
Microarray Profiling of Differentially Expressed Genes in Coronary Artery Bypass Grafts of High-Risk Patients with Postoperative Cognitive Dysfunctions
 , ,
, ,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients Selection
2.2. Neurocognitive Assessment
2.3. Data Collection
2.4. RNA Extraction
2.5. Sample Selection and Microarray Analysis
2.6. Statistical Analysis
3. Results
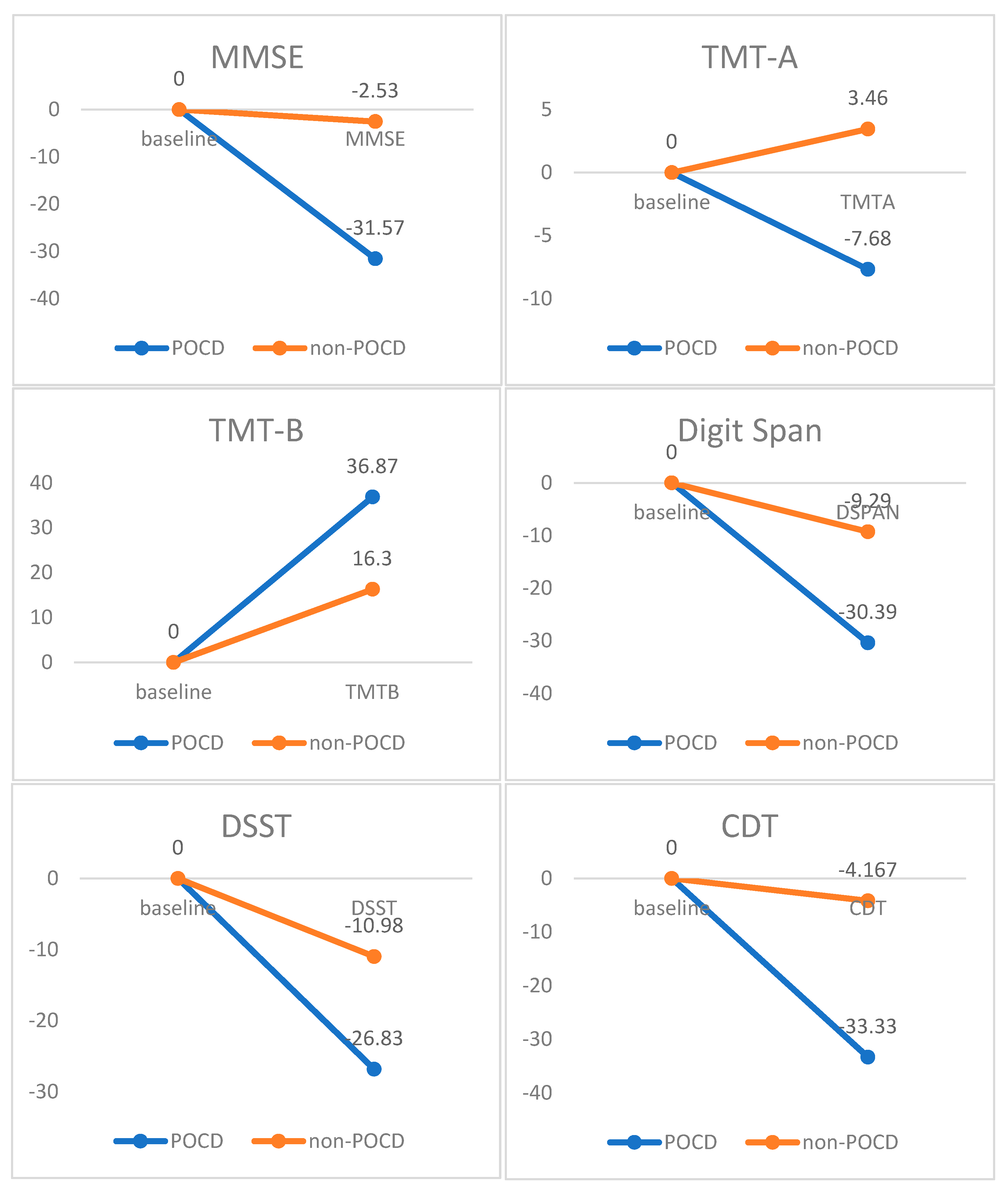
3.1. Neurocognitive Assessment
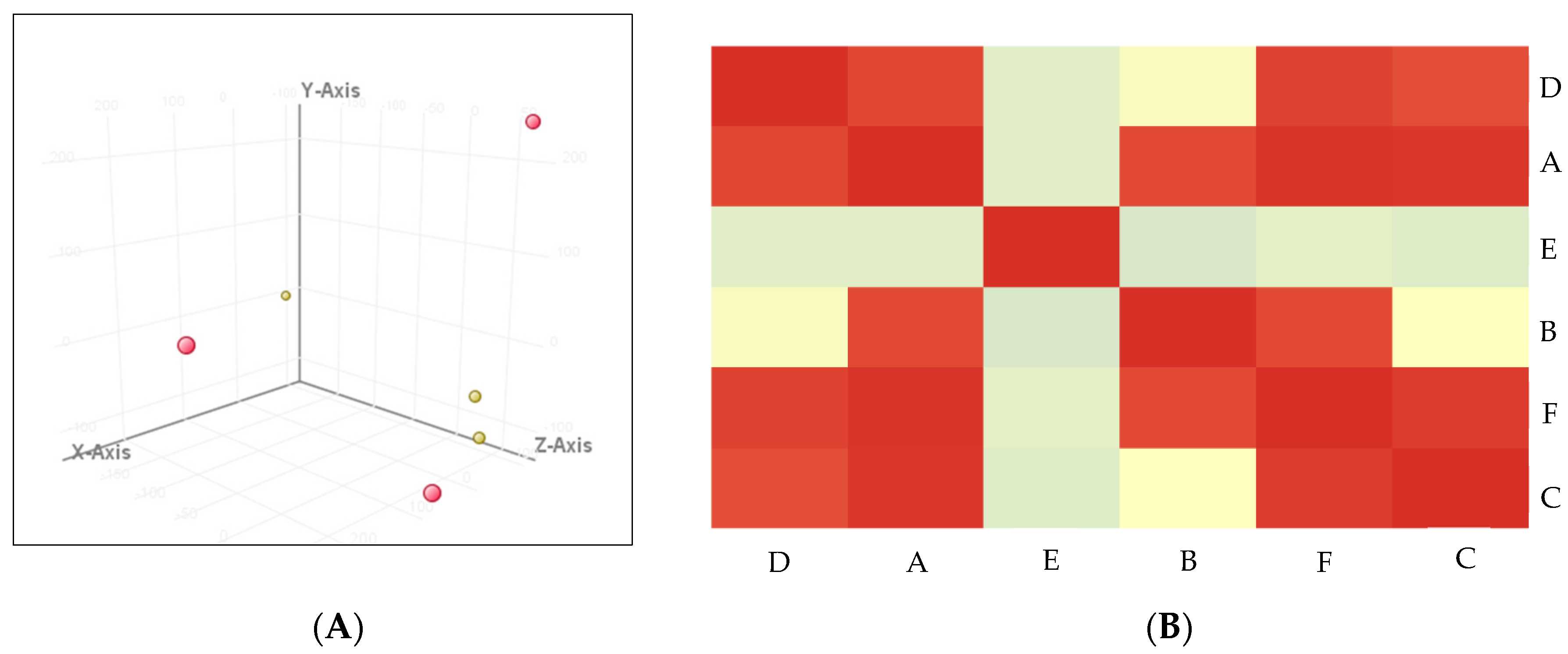
3.2. Samples Quality Detection
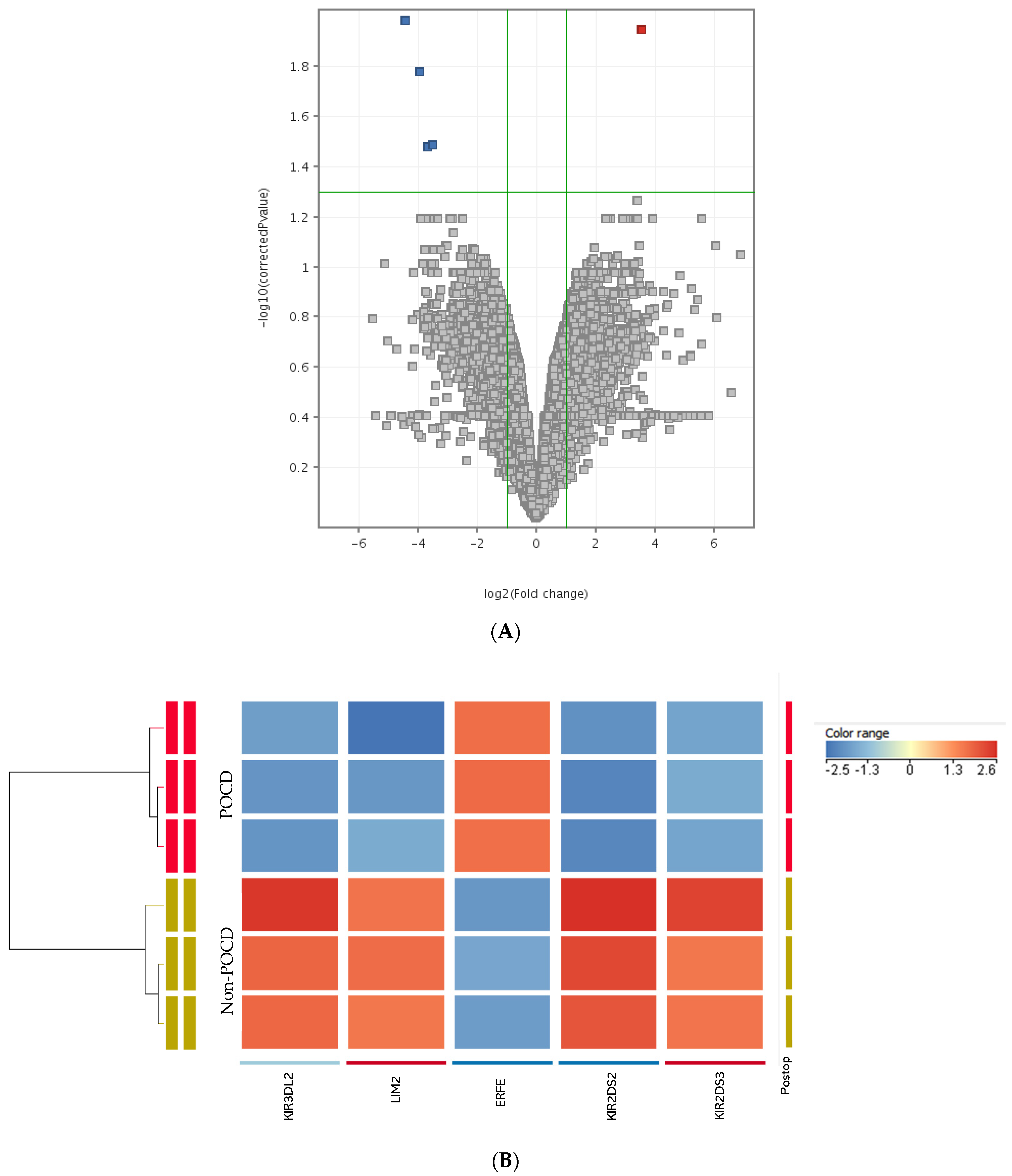
3.3. Differentially Expressed Genes
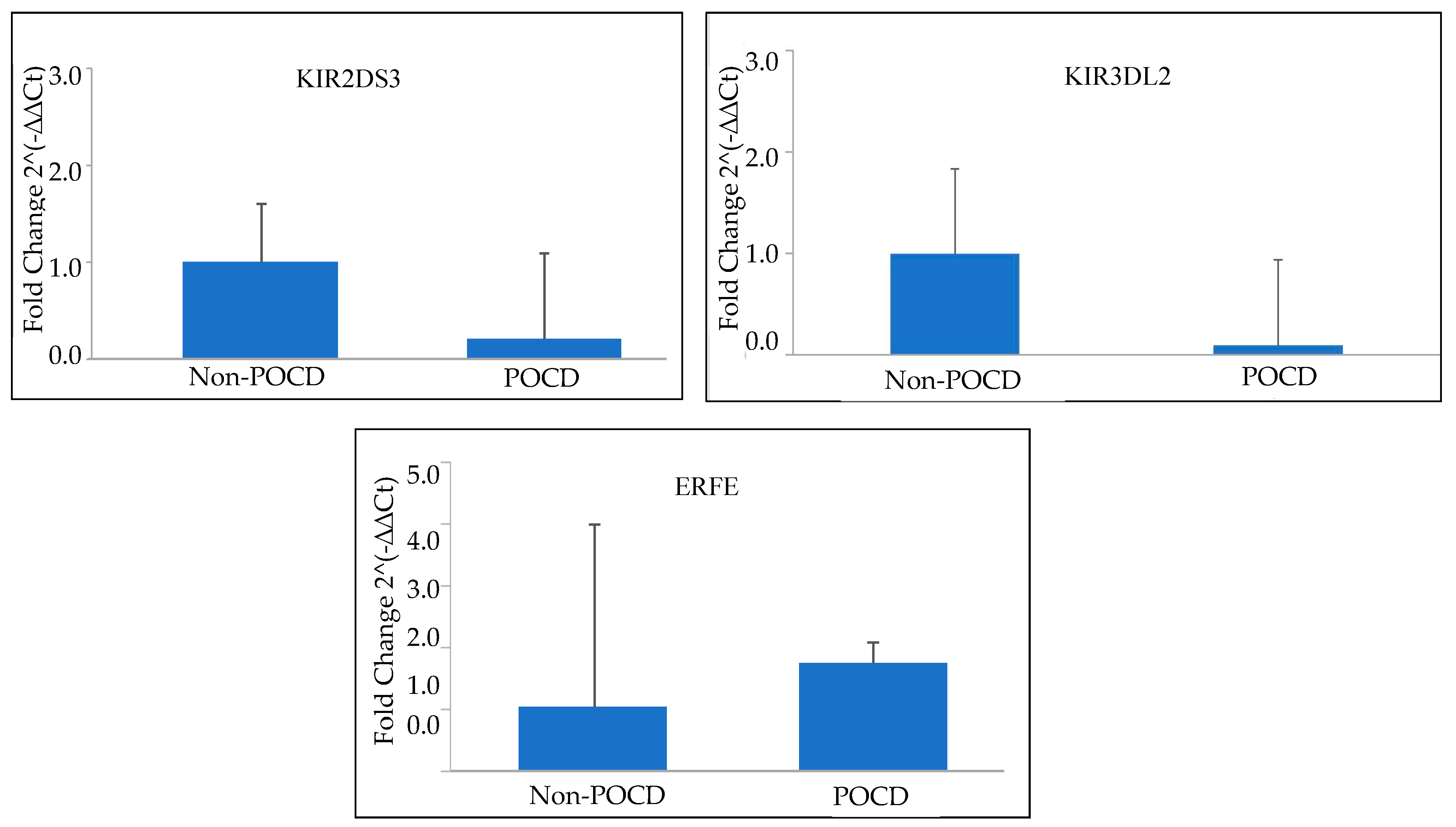
3.4. Quantitative RT-PCR Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| POCD | Postoperative Cognitive Dysfunction |
| RT-PCR | Real-Time Polymerase Chain Reaction |
| CABG | Coronary Artery Bypass Graft |
| RNA | Ribonucleic Acid |
| MMSE | Mini–Mental State Examination |
| TMT | Trail Making Test |
| DSST | Digit Symbol Substitution Test |
| CDT | Clock Drawing Test |
| ERFE | Erythroferrone |
| KIR | Killer Immunoglobulin-like Receptor |
| NK | Natural Killer |
| PD | Parkinson’s Disease |
References
- Evered, L.; Silbert, B.; Knopman, D.S.; Scott, D.A.; DeKosky, S.T.; Rasmussen, L.S.; Oh, E.S.; Crosby, G.; Berger, M.; Eckenhoff, R.G. Nomenclature Consensus Working Group. Recommendations for the nomenclature of cognitive change associated with anaesthesia and surgery. Anesthesiology 2018, 129, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Nemeth, E.; Vig, K.; Racz, K.; Koritsanszky, K.B.; Ronkay, K.I.; Hamvas, F.P.; Gal, J. Influence of the postoperative inflammatory response on cognitive decline in elderly patients undergoing on-pump cardiac surgery: A controlled, prospective observational study. BMC Anesth. 