

School-Based Nutrition Programs in the Eastern Mediterranean Region: A Systematic Review
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
- -
- Articles/Reports were included in this review if they provided information relevant to school-based (or preschool-based) nutrition programs or interventions that have been developed, adopted or implemented by a governmental entity in countries of the EMR, irrespective of study design.
- -
- Articles reporting on school interventions that did not involve a governmental entity or governmental oversight were not included in the review.
- -
- Interventions targeting specific populations (individuals on therapeutic diets etc.) were excluded.
- -
- Individual articles/reports were excluded if they were published prior to 2000, or if they were in languages other than English, Arabic, and French.
- -
- There were no exclusion criteria based on the design of the study.
2.3. Study Selection
2.4. Data Extraction
2.5. Analysis
3. Results
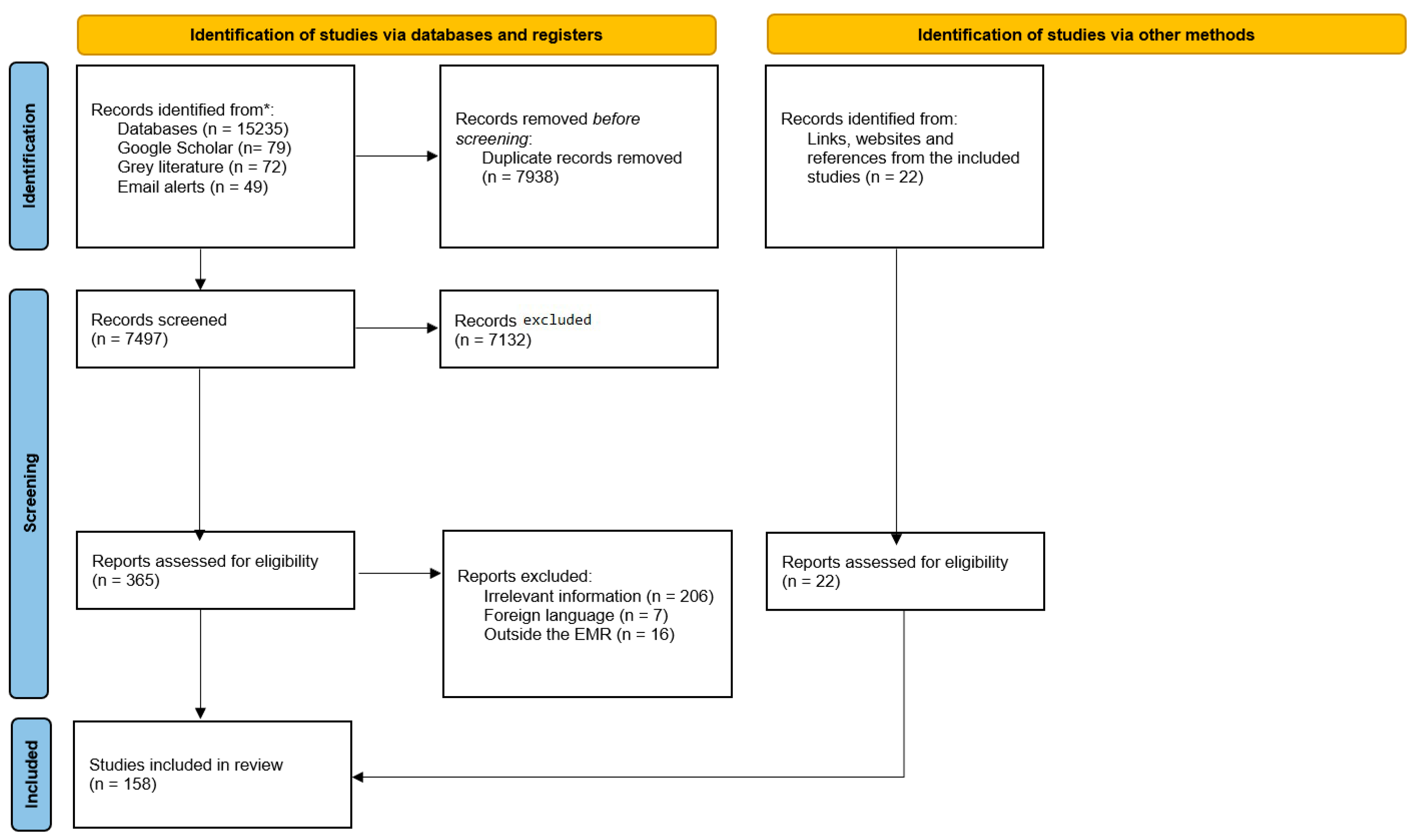
3.1. Search Results
3.2. Types of School-Based Programs/Interventions
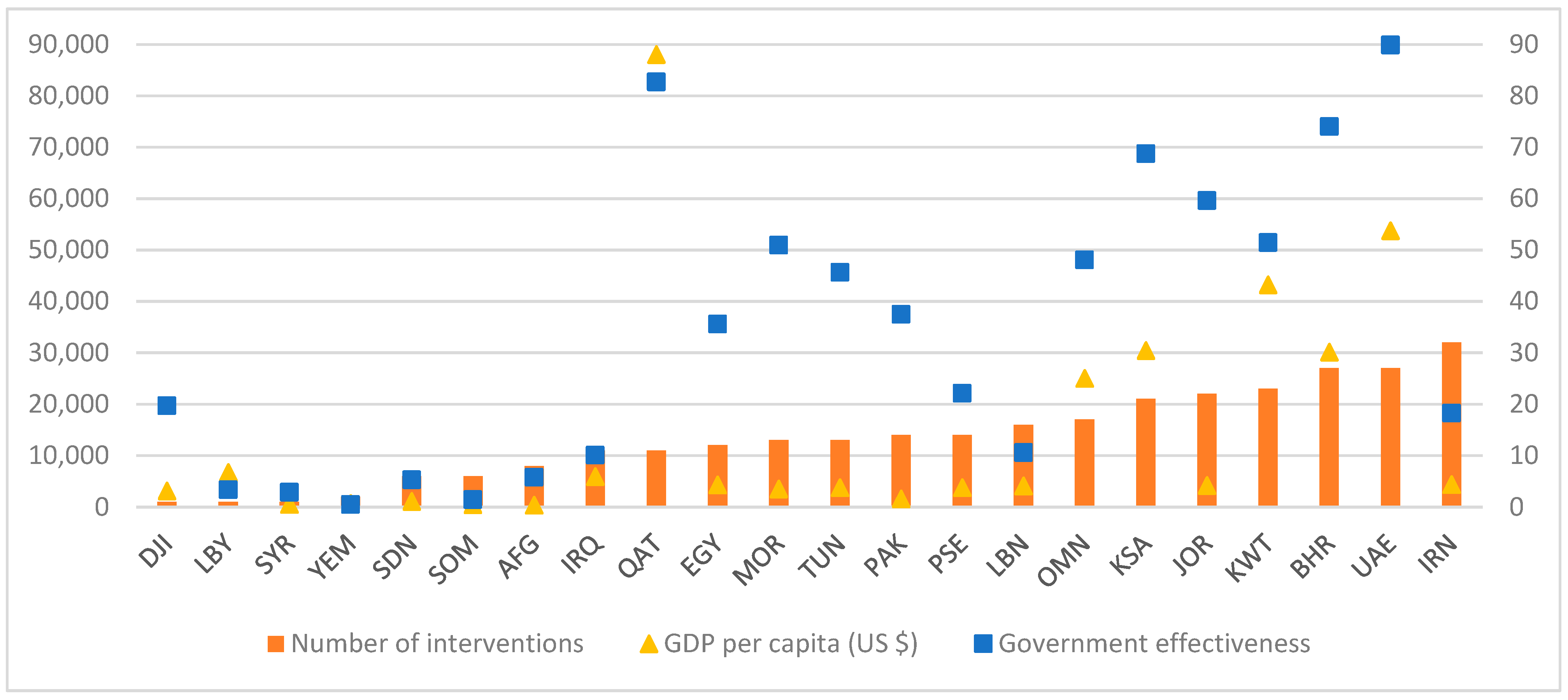
3.3. School-Based Nutrition Programs in Relation to Government Effectiveness and GDP
3.4. School-Feeding Programs
3.5. Micronutrient Supplementation Programs
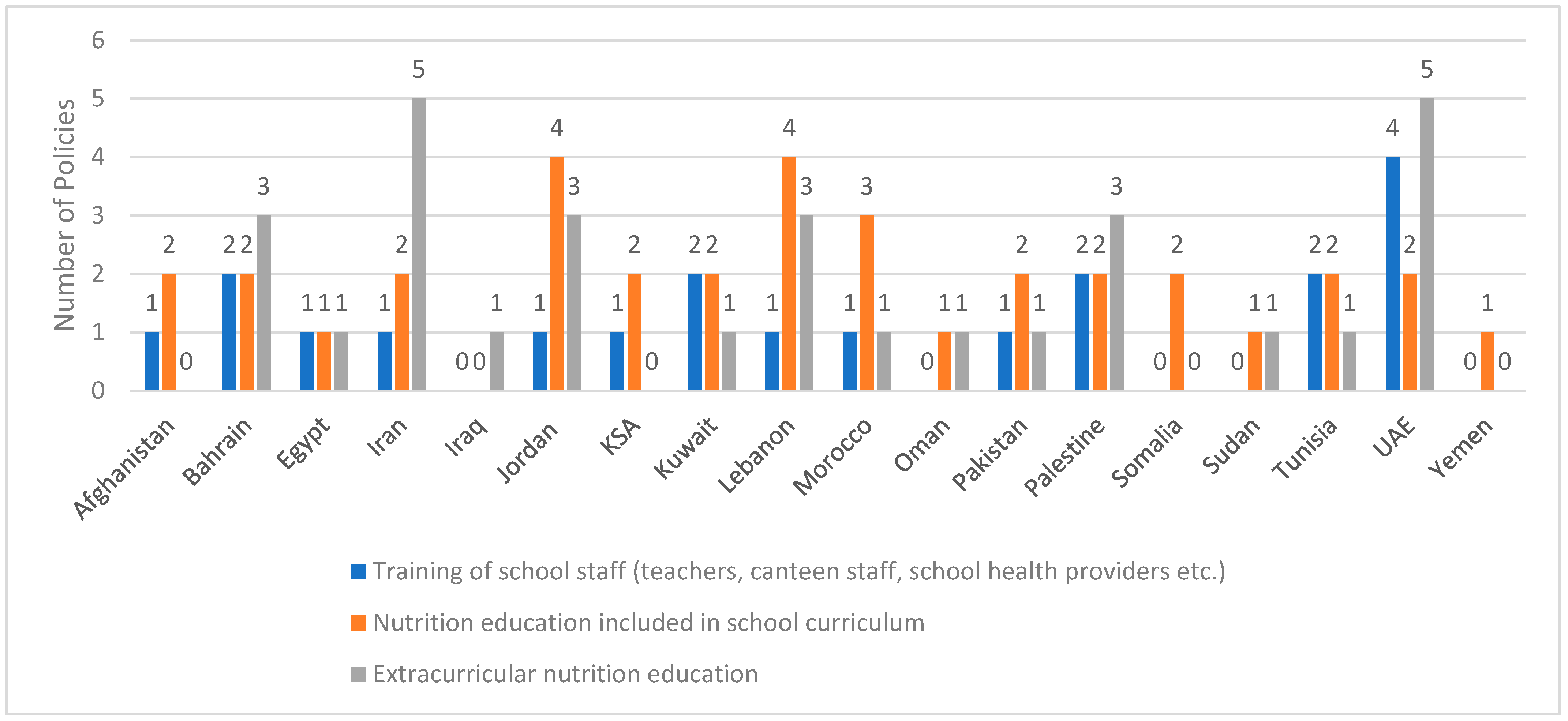
3.6. Inclusion of Nutrition Education in School Curricula
3.7. Inclusion of Extracurricular Nutrition Education
3.8. Training of School Staff
3.9. Standards Pertinent to School Canteens, Marketing of Food/Beverages or Vending Machines
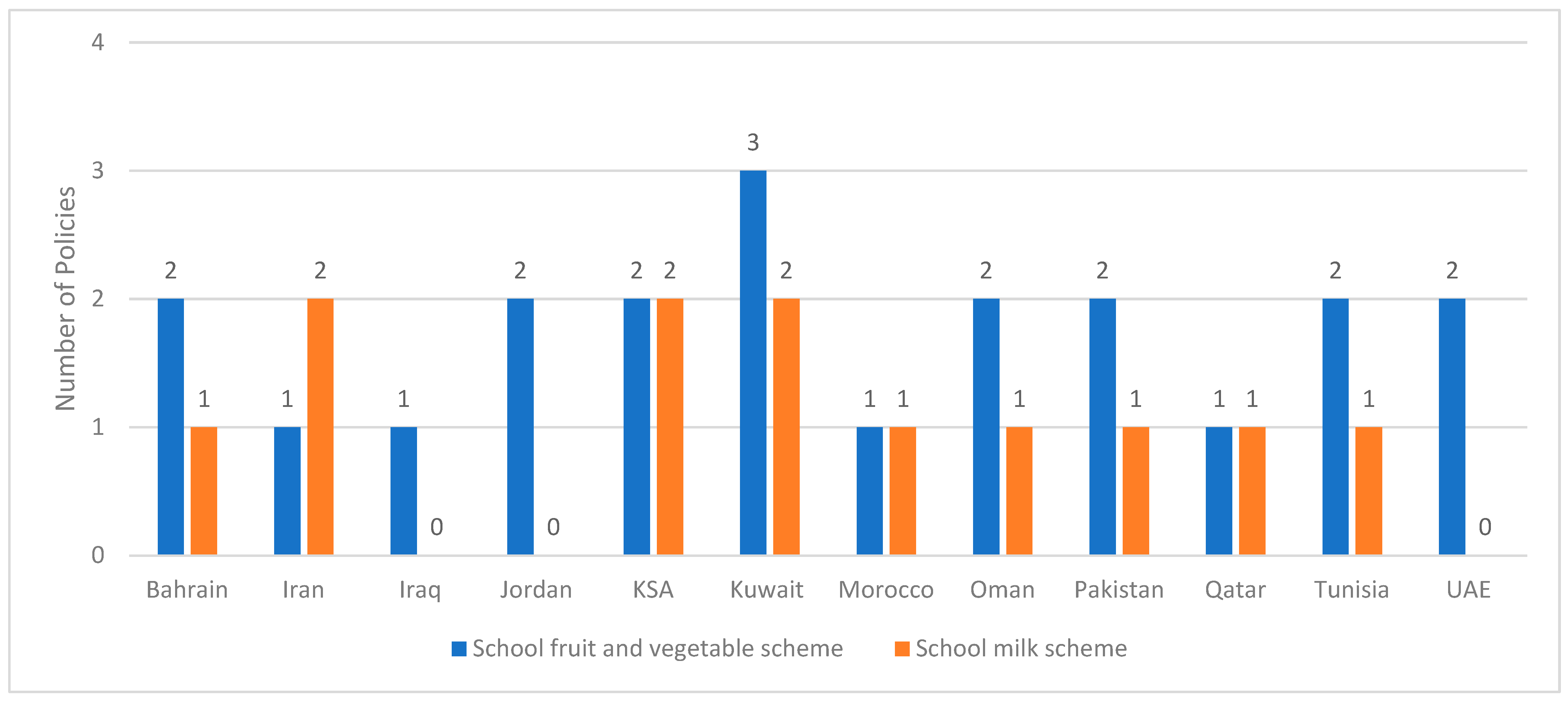
3.10. Fruit, Vegetable and Milk Schemes
3.11. Hygienic Cooking Facilities and Clean Environments in Schools
3.12. School Gardens
3.13. Monitoring and Process Evaluation
3.14. Impact Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concept 1: School | school * OR kindergarten * OR kindergarden * OR nurser * OR preschool * OR pre-school * OR “pre school *” OR pre-school * OR childcare OR “child care” OR daycare OR “day care” OR playschool * OR “senior high” OR “junior high” OR “k to 12” OR k-12 |
