
Factors Associated with Medication Adherence among Patients with Type 2 Diabetes Mellitus: A Hospital-Based Cross-Sectional Study in Nepal

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
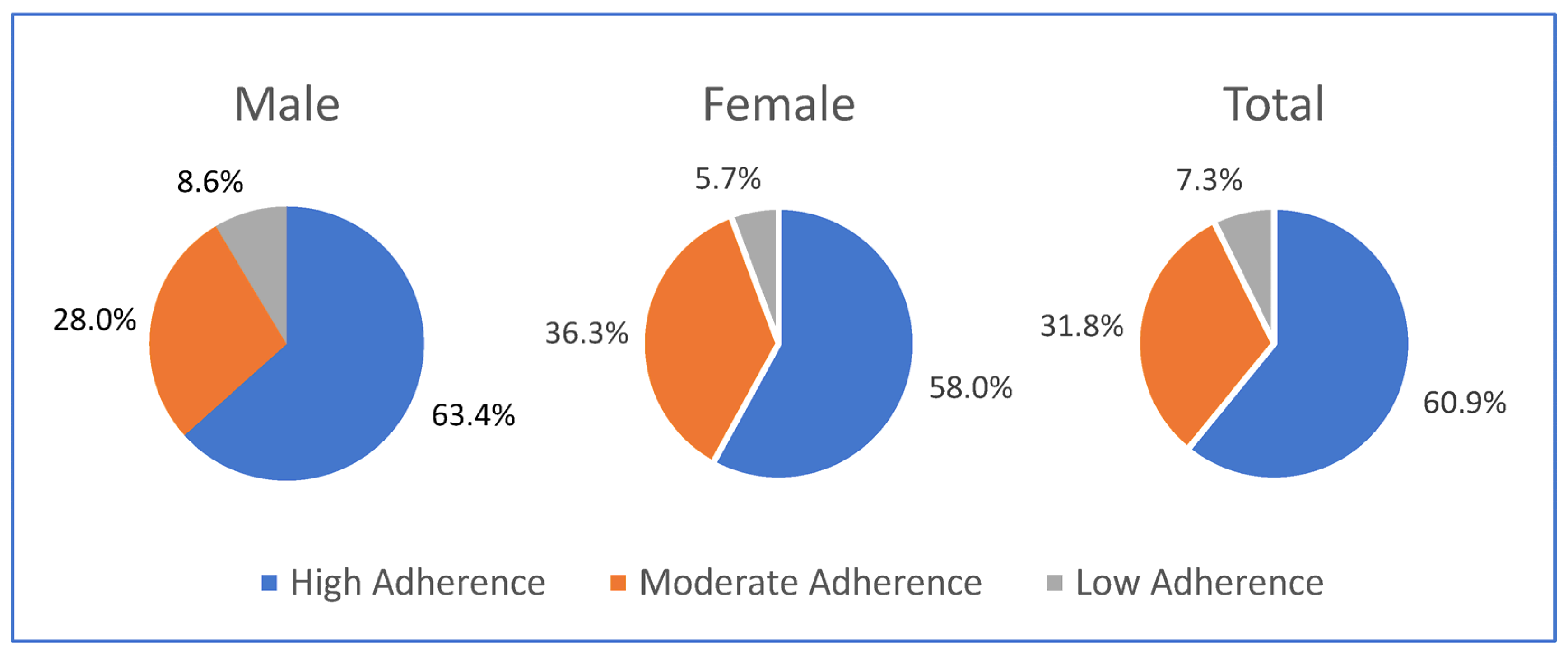
2.1. Outcome
2.2. Exposures
- Socio-demographic characteristics, which included age (years), gender (male/female), education (non-formal/up to School Leaving Certificate (SLC)/above SLC), ethnicity (Brahmin/Newars/others), residency (rural/urban), occupation (housewife/business/agriculture/office (professional)/unemployed/other occupation), and family support for medication (yes/no).