2017, 17, 113. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Xie, G.; Zhang, K.; Song, S.; Song, F.; Jin, Y.; Fang, X. Dexmedetomidine vs. propofol sedation reduces delirium in patients after cardiac surgery: A meta-analysis with trial sequential analysis of randomized controlled trials. J. Crit. Care 2017, 38, 190–196. [Google Scholar] [CrossRef]
- Duan, X.; Zhu, T.; Chen, C.; Zhang, G.; Zhang, J.; Wang, L.; Wang, X. Serum glial cell line–derived neurotrophic factor levels and postoperative cognitive dysfunction after surgery for rheumatic heart disease. J. Thorac. Cardiovasc. Surg. 2018, 155, 958–965. [Google Scholar] [CrossRef] [Green Version]
- Pappa, M.; Theodosiadis, N.; Tsounis, A.; Sarafis, P. Pathogenesis and treatment of post-operative cognitive dysfunction. Electron. Physician 2017, 9, 3768–3775. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Zhu, Y.; Kang, Y.; Qin, S.; Chai, J. Neuroinflammation as the underlying mechanism of postoperative cognitive dysfunction and therapeutic strategies. Front. Cell Neurosci. 2022, 16, 843069. [Google Scholar] [CrossRef] [PubMed]
- He, B.; Wang, J. METTL3 regulates hippocampal gene transcription via N6-methyladenosine methylation in sevoflurane-induced postoperative cognitive dysfunction mouse. Aging 2021, 13, 23108–23118. [Google Scholar] [CrossRef]
- Schenning, K.J.; Holden, S.; Davis, B.A.; Mulford, A.; Nevonen, K.A.; Quinn, J.F.; Raber, J.; Carbone, L.; Alkayed, N.J. Gene-specific DNA methylation linked to postoperative cognitive dysfunction in apolipoprotein E3 and E4 Mice. J. Alzheimers Dis. 2021, 83, 1251–1268. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, Y.X.; Xiao, Q.X.; Liu, Q.; Deng, R.; Bian, J.; Yu, F.X. Microarray expression profiles of lncRNAs and mRNAs in postoperative cognitive dysfunction. Front. Neurosci. 2018, 12, 694. [Google Scholar] [CrossRef]
