
Precursors of Prenatal Attachment and Anxiety during Pregnancy in Women Who Procreate Naturally and Pregnant Women following Assisted Reproduction Technology
 , ,
, ,
Abstract
:1. Introduction
2. Prenatal Attachment and Maternal–Fetal Representation during Vitro Fertilization Path
3. Research Goals and Hypothesis
4. Research Method
4.1. Participants and Procedures
- (a)
- Fifty pregnant women (control group), who conceived naturally, selected between the twenty-fourth and the thirty-seventh pregnancy week (M = 31.20; S.D. = 5.10), aged between 18 and 41 years (M = 29.94; S.D. = 5.92);
- (b)
- Forty-five pregnant women (experimental group) who were receiving an assisted reproduction treatment, aged between 21 and 42 years (M = 31.27; S.D. = 4.88), selected between the twenty-third to the thirty-seventh pregnancy week (M = 28.56; S.D. = 3.60).
4.2. Instruments
- (a)
- Differentiation from Self is represented by items showing the woman’s joy at thought of “another from herself” and the attribution of her child’s name (example: “I like to watch my belly move while the child is kicking”).
- (b)
- Interaction with the fetus, that underlines the woman’s intention to talk to her fetus and refer to him/her by a nickname (example: “I talk about the child using nicknames o terms of Endearment”).
- (c)
- Attributing characteristics and intentions, that highlights the woman’s recurring thoughts about what she may be feeling and process the fetus inside the own belly, or on the possible personality characteristics of fetus based on movements (example: “I can almost imagine what personality mine will have my child by how it moves”).
- (d)
- Giving of Self is represented by actions that show the woman’s willingness to commit herself during pregnancy in order to prevent potential harm to the fetus (example: “I eat healthy so that my child can benefit from a healthy diet”).
- (e)
- Role Taking is represented by items that highlight the woman’s ability to imagine oneself as a mother in the future and therefore thoughts related to maternal roles in feeding and caring for her child (example: “I imagine taking care of the child”).
- A.
- State anxiety represents a constellation of nervousness, fear, and discomfort induced by situations that are perceived as dangerous during a precise moment. Therefore, it is a measure of the level of contingent anxiety, i.e., related to feelings of insecurity and helplessness, which could lead to a consequent behavior of escape and avoidance from the dangerous situation.
- B.
- Trait anxiety represents a constellation of feelings of stress and daily discomfort; therefore, it can be considered the tendency to perceive stressful situations as dangerous with a consequent tendency to respond to situations with varying intensity.
5. Data Analysis
6. Preliminary Analysis
7. Results
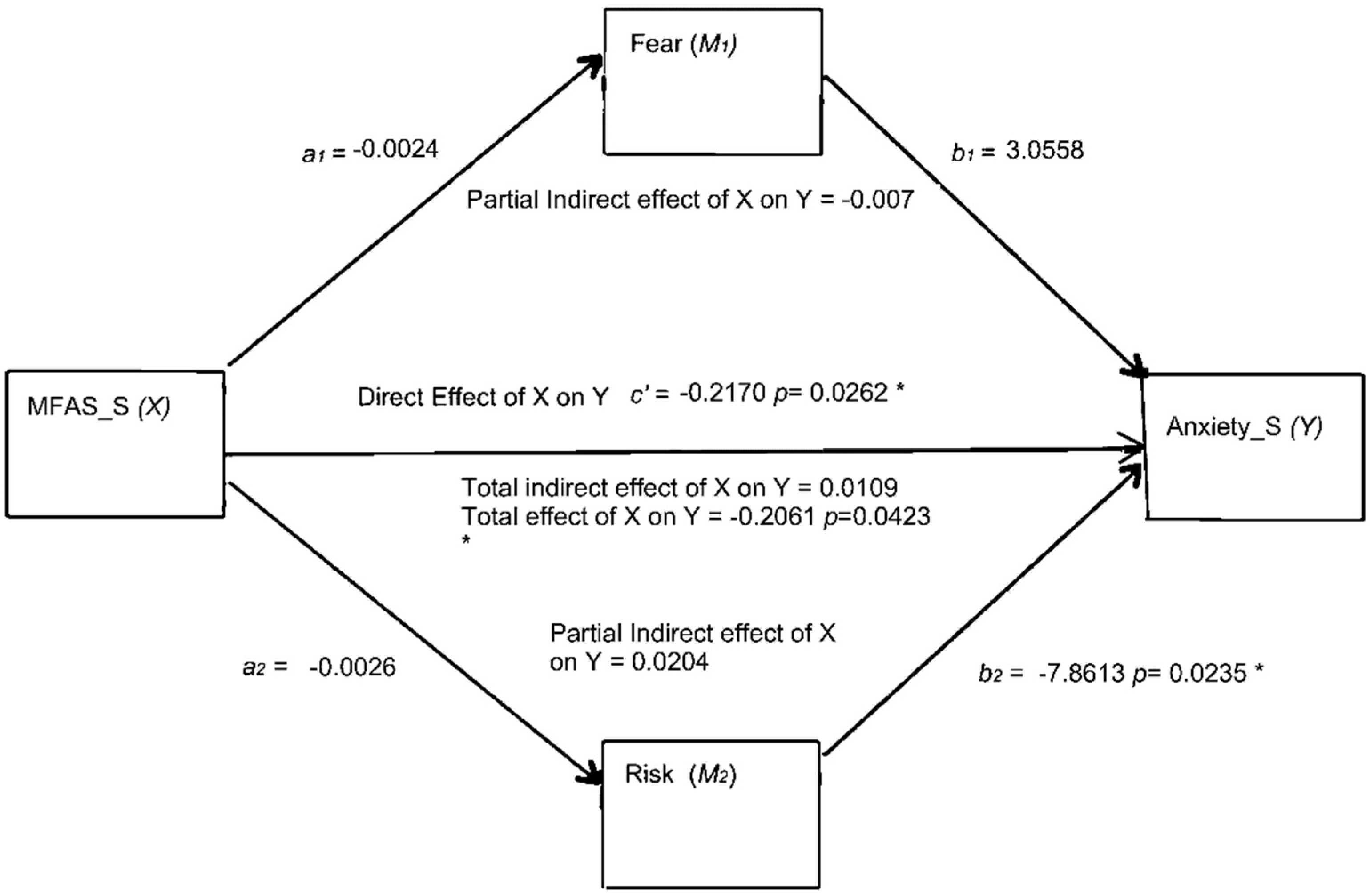
- (a)
- Indirect effect 1 (a1 ∗ b1): MFA →fear →anxiety; a1 (−0.0031) ∗ b1 (2.706) = −0.0084 (LLCI = −0.0356, ULCI = 0.0121). Because zero falls between the lower and upper bound of the 95% confidence interval, we infer that the indirect effect of MFA (X) through fear (MV1) on anxiety (Y) was not statistically significant.
