 (33.4–38.9) |
| Order of birth | ||||
| First | 907 (37.4) | 43.0 (39.9–46.3) | 83.3 (80.7–85.6) | 39.8 (36.6–43.0) |
| Second | 817 (33.7) | 37.2 (33.9–40.5) | 79.4 (76.6–82.1) | 34.7 (31.5–38.0) |
| Third or higher | 703 (29.0) | 33.8 (30.4–37.4) | 79.6 (76.5–82.4) | 31.6 (28.3–35.1) |
| Underweight | ||||
| No | 1957 (82.1) | 38.7 (36.6–40.8) | 80.5 (78.8–82.2) | 35.7 (33.7–37.9) |
| Yes | 428 (18.0) | 35.2 (30.7–40.0) | 82.4 (78.3–85.8) | 34.2 (29.8–39.0) |
| Stunting | ||||
| No | 1626 (69.5) | 38.0 (35.7–40.4) | 80.6 (78.7–82.5) | 35.3 (33.1–37.6) |
| Yes | 715 (30.5) | 38.4 (34.9–42.1) | 81.0 (77.9–83.8) | 35.9 (32.4–39.6) |
| Wasting | ||||
| No | 2167 (92.2) | 38.2 (36.2–40.3) | 80.7 (79.0–82.3) | 35.5 (33.5–37.5) |
| Yes | 183 (7.8) | 37.0 (30.3–44.1) | 80.1 (73.7–85.3) | 35.6 (29.0–42.7) |
| Mothers’ characteristics | ||||
| Mother’s age (years) | ||||
| 15–20 | 449 (18.5) | 36.2 (32.0–40.7) | 79.4 (75.6–82.9) | 33.5 (29.4–37.9) |
| 20–35 | 1824 (75.2) | 38.9 (36.7–41.1) | 80.9 (79.1–82.7) | 36.0 (33.9–38.3) |
| 35–49 | 154 (6.4) | 38.8 (31.4–46.8) | 85.5 (79.0–90.2) | 38.0 (30.7–46.0) |
| Mother’s educational status | ||||
| Not educated | 144 (5.9) | 18.5 (13.1–25.4) | 74.1 (66.6–80.4) | 16.3 (11.2–23.0) |
| Primary educated | 664 (27.4) | 30.6 (27.2–34.2) | 78.6 (75.3–81.5) | 28.7 (25.4–32.3) |
| Secondary educated | 1168 (48.1) | 38.8 (36.1–41.6) | 80.0 (77.7–82.2) | 36.0 (33.3–38.7) |
| Higher educated | 451 (18.6) | 56.0 (51.3–60.6) | 89.4 (86.1–91.9) | 52.4 (47.7–57.1) |
| Mother’s working status | ||||
| Not working | 1529 (63.0) | 37.7 (35.3–40.2) | 78.8 (76.6–80.7) | 34.4 (32.0–36.8) |
| Currently working | 898 (37.0) | 39.5 (36.4–42.7) | 84.6 (82.1–86.8) | 37.9 (34.8–41.1) |
| Access to mass media | ||||
| Not at all | 893 (36.8) | 30.5 (27.5–33.6) | 77.3 (74.3–80.0) | 27.7 (24.8–30.8) |
| Yes (at least to some extent) | 1534 (63.2) | 42.6 (40.2–45.1) | 82.9 (81.0–84.7) | 40.0 (37.6–42.5) |
| Number of ANC visits | ||||
| No ANC visits | 192 (7.9) | 24.1 (18.6–30.7) | 68.0 (61.0–74.2) | 20.7 (15.6–27.1) |
| 1–3 visits | 1081 (44.5) | 30.6 (27.9–33.3) | 78.7 (76.2–81.0) | 28.6 (26.1–31.4) |
| 4+ visits | 1154 (47.6) | 48.5 (45.6–51.4) | 85.3 (83.2–87.3) | 45.1 (42.3–48.1) |
| Household level | ||||
| Wealth quintile | ||||
| Q1 (poorest) | 517 (21.3) | 26.7 (23.0–30.7) | 77.4 (73.6–80.9) | 25.3 (21.7–29.3) |
| Q2 | 513 (21.1) | 34.4 (30.5–38.6) | 80.8 (77.2–84.0) | 32.6 (28.8–36.8) |
| Q3 | 424 (17.5) | 37.3 (32.9–41.9) | 79.5 (75.5–83.0) | 34.0 (29.8–38.5) |
