
Mi-CARE: Comparing Three Evidence-Based Interventions to Promote Colorectal Cancer Screening among Ethnic Minorities within Three Different Clinical Contexts
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AA | African American |
| CRC | Colorectal Cancer |
| Mi-CARE | Mile Square Health Center Colorectal Cancer Awareness, Referral and Education Program |
| FQHC | Federally Qualified Health Center |
| EHR | Electronic Health Record |
| LA | Latin American |
| MSHC | Mile Square Health Center |
| IPTW | Inverse Probability Treatment Weighting |
References
- Edwards, B.K.; Ward, E.; Kohler, B.A.; Eheman, C.; Zauber, A.G.; Anderson, R.N.; Jemal, A.; Schymura, M.J.; Lansdorp-Vogelaar, I.; Seeff, L.C.; et al. Annual report to the nation on the status of cancer, 1975–2006, featuring colorectal cancer trends and impact of interventions (risk factors, screening, and treatment) to reduce future rates. Cancer 2010, 116, 544–573. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.; Desantis, C.; Jemal, A. Colorectal cancer statistics. CA A Cancer J. Clin. 2014, 64, 104–117. [Google Scholar] [CrossRef] [PubMed]
- White, A.; Vernon, S.W.; Franzini, L.; Du, X.L. Racial and ethnic disparities in colorectal cancer screening persisted despite expansion of medicare’s screening reimbursement. Cancer Epidemiol. Biomark. Prev. 2011, 20, 811–817. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, N.U.; Pelletier, V.; Winter, K.; Albatineh, A.N. Factors explaining racial/ethnic disparities in rates of physician recommendation for colorectal cancer screening. Am. J. Public Health 2013, 103, e91–e99. [Google Scholar] [CrossRef] [PubMed]
- James, T.M.; Greiner, K.A.; Ellerbeck, E.F.; Feng, C.; Ahluwalia, J.S. Disparities in colorectal cancer screening: A guideline-based analysis of adherence. Ethn Dis. 2006, 16, 228–233. [Google Scholar] [PubMed]
- Liss, D.T.; Baker, D.W. Understanding current racial/ethnic disparities in colorectal cancer screening in the United States: The contribution of socioeconomic status and access to care. Am. J. Prev. Med. 2014, 46, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Wallace, D.A.C.; Baltrus, P.T.; Wallace, T.C.; Blumenthal, D.S.; Rust, G.S. Black white disparities in receiving a physician recommendation for colorectal cancer screening and reasons for not undergoing screening. J. Health Care Poor Underserved 2013, 24, 1115–1124. [Google Scholar] [CrossRef]
- Heintzman, J.D.; Ezekiel-Herrera, D.N.; Quiñones, A.R.; Lucas, J.A.; Carroll, J.E.; Gielbultowicz, S.H.; Cottrell, E.C.; Marino, M. Disparities in Colorectal Cancer Screening in Latinos and Non-Hispanic Whites. Am. J. Prev. Med. 2022, 62, 203–210. [Google Scholar] [CrossRef]
- Wang, J.; Moehring, J.; Stuhr, S.; Krug, M. Barriers to colorectal cancer screening in Hispanics in the United States: An integrative review. Appl. Nurs. Res. 2013, 26, 218–224. [Google Scholar] [CrossRef]
- Jones, L.A.; Ferrans, C.E.; Polite, B.N.; Brewer, K.C.; Maker, A.V.; Pauls, H.A.; Rauscher, G.H. Examining racial disparities in colon cancer clinical delay in the Colon Cancer Patterns of Care in Chicago study. Ann. Epidemiol. 2017, 27, 731–738.e1. [Google Scholar] [CrossRef]
- Carethers, J.M. Racial and ethnic disparities in colorectal cancer incidence and mortality. Adv. Cancer Res. 2021, 151, 197–229. [Google Scholar] [PubMed]
- McLeod, M.R.; Galoosian, A.; May, F.P. Racial and Ethnic Disparities in Colorectal Cancer Screening and Outcomes. Hematol. Clin. N. Am. 2022, 36, 415–428. [Google Scholar] [CrossRef] [PubMed]
- Mobley, L.R.; Kuo, T.-M. Demographic Disparities in Late-Stage Diagnosis of Breast and Colorectal Cancers Across the USA. J. Racial Ethn. Health Disparities 2017, 4, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.; Lopez, A.; Castaneda, G.; Bhuket, T.; Liu, B.; Yee, S.; Irwin, D.; Wong, R.J. Black Patients with Colorectal Cancer Have More Advanced Cancer Stage at Time of Diagnosis: A Community-Based Safety-Net Hospital Experience. J. Community Health 2017, 42, 724–729. [Google Scholar] [CrossRef] [PubMed]
- Chicago Health Atlas. Chicago Department of Public Health, Healthy Chicago Survey (2021–2022). Colorectal Cancer Screening Rate [% of Adults]. 2021. Available online: https://chicagohealthatlas.org/indicators/HCSCRP?topic=colorectal-cancer-screening-rate (accessed on 6 October 2023).