- (b)
- Indirect effect 2 (a2 ∗ b2): MFA → risk → anxiety; a2 (−0.0019) ∗ b2 (−7.543) = 0.0144 (LLCI = −0.0462, ULCI = 0.0887). Because zero (the null) falls between the lower and upper bound of the 95% confidence interval, we assume that the indirect effect of MFA (X) through risk (MV2) on anxiety (Y) was also not significantly different from zero.
8. Discussion
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bjelica, A.; Cetkovic, N.; Trninic-Pjevic, A.; Mladenovic-Segedi, L. The phenomenon of pregnancy—A psychological view. Ginekol. Pol. 2018, 89, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Teskereci, G.; Öncel, S.; Arslan, Ü. Developing compassion and emotional intelligence in nursing students: A quasi-experimental study. Perspect. Psychiatr. Care 2020, 56, 797–803. [Google Scholar] [CrossRef]
- Stern, D.N. La Costellazione Materna. Il Trattamento Psicoterapeutico Della Coppia Madre-Bambino. [The Mother Constellation. The Psychotherapeutic Treatment of the Mother-Child Couple]; Boringhieri Editore: Torino, Italy, 1995; pp. 35–52. [Google Scholar]
- Kendell, R.E.; Wainwright, S.; Hailey, A.; Shannon, B. The influence of childbirth on psychiatric morbidity. Psychol. Med. 1976, 6, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Ali, N.S.; Azam, I.S.; Ali, B.S.; Tabbusum, G.; Moin, S.S. Frequency and associated factors for anxiety and depression in pregnant women: A hospital-based cross-sectional study. Sci. World J. 2012, 2012, 653098. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, L.; Sobotka, T.; Bentzen, J.G.; Andersen, A.N. Demographic andmedical consequences of the postponement of parenthood. Hum. Reprod. 2012, 18, 29–43. [Google Scholar] [CrossRef]
- Boivin, J.; Takefman, J.E. Impact of the in-vitro fertilization process onemotional, physical and relational variables. Hum. Reprod. 1996, 11, 903–907. [Google Scholar] [CrossRef]
- Cousineau, T.M.; Domar, A.D. Psychological impact of infertility. Best Pract. Res. Clin. Obstet. Gynaecol. 2007, 21, 293–308. [Google Scholar] [CrossRef] [PubMed]
- Lykeridou, K.; Gourounti, K.; Deltsidou, A.; Loutradis, D.; Vaslamatzis, G. Theimpact of infertility diagnosis on psychological status of women undergoingfertility treatment. J. Reprod. Infant Psychol. 2009, 27, 223–237. [Google Scholar] [CrossRef]
- Turner, K.; Reynolds-May, M.F.; Zitek, E.M.; Tisdale, R.L.; Carlisle, A.B.; Westphal, L.M. Stress and Anxiety Scores in First and Repeat IVF Cycles: A PilotStudy. PLoS ONE 2013, 8, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Bryan, A.A. Enhancing parent-child interaction with a prenatal couple intervention. MCN: The American. J. Matern./Child. Nurs. 2000, 25, 139–145. [Google Scholar] [CrossRef]
- Deutsch, H. Psicologia Della Donna Adulta E Madre. Studio Psicoanalitico. [Psychology of the Adult Woman and Mother. Psychoanalytic Study]; Boringhieri: Torino, Italy, 1945; Volume 2, pp. 57–92. [Google Scholar]
- Torvisco, J.M.; Wichrowska, M.; Pellerone, M. Filio-parental violence analyzed through the Spanish press (2010–2020). Child-to-parent violence: A case of family violence. Front. Sociol. 2023, 8, 985173. [Google Scholar] [CrossRef]
