

Arsenic: A Perspective on Its Effect on Pioglitazone Bioavailability
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials and Reagents
2.2. Study Population
2.3. Clinical and Anthropometric Analyses
2.4. Methodology
2.4.1. Arsenic Determination
2.4.2. Determination of Pioglitazone in Human Plasma
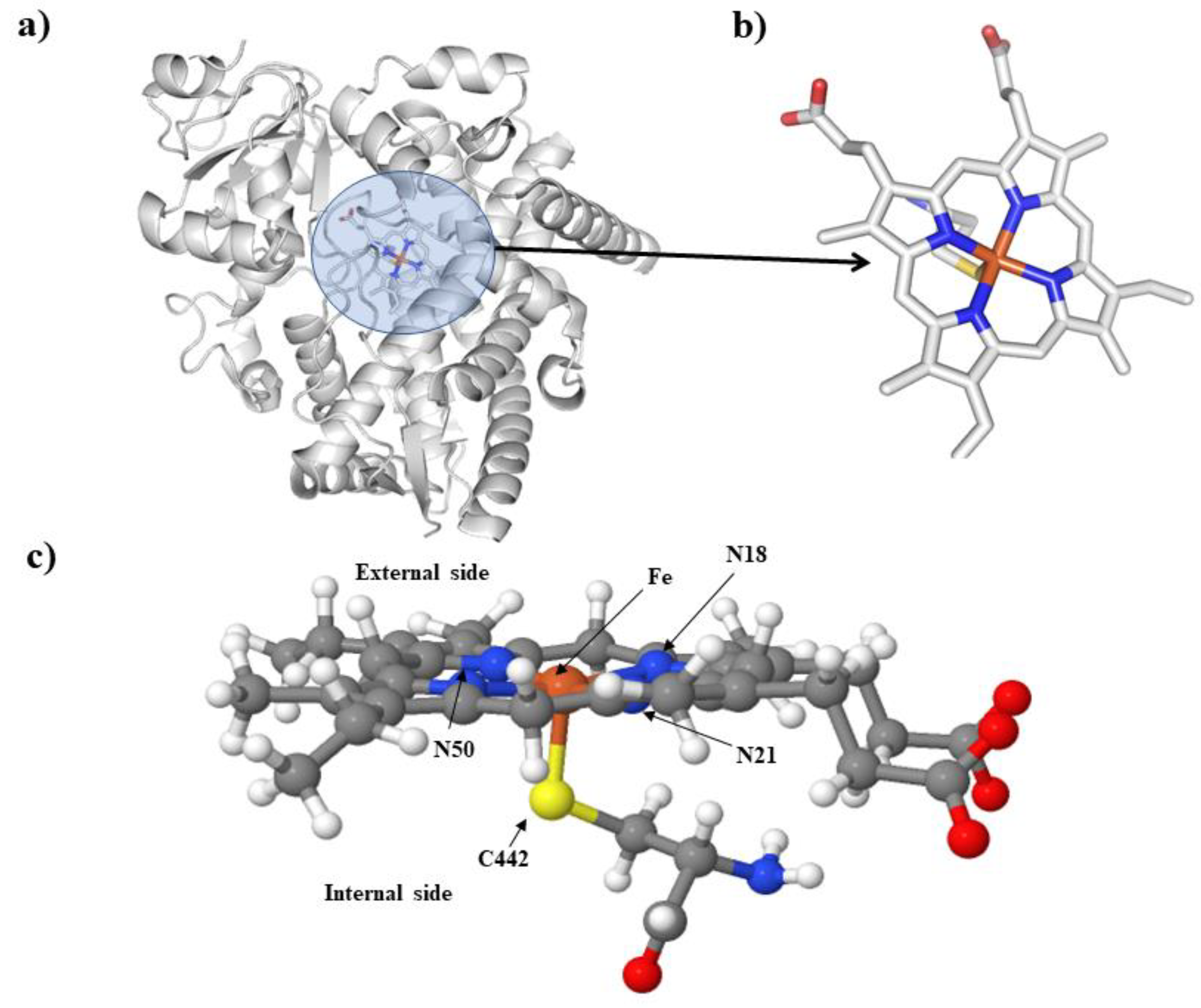
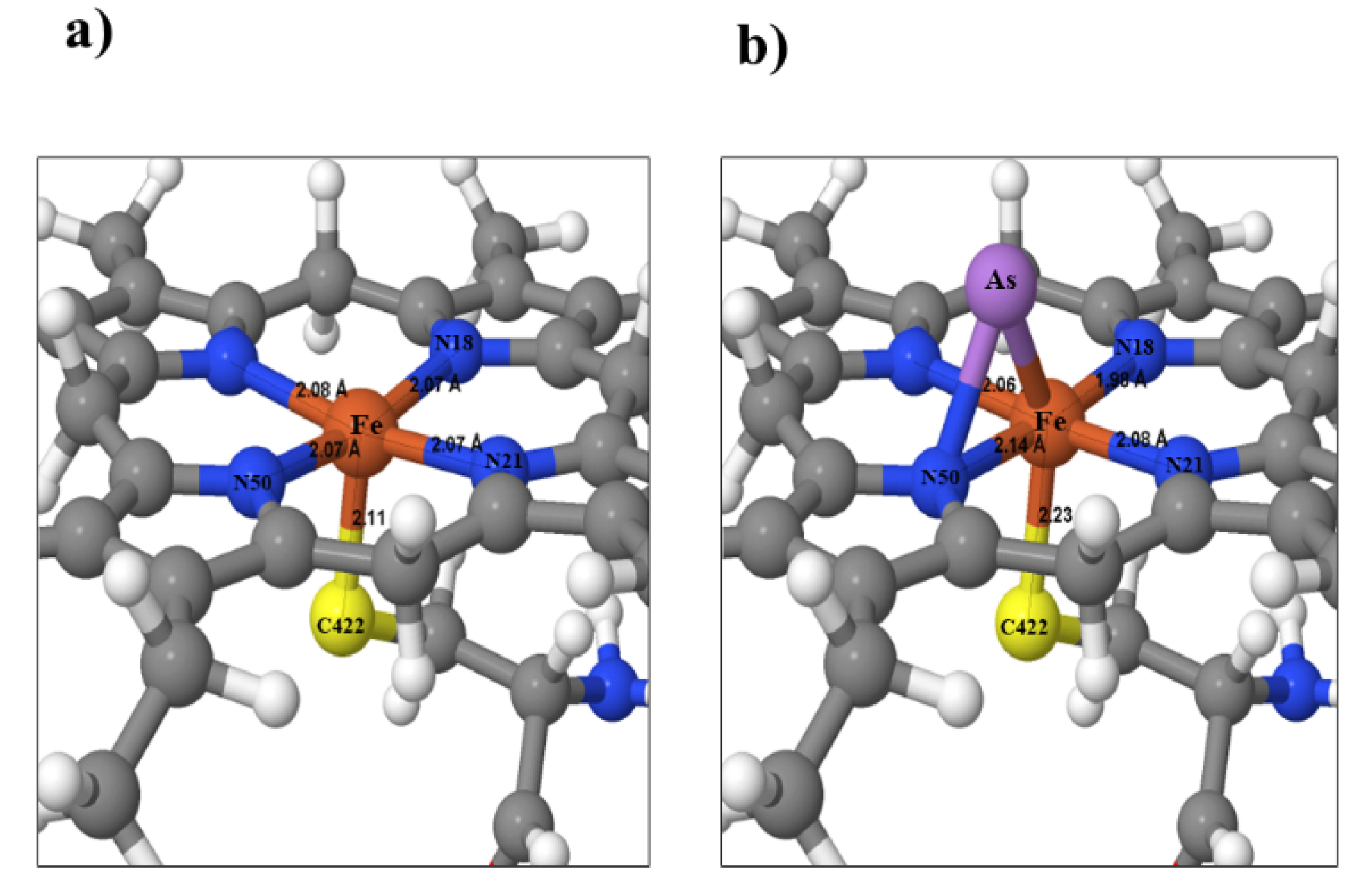
2.4.3. In Silico Analysis of Interaction of Isoenzymes CYP 3A4 and CYP 2C8 with As
2.4.4. Statistical Analyses
- Statistical analysis was performed using the Origin Pro 2018 package.
- Anthropometric parameters were compared by Mann–Whitney U test (p ≤ 0.05).
- For pioglitazone pharmacokinetics, Shapiro–Wilk analysis was used (n ≤ 3): p > 0.05, t-Student (independent group comparison).
- Arsenic interactions and anthropometric and clinical exposure parameters with pioglitazone pharmacokinetics were determined by Spearman correlation.