- Arnett, M.J.; Thorpe, R.J., Jr.; Gaskin, D.J.; Bowie, J.V.; LaVeist, T.A. Race, Medical Mistrust, and Segregation in Primary Care as Usual Source of Care: Findings from the Exploring Health Disparities in Integrated Communities Study. J. Urban Health 2016, 93, 456–467. [Google Scholar] [CrossRef] [PubMed]
- Olagoke, A.A.; Olagoke, O.O.; Hughes, A.M. Intention to Vaccinate Against the Novel 2019 Coronavirus Disease: The Role of Health Locus of Control and Religiosity. J. Relig. Health 2021, 60, 65–80. [Google Scholar] [CrossRef] [PubMed]
- Powell, W.; Richmond, J.; Mohottige, D.; Yen, I.; Joslyn, A.; Corbie-Smith, G. Medical Mistrust, Racism, and Delays in Preventive Health Screening Among African-American Men. Behav. Med. 2019, 45, 102–117. [Google Scholar] [CrossRef] [PubMed]
- Lucas, T.; Hayman, L.W.; Blessman, J.E.; Asabigi, K.; Novak, J.M. Gain versus loss-framed messaging and colorectal cancer screening among African Americans: A preliminary examination of perceived racism and culturally targeted dual messaging. Br. J. Health Psychol. 2016, 21, 249–267. [Google Scholar] [CrossRef]
- Rogers, C.R.; Mitchell, J.A.; Franta, G.J.; Foster, M.J.; Shires, D. Masculinity, Racism, Social Support, and Colorectal Cancer Screening Uptake Among African American Men: A Systematic Review. Am. J. Men’s Health 2017, 11, 1486–1500. [Google Scholar] [CrossRef]
- Crowley, R. Racial and Ethnic Disparities in Health Care; American College of Physicians: Philadelphia, PA, USA, 2010. [Google Scholar]
- Serchen, J.; Doherty, R.; Atiq, O.; Hilden, D. A Comprehensive Policy Framework to Understand and Address Disparities and Discrimination in Health and Health Care: A Policy Paper From the American College of Physicians. Ann. Intern. Med. 2021, 174, 529–532. [Google Scholar] [CrossRef]
- Serchen, J.; Doherty, R.; Hewett-Abbott, G.; Atiq, O.; Hilden, D. Understanding and Addressing Disparities and Discrimination in Education and in the Physician Workforce: A position Paper; American College of Physicians: Philadelphia, PA, USA, 2021. [Google Scholar]
- Centers for Disease Control and Prevention NC for HS. National Health Interview Survey, 1987–2021; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021.
- National Cancer Institute. SEER Cancer Statistics Factsheets: Common Cancer Sites. Available online: https://seer.cancer.gov/statfacts/html/disparities.html (accessed on 10 October 2023).
- Guide to Community Preventive Services. Cancer Screening: Multicomponent Interventions Colorectal Cancer. Available online: https://www.thecommunityguide.org/findings/cancer-screening-multicomponent-interventions-colorectal-cancer.html (accessed on 8 October 2019).