| Q4 | 498 (20.5) | 39.8 (35.6–44.2) | 81.1 (77.4–84.3) | 37.6 (33.5–42.0) |
| Q5 (richest) | 475 (19.6) | 54.9 (50.4–59.3) | 86.0 (82.5–88.8) | 49.9 (45.3–54.4) |
| Contextual factors | ||||
| Place of residence | ||||
| Urban | 808 (33.3) | 45.0 (41.2–48.9) | 83.2 (80.1–85.9) | 40.8 (37.0–44.6) |
| Rural | 1619 (66.7) | 36.0 (33.9–38.3) | 80.1 (78.2–81.9) | 33.9 (31.8–36.1) |
| Regions | ||||
| Barishal | 262 (10.8) | 34.1 (26.8–42.3) | 76.5 (68.8–82.8) | 32.0 (24.9–40.2) |
| Chattogram | 394 (16.2) | 37.9 (33.8–42.2) | 76.3 (72.4–79.8) | 34.2 (30.2–38.4) |
| Dhaka | 355 (14.6) | 40.3 (36.5–44.2) | 81.6 (78.4–84.5) | 37.2 (33.5–41.0) |
| Khulna | 240 (9.9) | 36.8 (30.7–43.4) | 87.3 (82.1–91.1) | 34.5 (28.5–41.0) |
| Mymensingh | 294 (12.1) | 36.7 (30.4–43.4) | 86.3 (81.0–90.3) | 35.3 (29.1–42.0) |
| Rajshahi | 255 (10.5) | 35.5 (30.1–41.2) | 77.9 (72.7–82.4) | 34.1 (28.8–39.8) |
| Rangpur | 285 (11.7) | 47.2 (41.4–53.1) | 86.0 (81.4–89.6) | 44.9 (39.2–50.8) |
| Sylhet | 342 (14.1) | 31.6 (25.4–38.5) | 78.1 (71.7–83.4) | 28.4 (22.5–35.1) |
| Overall | 2427 (100.0) | 38.4 (36.5–40.3) | 80.9 (79.3–82.4) | 35.7 (33.8–37.6) |
| Slope Index of Inequality | Socioeconomic Inequality | Education-Based Inequality | ||||
|---|---|---|---|---|---|---|
| Minimum Diet Diversity | Minimum Meal Frequency | Minimally Accepted Diet | Minimum Diet Diversity | Minimum Meal Frequency | Minimally Accepted Diet | |
| National | 29.8 (22.3–37.3) *** | 8.4 (2.3–14.5) ** | 26.0 (18.7–33.3) *** | 34.3 (26.4–42.1) *** | 13.3 (6.6–20.0) *** | 32.1 (24.4–39.9) *** |
| Place of residence | ||||||
| Urban | 37.5 (23.5–51.5) *** | 17.4 (6.7–28.1) ** | 32.1 (18.6–45.6) *** | 42.3 (29.4–55.2) *** | 15.2 (2.7–27.7) * | 42.9 (30.2–55.5) *** |
| Rural | 25.6 (16.9–34.4) *** | 5.7 (−2.1–13.5) | 23.8 (14.9–32.7) *** | 29.5 (20.1–39.0) *** | 12.3 (4.2–20.4) ** | 27.1 (17.6–36.6) *** |
| Regions | ||||||
| Barishal | 37.7 (15.8–59.7) ** | 8.2 (−11.0–27.4) | 35.7 (14.1–57.4) ** | 40.3 (22.3–58.3) *** | 17.3 (−2.4–37.1) | 40.7 (22.5–59.0) *** |
| Chattogram | 47.1 (31.9–62.2) *** | 18.9 (5.6–32.1) ** | 43.9 (28.0–59.8) *** | 24.7 (4.9–44.5) * | 6.7 (−7.7–21.2) | 28.4 (10.1–46.7) ** |
| Dhaka | 25.1 (6.7–43.5) ** | 5.1 (−7.5–17.7) | 14.1 (−3.2–31.5) | 33.5 (15.1–51.9) *** | 21.3 (5.3–37.2) ** | 27.6 (9.0–46.1) ** |
| Khulna | 29.5 (10.6–48.5) ** | 4.0 (−9.4–17.4) | 29.4 (10.5–48.2) ** | 38.0 (16.9–59.0) *** | 11.4 (−2.7–25.6) | 35.1 (13.6–56.7) ** |