3. Results
4. Discussion
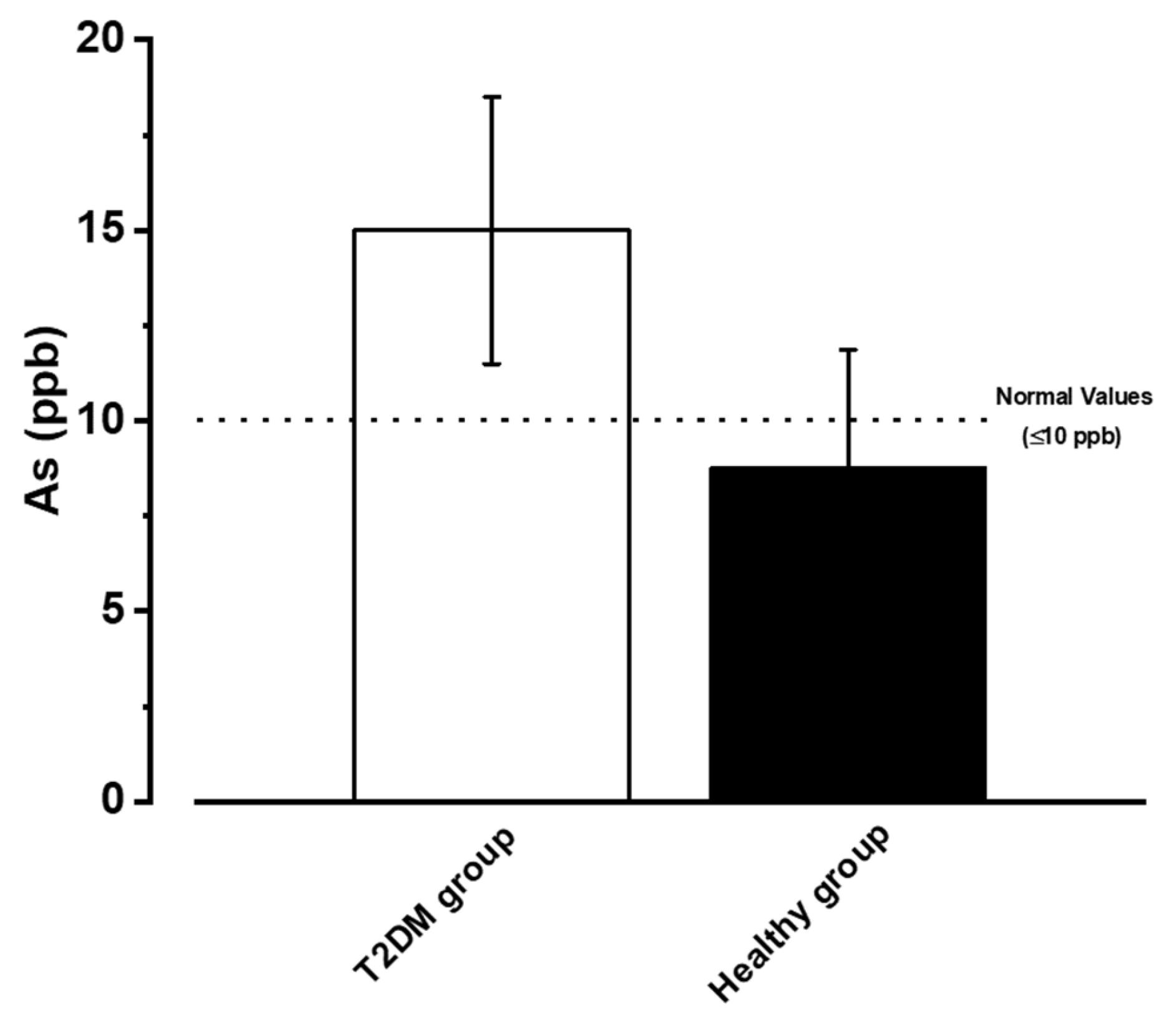
- The average age of populations is different, with the T2DM group being older than the healthy group and the older age group having higher As exposure.
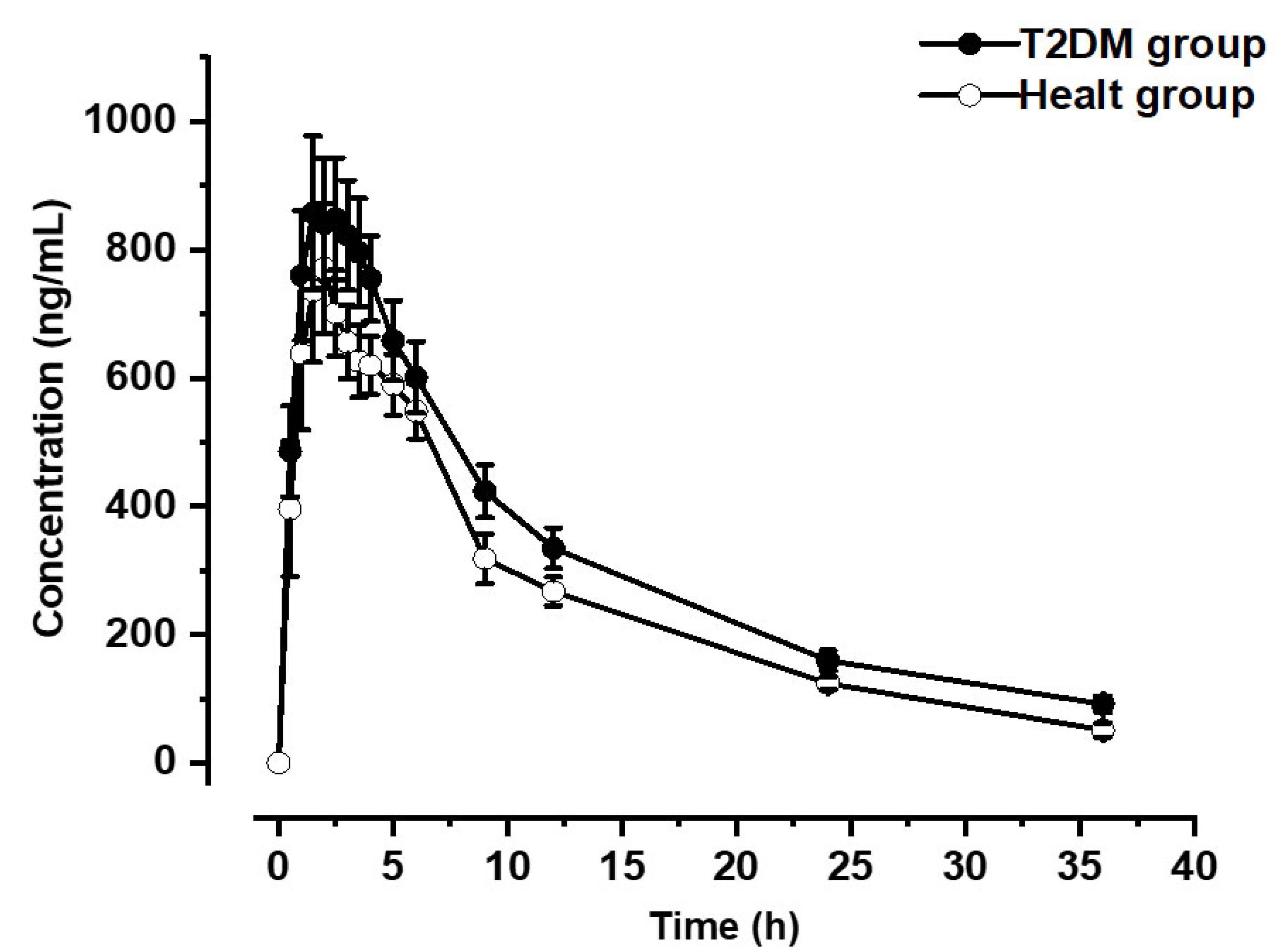
- Due to the associations previously established in the literature that refer to the fact that chronic exposure to high concentrations of As decreases the expression of cytochrome P450, the T2DM group tends to metabolize the drug slowly compared to the control population.
- The presence of As in the cytochrome P450 structure could generate variation in pharmacokinetic parameters, thus, the ABCt is higher in the TDM2 group compared to the healthy group.
- In the absence of sufficient cytochrome action, the drug seems more bioavailable in systemic circulation for a longer time, thus causing the difference in the populations.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reis, V.; Duarte, A.C. Occurrence, distribution, and significance of arsenic speciation. In Comprehensive Analytical Chemistry; Duarte, A.C., Reis, V., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; Volume 85, pp. 1–14. [Google Scholar]
- Abdul, K.S.M.; Jayasinghe, S.S.; Chandana, E.P.; Jayasumana, C.; De Silva, P.M.C. Arsenic and human health effects: A review. Environ. Toxicol. Pharmacol. 2015, 40, 828–846. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Zhao, K.; Suarez, F.; Pacquette, L.; Schmitz, D. Heavy metal contamination. Food Saf. China: Sci. Technol. Manag. Regul. 2017, 237–251. [Google Scholar] [CrossRef]
- Díaz-Palma, P.; Alfaro, G.; Hengst, M.; Pozo, P.; Stegen, S.; Queirolo, F.; Rojo, G.; Silva, P.; Arias, D.; Gallardo, K.; et al. Kinetics of arsenite removal by halobacteria from a highland Andean Chilean Salar. Aquat. Biosyst. 2013, 9, 8. [Google Scholar] [CrossRef] [Green Version]