| Concept 2: Nutrition | nutrition OR nutritional OR food * OR diet * OR eat OR eating OR “calor * intake” OR “energy intake” OR nutrient * OR feeding OR menu OR menus OR cafeteria * OR confection?r * OR canteen * OR vegetable * OR fruit * OR breakfast OR lunch OR meal OR meals OR snack * OR cooking |
| Concept 3: Intervention | interven * OR program * OR service * OR promot * OR policy OR policies OR strateg * OR initiative * OR project * OR monitor * OR assess * OR impact * OR evaluat * OR guideline * OR practice * OR legislat * OR action * OR plan OR plans OR law * OR campaign * OR marketing OR recommend * OR curriculum OR regulat * |
| Concept 4: EMR countries | Afghan * OR Bahrain * OR Iran * OR Persia * OR Iraq * OR Jordan * OR Kuwait * OR Lebanon * OR Lebanese OR Libya * OR Oman * OR Palestin * OR Gaza * OR “West Bank” OR Qatar * OR Saudi * OR Saudi-Arabia OR Syria * OR Tunis * OR “United Arab Emirate *” OR UAE OR Djibouti * OR Egypt * OR Morocc * OR Pakistan * OR Somal * OR Sudan * OR Yemen * OR Levant * OR “East * Mediterranean” OR “Gulf countr *” OR “Gulf Cooperation Council” OR GCC OR Arab OR Arabia OR Arabs OR EMR OR “Middle East *” OR MENA OR “North * Africa *” OR “East * Africa *” OR “Near East *” OR Dhabi OR Dabi OR Dubai OR Ajman OR Fujaira * OR Sharja * OR Khaima * OR Qaiwain * OR Quwain * |
References
- Kyere, P.; Veerman, J.L.; Lee, P.; Stewart, D.E. Effectiveness of school-based nutrition interventions in sub-Saharan Africa: A systematic review. Public Health Nutr. 2020, 23, 2626–2636. [Google Scholar] [CrossRef]
- World Health Organization. Implementing School Food and Nutrition Policies: A Review of Contextual Factors; World Health Organization: Geneva, Switzerland, 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/345130/9789240035072-eng.pdf (accessed on 9 June 2023).
