
Cost Consequence Analysis of Belimumab versus Standard of Care for the Management of Systemic Lupus Erythematosus in Saudi Arabia: A Retrospective Cohort Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Statistical Analysis
2.3. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Borchers, A.T.; Naguwa, S.M.; Shoenfeld, Y.; Gershwin, M.E. The geoepidemiology of systemic lupus erythematosus. Autoimmun. Rev. 2010, 9, A277–A287. [Google Scholar] [CrossRef] [PubMed]
- Cojocaru, M.; Cojocaru, I.M.; Silosi, I.; Vrabie, C.D. Manifestations of systemic lupus erythematosus. Maedica 2011, 6, 330–336. [Google Scholar]
- Muscal, E.; Brey, R.L. Neurologic manifestations of systemic lupus erythematosus in children and adults. Neurol. Clin. 2010, 28, 61–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barr, S.G.; Zonana-Nacach, A.; Magder, L.S.; Petri, M. Patterns of disease activity in systemic lupus erythematosus. Arthritis Rheum. 1999, 42, 2682–2688. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.R.; Yen, E.Y. SLE mortality remains disproportionately high, despite improvements over the last decade. Lupus 2018, 27, 1577–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gergianaki, I.; Bortoluzzi, A.; Bertsias, G. Update on the epidemiology, risk factors, and disease outcomes of systemic lupus erythematosus. Best Pract. Res. Clin. Rheumatol. 2018, 32, 188–205. [Google Scholar] [CrossRef] [PubMed]
- Kulczycka, L.; Sysa-Jedrzejowska, A.; Robak, E. Quality of life and satisfaction with life in SLE patients-the importance of clinical manifestations. Clin. Rheumatol. 2010, 29, 991–997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakshi, J.; Segura, B.T.; Wincup, C.; Rahman, A. Unmet Needs in the Pathogenesis and Treatment of Systemic Lupus Erythematosus. Clin. Rev. Allergy Immunol. 2018, 55, 352–367. [Google Scholar] [CrossRef] [Green Version]
- Wallace, D.J. Progress toward Better Treatment of Lupus. N. Engl. J. Med. 2022, 387, 939–940. [Google Scholar] [CrossRef]
- Basta, F.; Fasola, F.; Triantafyllias, K.; Schwarting, A. Systemic Lupus Erythematosus (SLE) Therapy: The Old and the New. Rheumatol. Ther. 2020, 7, 433–446. [Google Scholar] [CrossRef]