- Isokpehi, R.D.; Udensi, U.K.; Anyanwu, M.N.; Mbah, A.N.; Johnson, M.O.; Edusei, K.; Bauer, M.A.; Hall, R.A.; Awofolu, O.R. Knowledge Building Insights on Biomarkers of Arsenic Toxicity to Keratinocytes and Melanocytes. Biomark. Insights 2012, 7, BMI-S7799. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.Y.; Chai, L.Y.; Yang, W.C. Arsenic distribution and pollution characteristics. In Arsenic Pollution Control in Nonferrous Metallurgy; Chai, L.Y., Ed.; Springer: Singapore, 2019; pp. 1–15. [Google Scholar] [CrossRef]
- Basu, A.; Mitra, S.; Chung, J.; Guha Mazumder, D.N.; Ghosh, N.; Kalman, D.; Von Ehrenstein, O.S.; Steinmaus, C.; Liaw, J.; Smith, A.H. Creatinine, diet, micronutrients, and arsenic methylation in West Bengal, India. Environ. Health Perspect. 2011, 119, 1308–1313. [Google Scholar] [CrossRef]
- Bhattacharjee, P.; Banerjee, M.; Giri, A.K. Role of genomic instability in arsenic-induced carcinogenicity. A review. Environ. Int. 2013, 53, 29–40. [Google Scholar] [CrossRef]
- Litter, M.I. Chemistry and Occurrence of Arsenic in Water. In Arsenic in Plants: Uptake, Consequences and Remediation Techniques; Kumar, P., Singh, R., Parihar, P., Prasad, S.M., Eds.; Wiley Online Library: Hoboken, NJ, USA, 2022; pp. 25–48. [Google Scholar]
- Lee, M.S.; Lee, J.H.; An, Y.J.; Park, C.H.; Lee, S.H.; Park, J.H.; Lee, J.K.; Park, T.J. Development of water quality criteria for arsenic to protect aquatic life based on species sensitivity distribution. Ecotoxicol. Environ. Saf. 2020, 189, 109933. [Google Scholar] [CrossRef]
- Rahaman, M.S.; Rahman, M.M.; Mise, N.; Sikder, M.T.; Ichihara, G.; Uddin, M.K.; Kurasaki, M.; Ichihara, S. Environmental arsenic exposure and its contribution to human diseases, toxicity mechanism, and management. Environ. Pollut. 2021, 289, 117940. [Google Scholar] [CrossRef]