- Joseph, D.A.; Redwood, D.; DeGroff, A.; Butler, E.L. Use of Evidence-Based Interventions to Address Disparities in Colorectal Cancer Screening. MMWR Suppl. 2016, 65, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.J.; Milch, V.E.; Crawford-Williams, F.; Agbejule, O.A.; Joseph, R.; Johal, J.; Dick, N.; Wallen, M.P.; Ratcliffe, J.; Agarwal, A.; et al. Patient navigation across the cancer care continuum: An overview of systematic reviews and emerging literature. CA A Cancer J. Clin. 2023, 73, 565–589. [Google Scholar] [CrossRef] [PubMed]
- Naylor, K.; Ward, J.; Polite, B.N. Interventions to improve care related to colorectal cancer among racial and ethnic minorities: A systematic review. J. Gen. Intern. Med. 2012, 27, 1033–1046. [Google Scholar] [CrossRef] [PubMed]
- Piette, C.; Durand, G.; Bretagne, J.-F.; Faivre, J. Additional mailing phase for FIT after a medical offer phase: The best way to improve compliance with colorectal cancer screening in France. Dig. Liver Dis. 2017, 49, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Percac-Lima, S.; Grant, R.W.; Green, A.R.; Ashburner, J.M.; Gamba, G.; Oo, S.; Richter, J.M.; Atlas, S.J. A culturally tailored navigator program for colorectal cancer screening in a community health center: A randomized, controlled trial. J. Gen. Intern. Med. 2009, 24, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.A.; Santos, S.; Jandorf, L.; Christie, J.; Castillo, A.; Winkel, G.; Itzkowitz, S. A Program to Enhance Completion of Screening Colonoscopy Among Urban Minorities. Clin. Gastroenterol. Hepatol. 2008, 6, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.W.; Brown, T.; Buchanan, D.R.; Weil, J.; Balsley, K.; Ranalli, L.; Lee, J.Y.; Cameron, K.A.; Ferreira, M.R.; Stephens, Q.; et al. Comparative effectiveness of a multifaceted intervention to improve adherence to annual colorectal cancer screening in community health centers: A randomized clinical trial. JAMA Intern. Med. 2014, 174, 1235–1241. [Google Scholar] [CrossRef]
- Katz, M.L.; Fisher, J.L.; Fleming, K.; Paskett, E.D. Patient activation increases colorectal cancer screening rates: A randomized trial among low-income minority patients. Cancer Epidemiol. Biomark. Prev. 2012, 21, 45–52. [Google Scholar] [CrossRef]
- Green, B.B.; Wang, C.-Y.; Anderson, M.L.; Chubak, J.; Meenan, R.T.; Vernon, S.W.; Fuller, S.; Weinberg, D.S.; Barkun, A.; Turner, B.J.; et al. An Automated Intervention with Stepped Increases in Support to Increase Uptake of Colorectal Cancer Screening. Ann. Intern. Med. 2013, 158, 301–311. [Google Scholar] [CrossRef]
- Sharma, K.P.; DeGroff, A.; Maxwell, A.E.; Cole, A.M.; Escoffery, N.C.; Hannon, P.A. Evidence-Based Interventions and Colorectal Cancer Screening Rates: The Colorectal Cancer Screening Program, 2015–2017. Am. J. Prev. Med. 2021, 61, 402–409. [Google Scholar] [CrossRef]
- Kim, K.E.; Tangka, F.K.L.; Jayaprakash, M.; Randal, F.T.; Lam, H.; Freedman, D.; Carrier, L.A.; Sargant, C.; Maene, C.; Hoover, S.; et al. Effectiveness and Cost of Implementing Evidence-Based Interventions to Increase Colorectal Cancer Screening Among an Underserved Population in Chicago. Health Promot. Pr. 2020, 21, 884–890. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.A.; Rohweder, C.L.; Leeman, J.; Friedman, D.B.; Gizlice, Z.; Vanderpool, R.C.; Askelson, N.; Best, A.; Flocke, S.A.; Glanz, K.; et al. Use of Evidence-Based Interventions and Implementation Strategies to Increase Colorectal Cancer Screening in Federally Qualified Health Centers. J. Community Health 2018, 43, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Tu, S.-P.; Chun, A.; Yasui, Y.; Kuniyuki, A.; Yip, M.-P.; Taylor, V.; Bastani, R. Adaptation of an evidence-based intervention to promote colorectal cancer screening: A quasi-experimental study. Implement. Sci. 2014, 9, 85. [Google Scholar] [CrossRef] [PubMed]
- Buscemi, J.; Miguel, Y.S.; Tussing-Humphreys, L.; Watts, E.A.; Fitzgibbon, M.L.; Watson, K.; Winn, R.A.; Matthews, K.L.; Molina, Y. Rationale and design of Mi-CARE: The mile square colorectal cancer screening, awareness and referral and education project. Contemp. Clin. Trials 2017, 52, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Human Services US. Federally Qualified Health Center; Centers for Medicare & Medicaid Services: Baltimore, MD, USA, 2023.