- Skvarc, D.R.; Berk, M.; Byrne, L.K.; Dean, O.M.; Dodd, S.; Lewis, M.; Gray, L. Post-operative cognitive dysfunction: An exploration of the inflammatory hypothesis and novel therapies. Neurosci. Biobehav. Rev. 2018, 84, 116–133. [Google Scholar] [CrossRef]
- Yu, H.; Dong, R.; Lu, Y.; Yang, X.; Chen, C.; Zhang, Z.; Peng, M. Shortterm postoperative cognitive dysfunction and inflammatory response in patients undergoing cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: A pilot study. Mediat. Inflamm. 2017, 2017, 3605350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.; Mickey, W.P.; Koch, W.H. Clinical applications of microarray-based diagnostic tests. Biotechniques 2005, 39, S557–S582. [Google Scholar] [CrossRef]
- Yazit, N.A.; Juliana, N.; Das, S.; Teng, N.I.; Fahmy, N.M.; Azmani, S.; Kadiman, S. Association of micro RNA and postoperative cognitive dysfunction: A review. Mini Rev. Med. Chem. 2020, 20, 1781–1790. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Su, P.; Liu, Y.; Zhang, X.; Yan, J.; An, X.; Gu, S. Abnormal expression of circRNA_089763 in the plasma exosomes of patients with post-operative cognitive dysfunction after coronary artery bypass grafting. Mol. Med. Rep. 2019, 20, 2549–2562. [Google Scholar] [CrossRef] [Green Version]
- Zarina, Z.A.; Zahiruddin, O.; Che, W.A. Validation of Malay mini-mental state examination. Malays. J. Psychiatry 2007, 16, 16–19. [Google Scholar]
- Jaeger, J. Digit symbol substitution test: The case for sensitivity over specificity in neuropsychological testing. J. Clin. Psychopharmacol. 2018, 38, 513. [Google Scholar] [CrossRef]