- World Health Organization Regional Office for the Eastern Mediterranean. About Us. Available online: https://www.emro.who.int/entity/about-us/index.html (accessed on 12 June 2023).
- Nasreddine, L.; Ayoub, J.J.; Al Jawaldeh, A. Review of the nutrition situation in the Eastern Mediterranean Region. East Mediterr. Health J. 2018, 24, 77–91. [Google Scholar] [CrossRef]
- Food and Nutrition Administration and Ministry of Health-Kuwait. Kuwait National Surveillance System (KNSS); 2013 Annual Report (Upublished Data); Food and Nutrition Administration and Ministry of Health-Kuwait: Kuwait Cty, Kuwait, 2013.
- Gharib, N.; Rasheed, P. National Nutrition Survey for School Children Age 6–18 in Bahrain (Unpublished Data); Nutrition Section, Ministry of Health: Manama, Bahrain, 2011.
- Global School-Based Student Health Survey. 2010 GSHS Fact Sheet United Arab Emirates; WHO: Geneva, Switzerland, 2010. Available online: https://www.who.int/publications/m/item/2010-gshs-factsheet-united-arab-emirates (accessed on 9 June 2023).
- World Health Organization. Global Nutrition Policy Review 2016–2017: Country Progress in Creating Enabling Policy Environments for Promoting Healthy Diets and Nutrition; World Health Organization: Geneva, Switzerland, 2018. Available online: https://www.who.int/publications/i/item/9789241514873 (accessed on 30 January 2023).
- Saavedra, J.M.; Prentice, A.M. Nutrition in school-age children: A rationale for revisiting priorities. Nutr. Rev. 2023, 81, 823–843. [Google Scholar] [CrossRef]
- Barnes, C.; McCrabb, S.; Stacey, F.; Nathan, N.; Yoong, S.L.; Grady, A.; Sutherland, R.; Hodder, R.; Innes-Hughes, C.; Davies, M. Improving implementation of school-based healthy eating and physical activity policies, practices, and programs: A systematic review. Transl. Behav. Med. 2021, 11, 1365–1410. [Google Scholar] [CrossRef]
- Wolfenden, L.; Nathan, N.K.; Sutherland, R.; Yoong, S.L.; Hodder, R.K.; Wyse, R.J.; Delaney, T.; Grady, A.; Fielding, A.; Tzelepis, F. Strategies for enhancing the implementation of school-based policies or practices targeting risk factors for chronic disease. Cochrane Database Syst. Rev. 2017, 11, CD011677. [Google Scholar] [CrossRef] [PubMed]
- Costa-Urrutia, P.; Álvarez-Fariña, R.; Abud, C.; Franco-Trecu, V.; Esparza-Romero, J.; López-Morales, C.M.; Rodríguez-Arellano, M.E.; Valle Leal, J.; Colistro, V.; Granados, J. Effect of multi-component school-based program on body mass index, cardiovascular and diabetes risks in a multi-ethnic study. BMC Pediatr. 2019, 19, 401. [Google Scholar] [CrossRef]
- Saraf, D.S.; Nongkynrih, B.; Pandav, C.S.; Gupta, S.K.; Shah, B.; Kapoor, S.K.; Krishnan, A. A systematic review of school-based interventions to prevent risk factors associated with noncommunicable diseases. Asia Pac. J. Public Health 2012, 24, 733–752. [Google Scholar] [CrossRef]
- World Food Programme. State of School Feeding Worldwide; World Food Programme: Rome, Italy, 2013; Available online: https://www.wfp.org/publications/state-school-feeding-worldwide-2013-0 (accessed on 9 June 2023).
- Nelson, M. School food cost–benefits: England. Public Health Nutr. 2013, 16, 1006–1011. [Google Scholar] [CrossRef]
- Gillies, C.; Blanchet, R.; Gokiert, R.; Farmer, A.; Thorlakson, J.; Hamonic, L.; Willows, N.D. School-based nutrition interventions for Indigenous children in Canada: A scoping review. BMC Public Health 2020, 20, 11. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Regional Office for the Eastern Mediterranean. Countries. Available online: https://www.emro.who.int/countries.html (accessed on 12 June 2023).
- World Bank. World Development Indicators. Available online: https://databank.worldbank.org/source/world-development-indicators (accessed on 13 June 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- World Bank. Worldwide Governance Indicators: Interactive Data Access. Available online: https://info.worldbank.org/governance/wgi/Home/Reports (accessed on 26 July 2023).
- World Bank. DataBank: Metadata Glossary—Government Effectiveness. Available online: https://databank.worldbank.org/metadataglossary/worldwide-governance-indicators/series/GE.EST (accessed on 28 September 2023).
- World Bank. Worldwide Governance Indicators: Documentation. Available online: https://info.worldbank.org/governance/wgi/Home/Documents (accessed on 26 July 2023).
- World Bank. Countries and Economies. Available online: https://data.worldbank.org/country (accessed on 26 July 2023).
- World Bank. DataBank: Metadata Glossary—GDP. Available online: https://databank.worldbank.org/metadataglossary/statistical-capacity-indicators/series/5.51.01.10.gdp (accessed on 26 July 2023).
- Joulaei, H.; Nwagwu, E.; Nasihatkon, A.; Azadbahkt, L.; Shenavar, R.; Keshtkar, V.; Ahmadi, S.M. To assess the effects of nutritional intervention based on advocacy approach on malnutrition status among school-aged children in Shiraz. J. Res. Med. Sci. 2013, 18, 739–745. [Google Scholar] [PubMed]
- Evans, C.E.L.; Albar, S.A.; Vargas-Garcia, E.J.; Xu, F. School-based interventions to reduce obesity risk in children in high- and middle-income countries. Adv. Food Nutr. Res. 2015, 76, 29–77. [Google Scholar] [PubMed]
- Omidvar, N.; Babashahi, M.; Abdollahi, Z.; Al-Jawaldeh, A. Enabling food environment in kindergartens and schools in iran for promoting healthy diet: Is it on the right track? Int. J. Environ. Res. Public Health 2021, 18, 4114. [Google Scholar] [CrossRef]
- Zandieh, N.; Hemami, M.R.; Darvishi, A.; Hasheminejad, S.M.; Abdollahi, Z.; Zarei, M.; Heshmat, R. Economic evaluation of a national vitamin D supplementation program among Iranian adolescents for the prevention of adulthood type 2 diabetes mellitus. BMC Complement. Med. Ther. 2022, 22, 1. [Google Scholar] [CrossRef] [PubMed]
- Zandieh, N.; Hemami, M.R.; Darvishi, A.; Hasheminejad, S.M.; Abdollahi, Z.; Zarei, M.; Heshmat, R. The cost-effectiveness analysis of a nationwide vitamin D supplementation program among Iranian adolescents for adulthood cardiovascular diseases prevention. Public Health 2021, 198, 340–347. [Google Scholar] [CrossRef]
- Banayejeddi, M.; Masudi, S.; Nouri Saeidlou, S.; Rezaigoyjeloo, F.; Babaie, F.; Abdollahi, Z.; Safaralizadeh, F. Implementation evaluation of an iron supplementation programme in high-school students: The crosswise model. Public Health Nutr. 2019, 22, 2635–2642. [Google Scholar] [CrossRef] [PubMed]
- Sartipizadeh, M.; Yazdi-Feyzabadi, V.; Sakha, M.A.; Zarrin, A.; Bazyar, M.; Moghadam, T.Z.; Zandian, H. Evaluating the health promoting schools in Iran: A cross-sectional study. Health Educ. 2021, 121, 125–139. [Google Scholar] [CrossRef]
- Sayyari, A.A.; Abdollahi, Z.; Ziaodini, H.; Olang, B.; Fallah, H.; Salehi, F.; Heidari-Beni, M.; Imanzadeh, F.; Abasalti, Z.; Fozouni, F.; et al. Methodology of the comprehensive program on prevention and control of overweight and obesity in iranian children and adolescents: The Iran-ending childhood obesity (Iran-ECHO) program. Int. J. Prev. Med. 2017, 8, 107. [Google Scholar]
- Yazdi-Feyzabadi, V.; Omidvar, N.; Mohammadi, N.K.; Nedjat, S.; Karimi-Shahanjarini, A.; Rashidian, A. Is an Iranian health promoting school status associated with improving school food environment and snacking behaviors in adolescents? Health Promot. Int. 2018, 33, 1010–1021. [Google Scholar] [CrossRef]
- Gupta, N.; Goel, K.; Shah, P.; Misra, A. Childhood obesity in developing countries: Epidemiology, determinants, and prevention. Endocr. Rev. 2012, 33, 48–70. [Google Scholar] [CrossRef]
- Kelishadi, R.; Pour, M.H.; Sarraf-Zadegan, N.; Sadry, G.H.; Ansari, R.; Alikhassy, H.; Bashardoust, N. Obesity and associated modifiable environmental factors in Iranian adolescents: Isfahan healthy Heart program—Heart health promotion from childhood. Pediatr. Int. 2003, 45, 435–442. [Google Scholar] [CrossRef]
- Sarraf-Zadegan, N.; Sadri, G.; Malek Afzali, H.; Baghaei, M.; Mohammadi Fard, N.; Shahrokhi, S.; Tolooie, H.; Poormoghaddas, M.; Sadeghi, M.; Tavassoli, A.; et al. Isfahan Healthy Heart Programme: A comprehensive integrated community-based programme for cardiovascular disease prevention and control. Design, methods and initial experience. Acta Cardiol. 2003, 58, 309–320. [Google Scholar] [CrossRef]
- Garemo, M.; Elamin, A.; Van De Venter, A. A review of the nutritional guidelines for children at nurseries and schools in Middle Eastern countries. Mediterr. J. Nutr. Metab. 2019, 12, 255–270. [Google Scholar] [CrossRef]
- Yazdi-Feyzabadi, V.; Rashidian, A.; Rarani, M.A. Socio-economic inequality in unhealthy snacks consumption among adolescent students in Iran: A concentration index decomposition analysis. Public Health Nutr. 2019, 22, 2179–2188. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for the Eastern Mediterranean. Implementing the WHO Recommendations on the Marketing of Food and Non-Alcoholic Beverages to Children in the Eastern Mediterranean Region; World Health Organization: Cairo, Egypt, 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/328213/EMROPUB_2018_2248_en.pdf?sequence=1&isAllowed=y (accessed on 28 December 2022).
