
Recreational Skydiving—Really That Dangerous? A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
- (1)
- What are the most common injuries discussed in current literature?
- (2)
- What is the frequency of injuries in relation to the number of completed jumps?
- (3)
- In what phase of the jump do most of the injuries occur?
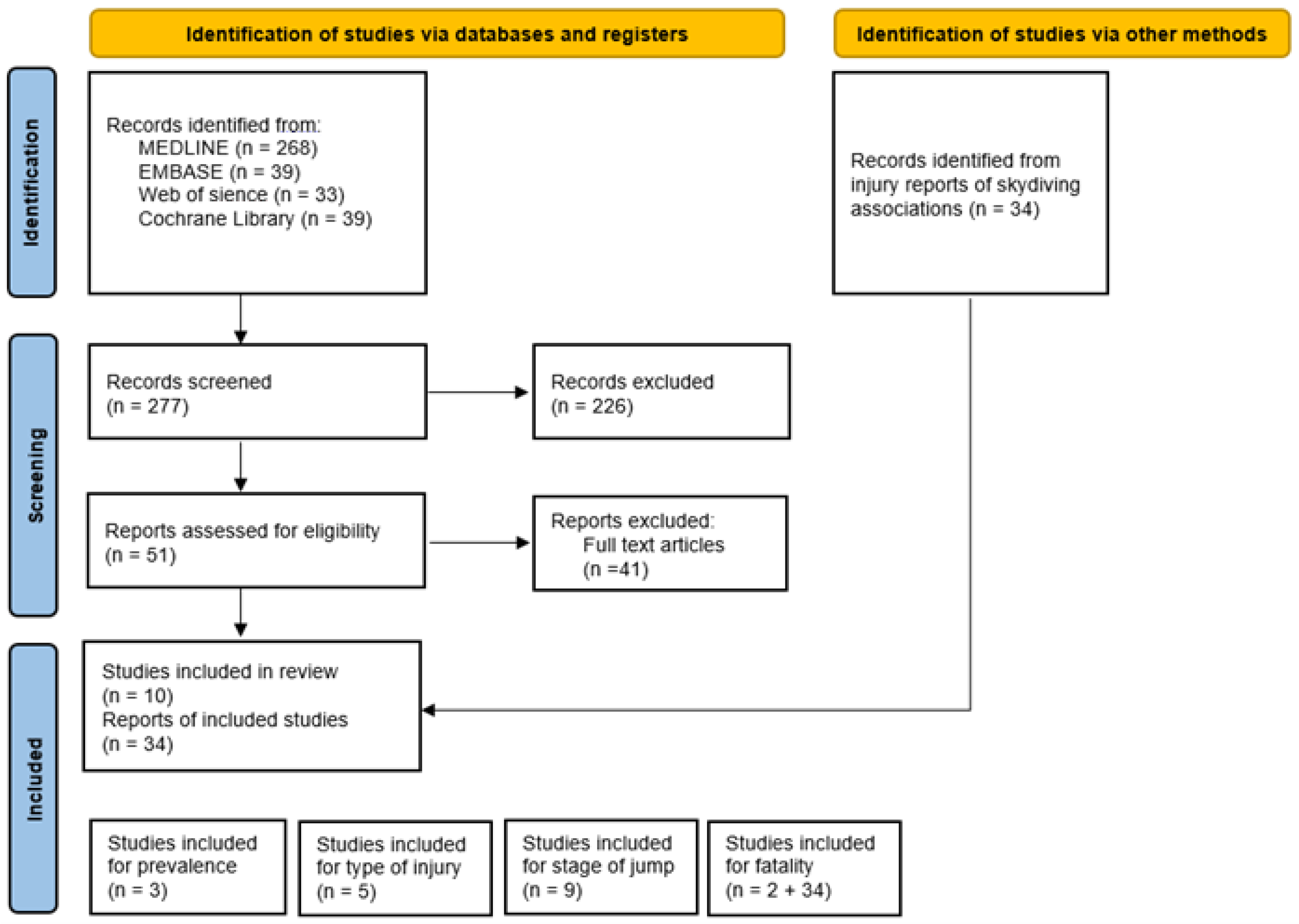
2. Materials and Methods
3. Results
3.1. Most Common Injuries
3.2. Jump Phase

{kind=link}
{kind=link}
| Title | Author | Country | Year | PMID | Stage | Subjects | Jumps |
|---|---|---|---|---|---|---|---|
| Injuries in Swedish skydiving | Westman A [6] | Sweden | 2007 | 17224436 | Landing | n/a | 539,885 |
| Serious parasport injuries in Auckland, New Zealand. | Christey GR [3] | Australia | 2005 | 15796732 | Landing | 38 | n/a |
| The epidemiology of skydiving injuries: World Freefall Convention, 2000–2001 | Barrows TH [8] | USA | 2005 | 15657007 | Landing | 8976 | 117,000 |
| Parachuting injuries: A study of 110,000 sports jumps | Ellitsgaard N [7] | Denmark | 1987 | 3580720 | Landing | 143 | 110,000 |
| Are hook turns a major obstacle to safe skydiving? A study of skydiving fatalities in the United States from 1992 to 2005 | Vidovic M [13] | USA | 2007 | 18229535 | Landing | 439 | n/a |
| An analysis of U.S. parachuting fatalities: 2000–2004 | Hart CL [12] | USA | 2006 | 17326520 | Landing | 125 | n/a |
| A summary of U.S. skydiving fatalities: 1993–1999 | Griffith JD [11] | USA | 2002 | 12186229 | Incorrect procedures | 241 | n/a |
| Fatalities in Swedish skydiving. | Westman A [6] | Sweden | 2005 | 16039597 | No/Low reserve activation | n/a | 2,176,471 |
| Rise in landing-related skydiving fatalities | Hart CL [12] | USA | 2003 | 14620223 | Landing | n/a | n/a |
| Title | Author | Country | Year | PMID | Subjects | Jumps | Prevalence of Any Injury during a Jump |
|---|---|---|---|---|---|---|---|
| Injuries in Swedish skydiving | Westman A [6] | Sweden | 2007 | 17224436 | n/a | 539,885 | 0.0476% |
| The epidemiology of skydiving injuries: World Freefall Convention, 2000–2001 | Barrows TH [8] | USA | 2005 | 15657007 | 8976 | 117,000 | 0.1740% |
| Parachuting injuries: A study of 110,000 sports jumps | Ellitsgaard N [7] | Denmark | 1987 | 3580720 | 143 | 110,000 | 0.1409% |
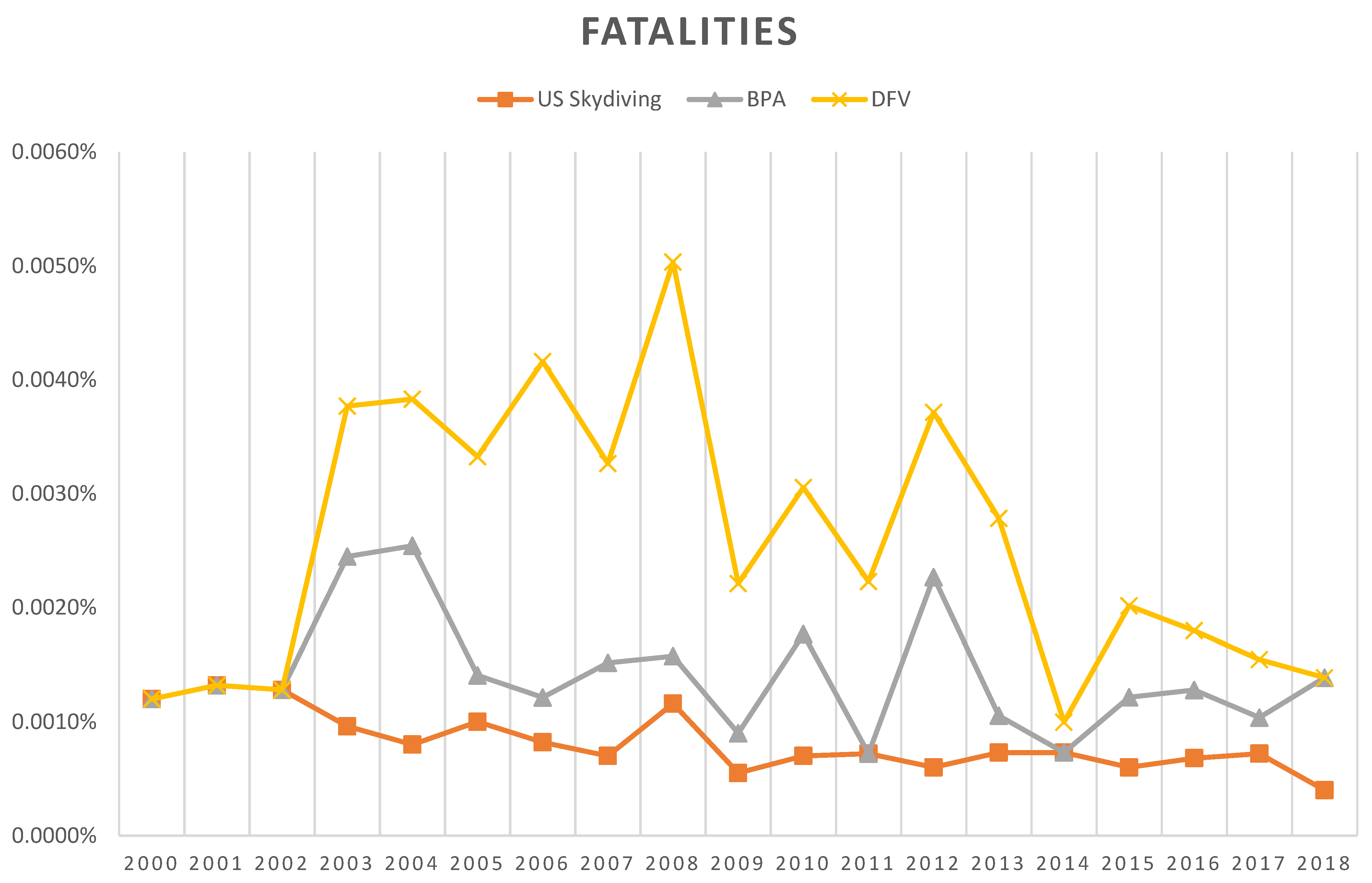
3.3. Prevalence of Accidents and Fatalities