- Adeloju, S.B.; Khan, S.; Patti, A.F. Arsenic Contamination of Groundwater and Its Implications for Drinking Water Quality and Human Health in Under-Developed Countries and Remote Communities—A Review. Appl. Sci. 2021, 11, 1926. [Google Scholar] [CrossRef]
- Palma-Lara, I.; Martínez-Castillo, M.; Quintana-Pérez, J.C.; Arellano-Mendoza, M.G.; Tamay-Cach, F.; Valenzuela-Limón, O.L.; García-Montalvo, E.A.; Hernández-Zavala, A. Arsenic exposure: A public health problem leading to several cancers. Regul. Toxicol. Pharmacol. 2020, 110, 104539. [Google Scholar] [CrossRef]
- Chen, Y.; Graziano, J.H.; Parvez, F.; Liu, M.; Slavkovich, V.; Kalra, T.; Argos, M.; Islam, T.; Ahmed, A.; Rakibuz-Zaman, M. Arsenic exposure from drinking water and mortality from cardiovascular disease in Bangladesh: Prospective cohort study. BMJ 2011, 342, d2431. [Google Scholar] [CrossRef] [Green Version]
- Basu, N.; Nam, D.H.; Kwansaa-Ansah, E.; Renne, E.P.; Nriagu, J.O. Multiple metals exposure in a small-scale artisanal gold mining community. Environ. Res. 2011, 111, 463–467. [Google Scholar] [CrossRef]
- Huang, C.F.; Chen, Y.W.; Yang, C.Y.; Tsai, K.S.; Yang, R.S.; Liu, S.H. Arsenic and diabetes: Current perspectives. Kaohsiung J. Med. Sci. 2011, 27, 402–410. [Google Scholar] [CrossRef] [Green Version]
- Lucio, M.; Barbir, R.; Lovrenčić, M.V.; Varžić, S.C.; Ljubić, S.; Duvnjak, L.S.; Milic, M.; Lovakovic, B.T.; Krivohlavek, A.; Vinkovic, I.; et al. Association between arsenic exposure and biomarkers of type 2 diabetes mellitus in a Croatian population: A comparative observational pilot study. Sci. Total Environ. 2020, 720, 137575. [Google Scholar] [CrossRef]
- PAHO (Pan American Health Organization). Plan of Action for the Prevention of Obesity in Children and Adolescents: Final Report. 2020. Available online: https://www.paho.org/en/documents/cd58inf5-plan-action-prevention-obesity-children-and-adolescents-final-report. (accessed on 14 November 2022).