- Winnicott, D.W. Dalla Pediatria Alla Psicoanalisi. [From Pediatrics to Psychoanalysis]; Martinelli: Florence, Italy, 1958; pp. 57–83. [Google Scholar]
- Laxton-Kane, M.; Slade, P. The role of maternal prenatal attachment in a woman’s experience of pregnancy and implications for the process of care. J. Reprod. Infant Psychol. 2002, 20, 253–266. [Google Scholar] [CrossRef]
- Cannella, B.L. Maternal-fetal attachment: An integrative review. J. Adv. Nurs. 2005, 50, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Heshmati, R.; Pellerone, M.; Esfandi, M.R.N.; Yeganeh, N.; Jafari, E. Interpersonal attachment styles and body dysmorphic symptoms in adolescent girls: The mediating role of body image. Clin. Neuropsychiatry 2023, 20, 141–150. [Google Scholar]
- Pines, D. The relevance of early psychic development to pregnancy and abortion. Int. J. Psycho-Anal. 1982, 63, 311–319. [Google Scholar]
- Trombetta, T.; Giordana, M.; Santoniccolo, F.; Vismara, L.; Della Vedova, A.M.; Rollè, L. Pre-natal attachment and parent-to-infant attachment: A systematic review. Front. Psychol. 2022, 12, 620942. [Google Scholar] [CrossRef]
- Mannino, G.; Montefiori, V.; Vitiello, M.; Iacolino, C.; Pellerone, M.; La Fiura, G.; Bernardone, A.; Faraci, E.; Giunta, S. The Psychosomatic Relationship As A Symbolic Circular Communication: Subjective And Transgenerational Dreams. World Futures 2019, 75, 426–441. [Google Scholar] [CrossRef]
- Brazelton, T.B.; Cramer, B.G. The Earliest Relationship: Parents, Infants, and the Drama of Early Attachment; Addison Wesley Longman: Upper Saddle River, NJ, USA, 1991; pp. 57–92. [Google Scholar]
- McMahon, C.; Boivin, J.; Gibson, F.L.; Hammarberg, K.; Wynter, K.; Saunders, D.; Fisher, J. Pregnancy specific anxiety, ART conception and infant temperament at 4 months post-partum. Hum. Reprod. 2012, 28, 997–1005. Available online: http://humrep.oxfordjournals.org/content/early/2013/02/20/humrep.det029.full (accessed on 3 February 2020). [CrossRef]
- McMahon, C.; Boivin, J.; Gibson, F.; Hammarberg, K.; Wynter, K.; Saunders, D.; Fisher, J. Age at first birth, mode of conception and psychological wellbeing in pregnancy: Findings from the Parental Age and Transition to Parenthood Australia (PATPA) Study. Hum. Reprod. 2011, 26, 1389–1398. Available online: http://humrep.oxfordjournals.org/content/early/2011/03/25/humrep.der076.full (accessed on 10 March 2020). [CrossRef] [PubMed]
- Santona, A. Trasformazione della coppia nel percorso verso la genitorialità adottiva. [Transformation of the couple on the path to adoptive parenthood]. Minor. Giust. 2003, 1, 29–38. [Google Scholar]
- Galasso, S.; Langher, V.; Ricci, M.E. Il corpo femminile e il mondo interno [The female body and the internal world]. Riv. Sessuol. 2017, 41, 12–24. [Google Scholar]
- Smorti, M.; Valoriani, V.; Vanni, C.; Benvenuti, P. Assisted reproduction and maternal representations during pregnancy Aims. Psicol. Salut. 2010, 1, 33–55. [Google Scholar] [CrossRef]