- Clinical characteristics, which included duration of diabetes (years), duration of medication intake (years), immediate family members with diabetes (yes/no), history of hypertension (yes/no), history of current antihypertensive medication (yes/no), history of diabetes complication (yes/no), time given by doctors (minutes per visit), diabetes counseling (yes/no) and types of diabetes medication (Oral Hypoglycemic Agents (OHA)/insulin/both).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AOR | Adjusted odds ratio |
| β | Beta coefficient |
| CI | Confidence interval |
| FBS | Fasting blood sugar |
| IQR | Interquartile range |
| LMIC | Low- and middle-income countries |
| MMAS-8 | Morisky medication adherence scale-8 (© 2006 Donald E. Morisky) |
| OHA | Oral hypoglycemic agents |
| SLC | School Leaving Certificate |
| SD | Standard deviation |
| OR | Odds ratio |
| USD | US Dollars |
References
- WHO. Diabetes 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 4 January 2023).
- IDF. IDF Diabetes Atlas, 10th ed.; IDF: Brussels, Belgium, 2021. [Google Scholar]
- Shrestha, D.B.; Budhathoki, P.; Sedhai, Y.R.; Marahatta, A.; Lamichhane, S.; Nepal, S.; Adhikari, A.; Poudel, A.; Nepal, S.; Atreya, A. Type 2 Diabetes Mellitus in Nepal from 2000 to 2020: A systematic review and meta-analysis. F1000Research 2021, 10, 543. [Google Scholar] [CrossRef]
- Shrestha, N.; Mishra, S.R.; Ghimire, S.; Gyawali, B.; Mehata, S. Burden of Diabetes and Prediabetes in Nepal: A Systematic Review and Meta-Analysis. Diabetes Ther. 2020, 11, 1935–1946. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Health Risks: Mortality and Burden of Disease Attributable to Selected Major Risks; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Pandey, A.R.; Aryal, K.K.; Shrestha, N.; Sharma, D.; Maskey, J.; Dhimal, M. Burden of Diabetes Mellitus in Nepal: An Analysis of Global Burden of Disease Study 2019. J. Diabetes Res. 2022, 2022, 4701796. [Google Scholar] [PubMed]
- Safiri, S.; Karamzad, N.; Kaufman, J.S.; Bell, A.W.; Nejadghaderi, S.A.; Sullman, M.J.; Moradi-Lakeh, M.; Collins, G.; Kolahi, A.A. Prevalence, Deaths and Disability-Adjusted-Life-Years (DALYs) Due to Type 2 Diabetes and Its Attributable Risk Factors in 204 Countries and Territories, 1990–2019: Results From the Global Burden of Disease Study 2019. Front. Endocrinol. 2022, 13, 838027. [Google Scholar] [CrossRef]
- Shrestha, N.; Lohani, S.P.; Angdembe, M.R.; Bhattarai, K.; Bhattarai, J. Cost of diabetes mellitus care among patients attending selected outpatient clinics. J. Nepal Med. Assoc. 2013, 52, 343–348. [Google Scholar] [CrossRef]
- Gupta, I.; Chowdhury, S. Correlates of out-of-pocket spending on health in Nepal: Implications for policy. WHO South-East Asia J. Public Health 2014, 3, 238–246. [Google Scholar] [CrossRef] [Green Version]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. 1. Improving Care and Promoting Health in Populations: Standards of Care in Diabetes—2023. Diabetes Care 2023, 46 (Suppl. 1), S10–S18. [Google Scholar] [CrossRef]
- Kikkawa, R. Chronic complications in diabetes mellitus. Br. J. Nutr. 2000, 84, S183–S185. [Google Scholar] [CrossRef]