4. Discussion
- The most common injuries were to the lumbar spine and lower extremities;
- Injuries occur at a rate of approximately 0.03% to 0.17% and fatalities in 3–10 fatalities per 1 million jumps;
- Injuries occur most commonly in the landing sequence.
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Injuries and Violence: The Facts 2014; World Health Organization: Geneva, Switzerland, 2014.
- Koordinationsgruppe für die Statistik der Unfallversicherung UVG (KSUV). Unfallstatisitk UVG 2018; Redaktion, Vertrieb und Auskünfte Sammelstelle für die Statistik der Unfallversicherung UVG (SSUV): Luzern, Switzerland, 2018. [Google Scholar]
- Christey, G.R. Serious parasport injuries in Auckland, New Zealand. Emerg. Med. Australas. 2005, 17, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Baluch, B.; Duffy, L.J. Defining Extreme Sport: Conceptions and Misconceptions. Front. Psychol. 2018, 9, 1974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coşkun Beyan, A.; Demiral, Y.; Dilek, B.; Alici, N.; Bediz, C.; Çimrin, A. Skydiving and the risk of cervical disc herniation. Int. J. Occup. Med. Environ. Health 2018, 31, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Westman, A.; Björnstig, U. Injuries in Swedish skydiving. Br. J. Sport. Med. 2007, 41, 356–364; discussion 364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ellitsgaard, N. Parachuting injuries: A study of 110,000 sports jumps. Br. J. Sport. Med. 1987, 21, 13–17. [Google Scholar] [CrossRef] [Green Version]
- Barrows, T.H.; Mills, T.J.; Kassing, S.D. The epidemiology of skydiving injuries: World freefall convention, 2000–2001. J. Emerg. Med. 2005, 28, 63–68. [Google Scholar] [CrossRef]
- Nilsson, J.; Fridén, C.; Burén, V.; Westman, A.; Lindholm, P.; Ang, B.O. Musculoskeletal pain and related risks in skydivers: A population-based survey. Aviat. Space Environ. Med. 2013, 84, 1034–1040. [Google Scholar] [CrossRef]
- Lee, C.T.; Williams, P.; Hadden, W.A. Parachuting for charity: Is it worth the money? A 5-year audit of parachute injuries in Tayside and the cost to the NHS. Injury 1999, 30, 283–287. [Google Scholar] [CrossRef]
- Griffith, J.D.; Hart, C.L. A summary of U.S. skydiving fatalities: 1993–1999. Percept. Mot. Ski. 2002, 94, 1089–1090. [Google Scholar] [CrossRef]