- Centers for Disease Control and Prevention. Leading Causes of Death; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2023.
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA A Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA A Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Alcaraz, K.I.; Wiedt, T.L.; Daniels, E.C.; Yabroff, K.R.; Guerra, C.E.; Wender, R.C. Understanding and addressing social determinants to advance cancer health equity in the United States: A blueprint for practice, research, and policy. CA A Cancer J. Clin. 2020, 70, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Braveman, P.A.; Kumanyika, S.; Fielding, J.; LaVeist, T.; Borrell, L.N.; Manderscheid, R.; Troutman, A. Health Disparities and Health Equity: The Issue Is Justice. Am. J. Public Health 2011, 101, S149–S155. [Google Scholar] [CrossRef]
- Singh, G.K.; Jemal, A. Socioeconomic and Racial/Ethnic Disparities in Cancer Mortality, Incidence, and Survival in the United States, 1950–2014: Over Six Decades of Changing Patterns and Widening Inequalities. J. Environ. Public Health 2017, 2819372. [Google Scholar] [CrossRef]
- Neighbors, H.W.; Mattingly, D.T.; Johnson, J.; Morse, K. The contribution of research to racial health equity? Blame and responsibility in navigating the status quo of anti-black systemic racism. Soc. Sci. Med. 2023, 316, 115209. [Google Scholar] [CrossRef]
- Cogburn, C.D. Culture, Race, and Health: Implications for Racial Inequities and Population Health. Milbank Q. 2019, 97, 736–761. [Google Scholar] [CrossRef] [PubMed]
- Avalos, N. What Does It Mean to Heal From Historical Trauma? AMA J. Ethics 2021, 23, E494–E498. [Google Scholar] [CrossRef] [PubMed]
- Mills, R.; AMA Adopts Guidelines that Confront Systemic Racism in Medicine. American Medical Association. 2021. Available online: https://www.ama-assn.org/press-center/press-releases/ama-adopts-guidelines-confront-systemic-racism-medicine (accessed on 22 September 2022).
- Pallok, K.; De Maio, F.; Ansell, D.A. Structural Racism—A 60-Year-Old Black Woman with Breast Cancer. N. Engl. J. Med. 2019, 380, 1489–1493. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. J. Natl. Med. Assoc. 2002, 94, 666–668. [Google Scholar] [PubMed]
- Bailey, Z.D.; Krieger, N.; Agénor, M.; Graves, J.; Linos, N.; Bassett, M.T. Structural racism and health inequities in the USA: Evidence and interventions. Lancet 2017, 389, 1453–1463. [Google Scholar] [CrossRef] [PubMed]
- Schouten, B.C.; Meeuwesen, L. Cultural differences in medical communication: A review of the literature. Patient Educ. Couns. 2006, 64, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Mead, E.L.; Doorenbos, A.Z.; Javid, S.H.; Haozous, E.A.; Alvord, L.A.; Flum, D.R.; Morris, A.M. Shared Decision-Making for Cancer Care Among Racial and Ethnic Minorities: A Systematic Review. Am. J. Public Health 2013, 103, e15–e29. [Google Scholar] [CrossRef]