- World Health Organization Regional Office for the Eastern Mediterranean. Nutrition: Success Stories. Available online: http://www.emro.who.int/nutrition/resources/success-stories.html (accessed on 27 January 2023).
- Ministry of Health and Medical Education. National Guidelines for Healthy Nutrition Canteen in Schools; Ministry of Health and Medical Education: Tehran, Iran, 2017.
- Babashahi, M.; Omidvar, N.; Joulaei, H.; Zargaraan, A.; Zayeri, F.; Veisi, E.; Doustmohammadian, A.; Kelishadi, R. Scrutinize of healthy school canteen policy in Iran’s primary schools: A mixed method study. BMC Public Health 2021, 21, 1566. [Google Scholar] [CrossRef]
- Al-Jawaldeh, A.; Hammerich, A.; Doggui, R.; Engesveen, K.; Lang, K.; McColl, K. Implementation of who recommended policies and interventions on healthy diet in the countries of the eastern mediterranean region: From policy to action. Nutrients 2020, 12, 3700. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Nutrition Policy Review: What Does It Take to Scale Up Nutrition Action? World Health Organization: Geneva, Switzerland, 2013. Available online: https://apps.who.int/iris/bitstream/handle/10665/84408/9789241505529_eng.pdf?sequence=1&isAllowed=y (accessed on 7 July 2023).
- Feyzabadi, V.Y.; Mohammadi, N.K.; Omidvar, N.; Karimi-Shahanjarini, A.; Nedjat, S.; Rashidian, A. Factors associated with unhealthy snacks consumption among adolescents in Iran’s schools. Int. J. Health Policy Manag. 2017, 6, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Kheirouri, S.; Alizadeh, M. Process evaluation of a national school-based iron supplementation program for adolescent girls in Iran. BMC Public Health 2014, 14, 959. [Google Scholar] [CrossRef]
- Khaleej Times. Food Items Banned in Dubai School Canteens [Internet]. Available online: https://www.khaleejtimes.com/news/uae-health/11-food-items-banned-in-dubai-school-canteens?_refresh=true (accessed on 1 June 2023).
- Musaiger, A.O.; Hassan, A.S.; Obeid, O. The Paradox of Nutrition-Related Diseases in the Arab Countries: The Need for Action. Int. J. Environ. Res. Public Health 2011, 8, 3637–3671. [Google Scholar] [CrossRef]
- Ministry of Education-UAE. Ministry of Education Announces a Brand New Physical and Health Education Reform in the UAE. Available online: https://www.moe.gov.ae/En/MediaCenter/News/Pages/sport.aspx (accessed on 16 March 2023).
- Habib-Mourad, C.; Hwalla, N.; Maliha, C.; Zahr, S.; Antoniades, K. Ajyal Salima a novel public–private partnership model for childhood obesity prevention in the Arab countries. Front. Public Health 2022, 10, 1012752. [Google Scholar] [CrossRef]
- Habib-Mourad, C.; Moore, H.; Zeidan, M.N.; Hwalla, N.; Summerbell, C. Health-E-PALS: Promoting healthy eating and physical activity in Lebanese school children—Intervention development. Educ. Health 2014, 32, 3–8. [Google Scholar]
- UAE Moments. The Emirates School Establishment to Launch a “Smart Canteen”. Available online: https://www.uaemoments.com/the-emirates-school-establishment-to-launch-a-%E2%80%9Csmart-canteen%E2%80%9D-513847.html (accessed on 2 June 2023).
- The National News. Smart School Canteen System to Fight Childhood Obesity in UAE. Available online: https://www.thenationalnews.com/uae/health/smart-school-canteen-system-to-fight-childhood-obesity-in-uae-1.58622 (accessed on 2 June 2023).
- Emirates News Agency-WAM. Launch of “The Fat Truth” Campaign to Fight Child Obesity. Available online: https://wam.ae/en/details/1395228347008 (accessed on 2 June 2023).
- Aldinger, C.E.; Whitman, C.V. Case Studies in Global School Health Promotion: From Research to Practice; Springer Science and Business Media: New York, NY, USA, 2009. [Google Scholar]
- Bani-Issa, W.; Dennis, C.L.; Brown, H.K.; Ibrahim, A.; Almomani, F.M.; Walton, L.M.; Al-Shujairi, A.M. The Influence of Parents and Schools on Adolescents’ Perceived Diet and Exercise Self-Efficacy: A School-Based Sample From the United Arab Emirates. J. Transcult. Nurs. 2020, 31, 479–491. [Google Scholar] [CrossRef] [PubMed]
- Emirates 24/7. New School Canteen Rules for Abu Dhabi. Available online: https://www.emirates247.com/news/emirates/new-school-canteen-rules-for-abu-dhabi-2015-09-05-1.602379 (accessed on 2 June 2023).
- The Health Authority Department of Health-Abu Dhabi. “Eat Right Get Active” Expands to Include 50 Private Schools. Available online: https://www.doh.gov.ae/en/news/eat-right-get-active-expands-to-include-50-private-schools (accessed on 23 March 2023).
- Ministry of Health and Prevention-UAE. National Action Plan in Nutrition 2017–2021; Ministry of Health and Prevention-UAE: Dubai, United Arab Emirates, 2017. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/ARE%202017%20National%20Strategy%20Plan%20in%20Nutrition.pdf (accessed on 17 January 2023).
- Ministry of Health-UAE. Healthy Recipes for School Lunch Bag. MA’KOM for a Balanced Diet, 1st ed.; Health Education and Promotion Department: Dubai, United Arab Emirates, 2019.
- Ahmed, A. Junk Food Banned from Every Dubai School Canteen, The National [Internet]. Available online: https://www.thenationalnews.com/uae/junk-food-banned-from-every-dubai-school-canteen-1.365770 (accessed on 1 June 2023).
- Abu Dhabi Education Council. ADEC Public Schools (P-12) Policy Manual 2014. Available online: https://docplayer.net/25406908-Adec-public-schools-p-12-policy-manual-september-2014.html (accessed on 17 March 2023).