- Samadaee-Gelehkolaee, K.; McCarthy, B.W.; Khalilian, A.; Hamzehgardeshi, Z.; Peyvandi, S.; Elyasi, F.; Shahidi, M. Factors associated with marital satisfaction in infertile couple: A comprehensive literature Review. Glob. J. Health Sci. 2015, 8, 96–109. [Google Scholar] [CrossRef]
- De Camillis, B. Strategie Di Coping Nelle Coppie Infertili. [Coping Strategies in Infertile Couples]. Psicoter.-Form. 2010, 5, 109–132. Available online: http://www.psicoterapeutiinformazione.it/wp-content/uploads/2020/05/6-De-Camillis-Infertilit%C3%A0.pdf (accessed on 5 February 2020).
- Lowyck, B.; Luyten, P.; Corveleyn, J.; D’Hooghe, T.; Buyse, E.; Demyttenaere, K. Well-being and relationship satisfaction of couples dealing with an in vitro fertilization/intracytoplasmic sperm injection procedure: A multilevel approach on the role of self-criticism, dependency, and romantic attachment. Fertil. Steril. 2009, 91, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Letherby, G.; Williams, C. Non-motherhood: Ambivalent autobiographies. Fem. Stud. 1999, 25, 719–728. [Google Scholar] [CrossRef]
- Langher, V.; Fedele, F.; Caputo, A.; Marchini, F.; Aragona, C. Extreme Desire for Motherhood: Analysis of Narratives From Women Undergoing Assisted Reproductive Technology (ART). Eur. J. Psychol. 2019, 7, 292–311. [Google Scholar] [CrossRef]
- Hjelmstedt, A.; Widström, A.M.; Wramsby, H.; Matthiesen, A.S.; Collins, A. Personality factors and emotional responses to pregnancy among IVF couples in early pregnancy: A comparative study. Acta Obstet. Gynecol. Scand. 2003, 82, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.; Schonbrun, Y.C.; Zlotnick, C.; Bates, N.; Todorova, R.; Kao, J.C.W.; Johnson, J. A qualitative study of treatment needs among pregnant and postpartum women with substance use and depression. Subst. Use Misuse 2013, 48, 1498–1508. [Google Scholar] [CrossRef]
- Fisher, L.; Skaff, M.M.; Mullan, J.T.; Arean, P.; Glasgow, R.; Masharani, U. A longitudinal study of affective and anxiety disorders, depressive affect and diabetes distress in adults with Type 2 diabetes. Diabet. Med. 2008, 25, 1096–1101. [Google Scholar] [CrossRef]
- Udry-Jørgensen, L.; Darwiche, J.; Germond, M.; Wunder, D.; Vial, Y. Anxiety, depression, and attachment before and after the first-trimester screening for Down syndrome: Comparing couples who undergo ART with those who conceive spontaneously. Prenat. Diagn. 2015, 35, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Ranjbar, F.; Warmelink, J.C.; Gharacheh, M. Prenatal attachment in pregnancy following assisted reproductive technology: A literature review. J. Reprod. Infant Psychol. 2020, 38, 86–108. [Google Scholar] [CrossRef] [PubMed]
- Aksu, H.; ŞATIR, D.G. Comparison of the Adaptation to Pregnancy in Women Who Received Infertility Treatment and Those Who Didn’t. J. Basic Clin. Health Sci. 2022, 6, 260–267. [Google Scholar] [CrossRef]
- McNamara, J.; Townsend, M.L.; Herbert, J.S. A systemic review of maternal wellbeing and its relationship with maternal fetal attachment and early postpartum bonding. PLoS ONE 2019, 14, e0220032. [Google Scholar] [CrossRef]
- Pellerone, M.; Miccichè, S. Prenatal attachment and anxiety: Women who decide to try in vitro fertilization and women who procreate naturally. Psychol. Res. 2014, 4, 6. [Google Scholar] [CrossRef]