- Gittner, L.S.; Clochesy, J.M.; Gutierrez, J.O.; Robinson, J.L. Be Heard: Healthcare Perspectives From Medically And Socially Disenfranchised Communities. J. Health Hum. Serv. Adm. 2015, 38, 215–236. [Google Scholar]
- Boulware, L.A.; Cooper, L.E.; Ratner, L.A. LaVeist, T.; Powe, N.R. Race and Trust in the Health Care System. Public Health Rep. 2003, 118, 358–365. [Google Scholar] [CrossRef]
- Sweeney, C.F.; Zinner, D.; Rust, G.; Fryer, G.E. Race/ethnicity and health care communication: Does patient-provider concordance matter? Med. Care 2005, 54, 1005–1009. [Google Scholar] [CrossRef]
- Betancourt, J.R.; Green, A.R.; Carrillo, J.E.; Ii, O.A.F. Defining Cultural Competence: A Practical Framework for Addressing Racial/Ethnic Disparities in Health and Health Care. Feature Artic. Public Health Rep. 2003, 118, 293–302. [Google Scholar] [CrossRef]
- Degrie, L.; Gastmans, C.; Mahieu, L.; de Casterlé, B.D.; Denier, Y. How do ethnic minority patients experience the intercultural care encounter in hospitals? A systematic review of qualitative research. BMC Med. Ethic 2017, 18, 2. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, K.; Putt, M.; Halbert, C.H.; Grande, D.; Schwartz, J.S.; Liao, K.; Marcus, N.; Demeter, M.B.; Shea, J.A. Prior experiences of racial discrimination and racial differences in health care system distrust. Med. Care 2013, 51, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A. Body and Soul: The Black Panther Party and the Fight against Medical Discrimination; University of Minnesota Press: Minneapolis, MI, USA, 2011. [Google Scholar]
- Flores, G. Culture and the patient-physician relationship: Achieving cultural competency in health care. J. Pediatr. 2000, 136, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Medina-Martínez, J.; Saus-Ortega, C.; Sánchez-Lorente, M.M.; Sosa-Palanca, E.M.; García-Martínez, P.; Mármol-López, M.I. Health Inequities in LGBT People and Nursing Interventions to Reduce Them: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 11801. [Google Scholar] [CrossRef] [PubMed]
- Washington, H.A. Medical Apartheid: The Dark History of Medical Experimentation on Black Americans from Colonial Times to the Present; DoubleDay: New York, NY, USA, 2006. [Google Scholar]
- Dimick, J.; Ruhter, J.; Sarrazin, M.V.; Birkmeyer, J.D.; Qi, A.C.; Butler, A.M.; Maddox, K.E.J.; Li, Y.; Cen, X.; Cai, X.; et al. Black patients more likely than whites to undergo surgery at low-quality hospitals in segregated regions. Health Aff. 2013, 32, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Hasnain-Wynia, R.; Baker, D.W.; Nerenz, D.; Feinglass, J.; Beal, A.C.; Mary, C. Disparities in Health Care Are Driven by Where Minority Patients Seek Care Examination of the Hospital Quality Alliance Measures. Arch Intern Med. 2007, 167, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- White, K.; Haas, J.S.; Williams, D.R. Elucidating the role of place in health care disparities: The example of racial/ethnic residential segregation. Health Serv. Res. 2012, 47, 1278–1299. [Google Scholar] [CrossRef]