- Ibrahim, N.M.; Shohaimi, S.; Chong, H.T.; Rahman, A.H.A.; Razali, R.; Esther, E.; Basri, H.B. Validation study of the Mini-Mental State Examination in a Malay-speaking elderly population in Malaysia. Dement. Geriatr. Cogn. Disord. 2009, 27, 247–253. [Google Scholar] [CrossRef]
- Greaves, D.; Psaltis, P.J.; Ross, T.J.; Davis, D.; Smith, A.E.; Boord, M.S.; Keage, H.A. Cognitive outcomes following coronary artery bypass grafting: A systematic review and meta-analysis of 91,829 patients. Int. J. Cardiol. 2019, 289, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Greaves, D.; Psaltis, P.J.; Davis, D.H.; Ross, T.J.; Ghezzi, E.S.; Lampit, A.; Keage, H.A. Risk factors for delirium and cognitive decline following coronary artery bypass grafting surgery: A systematic review and meta-analysis. J. Am. Heart Assoc. 2020, 9, e017275. [Google Scholar] [CrossRef]
- Newman, M.F.; Kirchner, J.L.; Phillips-Bute, B.; Gaver, V.; Grocott, H.; Jones, R.H.; Blumenthal, J.A. Longitudinal assessment of neurocognitive function after coronary-artery bypass surgery. N. Engl. J. Med. 2001, 344, 395–402. [Google Scholar] [CrossRef]
- Harrington, M.B.; Kraft, M.; Grande, L.J.; Rudolph, J.L. Independent association between preoperative cognitive status and discharge location after cardiac surgery. Am. J. Crit. Care 2011, 20, 129–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Z.; Wang, B.; Hu, S.; Zhang, C.; Ma, X.; Qi, Y. Genetic variations in GJA3, GJA8, LIM2, and age-related cataract in the Chinese population: A mutation screening study. Mol. Vis. 2011, 17, 621. [Google Scholar] [PubMed]