- Navarra, S.V.; Guzmán, R.M.; Gallacher, A.E.; Hall, S.; Levy, R.A.; Jimenez, R.E.; Li, E.K.M.; Thomas, M.; Kim, H.-Y.; León, M.G.; et al. Efficacy and safety of belimumab in patients with active systemic lupus erythematosus: A randomised, placebo-controlled, phase 3 trial. Lancet 2011, 377, 721–731. [Google Scholar] [CrossRef] [PubMed]
- Furie, R.; Petri, M.; Zamani, O.; Cervera, R.; Wallace, D.J.; Tegzová, D.; Sanchez-Guerrero, J.; Schwarting, A.; Merrill, J.T.; Chatham, W.W.; et al. A phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus. Arthritis Rheum. 2011, 63, 3918–3930. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Neuner, R.; Thompson, A.; Pottackal, G.; Petullo, D.; Liu, J.; Nikolov, N.; Sahajwalla, C.; Doddapaneni, S.; Chen, J. Clinical pharmacology considerations for the approval of belimumab for the treatment of adult patients with active lupus nephritis: A regulatory perspective. Lupus 2022, 31, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Furie, R.; Rovin, B.H.; Houssiau, F.; Malvar, A.; Teng, Y.K.O.; Contreras, G.; Amoura, Z.; Yu, X.; Mok, C.-C.; Santiago, M.B.; et al. Two-Year, Randomized, Controlled Trial of Belimumab in Lupus Nephritis. N. Engl. J. Med. 2020, 383, 1117–1128. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Azmi, S.; Wu, D.; Goh, A. Estimating the cost-effectiveness of belimumab versus standard care for sle patients in Hong Kong. Value Health 2013, 16, A117–A118. [Google Scholar] [CrossRef] [Green Version]
- Díaz-Cerezo, S.; García-Aparicio, Á.M.; Parrondo, J.; Vallejo-Aparicio, L.A. Cost-effectiveness analysis of Belimumab in patients with systemic lupus erythematosus in Spain. Farm. Hosp. 2015, 39, 161–170. [Google Scholar] [CrossRef]
- Mandrik, O.; Fotheringham, J.; Ren, S.; Tice, J.A.; Chapman, R.H.; Stevenson, M.D.; Pearson, S.D.; Herron-Smith, S.; Agboola, F.; Thokala, P. The Cost-Effectiveness of Belimumab and Voclosporin for Patients with Lupus Nephritis in the United States. Clin. J. Am. Soc. Nephrol. 2022, 17, 385–394. [Google Scholar] [CrossRef] [PubMed]
- Almaghlouth, I.A.; Hassen, L.M.; Alahmari, H.S.; Bedaiwi, A.; Albarrak, R.; Daghestani, M.; Alqurtas, E.; Alkhalaf, A.; Bedaiwi, M.; Omair, M.; et al. National systemic lupus erythematosus prospective cohort in Saudi Arabia: A study protocol. Medicine 2021, 100, e26704. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Isenberg, D.A.; Castrejon, I. Measures of Adult Systemic Lupus Erythematosus: Disease Activity and Damage. Arthritis Care Res. 2020, 72, 27–46. [Google Scholar] [CrossRef]