- Singh, A.; Kukreti, R.; Saso, L.; Kukreti, S. Mechanistic Insight into Oxidative Stress-Triggered Signaling Pathways and Type 2 Diabetes. Molecules 2022, 27, 950. [Google Scholar] [CrossRef]
- Bower, J.K.; Butler, B.N.; Bose-Brill, S.; Kue, J.; Wassel, C.L. Peer Reviewed: Racial/Ethnic Differences in Diabetes Screening and Hyperglycemia Among US Women After Gestational Diabetes. Prev. Chronic Dis. 2019, 16, E145. [Google Scholar] [CrossRef] [Green Version]
- Díaz-Villaseñor, A.; Granados, O.; González-Palacios, B.; Tovar-Palacio, C.; Torre-Villalvazo, I.; Olivares-García, V.; Torres, N.; Tovar, A.R. Differential modulation of the functionality of white adipose tissue of obese Zucker (fa/fa) rats by the type of protein and the amount and type of fat. J. Nutr. Biochem. 2013, 11, 1798–1809. [Google Scholar] [CrossRef]
- Gaytán-Pacheco, N.; Lima-Rogel, V.; Méndez-Mancilla, A.; Escalante-Padrón, F.; Toro-Ortíz, J.C.; Jiménez-Capdeville, M.E.; Zaga-Clavellina, V.; Portales-Pérez, D.P.; Noyola, D.E.; Salgado-Bustamante, M. Changes in PPAR-γ expression are associated with microRNA profiles during fetal programming due to maternal overweight and obesity. Gynecol. Obstet. Invest. 2021, 5, 415–426. [Google Scholar] [CrossRef]
- Nebert, D.W.; Wikvall, K.; Miller, W.L. Human cytochromes P450 in health and disease. Philos. Trans. R. Soc. B Biol. Sci. 2013, 368, 20120431. [Google Scholar] [CrossRef]
- Yang, X.; Zhang, B.; Molony, C.; Chudin, E.; Hao, K.; Zhu, J.; Gaedigk, A.; Suver, C.; Zhong, H.; Leeder, J.S.; et al. Systematic genetic and genomic analysis of cytochrome P450 enzyme activities in human liver. Genome Res. 2010, 20, 1020–1036. [Google Scholar] [CrossRef] [Green Version]
- Shirasaka, Y.; Chang, S.Y.; Grubb, M.F.; Peng, C.C.; Thummel, K.E.; Isoherranen, N.; Rodrigues, A.D. Effect of CYP3A5 expression on the inhibition of CYP3A-catalyzed drug metabolism: Impact on modeling CYP3A-mediated drug-drug interactions. Drug. Metab. Dispos. 2013, 41, 1566–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz de Montellano, P.R. Cytochrome P450-activated prodrugs. Future Med. Chem. 2013, 5, 213–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernández-Ordáz, G.; Segura-Castruita, M.A.; Álvarez-González, L.C.; Aldaco-Nuncio, R.A.; Fortis-Hernández, M.; González Cervantes, G. Behavior of arsenic in soils of the Región Lagunera of Coahuila, Mexico. Terra Latinoam. 2013, 31, 295–303. [Google Scholar]
- Johnson, E.F.; Stout, C.D. Structural diversity of eukaryotic membrane cytochrome p450s. J. Biol. Chem. 2013, 288, 17082–17090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noreault-Conti, T.L.; Fellows, A.; Jacobs, J.M.; Trask, H.W.; Strom, S.C.; Evans, R.M.; Wrighton, S.A.; Sinclair, P.R.; Sinclair, J.F.; Nichols, R.C. Arsenic decreases RXRalpha-dependent transcription of CYP3A and suppresses immune regulators in hepatocytes. Int. Immunopharmacol. 2012, 12, 651–656. [Google Scholar] [CrossRef] [Green Version]
- Naraharisetti, S.B.; Aggarwal, M.; Sarkar, S.N.; Malik, J.K. Concurrent subacute exposure to arsenic through drinking water and malathion via diet in male rats affects hepatic drug-metabolizing enzymes. Arch. Toxicol. 2008, 82, 543. [Google Scholar] [CrossRef]
- Pérez-Verdín, G. Los recursos forestales maderables y el desarrollo social y económico en el estado de Durango. Madera Y Bosques 2006, 12, 3–15. [Google Scholar] [CrossRef] [Green Version]