- Eskici, L.; Demir Akca, A.S.; Atasoy, N.; Arikan, İ.; Harma, M. Gebelerde depresyon ve anksiyete bozukluğunun obstetrik sonuçlari ve yenidoğan üzerine etkileri. Anatol. J. Clin. Investig. 2012, 6, 1. [Google Scholar]
- Özdemir, K.; Çevirme, A.; Başkaya, Y. Anxiety and prenatal attachment levels in pregnancy and influencing factors. Cukurova Med. J. 2020, 45, 502–510. [Google Scholar] [CrossRef]
- Bernstein, D.P.; Fink, L.; Handelsman, L.; Foote, J. Childhood Trauma Questionnaire (CTQ) [Database Record]; APA PsycTests: Washington, DC, USA, 1994. [Google Scholar]
- Berle, J.; Mykletun, A.; Daltveit, A.K.; Rasmussen, S.; Holsten, F.; Dahl, A.A. Neonatal outcomes in offspring of women with anxiety and depression during pregnancy. Arch. Womens Ment. Health 2005, 8, 181–189. [Google Scholar] [CrossRef]
- Cranley, M.S. Development of a tool for the measurement of maternal attachment during pregnancy. Nurs. Res. 1981, 30, 281–284. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorusch, R.L.; Lushene, R. The State-Trait Anxiety Inventory: Test Manual; American Psychological Association: Palo Alto, CA, USA, 1970. [Google Scholar]
- Pedrabissi, L.; Santinello, M. Verifica Della Validità Dello STAI Forma Y di Spielberger; Giunti Organizzazioni Speciali: Florence, Italy, 1989. [Google Scholar]
- Stehlik-Barry, K.; Bebinec, A.J. Data Analysis with IBM SPSS Statistics; Packt Publishing Ltd.: Birmingham, UK, 2017. [Google Scholar]
- Berryman, J.C.; Windridge, K.C. Pregnancy after 35 and attachment to the fetus. J. Reprod. Infant Psychol. 1996, 14, 133–143. [Google Scholar] [CrossRef]
- Zachariah, R. Mother-daughter and husband-wife attachment as predictors of psychological well-being during pregnancy. Clin. Nurs. Res. 1994, 3, 371–392. [Google Scholar] [CrossRef] [PubMed]
- Kenner, C.; Dreyer, L.A. Prenatal and neonatal testing and screening: A double-edged sword. Nurs. Clin. N. Am. 2000, 35, 627–642. [Google Scholar] [CrossRef]
- Laganà, A.S.; La Rosa, V.L.; Rapisarda, A.M.; Vitale, S.G. Reflections about the impact of infertility on female sexual function. Kathmandu Univ. Med. J. 2016, 14, 299–300. [Google Scholar]
- Maroufizadeh, S.; Karimi, E.; Vesali, S.; Omani-Samani, R. Anxiety and depression after failure of assisted reproductive treatment among patients experiencing infertility. Int. J. Gynaecol. Obstet. 2015, 130, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Pinto, T.M.; Samorinha, C.; Tendais, I.; Silva, S.; Figueiredo, B. Antenatal paternal adjustment and paternal attitudes after infertility treatment. Hum. Reprod. 2018, 33, 109–115. [Google Scholar] [CrossRef]
- Crespo, E.; Bestard, J. Psychosocial needs of women and their partners after successful assisted reproduction treatment in Barcelona. Reprod. Biomed. Soc. Online 2016, 3, 90–99. [Google Scholar] [CrossRef]
- Heshmati, R.; Pellerone, M. The big five personality traits and dispositional mindfulness as predictors of alexithymia in college students. Clin. Neuropsychiatry 2019, 16, 98. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8650186/ (accessed on 11 March 2020). [PubMed]