- Srole, D.N.; Ganz, T. Erythroferrone structure, function, and physiology: Iron homeostasis and beyond. J. Cell Physiol. 2021, 236, 4888–4901. [Google Scholar] [CrossRef] [PubMed]
- Coffey, R.; Ganz, T. Erythroferrone: An erythroid regulator of hepcidin and iron metabolism. Hemasphere 2018, 2, e35. [Google Scholar] [CrossRef]
- Juliana, N.; Abu Yazit, N.A.; Kadiman, S.; Muhammad Hafidz, K.; Azmani, S.; Mohd Fahmi Teng, N.I.; Das, S. Intraoperative cerebral oximetry in open heart surgeries reduced postoperative complications: A retrospective study. PLoS ONE 2021, 16, e0251157. [Google Scholar] [CrossRef]
- Wang, L.; Lang, Z.; Gao, H.; Liu, Y.; Dong, H.; Sun, X. The relationship between the incidence of postoperative cognitive dysfunction and intraoperative regional cerebral oxygen saturation after cardiovascular surgery: A systematic review and meta-analysis of randomized controlled trials. Rev. Cardiovasc. Med. 2022, 23, 388. [Google Scholar] [CrossRef]
- Navarro, A.G.; Kmiecik, J.; Leiss, L.; Zelkowski, M.; Engelsen, A.; Bruserud, Ø.; Chekenya, M. NK cells with KIR2DS2 immunogenotype have a functional activation advantage to efficiently kill glioblastoma and prolong animal survival. J. Immunol. 2014, 193, 6192–6206. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, R.; Bortolotti, D.; Gentili, V.; Rotola, A.; Bolzani, S.; Caselli, E.; Di Luca, D. Kir2ds2/kir2dl2/hla-c1 haplotype is associated with Alzheimer’s disease: Implication for the role of herpesvirus infections. J. Alzheimers Dis. 2019, 67, 1379–1389. [Google Scholar] [CrossRef]
- Earls, R.H.; Lee, J.K. The role of natural killer cells in Parkinson’s disease. Exp. Mol. Med. 2020, 52, 1517–1525. [Google Scholar] [CrossRef]