- Muller, C.; Ihionkhan, E.; Stoffel, E.M.; Kupfer, S.S. Disparities in Early-Onset Colorectal Cancer. Cells 2021, 10, 1018. [Google Scholar] [CrossRef]


{kind=link}
| Overall (n = 1252) | Mailed Birthday Reminders (n = 401) | Lay Navigation (n = 86) | Provider-Delivered Education (n = 765) | Chi-Square | ||
|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | Missing | p-Value | |
| Clinical Site | 0% | <0.0001 | ||||
| Multi-ethnic Provider | 500 (40%) | 80 (20%) | 34 (40%) | 386 (50%) | ||
| Predominantly AA Provider | 313 (25%) | 50 (12%) | 35 (40%) | 228 (30%) | ||
| Predominantly LA Provider | 439 (35%) | 271 (68%) | 17 (20%) | 151 (20%) | ||
| Patient Age | 0% | <0.0001 | ||||
| 50–64 | 995 (79%) | 295 (74%) | 78 (91%) | 622 (81%) | ||
| 65–75 | 257 (21%) | 106 (26%) | 8 (9%) | 143 (19%) | ||
| Patient Ethnicity | 0% | <0.0001 | ||||
| AA | 827 (66%) | 184 (46%) | 65 (75%) | 578 (76%) | ||
| LA | 425 (34%) | 217 (54%) | 21 (25%) | 187 (24%) | ||
| Patient Sex | 0% | 0.67 | ||||
| Female | 496 (40%) | 166 (41%) | 33 (38%) | 297 (39%) | ||
| Male | 756 (60%) | 235 (59%) | 53 (62%) | 468 (61%) | ||
| Patient Insurance | <1% | 0.15 | ||||
| Private | 302 (24%) | 113 (28%) | 20 (23%) | 169 (22%) | ||
| Public | 840 (67%) | 250 (62%) | 60 (70%) | 530 (69%) | ||
| Self-payer | 108 (9%) | 38 (9%) | 6 (7%) | 64 (8%) | ||
| Month of admission | <1% | <0.0001 | ||||
| Months 1–4 | 412 (33%) | 326 (81%) | 75 (87%) | 11 (1%) | ||
| Months 5–8 | 476 (38%) | 68 (17%) | 11 (13%) | 397 (52%) | ||
| Months 9–12 | 364 (29%) | 7 (2%) | 0 (0%) | 357 (47%) |
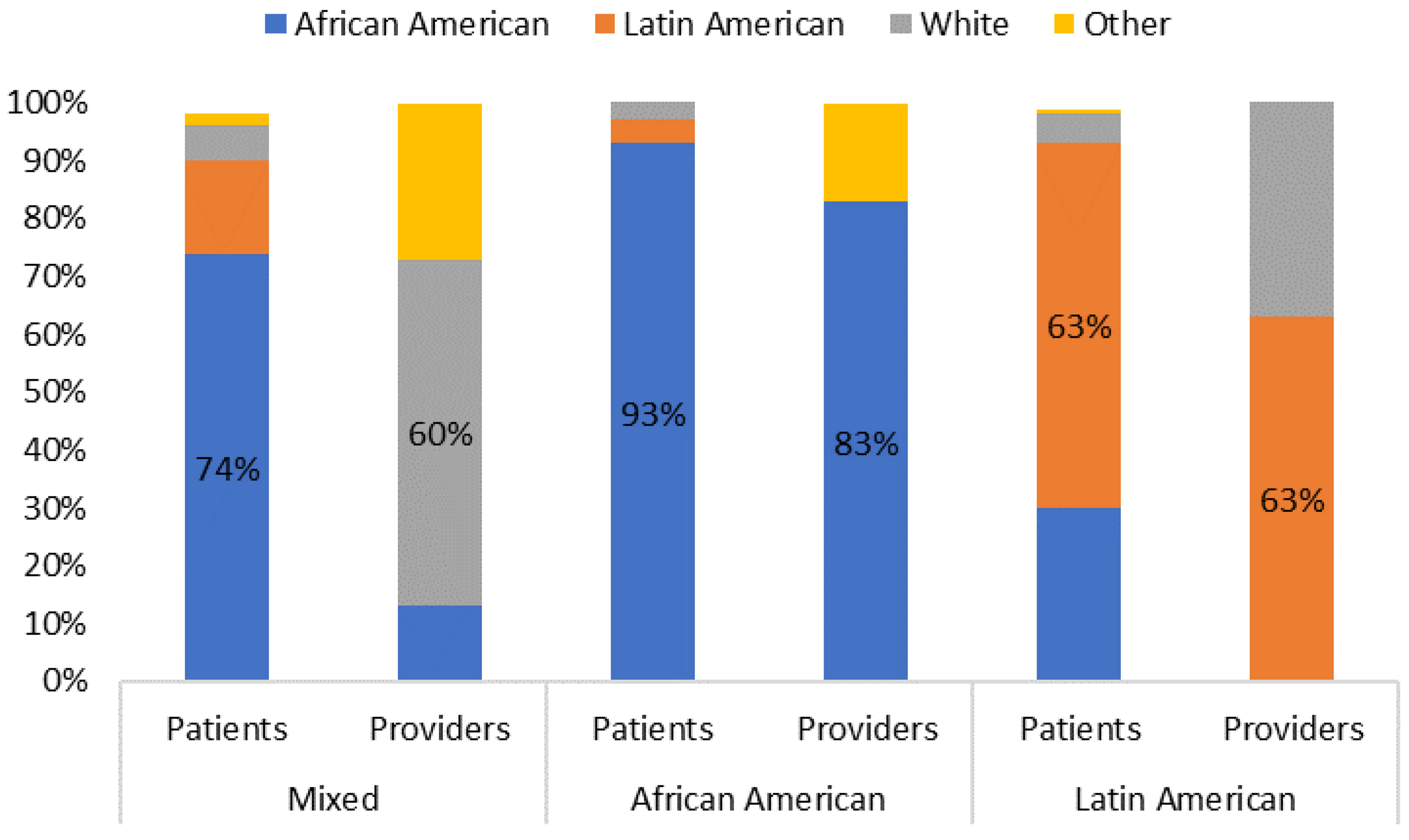
| Mixed Clinic | African American Clinic | Latin American Clinic | ||||
|---|---|---|---|---|---|---|
| Race/Ethnicity | Patients | Providers | Patients | Providers | Patients | Providers |
| African American | 74% | 13% | 93% | 83% | 30% | 0% |
| Latin American | 16% | 0% | 4% | 0% | 63% | 63% |
| White | 6% | 60% | 6% | 0% | 5% | 38% |
| Other | 2% | 27% | 2% | 17% | 1% | 0% |
| EBIs, Effect Modifiers, and Covariates | n (%) Received CRC Screening (n = 254) 1 | Chi-Square p-Value |
|---|---|---|
| Evidence-based Intervention (EBI) | 0.0004 | |
| Mailed Birthday Reminders | 99 (25%) | |
| Provider-delivered education | 129 (17%) | |
| Lay navigation | 26 (30%) | |
| Clinical Site | <0.0001 | |
| Multi-ethnic | 79 (16%) | |
| Predominantly AA | 29 (9%) | |
| Predominantly LA | 146 (33%) | |
| Patient Age | 0.77 | |
| 50–64 | 205 (21%) | |
| 65–75 years old | 49 (19%) | |
| Patient Ethnicity | <0.0001 | |
| AA | 115 (14%) | |
| LA | 139 (33%) | |
| Patient Sex | 0.23 | |
| Female | 109 (22%) | |
| Male | 145 (19%) | |
| Patient Insurance | 0.22 | |
| Private | 70 (23%) | |
| Public | 159 (19%) | |