- Hart, C.L.; Griffith, J.D.; Randell, J.A. An analysis of U.S. parachuting fatalities: 2000–2004. Percept. Mot. Ski. 2006, 103, 896–900. [Google Scholar] [CrossRef]
- Vidovic, M.; Rugai, N. Are hook turns a major obstacle to safe skydiving? A study of skydiving fatalities in the United States from 1992 to 2005. Percept. Mot. Ski. 2007, 105, 795–802. [Google Scholar] [CrossRef]
- Hart, C.L.; Griffith, J.D. Rise in landing-related skydiving fatalities. Percept. Mot. Ski. 2003, 97, 390–392. [Google Scholar] [CrossRef]
- Westman, A.; Björnstig, U. Fatalities in Swedish skydiving. Accid. Anal. Prev. 2005, 37, 1040–1048. [Google Scholar] [CrossRef]
- Fer, C.; Guiavarch, M.; Edouard, P. Epidemiology of skydiving-related deaths and injuries: A 10-years prospective study of 6.2 million jumps between 2010 and 2019 in France. J. Sci. Med. Sport 2021, 24, 448–453. [Google Scholar] [CrossRef]
- Westman, A.; Sjöling, M.; Lindberg, A.; Björnstig, U. The SKYNET data: Demography and injury reporting in Swedish skydiving. Accid. Anal. Prev. 2010, 42, 778–783. [Google Scholar] [CrossRef]
- Nilsson, J.; Fridén, C.; Burén, V.; Ang, B.O. Development and validation of a web-based questionnaire for surveying skydivers. Aviat. Space Environ. Med. 2011, 82, 610–614. [Google Scholar] [CrossRef]
- Knapik, J.J.; Darakjy, S.; Swedler, D.; Amoroso, P.; Jones, B.H. Parachute ankle brace and extrinsic injury risk factors during parachuting. Aviat. Space Environ. Med. 2008, 79, 408–415. [Google Scholar] [CrossRef]
- Loebel, F.; Fekonja, L.; Vajkoczy, P.; Hecht, N. Hangman’s Fracture Caused by Parachute Opening Deceleration Captured on Video. World Neurosurg. 2018, 119, 389–393. [Google Scholar] [CrossRef]
- Powell, E.K.; Galvagno, S.M.; Lucero, J.M.; Simoncavage, M.; Koroll, N.; O’Neal, P.; Bystry, M.; Castaneda, J.; Tilney, P.V. A 47-Year-Old Man With a Spinal Cord Injury After a Parachute Jump. Air. Med. J. 2016, 35, 326–330. [Google Scholar] [CrossRef]
- Esser, S.M.; Baima, J.; Hirschberg, R. Falling for sport: A case report of skydiving and SCI. Curr. Sport. Med. Rep. 2013, 12, 7–10. [Google Scholar] [CrossRef]
- Abbo, M.; Hussain, K.; Ali, M.B. Blunt traumatic internal carotid artery dissection with delayed stroke in a young skydiver. BMJ Case Rep. 2013, 2013, bcr2012008412. [Google Scholar] [CrossRef] [PubMed]