- Gladman, D.D.; Ibañez, D.; Urowitz, M.B. Systemic lupus erythematosus disease activity index 2000. J. Rheumatol. 2002, 29, 288–291. [Google Scholar]
- Mosca, M.; Bombardieri, S. Assessing remission in systemic lupus erythematosus. Clin. Exp. Rheumatol. 2006, 24, S99–S104. [Google Scholar] [PubMed]
- Haukoos, J.S.; Lewis, R.J. Advanced statistics: Bootstrapping confidence intervals for statistics with “difficult” distributions. Acad. Emerg. Med. 2005, 12, 360–365. [Google Scholar] [CrossRef] [PubMed]
- General Assembly of the World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 2014, 81, 14–18. [Google Scholar]
- Schwarting, A.; Schroeder, J.O.; Alexander, T.; Schmalzing, M.; Fiehn, C.; Specker, C.; Perna, A.; Cholmakow-Bodechtel, C.; Koscielny, V.B.; Carnarius, H. First Real-World Insights into Belimumab Use and Outcomes in Routine Clinical Care of Systemic Lupus Erythematosus in Germany: Results from the OBSErve Germany Study. Rheumatol. Ther. 2016, 3, 271–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wise, L.M.; Stohl, W. Belimumab and Rituximab in Systemic Lupus Erythematosus: A Tale of Two B Cell-Targeting Agents. Front. Med. 2020, 7, 303. [Google Scholar] [CrossRef]
- Singh, J.A.; Shah, N.P.; Mudano, A.S. Belimumab for systemic lupus erythematosus. Cochrane Database Syst. Rev. 2021. [Google Scholar] [CrossRef]
- Bruce, I.N.; O’Keeffe, A.G.; Farewell, V.; Hanly, J.G.; Manzi, S.; Su, L.; Gladman, D.D.; Bae, S.C.; Sanchez-Guerrero, J.; Romero-Diaz, J.; et al. Factors associated with damage accrual in patients with systemic lupus erythematosus: Results from the Systemic Lupus International Collaborating Clinics (SLICC) Inception Cohort. Ann. Rheum. Dis. 2015, 74, 1706–1713. [Google Scholar] [CrossRef]
- Urowitz, M.B.; Ohsfeldt, R.L.; Wielage, R.C.; Kelton, K.A.; Asukai, Y.; Ramachandran, S. Organ damage in patients treated with belimumab versus standard of care: A propensity score-matched comparative analysis. Ann. Rheum. Dis. 2019, 78, 372–379. [Google Scholar] [CrossRef] [Green Version]