- Algurg, R.S.; Mahfouz, N.H.A.; Otaki, F. Interviews with key informants to explore school nutrition programs: A case-study in dubai. IA13-COVER 2020, 106–116. [Google Scholar]
- Algurg, R.; Mahfouz, N.A.; Otaki, F.; Alameddine, M. Towards the Upscaling of School Nutrition Programs in Dubai: An Exploratory Study. Front. Public Health 2021, 10, 1038726. [Google Scholar] [CrossRef]
- Abdullatif, M.; AlAbady, K.; Altheeb, A.; Rishmawi, F.; Jaradat, H.; Farooq, S. Prevalence of Overweight, Obesity, and Dietary Behaviors among Adolescents in Dubai Schools: A Complex Design Survey 2019. Dubai Med. J. 2022, 5, 1–9. [Google Scholar] [CrossRef]
- Public Health Directorate Bahrain. Annual Report; Public Health Directorate: Manama, Bahrain, 2014. Available online: https://www.moh.gov.bh/Content/Files/Publications/X_635906124344978750.pdf (accessed on 14 December 2022).
- Ministry of Health-Bahrain. Bahrain’s Health Agenda. Health Improvement Strategy; Directorate of Health Planning: Manama, Bahrain, 2012. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/BHR%202012%20%20Health%20Improvement%20Strategy.pdf (accessed on 14 December 2022).
- AlMulla AlHarmasAlHajeri, M.; Al Thukair, L.A.A.A.; Sarhan, N. Bahrain: National Comprehensive School Health Program, Health-Promoting Schools. In Case Studies in Global School Health Promotion: From Research to Practice; Springer: New York, NY, USA, 2009; pp. 239–249. [Google Scholar]
- Ministry of Health-Bahrain. MOH Organize a Workshop for School Canteen Operators in Collaboration with School Health Section at the Ministry of Education. Available online: https://www.moh.gov.bh/News/Details/3453?lang=en (accessed on 8 February 2023).
- Ministry of Education-Kingdom of Saudi Arabia. Health Requirements in the Provision of School Feeding Services. 2022. Available online: https://moe.gov.sa/ar/education/generaleducation/Documents/%D8%AE%D8%AF%D9%85%D8%A7%D8%AA_%D8%A7%D9%84%D8%AA%D8%BA%D8%B0%D9%8A%D8%A9.pdf (accessed on 20 February 2023).
- Al-Eid, A.J.; Al-Ahmed, Z.A.; Al-Omary, S.A.; Al-Harbi, S.M. RASHAKA program: A collaborative initiative between Ministry of Health and Ministry of Education to control childhood obesity in Saudi Arabia. Saudi J. Obes. 2017, 5, 22–27. [Google Scholar] [CrossRef]
- Ministry of Health-Kingdom of Saudi Arabia. School-Based Obesity Control (Rashaqa). Available online: https://www.moh.gov.sa/en/Ministry/Projects/agility/Pages/default.aspx (accessed on 16 February 2023).
- Ministry of Health-KSA. Obesity Control Program; General Department for the Control of Genetic and Chronic Diseases: Riyadh, Saudi Arabia, 2017. Available online: https://extranet.who.int/nutrition/gina/en/node/39427 (accessed on 28 December 2022).
- Al-Shikheid, W.; Mistareehi, H. The extent of the national interactive curriculum contributes to health awareness concepts development among Public kindergarten children from female teachers’ perspective in of Zarqa governorate. Najah Natl. Univ. 2022, 36, 1703–1740. [Google Scholar] [CrossRef]
- Ministry of Health-Jordan; WHO. Nutrition in Jordan Update and Plan of Action. 2006. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/aNutrition%20in%20Jordan-Policy.pdf (accessed on 28 December 2022).
- Ministry of Education-Jordan. Department of School Nutrition and Health. Available online: https://moe.gov.jo/node/21657 (accessed on 16 February 2023).
- Ministry of Education-Jordan. Health Requirements for School Canteens and Foods Allowed and Prohibited to Be Sold for the Year 2012; 2012. Available online: https://extranet.who.int/nutrition/gina/en/node/66515 (accessed on 28 December 2022).
- Jamaluddine, Z.; Akik, C.; Safadi, G.; Abou Fakher, S.; El-Helou, N.; Moussa, S.; Anid, D.; Ghattas, H. Does a school snack make a difference? An evaluation of the World Food Programme emergency school feeding programme in Lebanon among Lebanese and Syrian refugee children. Public Health Nutr. 2022, 25, 1678–1690. [Google Scholar] [CrossRef]
- Ministry of Education and Higher Education-Lebanon. School Health Strategy. 2009. Available online: https://www.mehe.gov.lb/ar/Projects/%D8%A7%D9%84%D8%AA%D8%B9%D9%84%D9%8A%D9%85%20%D8%A7%D9%84%D8%B9%D8%A7%D9%85/School%20Health%20Strategy.pdf (accessed on 16 February 2023).
- El Halabi Ezzeddine, S.; Salameh, P. Incorporating an Innovative Health Promoting Model Into Lebanese Public Schools: Impact on Adolescents’ Dietary and Physical Activity Practices—Comparison of HPS With Other Public and Private Schools in Lebanon. Glob. J. Health Educ. Promot. 2016, 17, 53–87. [Google Scholar] [CrossRef]
- Ministry of Public Health-Lebanon. The MOH Strategic Plan. 2007. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/LBN%202007%20The%20MOH%20Strategy%20Plan%20.pdf (accessed on 29 December 2022).
- Behbehani, K. Kuwait national programme for healthy living: First 5-year plan (2013–2017). Med. Princ. Pract. 2014, 23, 32–42. [Google Scholar] [CrossRef]
- Ministry of Health-Kuwait; Gulf Health Council; United Nations Development Programme; World Health Organization; Secretariat of the UN Inter-Agency Task Force on NCDS. The Case for Investment in Prevention and Control of Non-Communicable Diseases in Kuwait; Ministry of Health: Kuwait City, Kuwait, 2021.
- World Health Organization Regional Office for the Eastern Mediterranean. Kuwait Health Profile 2015; World Health Organization Regional Office for the Eastern Mediterranean: Cairo, Egypt, 2016. Available online: https://apps.who.int/iris/bitstream/handle/10665/253770/EMROPUB_2016_EN_19271.pdf?sequence=1&isAllowed=y (accessed on 26 January 2023).
- Ministry of Education and Technical Education-Egypt. The Ministers of “Health” and “Education” Are Discussing Ways of Cooperation to Provide Healthy Meals for School Students. Available online: https://moe.gov.eg/en/what-s-on/news/the-ministers-of-health-and-education/ (accessed on 16 February 2023).
- World Food Programme. WFP Egypt Country Brief, November 2022. 2022. Available online: https://reliefweb.int/report/egypt/wfp-egypt-country-brief-november-2022 (accessed on 10 January 2023).
- Metwally, A.M.; El-Sonbaty, M.M.; El Etreby, L.A.; Salah El-Din, E.M.; Abdel Hamid, N.; Hussien, H.A.; Hassanin, A.M.; Monir, Z.M. Impact of National Egyptian school feeding program on growth, development, and school achievement of school children. World J. Pediatr. 2020, 16, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Salah, E.M.; Khalifa, A.G.; Metwally, A.M.; Hamid, N.A.; Hussien, H.A.; Moneer, Z.M. The impact of school snacks on cognitive function of primary school children in Egypt. J. Appl. Sci. Res. 2012, 8, 5639–5650. [Google Scholar]
- World Food Programme. Annual Report—World Food Programme 2003; World Food Programme: Rome, Italy, 2004; Available online: https://www.cabdirect.org/cabdirect/abstract/20043140475 (accessed on 3 March 2023).
- Hanel, T.; Miller, B.; Aboul-Enein, B.; Benajiba, N.; Kruk, J. Farm-to-school nutrition programs with special reference to Egypt and Morocco. N. Afr. J. Food Nutr. Res. 2021, 5, 100–104. [Google Scholar] [CrossRef]
- World Food Programme. Capacity Development and Support for the National School Feeding Programme. Standard Project Report. 2016. Available online: https://docs.wfp.org/api/documents/39eb14d12a174f2a996ebb37ce2b56c9/download/ (accessed on 13 March 2023).
- Amahmid, O.; El Guamri, Y.; Rakibi, Y.; Yazidi, M.; Razoki, B.; Rassou, K.K.; El Boukaoui, S.; Izerg, O.; Belghyti, D. Nutrition education in school curriculum: Impact on adolescents’ attitudes and dietary behaviours. Int. J. Health Promot. Educ. 2020, 58, 242–258. [Google Scholar] [CrossRef]
- Akeed, F. Tackling Health Education in the Textbooks of Life and Earth Sciences at the Lower Secondary Education in the Kingdom of Morocco. J.Al-Quds Open Univ. Educ. Psychol. Res. Stud. 2015, 3, 271–298. [Google Scholar]
- Ministry of Health-Morocco; UNICEF. La Stratégie Nationale de la Nutrition. 2011. Available online: https://extranet.who.int/nutrition/gina/en/node/17819 (accessed on 29 December 2022).