- Coronado-González, J.A.; Del Razo, L.M.; García-Vargas, G.; Sanmiguel-Salazar, F.; Escobedo-De la Peña, J. Inorganic arsenic exposure and type 2 diabetes mellitus in Mexico. Environ. Res. 2007, 104, 383–389. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines for Drinking Water Quality, 3rd ed.; World Health Organization: Geneva, Switzerland, 2004; Volume 1. [Google Scholar]
- Navas-Acien, A.; Silbergeld, E.K.; Streeter, R.A.; Clark, J.M.; Burke, T.A.; Guallar, E. Arsenic exposure and type 2 diabetes: A systematic review of the experimental and epidemiologic evidence. Environ. Health Perspect. 2006, 114, 641–648. [Google Scholar] [CrossRef] [Green Version]
- El-Ghiaty, M.A.; El-Kadi, A.O. The Duality of Arsenic Metabolism: Impact on Human Health. Annu. Rev. Pharmacol. 2022, 63. [Google Scholar] [CrossRef]
- El-Ghiaty, M.A.; Alqahtani, M.A.; El-Kadi, A.O.S. Down-regulation of hepatic cytochromes P450 1A1 and 1A2 by arsenic trioxide (ATO) in vivo and in vitro: A role of heme oxygenase 1. Chem-Biol. Interact. 2022, 364, 110049. [Google Scholar] [CrossRef]
- Noreault, T.L. Mechanisms by which Arsenite Decreases CYP3A; Dissertations Publishing; Dartmouth College: Hanover, NH, USA, 2005; p. 3179243. [Google Scholar]
- Yamada, Y.; Matsuo, H.; Watanabe, S.; Kato, K.; Yajima, K.; Hibino, T.; Yokoi, K.; Ichihara, S.; Metoki, N.; Yoshida, H.; et al. Association of a polymorphism of CYP3A4 with type 2 diabetes mellitus. Int. J. Mol. Med. 2007, 20, 703–707. [Google Scholar] [CrossRef] [Green Version]
- Jamil, K.; Kandula, V.; Kandula, R.; Asimuddin, M.; Joshi, S.; Yerra, S.K. Polymorphism of CYP3A4* 2 and eNOS genes in the diabetic patients with hyperlipidemia undergoing statin treatment. Mol. Biol. Rep. 2014, 41, 6719–6727. [Google Scholar] [CrossRef]
- Hart, S.N.; Zhong, X.B. P450 oxidoreductase: Genetic polymorphisms and implications for drug metabolism and toxicity. Expert Opin. Drug Metab. Toxicol. 2008, 4, 439–452. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Healthy Group | T2DM Group |
|---|---|---|
| Males (n 1) | 1 | 9 |
| Females (n) | 10 | 11 |
| Median (Xmin 3–Xmax 2) | Median (Xmin–Xmax) | |
| Age (years) | 44 (29–84) | 56 (33–71) |
| Weight (kg) | 75 (55–92) | 75 (53–104) |
| Height (meters) | 1.6 (1.52–1.66) | 1.6 (0.94–1.75) |
| Systolic blood pressure (mmHg) | 110 (100–150) | 130 (100–188) * |
| Diastolic blood pressure (mmHg) | 80 (60–100) | 80 (50–120) |
| Cardiac frequency (beats per minute, bpm) | 78 (68–92) | 72 (59–92) * |
| Fasting glucose (mg/dL) | 85 (68–95) | 174 (101–322) * |
| HbAc1α (%) | 5.5 (4.8–13.1) | 9 (6–12.5) * |
| Insulin (IU/mL) | 9.09 (2098–21.4) | 5.55 (2–12.9) * |
| TGO (UI/mL) | 24 (12–37) | 41.2 (19.3–89.3) * |
| TGP (UI/mL) | 16 (10–52) | 31 (14–69) * |
| Coordinates | As mg/L | Average As mg/L | % Above the Limit NOM-127- SSA1-2021 | |||
|---|---|---|---|---|---|---|
| Latitude (N) | Longitude (O) | 1st Sampling | 2nd Sampling | |||
| 1 | 24°47.611′ | 104°1.511′ | 0.058 | 0.036 | 0.047 | 89.65% |
| 2 | 24°47.246′ | 104°2.367′ | 0.074 | 0.071 | 0.073 | 193.16% |
| 3 | 24°47.425′ | 104°2.229′ | MNE | 0.071 | 0.071 | 184% |
| 4 | 24°47.529′ | 104°2.059′ | 0.046 | 0.074 | 0.061 | 141.67% |
| 5 | 24°47.244′ | 104°2.098′ | 0.223 | 0.074 | 0.149 | 497.03% |
| 6 | 24°48.013′ | 104°1.273′ | 0.066 | 0.00022 | 0.033 | 33.67% |
| 7 | 24°47.941′ | 104°2.372′ | 0.034 | 0.038 | 0.036 | 44.85% |
| 8 | 24°47.281′ | 104°1.855′ | 0.279 | 0.00022 | 0.139 | 459.39% |
| 9 | 24°47.914′ | 104°1.349′ | 0.096 | 0.079 | 0.087 | 251.88% |