- Samnaliev, M.; Barut, V.; Weir, S.; Langham, J.; Langham, S.; Wang, X.; Desta, B.; Hammond, E. Health-care utilization and costs in adults with systemic lupus erythematosus in the United Kingdom: A real-world observational retrospective cohort analysis. Rheumatol. Adv. Pract. 2021, 5, rkab071. [Google Scholar] [CrossRef]
- Libert, C.; Dejager, L.; Pinheiro, I. The X chromosome in immune functions: When a chromosome makes the difference. Nat. Rev. Immunol. 2010, 10, 594–604. [Google Scholar] [CrossRef]
- López, P.; Mozo, L.; Gutiérrez, C.; Suárez, A. Epidemiology of systemic lupus erythematosus in a northern Spanish population: Gender and age influence on immunological features. Lupus 2003, 12, 860–865. [Google Scholar] [CrossRef] [PubMed]
- Kariburyo, F.; Xie, L.; Sah, J.; Li, N.; Lofland, J.H. Real-world medication use and economic outcomes in incident systemic lupus erythematosus patients in the United States. J. Med. Econ. 2020, 23, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lokhandwala, T.; Coutinho, A.D.; Bell, C.F. Retrospective Analysis of Disease Severity, Health Care Resource Utilization, and Costs Among Patients Initiating Belimumab for the Treatment of Systemic Lupus Erythematosus. Clin. Ther. 2021, 43, 1320–1335. [Google Scholar] [CrossRef]
- AlRuthia, Y.; Alrashed, S.A.; Balkhi, B.; Aljamal, M.S.; Alsifri, S.; Alrumaih, A.M.; Alsabaan, F.; Alsaqa’aby, M.; Al-Abdulkarim, H.A.; Altowaijri, A.I. COVID-19 and Saudi Arabia public financing of prescription drugs: An opportunity for reform. Health Policy Technol. 2020. [Google Scholar] [CrossRef]
- Klein, R.; Moghadam-Kia, S.; LoMonico, J.; Okawa, J.; Coley, C.; Taylor, L.; Troxel, A.B.; Werth, V.P. Development of the CLASI as a tool to measure disease severity and responsiveness to therapy in cutaneous lupus erythematosus. Arch. Dermatol. 2011, 147, 203–208. [Google Scholar] [CrossRef]
- Aberle, T.; Bourn, R.L.; Chen, H.; Roberts, V.C.; Guthridge, J.M.; Bean, K.; Robertson, J.M.; Sivils, K.L.; Rasmussen, A.; Liles, M.; et al. Use of SLICC criteria in a large, diverse lupus registry enables SLE classification of a subset of ACR-designated subjects with incomplete lupus. Lupus Sci. Med. 2017, 4, e000176. [Google Scholar] [CrossRef] [Green Version]