- Herkert, D.; Vijayakumar, P.; Luo, J.; Schwartz, J.I.; Rabin, T.L.; DeFilippo, E.; Lipska, K.J. Cost-related insulin underuse among patients with diabetes. JAMA Intern. Med. 2019, 179, 112–114. [Google Scholar] [CrossRef]
- Abebe, S.M.; Berhane, Y.; Worku, A.; Alemu, S.; Mesfin, N. Level of sustained glycemic control and associated factors among patients with diabetes mellitus in Ethiopia: A hospital-based cross-sectional study. Diabetes Metab. Syndr. Obes. Targets Ther. 2015, 8, 65–71. [Google Scholar] [CrossRef]
- Al-Qazaz, H.; Hassali, M.A.; Shafie, A.A.; Sulaiman, S.A.; Sundram, S.; Morisky, D.E. The eight-item Morisky Medication Adherence Scale MMAS: Translation and validation of the Malaysian version. Diabetes Res Clin Pract. 2010, 90, 216–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, D.; Refaat, M.; Mohammedi, K.; Jayyousi, A.; Al Suwaidi, J.; Abi Khalil, C. Macrovascular Complications in Patients with Diabetes and Prediabetes. Biomed. Res. Int. 2017, 2017, 7839101. [Google Scholar] [CrossRef] [PubMed]
- Kopf, S.; Groener, J.B.; Kender, Z.; Fleming, T.; Bischoff, S.; Jende, J.; Schumann, C.; Ries, S.; Bendszus, M.; Schuh-Hofer, S.; et al. Deep phenotyping neuropathy: An underestimated complication in patients with pre-diabetes and type 2 diabetes associated with albuminuria. Diabetes Res. Clin. Pract. 2018, 146, 191–201. [Google Scholar] [CrossRef] [PubMed]
- Elsous, A.; Radwan, M.; Al-Sharif, H.; Abu Mustafa, A. Medications adherence and associated factors among patients with type 2 diabetes mellitus in the Gaza Strip, Palestine. Front. Endocrinol. 2017, 8, 100. [Google Scholar] [CrossRef] [Green Version]
- Atekha, B.O. Factors Associated with Adherence to Diabetes Medication among Individuals with Type 2 Diabetes in Cambridge, Ontario, Canada. Ph.D. Thesis, Walden University, Minneapolis, MN, USA, 2018. [Google Scholar]
- Abebaw, M.; Messele, A.; Hailu, M.; Zewdu, F. Adherence and Associated Factors towards Antidiabetic Medication among Type II Diabetic Patients on Follow-Up at University of Gondar Hospital, Northwest Ethiopia. Adv. Nurs. 2016, 2016, 8579157. [Google Scholar] [CrossRef] [Green Version]
- Feldman, B.S.; Cohen-Stavi, C.J.; Leibowitz, M.; Hoshen, M.B.; Singer, S.R.; Bitterman, H.; Lieberman, N.; Balicer, R.D. Defining the role of medication adherence in poor glycemic control among a general adult population with diabetes. PLoS ONE 2014, 9, e108145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shrestha, K.D.; Takma, K.; Ghimire, R. Adherence to Therapeutic Regimen in Diabetic Patients Attending a Tertiary Level Hospital. J. Inst. Med. Nepal 2020, 42, 47–53. [Google Scholar] [CrossRef]
- Shrestha, S.S.; Shakya, R.; Karmacharya, B.M.; Thapa, P. Medication adherence to oral hypoglycemic agents among type II diabetic patients and their clinical outcomes with special reference to fasting blood glucose and glycosylated hemoglobin levels. Kathmandu Univ. Med. J. (KUMJ) 2013, 11, 226–232. [Google Scholar] [CrossRef] [Green Version]