| Self-payer | 25 (23%) | |
| Month of admission | 0.02 | |
| Months 1–4 | 102 (25%) | |
| Months 5–8 | 89 (19%) | |
| Months 9–12 | 63 (17%) |
| PRIMARY LOGISTIC REGRESSION MODELS (n = 1252) | OR | 95% CI | p | |
|---|---|---|---|---|
| Evidence-based Intervention (EBI) | ||||
| Mailed Birthday Reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 1.11 | 0.77 | 1.61 | 0.58 |
| Lay navigation | 2.62 | 1.47 | 4.64 | 0.001 |
| Interaction Term (EBI × Clinical Context) | 0.005 | |||
| Stratification by Clinical Site | ||||
| Clinic—Multi-ethnic | ||||
| Mailed Birthday Reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 0.50 | 0.27 | 0.94 | 0.03 |
| Lay navigation | 1.22 | 0.47 | 3.15 | 0.68 |
| Clinic—Predominantly AA | ||||
| Mailed Birthday Reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 1.20 | 0.34 | 4.32 | 0.78 |
| Lay navigation | 4.76 | 1.15 | 19.72 | 0.03 |
| Clinic—Predominantly LA | ||||
| Mailed Birthday Reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 1.63 | 1.07 | 2.49 | 0.02 |
| Lay navigation | 1.90 | 0.70 | 5.17 | 0.21 |
| SENSITIVITY LOGISTIC REGRESSION MODELS #1—NON-IMPUTED DATA (n = 1247) | ||||
| EBI | ||||
| Mailed Birthday Reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 1.00 | 0.67 | 1.50 | 0.98 |
| Lay navigation | 2.01 | 1.20 | 3.64 | 0.009 |
| Interaction Term (EBI × Clinical Context) | 0.04 | |||
| Stratification by Clinical Site | ||||
| Clinic—Multi-ethnic | ||||
| Mailed Birthday Reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 0.50 | 0.27 | 0.94 | 0.03 |
| Lay navigation | 1.22 | 0.47 | 3.13 | 0.69 |
| Clinic—Predominantly AA | ||||
| Mailed Birthday Reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 1.20 | 0.34 | 4.32 | 0.78 |
| Lay navigation | 4.76 | 1.15 | 19.72 | 0.03 |
| Clinic—Predominantly LA | ||||
| Mailed Birthday Reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 1.63 | 1.07 | 2.50 | 0.02 |
| Lay navigation | 1.90 | 0.70 | 5.17 | 0.21 |
| SENSITIVITY LOGISTIC REGRESSION MODELS #2—USING INVERSE PROBABILITY OF TREATMENT WEIGHING (IPTW) AND PROPENSITY SCORES (n = 1252) | ||||
| EBI | ||||
| Mailed Birthday Reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 1.15 | 0.83 | 1.63 | 0.42 |
| Lay navigation | 3.17 | 1.65 | 6.10 | 0.001 |
| Interaction Term (EBI × Clinical Context) | <0.0001 | |||
| Stratification by Clinical Site | ||||
| Clinic—Multi-ethnic | ||||
| Mailed Birthday Reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 0.76 | 0.35 | 1.63 | 0.48 |
| Lay navigation | 1.09 | 0.23 | 5.07 | 0.92 |
| Clinic—Predominantly AA | ||||
| Mailed Birthday Reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 4.31 | 0.58 | 32.00 | 0.15 |
| Lay navigation | 31.78 | 2.40 | 421.04 | 0.009 |
| Clinic—Predominantly LA | ||||
| Mailed Birthday Reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 3.49 | 2.30 | 5.29 | <0.0001 |
| Lay navigation | 2.20 | 1.01 | 4.75 | 0.05 |