- Huang, M.Z.; Sun, Y.C.; Gau, M.L.; Puthussery, S.; Kao, C.H. First-time mothers’ experiences of pregnancy and birth following assisted reproductive technology treatment in Taiwan. J. Health Popul. Nutr. 2019, 38, 10. [Google Scholar] [CrossRef] [PubMed]
- Formica, I.; Barberis, N.; Costa, S.; Nucera, J.; Falduto, M.L.; Maganuco, N.R.; Pellerone, M.; Schimmenti, A. The role of social support and emotional intelligence on negative mood states among couples during pregnancy: An actor-partner interdependence model approach. Clin. Neuropsychiatry 2018, 15, 19–26. [Google Scholar]
- Pellerone, M.; Tomasello, G.; Migliorisi, S. Relationship between parenting, alexithymia and adult attachment styles: A cross-sectional study on a group of adolescents and young adults. Clin. Neuropsychiatry 2017, 14, 125–134. [Google Scholar]
- Pellerone, M.; Ramaci, T.; Herrera López, M.; Craparo, G. The role of identity development and decision making process on adult attachment: A cross-national study in Sicilian and andalusian adolescents. Clin. Neuropsychiatry 2017, 14, 141–150. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| N | Min. | Max. | Mean | Std. Dev. | |
|---|---|---|---|---|---|
| Gestational age | 50 | 24 | 37 | 31.20 | 3.94 |
| Waiting period | 50 | 0 | 24 | 2.86 | 5.10 |
| Fear of not being pregnant | 50 | 0 | 1 | 0.46 | 0.50 |
| Perception of a high-risk pregnancy | 49 | 0 | 1 | 0.20 | 0.41 |
| Presence of other children | 50 | 0 | 1 | 0.38 | 0.49 |
| N | Min. | Max. | Mean | Std. Devi. | |
|---|---|---|---|---|---|
| Gestational age | 45 | 23 | 37 | 28.56 | 3.60 |
| Waiting period | 45 | 12 | 96 | 26.22 | 14.48 |
| Fear of not being pregnant | 45 | 0 | 1 | 0.84 | 0.37 |
| Perception of a high-risk pregnancy | 45 | 0 | 1 | 0.31 | 0.47 |
| Assisted fertilization attempts | 45 | 1 | 6 | 2.40 | 1.286 |
| Presence of other children | 45 | 0 | 1 | 0.07 | 0.252 |
| Variables | A. | B. | C. | D. | E. | F. |
|---|---|---|---|---|---|---|
| A. Gestational age | - | |||||
| B. Age | 0.15 | - | ||||
| C. Waiting period | 0.06 | −0.04 | - | |||
| D. Fear of not being pregnant | 0.31 * | 0.18 | 0.06 | - | ||
| E. Perception of a high-risk pregnancy | 0.65 ** | 0.18 | 0.04 | 0.34 * | - | |
| F. Presence of other children | 0.50 ** | 0.31 * | −0.04 | 0.02 | 0.35 * | - |
| G. Total MFAS | 0.05 | −0.24 | −0.19 | −0.01 | −0.06 | 0.11 |
| Variables | A. | B. | C. | D. | E. | F. | G. | H. |
|---|---|---|---|---|---|---|---|---|
| A. Gestational age | - | |||||||
| B. Age | −0.13 | - | ||||||
| C. Waiting period | 0.512 * | −0.08 | - | |||||
| D. Fear of not being pregnant | 0.20 | 0.29 | 0.02 | - | ||||
| E. Perception of the high-risk pregnancy | 0.07 | 0.10 | −0.21 | 0.29 | - | |||
| F. Fertilization technique | 0.15 | −0.22 | 0.20 | −0.15 | −0.13 | - | ||
| G. Assisted fertilization attempts | 0.26 | −0.12 | 0.10 | 0.33 * | −0.02 | 0.05 | - | |
| H. Presence of other children | 0.34 * | −0.02 | 0.56 ** | 0.12 | −0.18 | 0.22 | 0.13 | - |
| I. Total MFAS | −0.32 * | −0.09 | 0.07 | −0.16 | −0.08 | 0.28 | 0.02 | 0.03 |
| Dimensions | Sub-Dimensions | Group | N | M. | S.D | T | p-Value |
|---|---|---|---|---|---|---|---|