- Kpodonu, J.; Wheatley, G.H., III; Ramaiah, V.G.; Diethrich, E.B. Endovascular management of a thoracic aortic disruption following failure of deployment of a parachute. Interact. Cardiovasc. Thorac. Surg. 2007, 6, 823–824. [Google Scholar] [CrossRef] [PubMed]
- Schipper, D. A 29-year-old man with dizziness and headache after skydiving. J. Emerg. Nurs. 2011, 37, 554–556. [Google Scholar] [CrossRef] [PubMed]
- Ejnisman, B.; de Figueiredo, E.A.; Terra, B.B.; Monteiro, G.C.; Pochini Ade, C.; Andreoli, C.V. Exact moment of bilateral scapular fracture during skydiving captured on video. Case Rep. 2011, 2011, bcr0920103351. [Google Scholar] [CrossRef] [Green Version]
- Bourghli, A.; Fabre, A. Proximal end clavicle fracture from a parachute jumping injury. Orthop. Traumatol. Surg. Res. OTSR 2012, 98, 238–241. [Google Scholar] [CrossRef] [Green Version]
- Davis, J.R.; Stepanek, J.; Fogarty, J.A. Fundamentals of Aerospace Medicine, 4th ed.; Wolters Kluwer Health Adis (ESP): Zurich, Switzerland, 2011. [Google Scholar]
- Rooks, T.F.; Novotny, B.L.; McGovern, S.M.; Winegar, A.; Shivers, B.L.; Brozoski, F.T. Evaluation of Head and Body Kinematics Experienced During Parachute Opening Shock. Mil. Med. 2021, 186, e1149–e1156. [Google Scholar] [CrossRef]
- Gladh, K.; Ang, B.O.; Lindholm, P.; Nilsson, J.; Westman, A. Decelerations and muscle responses during parachute opening shock. Aviat. Space Environ. Med. 2013, 84, 1205–1210. [Google Scholar] [CrossRef]
- Alevras, A.J.; Fuller, J.T.; Mitchell, R.; Lystad, R.P. Epidemiology of injuries in amateur boxing: A systematic review and meta-analysis. J. Sci. Med. Sport 2022, 25, 995–1001. [Google Scholar] [CrossRef]
- Furness, J.; McArthur, K.; Remnant, D.; Jorgensen, D.; Bacon, C.J.; Moran, R.W.; Hing, W.; Climstein, M. Traumatic surfing injuries in New Zealand: A descriptive epidemiology study. PeerJ 2021, 9, e12334. [Google Scholar] [CrossRef]


| Title | Author | Country | Year | PMID | 1. Most Injury | 2. Most Injury | 3. Most Injury | Subjects | Jumps |
|---|---|---|---|---|---|---|---|---|---|
| Injuries in Swedish skydiving | Westman A [6] | Sweden | 2007 | 17224436 | 51% lower extremities | 19% upper extremity | 18% spine | n/a | 539,885 |
| Parachuting injuries: a study of 110,000 sports jumps | Ellitsgaard N [7] | Denmark | 1987 | 3580720 | 59.7% lower extremities | 17% upper extremity | 10% spine | 143 | 110,000 |