- Niewold, T.B. Advances in lupus genetics. Curr. Opin. Rheumatol. 2015, 27, 440–447. [Google Scholar] [CrossRef] [Green Version]
- Barliana, M.I.; Afifah, N.N.; Amalia, R.; Hamijoyo, L.; Abdulah, R. Genetic Polymorphisms and the Clinical Response to Systemic Lupus Erythematosus Treatment Towards Personalized Medicine. Front. Pharmacol. 2022, 13, 820927. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Belimumab (n = 15) | Standard of Care (SoC) (n = 41) | p-Value | Total (n = 56) |
|---|---|---|---|---|
| Age in yrs., (mean ± SD) | 34.54 ± 7.70 | 39.93 ± 10.95 | 0.0861 | 38.48 ± 10.40 |
| Gender, (n, %) | ||||
| Male | 1 (6.67) | 4 (9.76) | 0.7196 | 5 (8.93) |
| Female | 14 (93.33) | 37 (90.24) | 51 (91.07) | |
| Disease duration in years, (mean ± SD) | 12.40 ± 7.05 | 13.37 ± 6.02 | 0.6118 | 13.11 ± 6.26 |
| Duration of therapy in months, (mean ± SD) | 10.00 ± 7.19 | 9.97 ± 3.03 | 0.9900 | 9.98 ± 4.45 |
| Proteinuria, (n, %) | 1 (6.67) | 5 (12.20) | 0.5536 | 6 (10.71) |
| Hypertension (HTN), (n, %) | 1 (6.67) | 6 (14.63) | 0.5879 | 7 (12.50) |
| Hematuria, (n, %) | 1 (6.67) | 2 (4.88) | 0.7924 | 3 (5.36) |
| Hemolytic anemia, (n, %) | 2 (13.33) | 1 (2.44) | 0.201 | 3 (5.36) |
| Leukopenia, (n, %) | 1 (6.67) | 7 (17.07) | 0.4276 | 8 (14.29) |
| Arthritis, (n, %) | 10 (66.67) | 17 (41.46) | 0.1334 | 27 (48.21) |
| Serositis, (n, %) | 1 (6.67) | 3 (7.32) | 0.9333 | 4 (7.14) |
| Lupus nephritis, (n, %) | 4 (26.67) | 21 (51.22) | 0.0902 | 25 (44.64) |
| Thrombocytopenia, (n, %) | 1 (6.67) | 6 (14.63) | 0.6607 | 7 (12.50) |
| Diabetes, (n, %) | 0 (0.00) | 3 (7.32) | 0.5563 | 3 (5.36) |
| Dyslipidemia, (n, %) | 2 (13.33) | 4 (9.76) | 0.7793 | 6 (10.71) |
| Alopecia, (n, %) | 5 (33.33) | 4 (9.76) | 0.0479 | 9 (16.07) |
| Myositis, (n, %) | 1 (6.67) | 3 (7.32) | 0.9333 | 4 (7.14) |
| Chronic cutaneous lupus, (n, %) | 9 (60.00) | 5 (12.20) | 0.0011 | 14 (25.00) |
| Acute or subacute cutaneous lupus, (n, %) | 8 (53.33) | 12 (29.27) | 0.1218 | 20 (35.71) |
| Baseline systemic lupus erythematosus disease activity index (SLEDAI-2K) | ||||
| No activity (SLEDAI = 0) | 0 (0.00) | 10 (24.39) | 0.1598 | 10 (17.86) |
| Mild activity (SLEDAI = 1 to 5) | 5 (33.33) | 15 (36.59) | 20 (35.71) | |
| Moderate activity (SLEDAI = 6 to 10) | 5 (33.33) | 9 (21.95) | 14 (25.00) | |
| High activity (SLEDAI = 11 to 19) | 5 (33.33) | 6 (14.63) | 11 (19.64) | |