| MFAS | Role Taking | Experimental Group | 45 | 17.00 | 2.11 | 0.76 | |
| Control Group | 50 | 16.68 | 2.00 | 0.76 | 0.45 | ||
| Differentiation from Self | Experimental Group | 45 | 15.91 | 2.10 | 0.94 | ||
| Control Group | 50 | 15.56 | 1.54 | 0.92 | 0.36 | ||
| Interaction with the fetus | Experimental Group | 45 | 17.00 | 2.41 | −0.42 | ||
| Control Group | 50 | 17.20 | 2.24 | −0.42 | 0.68 | ||
| Attributing characteristics and intentions | Experimental Group | 45 | 20.80 | 3.18 | 1.43 | ||
| Control Group | 50 | 19.96 | 2.55 | 1.41 | 0.16 | ||
| Giving of Self | Experimental Group | 45 | 18.76 | 1.84 | 0.86 | ||
| Control Group | 50 | 18.34 | 2.73 | 0.88 | 0.38 | ||
| Total MFAS | Experimental Group | 45 | 100.87 | 17.90 | −4.44 | ||
| Control Group | 50 | 115.01 | 12.98 | −4.37 | 0.00 | ||
| STAI | STAI S (State anxiety) | Experimental Group | 45 | 43.27 | 9.62 | 2.06 | |
| Control Group | 50 | 39.28 | 9.24 | 2.06 | 0.04 | ||
| STAI T (Trait anxiety) | Experimental Group | 45 | 44.47 | 7.55 | 1.59 | ||
| Control Group | 50 | 41.94 | 7.92 | 1.59 | 0.12 |
| Variables | A. | B. | C. | D. | E. | F. | G. |
|---|---|---|---|---|---|---|---|
| A. Role taking | - | ||||||
| B. Differentiation from self | 0.37 * | - | |||||
| C. Interaction with fetus | 0.33 * | −0.04 | - | ||||
| D. Attributing characteristics and intentions | 0.21 | −0.07 | 0.26 | - | |||
| E. Giving of self | −0.14 | −0.25 | 0.27 | 0.13 | - | ||
| F. Total MFAS | −0.27 | 0.16 | −0.37 * | −0.53 ** | −0.17 | - | |
| G. STAI S | 0.13 | 0.23 | 0.12 | 0.26 | 0.01 | −0.38 ** | - |
| H. STAI T | −0.04 | 0.09 | 0.05 | 0.28 | −0.21 | −0.44 ** | 0.46 ** |
| Total Effect IV- > DV | Direct Effect IV- > DV | Relationship | Indirect Effect | Confidence Interval | t-Student | Conclusion | |
|---|---|---|---|---|---|---|---|
| Lower Bound Upper Bound | |||||||
| −0.206 (0.009) | −0.211 (0.005) | IV Hypothesis IV- > MV1-VD Hp 4VI > MV2- > V | 0.0060; SE = 0.0331 | −0.0592 | 0.0769 | −2.720 | Partial mediation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pellerone, M.; Martinez-Torvisco, J.; Razza, S.G.; Commodari, E.; Miccichè, S. Precursors of Prenatal Attachment and Anxiety during Pregnancy in Women Who Procreate Naturally and Pregnant Women following Assisted Reproduction Technology. Int. J. Environ. Res. Public Health 2023, 20, 6945. https://doi.org/10.3390/ijerph20206945
Pellerone M, Martinez-Torvisco J, Razza SG, Commodari E, Miccichè S. Precursors of Prenatal Attachment and Anxiety during Pregnancy in Women Who Procreate Naturally and Pregnant Women following Assisted Reproduction Technology. International Journal of Environmental Research and Public Health. 2023; 20(20):6945. https://doi.org/10.3390/ijerph20206945
Chicago/Turabian StylePellerone, Monica, Juan Martinez-Torvisco, Stesy Giuseppa Razza, Elena Commodari, and Sandra Miccichè. 2023. "Precursors of Prenatal Attachment and Anxiety during Pregnancy in Women Who Procreate Naturally and Pregnant Women following Assisted Reproduction Technology" International Journal of Environmental Research and Public Health 20, no. 20: 6945. https://doi.org/10.3390/ijerph20206945