- Garofalo, S.; Cocozza, G.; Porzia, A.; Inghilleri, M.; Raspa, M.; Scavizzi, F.; Limatola, C. Natural killer cells modulate motor neuron-immune cell cross talk in models of Amyotrophic Lateral Sclerosis. Nat. Commun. 2020, 11, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Shahsavar, F.; Tajik, N.; Entezami, K.Z.; Radjabzadeh, M.F.; Asadifar, B.; Alimoghaddam, K.; Ghavamzadeh, A. KIR2DS3 is associated with protection against acute myeloid leukemia. Iran J. Immunol. 2010, 7, 8–17. [Google Scholar] [PubMed]
- Hurabielle, C.; Thonnart, N.; Ram-Wolff, C.; Sicard, H.; Bensussan, A.; Bagot, M.; Marie-Cardine, A. Usefulness of KIR3DL2 to Diagnose, Follow-Up, and Manage the Treatment of Patients with Sézary Syndrome. Clin. Cancer Res. 2017, 23, 3619–3627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, S.; Miranda, C.J.; Braun, L.; Meyer, K.; Frakes, A.E.; Ferraiuolo, L.; Kaspar, B.K. Major histocompatibility complex class I molecules protect motor neurons from astrocyte-induced toxicity in amyotrophic lateral sclerosis. Nat. Med. 2016, 22, 397–403. [Google Scholar] [CrossRef] [Green Version]
- Kats, S.; Schönberger, J.P.; Brands, R.; Seinen, W.; van Oeveren, W. Endotoxin release in cardiac surgery with cardiopulmonary bypass: Pathophysiology and possible therapeutic strategies. An update. Eur. J. Cardiothorac. Surg. 2011, 39, 451–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paparella, D.; Yau, T.M.; Young, E. Cardiopulmonary bypass induced inflammation: Pathophysiology and treatment. An update. Eur. J. Cardiothorac. Surg. 2002, 21, 232–244. [Google Scholar] [CrossRef] [Green Version]
- Waggoner, S.N.; Kumar, V. Evolving role of 2B4/CD244 in T and NK cell responses during virus infection. Front. Immunol. 2012, 3, 377. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Non-POCD (n = 38), Mean ± SD/n (%) | POCD (n = 8), Mean ± SD/n (%) | p-Value |