- Sah, B.; Basyal, D.; Gaire, A. Medication Non-Adherence among Type-II Diabetes Mellitus Out-Patients Attending at Tertiary Care Hospital, Nepal. Clin. Pharmacol. Biopharm. 2021, 10, 2. [Google Scholar]
- Bhattarai, B.; Bista, B.; Shrestha, S.; Budhathoki, B.; Dhamala, B. Contributing factors of non-adherence to treatment among the patients with type II diabetes mellitus. J. Manmohan Meml. Inst. Health Sci. 2019, 5, 68–78. [Google Scholar] [CrossRef]
- Kafle, N.K.; Poudel, R.R.; Shrestha, S.M. Noncompliance to diet and medication among patients with type 2 diabetes mellitus in selected hospitals of Kathmandu, Nepal. J. Soc. Health Diabetes 2018, 6, 90–95. [Google Scholar] [CrossRef]
- Sapkota, S.; Brien, J.-A.E.; Aslani, P. Nepalese patients’ anti-diabetic medication taking behaviour: An exploratory study. Ethn. Health 2018, 23, 718–736. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.C.; Wu, C.H.; Wang, H.H.; Li, H.W.; Hui, E.M.; Lam, A.T.; Chung, R.Y.; Yip, B.H.; Morisky, D.E. Association between the 8-item Morisky medication adherence scale (MMAS-8) score and glycaemic control among Chinese diabetes patients. J. Clin. Pharmacol. 2015, 55, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Shakya, P.; Shrestha, A.; Karmacharya, B.M.; Kulseng, B.E. Glycemic Control and Its Association with Medication Adherence among Type 2 Diabetes Mellitus Patients in Nepal—A Hospital based Cross-Sectional Study in Dhulikhel Hospital, Nepal. Master’s Thesis, Norwegian University of Science and Technology, Trondheim, Norway, 2017. [Google Scholar]
- Morisky, D.E.; Ang, A.; Krousel-Wood, M.; Ward, H.J. Predictive validity of a medication adherence measure in an outpatient setting. J. Clin. Hypertens. 2008, 10, 348–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berlowitz, D.R.; Foy, C.G.; Kazis, L.E.; Bolin, L.P.; Conroy, M.B.; Fitzpatrick, P.; Gure, T.R.; Kimmel, P.L.; Kirchner, K.; Morisky, D.E.; et al. Effect of intensive blood-pressure treatment on patient-reported outcomes. N. Engl. J. Med. 2017, 377, 733–744. [Google Scholar] [CrossRef]
- Bress, A.P.; Bellows, B.K.; King, J.B.; Hess, R.; Beddhu, S.; Zhang, Z.; Berlowitz, D.R.; Conroy, M.B.; Fine, L.; Oparil, S.; et al. Cost-effectiveness of intensive versus standard blood-pressure control. N. Engl. J. Med. 2017, 377, 745–755. [Google Scholar] [CrossRef]
- Koju, R.; Karmacharya, B.M.; Shrestha, A.K.; Shrestha, S.; Shakya, P.; Yogal, C.; Humagain, S.; Gyawali, P.; Amatya, B.; Fitzpatrick, A. Design of the Dhulikhel Heart Study (DHS): The epidemiology of emerging cardiovascular disease in Nepal. Ann. Glob. Health 2014, 3, 204–205. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Strobe Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- MuKherjee, S.; SharMaSarKar, B.; DaS, K.K.; Bhattacharyya, A.; Deb, A. Compliance to anti-diabetic drugs: Observations from the diabetic clinic of a medical college in kolkata, India. J. Clin. Diagn. Res. JCDR 2013, 7, 661. [Google Scholar] [CrossRef]