| SENSITIVITY LOGISTIC REGRESSION MODELS #3—IN-PERSON APPROACHES ONLY (n = 851) | ||||
| EBI | ||||
| Provider-delivered education (Reference Group) | REF | REF | REF | |
| Lay navigation | 2.42 | 1.37 | 4.25 | 0.002 |
| Interaction Term (EBI × Clinical Context) | 0.03 | |||
| Stratification by Clinical Site | ||||
| Clinic—Multi-ethnic | ||||
| Provider-delivered education (Reference Group) | REF | REF | REF | |
| Lay navigation | 2.40 | 1.04 | 5.41 | 0.04 |
| Clinic—Predominantly AA | ||||
| Provider-delivered education (Reference Group) | REF | REF | REF | |
| Lay navigation | 3.92 | 1.51 | 10.19 | .005 |
| Clinic—Predominantly LA | ||||
| Provider-delivered education (Reference Group) | REF | REF | REF | |
| Lay navigation | 1.14 | 0.37 | 3.44 | 0.82 |
| SENSITIVITY LOGISTIC REGRESSION MODELS #4—(Patient race or ethnicity × clinical site) | ||||
| Clinic—Predominantly AA (Only AA patients; N = 418) | ||||
| Mailed birthday reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 1.52 | 0.53 | 4.34 | 0.44 |
| Lay navigation | 0.60 | 0.29 | 1.26 | 0.18 |
| Clinic—Predominantly LA (Only LA patients; N = 336) | ||||
| Mailed birthday reminders (Reference Group) | REF | REF | REF | |
| Provider-delivered education | 1.63 | 0.97 | 2.73 | 0.06 |
| Lay navigation | 1.97 | 0.72 | 5.40 | 0.19 |
| Clinical Site | ||||
|---|---|---|---|---|
| Approach | AA | LA | Mixed | |
| All (ref = mailed birthday reminder) | Lay | + | = | = |
| Provider | = | + | − | |
| In-person Approaches (ref = provider) | Lay | + | = | + |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watson, K.S.; Tossas, K.Y.; San Miguel, Y.; Gastala, N.; San Miguel, L.G.; Grumeretz, S.; Henderson, V.; Winn, R.; Jimbo, M.; Naylor, K.B.; et al. Mi-CARE: Comparing Three Evidence-Based Interventions to Promote Colorectal Cancer Screening among Ethnic Minorities within Three Different Clinical Contexts. Int. J. Environ. Res. Public Health 2023, 20, 7049. https://doi.org/10.3390/ijerph20227049
Watson KS, Tossas KY, San Miguel Y, Gastala N, San Miguel LG, Grumeretz S, Henderson V, Winn R, Jimbo M, Naylor KB, et al. Mi-CARE: Comparing Three Evidence-Based Interventions to Promote Colorectal Cancer Screening among Ethnic Minorities within Three Different Clinical Contexts. International Journal of Environmental Research and Public Health. 2023; 20(22):7049. https://doi.org/10.3390/ijerph20227049
Chicago/Turabian StyleWatson, Karriem S., Katherine Y. Tossas, Yazmin San Miguel, Nicole Gastala, Liliana G. San Miguel, Scott Grumeretz, Vida Henderson, Robert Winn, Masahito Jimbo, Keith B. Naylor, and et al. 2023. "Mi-CARE: Comparing Three Evidence-Based Interventions to Promote Colorectal Cancer Screening among Ethnic Minorities within Three Different Clinical Contexts" International Journal of Environmental Research and Public Health 20, no. 22: 7049. https://doi.org/10.3390/ijerph20227049