|---|---|---|---|
| Age (years) | 56.21 ± 13.191 | 66.00 ± 5.976 | 0.047 * |
| Gender | |||
| Male | 23 (79.3) | 6 (20.7) | 0.366 |
| Female | 15 (88.2) | 2 (11.8) | |
| Education (years) | 11.82 ± 2.710 | 8.00 ± 4.036 | 0.002 * |
| Body Mass Index (BMI) | 26.44 ± 4.199 | 28.34 ± 13.07 | 2.44 |
| Bypass time (minutes) | 127.24 ± 72.431 | 123.86 ± 26.55 | 0.905 |
| Cross Clamp time (minutes) | 99.35 ± 63.141 | 84.86 ± 28.956 | 0.559 |
| Preoperative scores | |||
| MMSE | 28.34 ± 2.096 | 25.50 ± 2.563 | 0.002 * |
| TMT-A (seconds) | 49.16 ± 26.054 | 69.38 ± 29.306 | 0.57 |
| TMT-B (seconds) | 107.53 ± 56.125 | 162.50 ± 62.452 | 0.017 * |
| Digit Span | 13.63 ± 3.183 | 10.75 ± 3.370 | 0.026 * |
| DSST | 53.39 ± 16.839 | 29.75 ± 14.469 | 0.001 * |
| CDT | 1.92 ± 0.273 | 1.75 ± 0.707 | 0.250 |
| Postoperative scores | |||
| MMSE | 27.63 ± 2.454 | 18.00 ± 7.483 | <0.001 ** |
| TMT-A (seconds) | 47.8 ± 22.512 | 71.80 ± 47.484 | 0.064 |
| TMT-B (seconds) | 123.31 ± 71.160 | 184.20 ± 45.069 | 0.072 |
| Digit Span | 12.08 ± 3.631 | 6.88 ± 4.853 | 0.001 * |
| DSST | 47.56 ± 19.166 | 23.14 ± 14.565 | 0.003 * |
| CDT | 1.86 ± 0.487 | 1.14 ± 1.069 | 0.007 * |
| Samples | Purity | Concentration | RIN Number |
|---|---|---|---|
| A | 1.832 | 43.2 | 8.80 |
| B | 1.855 | 61.6 | 6.80 |
| C | 1.857 | 46.8 | 8.00 |
| D | 1.892 | 25.2 | 8.80 |
| E | 1.842 | 135.6 | 8.00 |
| F | 1.816 | 63.2 | 8.40 |
| No | Fold Change | p-Value | Regulation | Gene Symbol | Description |
|---|---|---|---|---|---|
| 1 | 11.606633 | 0.01127 | Up | ERFE | erythroferrone |
| 2 | −11.387419 | 0.03253 | Down | KIR2DS2 | killer cell immunoglobulin-like receptor, two Ig domains, and short cytoplasmic tail 2 |