- Ministry of National Education-Morocco. Nutrition Education. Available online: https://www.men.gov.ma/Fr/Pages/Edunutri.aspx (accessed on 20 February 2023).
- Ministry of Education and Higher Education-Qatar. Guidance for Supervisors of School Canteens for the Academic Year 2018–2019; Health and Safety Department: Doha, Qatar, 2018. Available online: https://www.edu.gov.qa/ar/Deputy/sharedservicesaffairs/healthandsafety-dept/Documents/FilesLibrary/2-GuidetoSchoolCafeteriaSupervisors.pdf (accessed on 16 January 2023).
- Choudhury, S.; Omar, O.; Arora, T.; Rifai, N.; Chagoury, O. Qatar obesity reduction study (QORS): Report on a pilot school-based nutrition education campaign in Qatar. J. Child. Obes. S 2018, 2, 007. [Google Scholar]
- Ministry of Education and Higher Education-Qatar. Food Safety and Health Guide; Health and Safety Department: Doha, Qatar, 2017. Available online: https://www.edu.gov.qa/ar/Deputy/sharedservicesaffairs/healthandsafety-dept/Documents/FilesLibrary/8-FoodSafetyandHealthGuide.pdf (accessed on 16 January 2023).
- Ministry of Public Health-Qatar. National Nutrition and Physical Activity Action Plan. 2011. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/QAT%202011%20National%20Nutrition%20and%20Physical%20Activity%20Action%20Plan.pdf (accessed on 16 January 2023).
- Bajraktarevic, S.; Qadi, K.; Jouda, A.; Awadallah, Y.; Abueita, R. Improving the nutritional well-being of school-age children through the nutrition-friendly schools initiative (NFSI) in the State of Palestine. Field Exch.-Emerg. Nutr. Netw. 2021, 66, 47–50. [Google Scholar]
- World Health Organization. Nutrition Action in Schools: A Review of Evidence Related to the Nutrition-Friendly Schools Initiative; World Health Organization: Geneva, Switzerland, 2021. Available online: https://www.who.int/publications/i/item/9789241516969 (accessed on 31 May 2023).
- Ministry of Education and Higher Education-Palestine. General Directorate of School Health. Available online: https://www.mohe.ps/home/%D8%A7%D9%84%D8%A5%D8%AF%D8%A7%D8%B1%D8%A9-%D8%A7%D9%84%D8%B9%D8%A7%D9%85%D8%A9-%D9%84%D9%84%D8%B5%D8%AD%D8%A9-%D8%A7%D9%84%D9%85%D8%AF%D8%B1%D8%B3%D9%8A%D8%A9/ (accessed on 23 February 2023).
- World Health Organization. Health-Promoting Schools Initiative in Oman. A WHO Case Study in Intersectoral Action; World Health Organization: Cairo, Egypt, 2013. Available online: https://applications.emro.who.int/dsaf/EMROPUB_2013_EN_1587.pdf (accessed on 31 May 2023).
- Hrairi, S.; Berger, D. Nutrition Education in Tunisian schools: Analysis of practices reported by primary teachers. Quest. Vives-Rech. En Educ. 2017, 27. [Google Scholar] [CrossRef]
- Ministry of Health-Republic of Tunisia. National Multisectoral Strategy for the Prevention and Control of Non-Communicable Diseases (NCD) 2018–2025. 2018. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/TUN%202018%20Strat%C3%A9gie%20Nationale%20MNT.pdf (accessed on 17 January 2023).
- Ministry of Health-Republic of Tunisia. Obesity Prevention and Control Strategy. 2012. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/TUN_2014_SPLO.pdf (accessed on 17 January 2023).
- Khan, K.S.; Ajmal, A. Women’s Empowerment and Its Challenges: Review of a Multi-Partner National Project to Reduce Malnutrition in Rural Girls in Pakistan; World Health Organization: Geneva, Switzerland, 2011; pp. 117–128.
- Badruddin, S.H.; Agha, A.; Peermohamed, H.; Rafique, G.; Khan, K.S.; Pappas, G. Tawana project-school nutrition program in Pakistan—Its success, bottlenecks and lessons learned. Asia Pac. J. Clin. Nutr. 2008, 17, 357–360. [Google Scholar]
- Government of Balochistan. Balochistan—An Inter-Sectoral Nutrition Strategy; Planning and Development Department: Balochistan, Pakistan, 2014. Available online: https://extranet.who.int/nutrition/gina/en/node/39754 (accessed on 10 January 2023).
- Government of Khyber Pakhtunkhwa. Khyber Pakhtunkhwa Multi-Sectoral Integrated Nutrition Strategy; Planning and Development Department: Khyber Paktunknwa, Pakistan, 2014. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/PAK_2014_Khyber%20Pakhtunkhwa%20Integrated%20Nutrition%20Strategy.pdf (accessed on 16 January 2023).
- Hees, J.V.; Sankei, K. Home Fortification in School Feeding; Sight and Life: Basel, Switzerland, 2013; pp. 39–41. [Google Scholar]
- Ministry of Public Health-Afghanistan. National Public Nutrition Policy and Strategy 2015–2020. 2015. Available online: https://extranet.who.int/ncdccs/Data/AFG_B14_Public_Nutrition_Policy_Strategy_2015.pdf (accessed on 13 December 2022).
- Ministry of Public Health-Afghanistan. National Public Nutrition Policy and Strategy 2009–2013. 2009. Available online: https://extranet.who.int/nutrition/gina/en/node/17851 (accessed on 13 December 2022).
- Ministry of Public Health-Islamic Republic of Afghanistan. National Public Nutrition Policy & Strategy 1388–1392 (2009–2013); Ministry of Public Health: Kabul, Afghanistan, 2010. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/AFG%202009%20National%20Public%20Nutrition%20Policy%20and%20Strategy.pdf (accessed on 1 March 2023).
- Ministry of Health-Iraq. National Nutrition Strategy 2012–2021. 2012. Available online: https://extranet.who.int/nutrition/gina/en/node/8387 (accessed on 28 December 2022).
- Supreme Committee for the Prevention and Control of Non-communicable Diseases; Ministry of Health-Iraq. The National Strategy for Prevention and Control of Noncommunicable Diseases 2013. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/IRQ_The%20National%20Strategy%20for%20Prevention%20and%20Control%20of%20Noncommunicable%20Diseases-2013.pdf (accessed on 28 December 2022).
- Government of Somalia. Somali National Micronutrient Deficiency Control Strategy 2014–2016. 2014. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/SOM_MN%20Strategy%20-%202014-2016.pdf (accessed on 17 January 2023).
- World Health Organization; UNICEF; WFP; FAO; FSNAU. Somali Nutrition Strategy 2011–2013. 2010. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/SOM%202010%20Nutrition%20Strategy.pdf (accessed on 17 January 2023).
- Federal Ministry of Health-Republic of Sudan. National Nutrition Policy and Key Strategies; Maternal and Child Health Directorate: Khartoum, Sudan, 2009. Available online: http://www.fmoh.gov.sd/Health-policy/nationalnutritionpolicy.pdf (accessed on 17 January 2023).
- Federal Ministry of Health-Republic of Sudan. National Nutrition Strategy & Key Strategies (2008–2012); Maternal and Child Health Directorate: Khartoum, Sudan, 2008. Available online: https://extranet.who.int/nutrition/gina/sites/default/filesstore/SDN%202008_National%20Nutrition%20Policy.pdf (accessed on 17 January 2023).
- World Food Programme. The State of School Feeding Worldwide 2022; World Food Programme: Rome, Italy, 2022; Available online: https://www.wfp.org/publications/state-school-feeding-worldwide-2022 (accessed on 1 June 2023).
- UNICEF. UNICEF Annual Report 2013—Djibouti. 2013. Available online: http://www.unicef.org/about/annualreport/files/Djibouti_COAR_2013.pdf (accessed on 25 July 2023).
- Supreme Committee for the Prevention and Control of Non-communicable Diseases; Ministry of Health-Iraq. National Strategy for the Prevention and Control of Non-Communicable Diseases 2018–2022; Ministry of Health: Baghdad, Iraq, 2018. Available online: https://extranet.who.int/nutrition/gina/en/node/40323 (accessed on 27 December 2022).