- Powers, M.A.; Bardsley, J.; Cypress, M.; Duker, P.; Funnell, M.M.; Hess Fischl, A.; Maryniuk, M.D.; Siminerio, L.; Vivian, E. Diabetes self-management education and support in type 2 diabetes: A joint position statement of the American Diabetes Association, the American Association of Diabetes Educators, and the Academy of Nutrition and Dietetics. Diabetes Educ. 2017, 43, 40–53. [Google Scholar] [CrossRef]
- Cornell, S.; McKoy, J.M.; Letassy, N.; Haas, L.; Boren, S.A.; Fitzner, K.A.; Quintana, M. Taking medication in diabetes self-management: Issues and recommendations for reducing barriers. Am. J. Pharm. Benefits 2011, 3, 263–271. [Google Scholar]
- Tavares, N.U.L.; Bertoldi, A.D.; Thume, E.; Facchini, L.A.; França, G.V.A.D.; Mengue, S.S. Factors associated with low adherence to medication in older adults. Rev. De Saude Publica 2013, 47, 1092–1101. [Google Scholar] [CrossRef]
- Tiv, M.; Viel, J.F.; Mauny, F.; Eschwege, E.; Weill, A.; Fournier, C.; Fagot-Campagna, A.; Penfornis, A. Medication adherence in type 2 diabetes: The ENTRED study 2007, a French population-based study. PLoS ONE 2012, 7, e32412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinho, F.S.; Moram, C.; Rodrigues, P.C.; Leite, N.C.; Salles, G.F.; Cardoso, C.R. Treatment adherence and its associated factors in patients with type 2 diabetes: Results from the Rio de Janeiro type 2 diabetes cohort study. J. Diabetes Res. 2018, 2018, 8970196. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Male (n = 186) | Female (n = 157) | Total (n = 343) | |||
|---|---|---|---|---|---|---|
| n | (%) | n | (%) | n | (%) | |
| Age, years mean (SD) | 57.1 ± 11.4 | 54.3 ± 11.4 | 55.8 ± 11.5 | |||
| Ethnicity | ||||||
| Newar | 91 | (48.9) | 77 | (49.0) | 168 | (49.0) |
| Brahmin/Chhetri | 68 | (36.6) | 60 | (38.2) | 128 | (37.3) |
| Other | 27 | (14.5) | 20 | (12.7) | 47 | (13.7) |
| Marital Status | ||||||
| Currently married | 179 | (96.2) | 129 | (82.2) | 308 | (89.8) |
| Not currently married | 7 | (3.8) | 28 | (17.8) | 35 | (10.2) |
| Education | ||||||
| No formal education | 28 | (15.1) | 100 | (63.7) | 128 | (37.3) |
| School Leaving Certificate (SLC) | 112 | (60.2) | 49 | (31.2) | 161 | (47.0) |
| Above SLC | 46 | (24.7) | 8 | (5.1) | 54 | (15.7) |
| Occupation | ||||||
| Housewife | 0 | (0.0) | 98 | (62.4) | 98 | (28.6) |
| Business | 64 | (34.4) | 11 | (7.0) | 75 | (21.9) |
| Agriculture | 44 | (23.7) | 30 | (19.1) | 74 | (21.6) |
| Office (professional) | 29 | (15.6) | 5 | (3.2) | 34 | (9.9) |
| Unemployed | 19 | (10.2) | 5 | (3.2) | 24 | (7.0) |
| Other occupation | 30 | (16.1) | 8 | (5.1) | 38 | (11.0) |
| Residency * | ||||||
| Urban | 164 | (90.6) | 132 | (88) | 296 | (89.4) |
| Rural | 17 | (9.4) | 18 | (12.0) | 35 | (10.6) |
| Characteristics | Male (n = 186) | Female (n = 157) | Total (n = 343) | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Types of diabetes medicines | ||||||
| OHA | 153 | (82.3) | 136 | (86.6) | 289 | (84.3) |
| OHA and insulin | 22 | (11.8) | 16 | (10.2) | 38 | (11.0) |
| Insulin only | 11 | (5.9) | 5 | (3.2) | 16 | (4.7) |
| Medicine intake, years Median (IQR) | 3 (1, 6) | 2.5 (1, 6) | 3 (1, 6) | |||
| MMAS-8 (© 2006 Donald E. Morisky) Mean (SD) 1 | 7.4 ± 0.9 | 7.3 ± 1 | 7.4 ± 1 | |||