| Mymensingh | 33.0 (12.2–53.8) ** | 12.5 (0.9–24.0) * | 32.2 (12.2–52.2)** | 37.8 (18.9–56.8) *** | 15.0 (2.8–27.2) ** | 36.8 (17.8–55.8) *** |
| Rajshahi | 31.1 (11.2–51.1) ** | 23.2 (7.0–39.4) ** | 35.2 (16.7–53.7) *** | 32.2 (11.8–52.6) ** | 27.9 (9.2–46.6) | 39.2 (21.1–57.4) *** |
| Rangpur | 24.3 (4.0–44.6) * | 10.4 (−2.9–23.7) | 28.8 (9.2–48.4) ** | 41.2 (21.8–60.6) *** | −5.3 (−18.1–7.5) | 35.6 (16.3–54.9) *** |
| Sylhet | 44.4 (28.1–60.8) *** | 14.4 (−1.1–30.0) | 39.9 (23.1–56.7) *** | 51.5 (37.0–66.0) *** | 6.6 (−7.5–20.8) | 47.7 (31.9–63.5) *** |
| Characteristics | Odds Ratio (95% Confidence Intervals) | |||
|---|---|---|---|---|
| Model 1 a | Model 2 b | Model 3 c | Model 4 d | |
| Child characteristics | ||||
| Age group (months) | ||||
| 6–11 (ref.) | 1.00 | 1.00 | 1.00 | 1.00 |
| 12–17 | 2.42 (1.96–3.00) | 2.52 (2.01–3.15) | 2.52 (2.01–3.15) | 2.53 (2.02–3.17) |
| 18–23 | 2.56 (2.06–3.17) | 2.68 (2.13–3.36) | 2.70 (2.15–3.39) | 2.70 (2.14–3.39) |
| Sex | ||||
| Boys (ref.) | 1.00 | 1.00 | 1.00 | 1.00 |
| Girls | 1.08 (0.91–1.27) | 1.07 (0.90–1.28) | 1.08 (0.90–1.28) | 1.08 (0.90–1.29) |
| Order of birth | ||||
| First | 1.28 (1.06–1.56) | 1.11 (0.88–1.41) | 1.13 (0.89–1.43) | 1.14 (0.90–1.44) |
| Second (ref.) | 1.00 | 1.00 | 1.00 | 1.00 |
| Third or higher | 0.85 (0.69–1.06) | 1.05 (0.82–1.34) | 1.06 (0.83–1.35) | 1.06 (0.83–1.35) |
| Underweight | ||||
| No (ref.) | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 0.84 (0.67–1.04) | 1.07 (0.84–1.35) | 1.09 (0.86–1.39) | 1.09 (0.85–1.39) |
| Mothers’ characteristics | ||||
| Mother’s age (years) | ||||
| 15–20 (<20) (ref.) | 1.00 | 1.00 | 1.00 | 1.00 |
| 20–35 | 1.07 (0.86–1.33) | 1.01 (0.77–1.32) | 0.97 (0.74–1.27) | 0.98 (0.75–1.29) |
| 35–49 (≥35) | 1.12 (0.77–1.64) | 1.24 (0.77–2.01) | 1.18 (0.73–1.91) | 1.18 (0.73–1.92) |
| Mother’s educational status | ||||
| Not educated (ref.) | 1.00 | 1.00 | 1.00 | 1.00 |
| Primary educated | 1.68 (1.06–2.65) | 1.56 (0.97–2.51) | 1.55 (0.97–2.50) | 1.55 (0.96–2.50) |
| Secondary educated | 2.60 (1.67–4.04) | 2.25 (1.41–3.60) | 2.15 (1.34–3.44) | 2.10 (1.30–3.38) |
| Higher educated | 5.70 (3.58–9.05) | 4.24 (2.55–7.03) | 3.66 (2.19–6.12) | 3.47 (2.06–5.85) |
| Mother’s working status | ||||
| Not working (ref.) | 1.00 | 1.00 | 1.00 | 1.00 |
| Currently working | 1.10 (0.92–1.3) | 1.28 (1.06–1.54) | 1.36 (1.13–1.65) | 1.31 (1.08–1.59) |
| Access to mass media | ||||
| Not at all (ref.) | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes (at least to some extent) | 1.86 (1.55–2.22) | 1.33 (1.09–1.62) | 1.22 (0.98–1.51) | 1.20 (0.96–1.49) |