- Habib-Mourad, C.; Ghandour, L.A.; Moore, H.J.; Nabhani-Zeidan, M.; Adetayo, K.; Hwalla, N.; Summerbell, C. Promoting healthy eating and physical activity among school children: Findings from Health-E-PALS, the first pilot intervention from Lebanon. BMC Public Health 2014, 14, 940. [Google Scholar] [CrossRef]
- Editorial. East Mediterr. Health J. 2019, 25, 223–224. [CrossRef] [PubMed]
- Khatib, I.M.; Hijazi, S.S. Micronutrient deficiencies among children may be endemic in underprivileged areas in Jordan. Jordan Med. J. 2009, 43, 324–332. [Google Scholar]
- Aldubayan, K.; Murimi, M. Compliance with school nutrition policy in saudi arabia: A quantitative study. East Mediterr. Health J. 2019, 25, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Gordon, K.; Caine-Bish, N.; Yahya, L. P46 Nutritional Composition of Breakfast Meals Served in All-Girl Intermediate and Secondary Public Schools in Mecca, Saudi Arabia. J. Nutr. Educ. Behav. 2019, 51, S53. [Google Scholar]
- Ghammam, R.; Maatoug, J.; Zammit, N.; Kebaili, R.; Boughammoura, L.; Al’Absi, M.; Lando, H.; Ghannem, H. Long term effect of a school based intervention to prevent chronic diseases in Tunisia, 2009–2015. Afr. Health Sci. 2017, 17, 1137–1148. [Google Scholar] [CrossRef]
- Nasreddine, L.M.; Kassis, A.N.; Ayoub, J.J.; Naja, F.A.; Hwalla, N.C. Nutritional status and dietary intakes of children amid the nutrition transition: The case of the Eastern Mediterranean Region. Nutr. Res. 2018, 57, 12–27. [Google Scholar] [CrossRef] [PubMed]
- Al-Jawaldeh, A.; Taktouk, M.; Nasreddine, L. Food consumption patterns and nutrient intakes of children and adolescents in the Eastern Mediterranean Region: A call for policy action. Nutrients 2020, 12, 3345. [Google Scholar] [CrossRef]
- Halleröd, B.; Rothstein, B.; Daoud, A.; Nandy, S. Bad governance and poor children: A comparative analysis of government efficiency and severe child deprivation in 68 low-and middle-income countries. World Dev. 2013, 48, 19–31. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; McKee, M. A comparative analysis of health policy performance in 43 European countries. Eur. J. Public Health 2013, 23, 195–201. [Google Scholar] [CrossRef]
- Klomp, J.; De Haan, J. Effects of governance on health: A cross-national analysis of 101 countries. Kyklos 2008, 61, 599–614. [Google Scholar] [CrossRef]
- Ministry of Public Health and Population and Central Statistical Organization. Yemen National Health and Demographic Survey 2013. Preliminary Report. Sana’a. Yemen; The Pan Arab Program for Family Health (PAPFAM): Cairo, Egypt, 2014. Available online: http://dhsprogram.com/pubs/pdf/PR50/PR50.pdf (accessed on 25 July 2023).
- Ministry of Public Health and UNICEF. National Nutrition Survey Afghanistan (2013): Survey Report; Ministry of Public Health: Kabul, Afghanistan, 2013. Available online: https://reliefweb.int/report/afghanistan/national-nutrition-survey-afghanistan-2013 (accessed on 25 July 2023).
- Hwalla, N.; Al Dhaheri, A.S.; Radwan, H.; Alfawaz, H.A.; Fouda, M.A.; Al-Daghri, N.M.; Zaghloul, S.; Blumberg, J.B. The prevalence of micronutrient deficiencies and inadequacies in the Middle East and approaches to interventions. Nutrients 2017, 9, 229. [Google Scholar] [CrossRef] [PubMed]
- Kassim, I.; Seal, A.; Moloney, G. National Micronutrient and Anthropometric Survey, Somalia 2009; Food Security and Nutrition Analysis Unit (FSNAU): Somalia, 2010; Available online: https://fsnau.org/downloads/Somalia-National-Micronutrient-Study.pdf (accessed on 25 July 2023).
- Ministry of Health-Syria and UNICEF. Rapid Nutrition Assessment (RNA). Final RNA Report; Central Bureau of Statistics: Damascus, Syria, 2014.
- National Center for Infectious and Chronic Disease Control [Jamahiriya] and Pan-Arab Project for Family Health. National Libyan Family Health Survey. PAPFAM Surveys; The League of Arab States: Cairo, Egypt, 2008. [Google Scholar]
- Federal Ministry of Health and Central Bureau of Statistics. Sudan Household Health Survey—Round 2. National Report. 2010; Federal Ministry of Health and Central Bureau of Statistics: Khartoum, Sudan, 2012; Available online: https://mics-surveys-prod.s3.amazonaws.com/MICS4/Middle%20East%20and%20North%20Africa/Sudan/2010/Final/Sudan%202010%20MICS_English.pdf (accessed on 25 July 2023).
- World Health Organization. Global Action Plan for the Prevention and Control of NCDs 2013–2020; World Health Organization: Geneva, Switzerland, 2013. Available online: https://www.who.int/publications/i/item/9789241506236 (accessed on 26 July 2023).
- World Health Organization. Report of the Commission on Ending Childhood Obesity; World Health Organization: Geneva, Switzerland, 2016. Available online: http://apps.who.int/iris/bitstream/handle/10665/204176/9789241510066_eng.pdf?sequence=1 (accessed on 26 July 2023).
- Strauss, R. Childhood obesity. Curr. Probl. Pediatr. 1999, 29, 5–29. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Ye, D.; Li, Y.; Huang, Y.; Li, L.; Gao, Y.; Wang, S. Evaluation of a kindergarten-based nutrition education intervention for pre-school children in China. Public Health Nutr. 2010, 13, 253–260. [Google Scholar] [CrossRef]
- Longbottom, P.; Wrieden, W.; Pine, C. Is there a relationship between the food intakes of Scottish 5½–8½-year-olds and those of their mothers? J. Hum. Nutr. Diet 2002, 15, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Hart, K.; Herriot, A.; Bishop, J.; Truby, H. Promoting healthy diet and exercise patterns amongst primary school children: A qualitative investigation of parental perspectives. J. Hum. Nutr. Diet 2003, 16, 89–96. [Google Scholar] [CrossRef]
- Global Child Nutrition Foundation. Are School Food Programs Good Investments? A Brief History of US Government Support for Domestic and International School Meal Programs and a Summary of Evidence Regarding Their Effectiveness. 2017. Available online: https://gcnf.org/wp-content/uploads/2017/09/Evidence-based-Support-for-School-Meal-Programs-GCNF-August-15-2017.pdf (accessed on 26 July 2023).
- Al-Daghri, N.M.; Aljohani, N.; Al-Attas, O.S.; Krishnaswamy, S.; Alfawaz, H.; Al-Ajlan, A.; Alokail, M.S. Dairy products consumption and serum 25-hydroxyvitamin D level in Saudi children and adults. Int. J. Clin. Exp. Pathol. 2015, 8, 8480–8486. [Google Scholar] [PubMed]
- Dawodu, A.; Agarwal, M.; Sankarankutty, M.; Hardy, D.; Kochiyil, J.; Badrinath, P. Higher prevalence of vitamin D deficiency in mothers of rachitic than nonrachitic children. J. Pediatr. 2005, 147, 109–111. [Google Scholar] [CrossRef]
- Al-Jurayyan, N.A.; El-Desouki, M.E.; Al-Herbish, A.S.; Al-Mazyad, A.S.; Al-Qhtani, M.M. Nutritional rickets and osteomalacia in school children and adolescents. Saudi Med. J. 2002, 23, 182–185. [Google Scholar]
- Muhairi, S.J.; Mehairi, A.E.; Khouri, A.A.; Naqbi, M.M.; Maskari, F.A.; Kaabi, J.A.; Al Dhaheri, A.S.; Nagelkerke, N.; Shah, S.M. Vitamin D deficiency among healthy adolescents in al ain, united arab emirates. BMC Public Health 2013, 13, 33. [Google Scholar] [CrossRef]
- Miller, C.J.; Dunn, E.V.; Berg, B.; Abdouni, S.F. A hematological survey of preschool children of the United Arab Emirates. Saudi Med. J. 2003, 24, 609–613. [Google Scholar]
- Abalkhail, B.; Shawky, S. Prevalence of daily breakfast intake, iron deficiency anaemia and awareness of being anaemic among Saudi school students. Int. J. Food Sci. Nutr. 2002, 53, 519–528. [Google Scholar] [CrossRef]
- Alquaiz, A.-J.M.; Khoja, T.A.; Alsharif, A.; Kazi, A.; Mohamed, A.G.; Al Mane, H.; Aldiris, A.; Shaikh, S.A. Prevalence and correlates of anaemia in adolescents in Riyadh city, Kingdom of Saudi Arabia. Public Health Nutr. 2015, 18, 3192–3200. [Google Scholar] [CrossRef]
- Al Ghwass, M.M.; Halawa, E.F.; Sabry, S.M.; Ahmed, D. Iron deficiency anemia in an Egyptian pediatric population: A cross-sectional study. Ann. Afr. Med. 2015, 14, 25. [Google Scholar]
- Aguayo, V.M.; Menon, P. Stop stunting: Improving child feeding, women’s nutrition and household sanitation in South Asia. Matern. Child. Nutr. 2016, 12, 3–11. [Google Scholar] [CrossRef]
- Lakshman, R.R.; Sharp, S.J.; Ong, K.K.; Forouhi, N.G. A novel school-based intervention to improve nutrition knowledge in children: Cluster randomised controlled trial. BMC Public Health 2010, 10, 23. [Google Scholar] [CrossRef]
- Sharrif, Z.; Bukhari, S.; Othman, N.; Hashim, N.; Ismail, M.; Jamil, Z.; Kasim, S.; Paim, L.; Samah, B.; Hussein, Z. Nutrition education intervention improves nutrition knowledge, attitude and practices of primary school children: A pilot study. Int. Electron. J. Healthy Educ. 2008, 11, 119–244. [Google Scholar]
- Kupolati, M.D.; MacIntyre, U.E.; Gericke, G.J.; Becker, P. A contextual nutrition education program improves nutrition knowledge and attitudes of South African teachers and learners. Front. Public Health 2019, 7, 258. [Google Scholar] [CrossRef]
- Elmas, C.; Arslan, P. Effect of nutrition education received by teachers on primary school students’ nutrition knowledge. Nutr. Res. Pract. 2020, 14, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Association, A.H.; Gidding, S.S.; Dennison, B.A.; Birch, L.L.; Daniels, S.R.; Gilman, M.W.; Lichtenstein, A.H.; Rattay, K.T.; Steinberger, J.; Stettler, N. Dietary recommendations for children and adolescents: A guide for practitioners. Pediatrics 2006, 117, 544–559. [Google Scholar] [CrossRef] [PubMed]
- US Department of Agriculture and US Department of Health and Human Services. Dietary Guidelines for Americans 2020–2025. 2020. Available online: https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.pdf (accessed on 1 August 2023).