| Very high activity (SLEDAI ≥ 20) | 0 (0.00) | 1 (2.44) | 1 (1.79) |
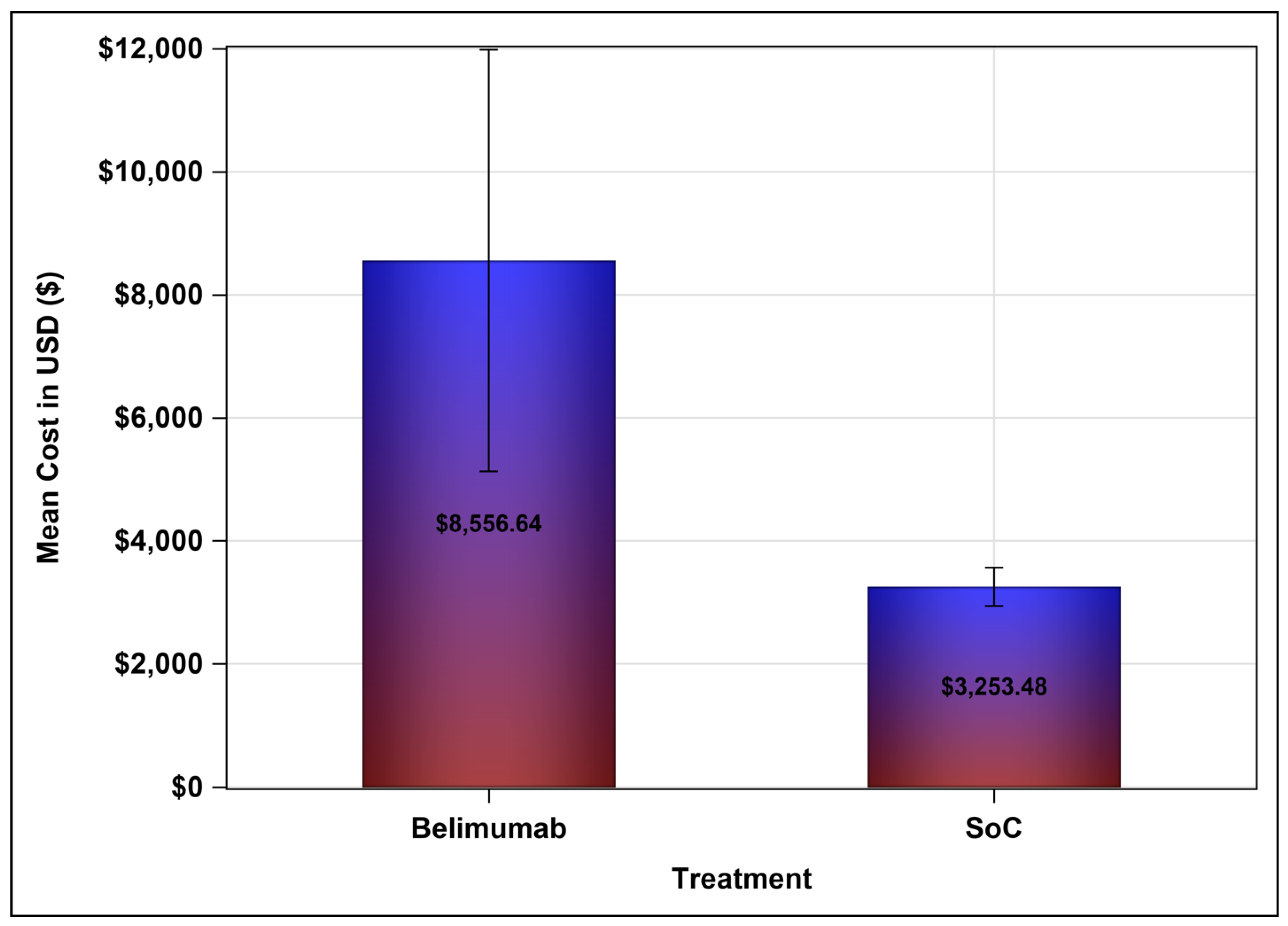
| Belimumab | SoC | Mean Difference (95% Confidence Interval) | |
|---|---|---|---|
| Cost of treatment (USD), mean ± SD | 8556.64 ± 6189.75 | 3253.48 ± 987.86 | 5303.16 (2735.61–7802.52) |
| Difference between baseline and follow–up SLEDAI–2K score, mean ± SD | 3.33 ± 4.59 | −0.0487 ± 5.48 | 3.378 (1.769–6.831) |
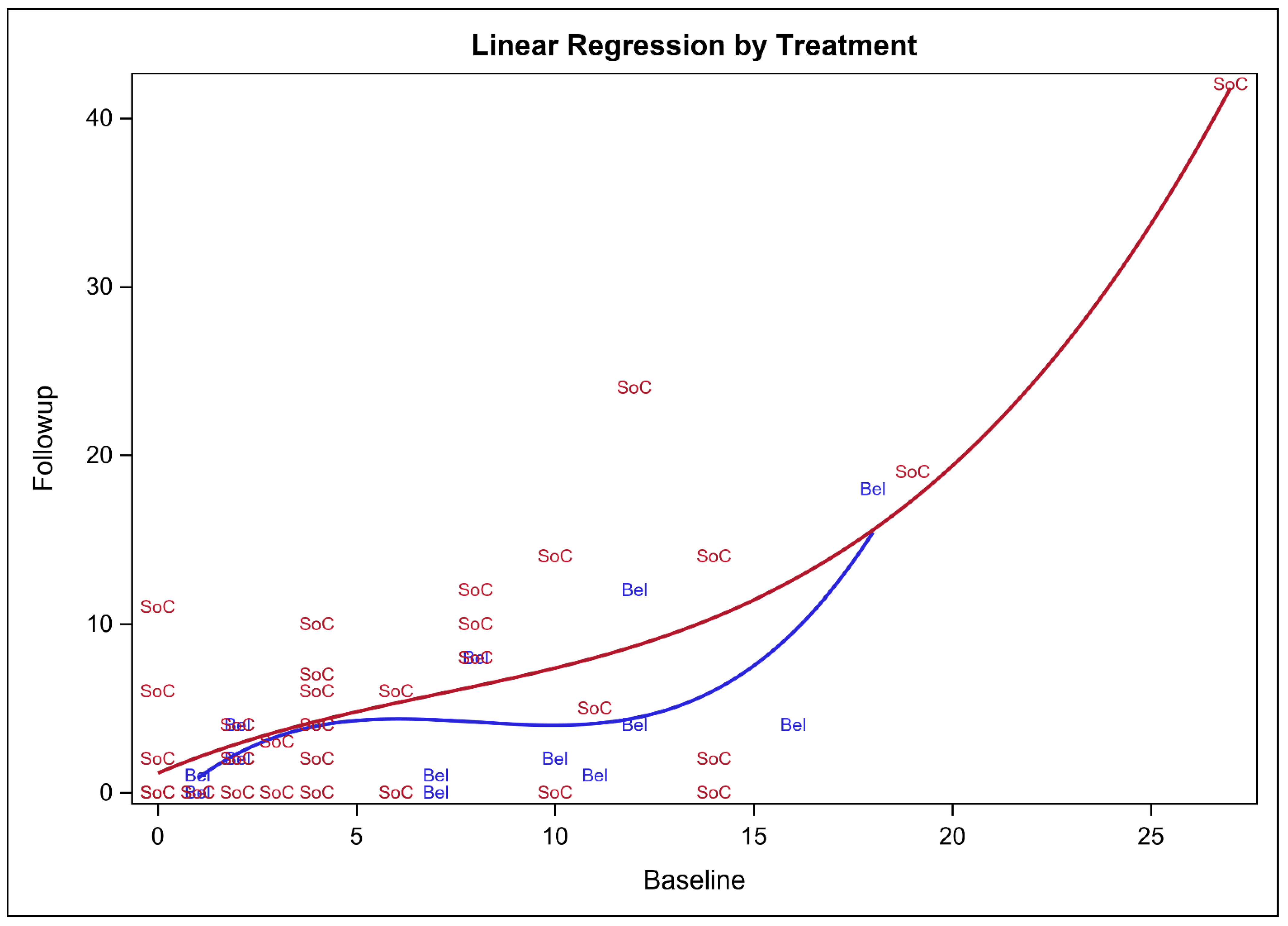
| Variable | Regression Coefficient (β-Estimate) | p-Value | 95% Confidence Interval |
|---|---|---|---|
| Belimumab vs. SoC | 3.6400 | 0.0409 * | 0.15735–7.1227 |
| Baseline SLEDAI-2K score | 0.0932 | 0.4647 | −0.1610–0.3474 |
| Duration of treatment | 0.9336 | 0.3079 | −0.8873–2.7546 |
| Age | 0.0418 | 0.5736 | −0.1065–0.1902 |
| Female vs. male | 1.5707 | 0.5496 | −3.6681–6.8095 |
| Duration of illness | −0.6195 | 0.5796 | −2.8520–1.6130 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsuwayegh, A.; Almaghlouth, I.A.; Almasaoud, M.A.; Alzaid, A.S.; Alsuhaibani, A.A.; Almana, L.H.; Alabdulkareem, S.M.; Abudahesh, J.A.; AlRuthia, Y. Cost Consequence Analysis of Belimumab versus Standard of Care for the Management of Systemic Lupus Erythematosus in Saudi Arabia: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2023, 20, 1917. https://doi.org/10.3390/ijerph20031917
Alsuwayegh A, Almaghlouth IA, Almasaoud MA, Alzaid AS, Alsuhaibani AA, Almana LH, Alabdulkareem SM, Abudahesh JA, AlRuthia Y. Cost Consequence Analysis of Belimumab versus Standard of Care for the Management of Systemic Lupus Erythematosus in Saudi Arabia: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2023; 20(3):1917. https://doi.org/10.3390/ijerph20031917
Chicago/Turabian StyleAlsuwayegh, Aseel, Ibrahim A. Almaghlouth, Majed Ali Almasaoud, Abdullah Sulaiman Alzaid, Adel Abdulaziz Alsuhaibani, Lyan Hassan Almana, Sara Mohammed Alabdulkareem, Joud Abdullah Abudahesh, and Yazed AlRuthia. 2023. "Cost Consequence Analysis of Belimumab versus Standard of Care for the Management of Systemic Lupus Erythematosus in Saudi Arabia: A Retrospective Cohort Study" International Journal of Environmental Research and Public Health 20, no. 3: 1917. https://doi.org/10.3390/ijerph20031917