| 10 | 24°48.448′ | 104°1.963′ | MNE | 0.019 | 0.019 | Acceptable |
| 11 | 24°47.910′ | 104°1.439′ | 0.083 | 0.084 | 0.084 | 236.09% |
| 12 | 24°47.324′ | 104°2.026′ | 0.00022 | 0.078 | 0.039 | 58.33% |
| 13 | 24°47.733′ | 104°1.667′ | 0.074 | 0.072 | 0.073 | 194.13% |
| 14 | --- | --- | 0.287 | --- | 0.211 | 747.06% |
| 15 | 24°48.208′ | 104°1.460′ | 0.043 | MNE | 0.043 | 72% |
| 16 | 24°47.283′ | 104°2.395′ | 0.074 | 0.1004 | 0.087 | 250.69% |
| 17 | 24°47.569′ | 104°2.121′ | 0.068 | 0.095 | 0.082 | 228.01% |
| 18 | 24°47.733′ | 104°1.667′ | 0.066 | 0.00022 | 0.033 | 32.55% |
| 19 | 24°48.157′ | 104°1.428′ | 0.082 | 0.0805 | 0.081 | 226.34% |
| 20 | 24°47.233′ | 104°2.282′ | 0.072 | 0.068 | 0.071 | 182.43% |
| 21 | 24°47.596′ | 104°2.342′ | 0.00022 | 0.096 | 0.048 | 92.46% |
| 22 | 24°43.940′ | 104°5.330′ | 0.058 | 0.102 | 0.081 | 221.96% |
| 23 | 24°47.800′ | 104°2.290′ | 0.027 | 0.095 | 0.061 | 146.35% |
| 24 | 24°47.809′ | 104°2.027′ | 0.071 | 0.092 | 0.081 | 226.21% |
| 25 | 24°47.727′ | 104°1.677′ | 0.065 | 0.0804 | 0.073 | 192.16% |
| 26 | 24°47.417′ | 104°2.200′ | 0.067 | 0.086 | 0.076 | 207.48% |
| 27 | 24°47.429′ | 104°2.245′ | 0.084 | 0.083 | 0.084 | 236.82% |
| 28 | 24°48.030′ | 104°1.319′ | 0.044 | 0.063 | 0.054 | 116.73% |
| 29 | 24°47.348′ | 104°2.272′ | 0.231 | 0.247 | 0.239 | 857.49% |
| 30 | 24°47.769′ | 104°1.516′ | 0.064 | 0.062 | 0.063 | 155.44% |
| 31 | 24°47.266′ | 104°2.402′ | 0.024 | 0.026 | 0.025 | 2.41% |
| 32 | 24°47.700′ | 104°1.695′ | 0.049 | 0.053 | 0.051 | 107.51% |
| 33 | 24°47.725′ | 104°1.716′ | 0.062 | 0.0604 | 0.061 | 145.38% |
| 34 | 24°46.848′ | 104°1.705′ | 0.041 | 0.046 | 0.043 | 73.92% |
| 35 | 24°47.010′ | 104°1.939′ | 0.219 | 0.269 | 0.244 | 877.08% |
| 36 | 24°46.779′ | 104°2.883′ | 0.016 | 0.022 | 0.019 | Acceptable |
| Population | 1 Ke (1/h) | 2 T ½ (h) | 3 ABCt (ng.h/mL) * | 4 Cmax (ng) | 5 Tmax (h) | 6 Ka (1/h) * | 7 Vd (L) | 8 Cl (L/h) * |
|---|---|---|---|---|---|---|---|---|
| Diabetes | 0.066 ± 0.012 | 15.22 ± 2.005 | 13747.49 ± 733.667 | 1066.594 ± 121.964 | 2.15 ± 0.254 | 0.501 ± 0.116 | 39.202 ± 4.5438 | 1.859 ± 0.106 |
| Controls | 0.089 ± 0.017 | 10.56 ± 1.657 | 10909.6 ± 1039.06 | 883.081 ± 87.9569 | 2 ± 0.387 | 2.396 ± 0.467 | 37.810 ± 5.234 | 2.640 ± 0.232 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terrones-Gurrola, M.C.d.R.; Ponce-Peña, P.; Salas-Pacheco, J.M.; Camacho-Luis, A.; Pozos-Guillén, A.d.J.; Nieto-Delgado, G.; López-Guzmán, O.D.; Vértiz-Hernández, A.A. Arsenic: A Perspective on Its Effect on Pioglitazone Bioavailability. Int. J. Environ. Res. Public Health 2023, 20, 1901. https://doi.org/10.3390/ijerph20031901
Terrones-Gurrola MCdR, Ponce-Peña P, Salas-Pacheco JM, Camacho-Luis A, Pozos-Guillén AdJ, Nieto-Delgado G, López-Guzmán OD, Vértiz-Hernández AA. Arsenic: A Perspective on Its Effect on Pioglitazone Bioavailability. International Journal of Environmental Research and Public Health. 2023; 20(3):1901. https://doi.org/10.3390/ijerph20031901
Chicago/Turabian StyleTerrones-Gurrola, María Cruz del Rocío, Patricia Ponce-Peña, José Manuel Salas-Pacheco, Abelardo Camacho-Luis, Amaury de Jesús Pozos-Guillén, Guillermo Nieto-Delgado, Olga Dania López-Guzmán, and Angel Antonio Vértiz-Hernández. 2023. "Arsenic: A Perspective on Its Effect on Pioglitazone Bioavailability" International Journal of Environmental Research and Public Health 20, no. 3: 1901. https://doi.org/10.3390/ijerph20031901