| Financial support for diabetes medicine * | ||||||
| Self | 132 | (76.3) | 27 | (18.5) | 159 | (49.8) |
| Family member | 41 | (23.7) | 119 | (81.5) | 160 | (50.2) |
| Immediate family member with diabetes | ||||||
| Yes | 29 | (15.6) | 22 | (14) | 51 | (14.9) |
| No | 157 | (84.4) | 135 | (86) | 292 | (85.1) |
| Attendance diabetes counselling | ||||||
| Yes | 74 | (39.8) | 70 | (44.6) | 144 | (42) |
| No | 112 | (60.2) | 87 | (55.4) | 199 | (58) |
| Duration of doctor–patient interaction, minutes mean (SD) | 8.8 ± 5.7 | 8.3 ± 3.9 | 8.6 ± 4.9 | |||
| Hypertension | ||||||
| Yes | 100 | (53.8) | 63 | (40.1) | 163 | (47.5) |
| No | 86 | (46.2) | 94 | (59.9) | 180 | (52.5) |
| Self-reported chronic complications | ||||||
| Yes | 20 | (10.8) | 9 | (5.8) | 29 | (8.5) |
| No | 165 | (89.2) | 147 | (94.2) | 312 | (91.5) |
| Characteristics | Model 1 | Model 2 ** | Model 3 *** | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Bivariate Analysis | Adjusted for Sociodemographic Variables | Adjusted for Sociodemographic & Clinical History | |||||||
| (n = 343) | (n = 343) | (n = 343) | |||||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age, years | 0.99 | (0.97, 1.01) | 0.28 | 0.99 | (0.97, 1.01) | 0.40 | 0.99 | (0.97, 1.02) | 0.73 |
| Education | |||||||||
| No formal education | Ref | Ref | Ref | ||||||
| Formal education | 2.43 | (1.55, 3.81) | <0.001 | 2.36 | (1.32, 4.23) | <0.001 | 2.43 | (1.34, 4.39) | 0.003 |
| Occupation | |||||||||
| Unemployed | Ref | Ref | Ref | ||||||
| Employed | 1.19 | (0.76, 1.88) | 0.44 | 0.71 | (0.39, 1.29) | 0.26 | 0.70 | (0.38, 1.29) | 0.25 |
| Medicine intake duration, Years (nat.log) | 1.00 | (0.95, 1.04) | 0.85 | - | - | - | 0.91 | (0.73, 1.13) | 0.41 |
| Attendance diabetes counseling | |||||||||
| No | Ref | Ref | |||||||
| Yes | 1.78 | (1.14, 2.79) | 0.01 | - | - | - | 1.76 | (1.02, 3.04) | 0.04 |
| Diabetes medicine types | |||||||||
| Only OHA | Ref | Ref | |||||||
| Insulin or Insulin with OHA | 1.34 | (0.73, 2.47) | 0.35 | - | - | - | 1.28 | (0.60,2.73) | 0.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shakya, P.; Shrestha, A.; Karmacharya, B.M.; Morisky, D.E.; Kulseng, B.E. Factors Associated with Medication Adherence among Patients with Type 2 Diabetes Mellitus: A Hospital-Based Cross-Sectional Study in Nepal. Int. J. Environ. Res. Public Health 2023, 20, 1537. https://doi.org/10.3390/ijerph20021537
Shakya P, Shrestha A, Karmacharya BM, Morisky DE, Kulseng BE. Factors Associated with Medication Adherence among Patients with Type 2 Diabetes Mellitus: A Hospital-Based Cross-Sectional Study in Nepal. International Journal of Environmental Research and Public Health. 2023; 20(2):1537. https://doi.org/10.3390/ijerph20021537
Chicago/Turabian StyleShakya, Pushpanjali, Archana Shrestha, Biraj Man Karmacharya, Donald E. Morisky, and Bård Eirik Kulseng. 2023. "Factors Associated with Medication Adherence among Patients with Type 2 Diabetes Mellitus: A Hospital-Based Cross-Sectional Study in Nepal" International Journal of Environmental Research and Public Health 20, no. 2: 1537. https://doi.org/10.3390/ijerph20021537