| Number of ANC visits | ||||
| No ANC visits (ref.) | 1.00 | 1.00 | 1.00 | 1.00 |
| 1–3 visits | 1.88 (1.27–2.78) | 1.53 (1.02–2.30) | 1.49 (0.99–2.24) | 1.44 (0.95–2.17) |
| 4+ visits | 4.03 (2.73–5.94) | 2.66 (1.76–4.03) | 2.46 (1.62–3.75) | 2.30 (1.51–3.51) |
| Household level | ||||
| Wealth quintile | ||||
| Q1 (poorest) (ref.) | 1.00 | 1.00 | 1.00 | |
| Q2 | 1.51 (1.15–1.98) | 1.28 (0.96–1.71) | 1.34 (1.00–1.80) | |
| Q3 | 1.50 (1.13–1.99) | 1.05 (0.77–1.45) | 1.12 (0.81–1.55) | |
| Q4 | 1.89 (1.44–2.48) | 1.21 (0.88–1.66) | 1.32 (0.95–1.84) | |
| Q5 (richest) | 3.43 (2.62–4.49) | 1.76 (1.25–2.48) | 1.95 (1.34–2.84) | |
| Contextual factors | ||||
| Place of residence | ||||
| Rural (ref.) | 1.00 | 1.00 | ||
| Urban | 1.48 (1.25–1.76) | 1.07 (0.87–1.33) | ||
| Regions | ||||
| Barishal | 0.83 (0.57–1.20) | 1.11 (0.74–1.65) | ||
| Chattogram | 0.94 (0.67–1.32) | 1.10 (0.76–1.58) | ||
| Dhaka | 1.03 (0.74–1.45) | 1.02 (0.71–1.48) | ||
| Khulna (ref.) | 1.00 | 1.00 | ||
| Mymensingh | 0.93 (0.65–1.33) | 1.25 (0.85–1.83) | ||
| Rajshahi | 0.99 (0.69–1.43) | 1.11 (0.75–1.63) | ||
| Rangpur | 1.51 (1.06–2.15) | 1.68 (1.15–2.46) | ||
| Sylhet | 0.79 (0.56–1.11) | 1.04 (0.71–1.53) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahman, M.S.; Chowdhury, M.R.K.; Islam, M.R.; Krull Abe, S.; Hossain, K.; Iwabuchi, T.; Tsuchiya, K.J.; Gilmour, S. Determinants and Projections of Minimum Acceptable Diet among Children Aged 6–23 Months: A National and Subnational Inequality Assessment in Bangladesh. Int. J. Environ. Res. Public Health 2023, 20, 2010. https://doi.org/10.3390/ijerph20032010
Rahman MS, Chowdhury MRK, Islam MR, Krull Abe S, Hossain K, Iwabuchi T, Tsuchiya KJ, Gilmour S. Determinants and Projections of Minimum Acceptable Diet among Children Aged 6–23 Months: A National and Subnational Inequality Assessment in Bangladesh. International Journal of Environmental Research and Public Health. 2023; 20(3):2010. https://doi.org/10.3390/ijerph20032010
Chicago/Turabian StyleRahman, Md. Shafiur, Md. Rocky Khan Chowdhury, Md. Rashedul Islam, Sarah Krull Abe, Kamal Hossain, Toshiki Iwabuchi, Kenji J. Tsuchiya, and Stuart Gilmour. 2023. "Determinants and Projections of Minimum Acceptable Diet among Children Aged 6–23 Months: A National and Subnational Inequality Assessment in Bangladesh" International Journal of Environmental Research and Public Health 20, no. 3: 2010. https://doi.org/10.3390/ijerph20032010