| The epidemiology of skydiving injuries: World freefall convention, 2000–2001 | Barrows TH [8] | USA | 2005 | 15657007 | 47% extremity injury | 17.1% back injury | 12.9% lacerations | 8976 | 117,000 |
| Serious parasport injuries in Auckland, New Zealand. | Christey GR [3] | New Zealand | 2005 | 15796732 | 47% lower limb | 8% upper extremity | 6% thoracic spine | 38 | n/a |
| Musculoskeletal pain and related risks in skydivers: a population-based survey | Nilsson J [9] | Sweden | 2013 | 24261055 | 25% neck region | 16% shoulder | 10% thoracic spine | 658 | n/a |
| Reported Injuries | ||||||
|---|---|---|---|---|---|---|
| BPA | DFV | |||||
| Year | Jumps | Reported Injuries | Jumps | Reported Injuries | ||
| 2003 | 268,816 | 242 | 0.0900% | 302,760 | 77 | 0.0254% |
| 2004 | 229,565 | 180 | 0.0784% | 310,650 | 98 | 0.0315% |
| 2005 | 245,472 | 175 | 0.0713% | 260,800 | 65 | 0.0249% |
| 2006 | 253,994 | 219 | 0.0862% | 271,500 | 91 | 0.0335% |
| 2007 | 244,838 | 200 | 0.0817% | 286,000 | 87 | 0.0304% |
| 2008 | 240,426 | 165 | 0.0686% | 289,200 | 77 | 0.0266% |
| 2009 | 286,794 | 206 | 0.0718% | 304,700 | 85 | 0.0279% |
| 2010 | 280,752 | 223 | 0.0794% | 311,245 | 74 | 0.0238% |
| 2011 | 286,840 | 199 | 0.0694% | 331,410 | 93 | 0.0281% |
| 2012 | 299,921 | 168 | 0.0560% | 345,430 | 95 | 0.0275% |
| 2013 | 309,529 | 163 | 0.0527% | 346,815 | 82 | 0.0236% |
| 2014 | 344,607 | 168 | 0.0488% | 374,545 | 90 | 0.0240% |
| 2015 | 325,254 | 154 | 0.0473% | 374,620 | 10 | 0.0027% |
| 2016 | 333,955 | 163 | 0.0488% | 385,625 | 96 | 0.0249% |
| 2017 | 315,290 | 142 | 0.0450% | 393,200 | 83 | 0.0211% |
| 2018 | 303,882 | 144 | 0.0474% | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barthel, C.; Halvachizadeh, S.; Gamble, J.G.; Pape, H.-C.; Rauer, T. Recreational Skydiving—Really That Dangerous? A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 1254. https://doi.org/10.3390/ijerph20021254
Barthel C, Halvachizadeh S, Gamble JG, Pape H-C, Rauer T. Recreational Skydiving—Really That Dangerous? A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(2):1254. https://doi.org/10.3390/ijerph20021254
Chicago/Turabian StyleBarthel, Christiane, Sacha Halvachizadeh, Jamison G. Gamble, Hans-Christoph Pape, and Thomas Rauer. 2023. "Recreational Skydiving—Really That Dangerous? A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 2: 1254. https://doi.org/10.3390/ijerph20021254