| 3 | −12.647894 | 0.03299 | Down | LIM2 | lens intrinsic membrane protein 2 |
| 4 | −15.381129 | 0.01660 | Down | KIR3DL2 | killer cell immunoglobulin-like receptor, three Ig domains, and long cytoplasmic tail 2 |
| 5 | −21.730328 | 0.01028 | Down | KIR2DS3 | killer cell immunoglobulin-like receptor, two Ig domains, and short cytoplasmic tail 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yazit, N.A.A.; Juliana, N.; Kadiman, S.; Hafidz, K.M.; Mohd Fahmi Teng, N.I.; Abdul Hamid, N.; Effendy, N.; Azmani, S.; Abu, I.F.; Aziz, N.A.S.A.; et al. Microarray Profiling of Differentially Expressed Genes in Coronary Artery Bypass Grafts of High-Risk Patients with Postoperative Cognitive Dysfunctions. Int. J. Environ. Res. Public Health 2023, 20, 1457. https://doi.org/10.3390/ijerph20021457
Yazit NAA, Juliana N, Kadiman S, Hafidz KM, Mohd Fahmi Teng NI, Abdul Hamid N, Effendy N, Azmani S, Abu IF, Aziz NASA, et al. Microarray Profiling of Differentially Expressed Genes in Coronary Artery Bypass Grafts of High-Risk Patients with Postoperative Cognitive Dysfunctions. International Journal of Environmental Research and Public Health. 2023; 20(2):1457. https://doi.org/10.3390/ijerph20021457
Chicago/Turabian StyleYazit, Noor Anisah Abu, Norsham Juliana, Suhaini Kadiman, Kamilah Muhammad Hafidz, Nur Islami Mohd Fahmi Teng, Nazefah Abdul Hamid, Nadia Effendy, Sahar Azmani, Izuddin Fahmy Abu, Nur Adilah Shuhada Abd Aziz, and et al. 2023. "Microarray Profiling of Differentially Expressed Genes in Coronary Artery Bypass Grafts of High-Risk Patients with Postoperative Cognitive Dysfunctions" International Journal of Environmental Research and Public Health 20, no. 2: 1457. https://doi.org/10.3390/ijerph20021457