- Velazquez, C.E.; Black, J.L.; Potvin Kent, M. Food and beverage marketing in schools: A review of the evidence. Int. J. Environ. Res. Public Health 2017, 14, 1054. [Google Scholar] [CrossRef]
- Signal, L.N.; Stanley, J.; Smith, M.; Barr, M.; Chambers, T.J.; Zhou, J.; Duane, A.; Gurrin, C.; Smeaton, A.F.; McKerchar, C. Children’s everyday exposure to food marketing: An objective analysis using wearable cameras. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 137. [Google Scholar] [CrossRef] [PubMed]
- Dalton, M.A.; Longacre, M.R.; Drake, K.M.; Cleveland, L.P.; Harris, J.L.; Hendricks, K.; Titus, L.J. Child-targeted fast-food television advertising exposure is linked with fast-food intake among pre-school children. Public Health Nutr. 2017, 20, 1548–1556. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization and UNICEF. Taking Action to Protect Children from the Harmful Impact of Food Marketing: A Child Rights-Based Approach; World Health Organization and UNICEF: Geneva, Switzerland, 2023. Available online: https://www.who.int/publications/i/item/9789240047518 (accessed on 1 August 2023).
- Bevans, K.B.; Sanchez, B.; Teneralli, R.; Forrest, C.B. Children’s eating behavior: The importance of nutrition standards for foods in schools. J. Sch. Health 2011, 81, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Micha, R.; Karageorgou, D.; Bakogianni, I.; Trichia, E.; Whitsel, L.P.; Story, M.; Penalvo, J.L.; Mozaffarian, D. Effectiveness of school food environment policies on children’s dietary behaviors: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0194555. [Google Scholar] [CrossRef]
- Murimi, M.W.; Kanyi, M.; Mupfudze, T.; Amin, M.R.; Mbogori, T.; Aldubayan, K. Factors influencing efficacy of nutrition education interventions: A systematic review. J. Nutr. Educ. Behav. 2017, 49, 142–165.e1. [Google Scholar] [CrossRef]






| Government Effectiveness | 0.48 | 1.44 | 2.88 | 3.37 | 5.29 | 5.77 | 10.1 | 10.58 | 18.27 | 19.71 | 22.12 | 35.58 | 37.5 | 45.67 | 48.08 | 50.96 | 51.44 | 59.62 | 68.75 | 74.04 | 82.69 | 89.9 |
| Country * | YEM | SOM | SYR | LBY | SDN | AFG | IRQ | LBN | IRN | DJI | PSE | EGY | PAK | TUN | OMN | MOR | KWT | JOR | KSA | BHR | QAT | UAE |
| Take-home rations | ||||||||||||||||||||||
| School gardens | ||||||||||||||||||||||
| Bans or standards on vending machines | ||||||||||||||||||||||
| School milk scheme | ||||||||||||||||||||||
| Micronutrient supplementation (e.g., iron, vitamin a) | ||||||||||||||||||||||
| Standards for marketing of food and non-alcoholic beverage | ||||||||||||||||||||||
| Hygienic cooking facilities and clean eating environment in schools | ||||||||||||||||||||||
| School fruit and vegetable scheme | ||||||||||||||||||||||
| Training of school staff (teachers, canteen staff, school health providers etc.) | ||||||||||||||||||||||
| School canteens or standards or rules for foods and beverages available in schools | ||||||||||||||||||||||
| Extracurricular nutrition education | ||||||||||||||||||||||
| Nutrition education included in school curriculum | ||||||||||||||||||||||
| Provision of school meals, school feeding program |
| Number of Children Receiving School Feeding | Estimated Coverage (%) | Number of Children Receiving School Feeding | Estimated Coverage (%) | Number of Children Receiving School Feeding | Estimated Coverage (%) | |
|---|---|---|---|---|---|---|
| 2022 | 2020 | 2013 | ||||
| Afghanistan | 1,341,812 | - | 1,341,812 | - | 1,841,000 | 35 |
| Bahrain | 96,300 | - | 96,300 | - | 59,000 | - |
| Djibouti | 19,590 | 28 | 19,590 | 29 | 28,000 | 43 |
| Egypt | 11,200,000 | 73 | 11,200,000 | 77 | 7,002,000 | 64 |
| Iran | 2812 | - | 2812 | - | 3000 | - |
| Iraq | 350,000 | - | 633,351 | - | 555,000 | 11 |
| Jordan | 419,327 | 37 | 419,327 | 37 | 115,000 | - |
| KSA | 2,789,606 | - | 2,789,606 | - | 2,136,000 | - |
| Kuwait | 236,744 | - | 236,744 | - | 137,000 | - |
| Lebanon | 31,929 | 6 | 31,929 | 6 | 297,000 | - |
| Libya | 18,000 | - | 20,754 | - | - | - |
| Morocco | 1,267,109 | 28 | 1,267,109 | 29 | 1,423,000 | 31 |
| Palestine | 65,000 | 13 | 65,000 | 13 | 389,000 | 97 |
| Pakistan | 10,400,000 | - | 10,400,000 | - | 2,078,000 | 11 |
| Oman | - | - | - | - | - | - |
| Qatar | 130,152 | - | 130,152 | - | 57,000 | - |
| Somalia | 170,796 | - | 164,708 | - | 139,000 | 30 |
| Sudan | 1,890,277 | 39 | 1,361,789 | 27 | 1,630,000 | 34 |
| Syria | 651,728 | 42 | 1,308,648 | 63 | 46,000 | 2 |
| Tunisia | 350,000 | 20 | 360,000 | 22 | 240,000 | - |
| UAE | 288,795 | 18 | 821,236 | 85 | - | - |
| Yemen | 680,000 | 17 | 680,000 | 17 | 65,000 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Jawaldeh, A.; Matbouli, D.; Diab, S.; Taktouk, M.; Hojeij, L.; Naalbandian, S.; Nasreddine, L. School-Based Nutrition Programs in the Eastern Mediterranean Region: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 7047. https://doi.org/10.3390/ijerph20227047
Al-Jawaldeh A, Matbouli D, Diab S, Taktouk M, Hojeij L, Naalbandian S, Nasreddine L. School-Based Nutrition Programs in the Eastern Mediterranean Region: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(22):7047. https://doi.org/10.3390/ijerph20227047
Chicago/Turabian StyleAl-Jawaldeh, Ayoub, Dana Matbouli, Sarah Diab, Mandy Taktouk, Leila Hojeij, Sally Naalbandian, and Lara Nasreddine. 2023. "School-Based Nutrition Programs in the Eastern Mediterranean Region: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 22: 7047. https://doi.org/10.3390/ijerph20227047