
The Impact of COVID-19 on Pediatric Cardiac Arrest Outcomes: A Systematic Review and Meta-Analysis
 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results
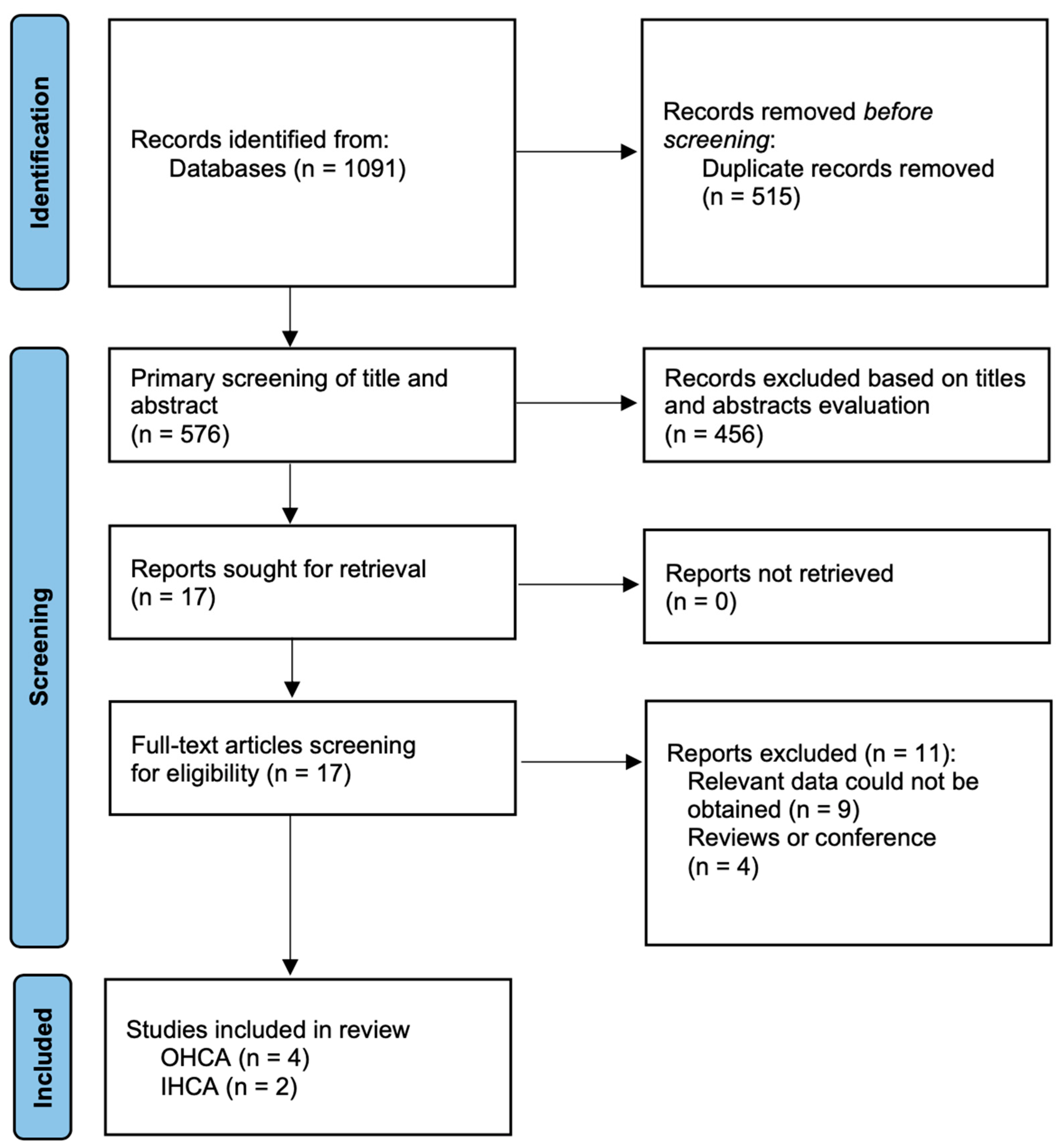
3.1. Search Results and Study Characteristics
3.2. Out-of-Hospital Cardiac Arrest
3.3. In-Hospital Cardiac Arrest
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Dzieciatkowski, T.; Szarpak, L.; Filipiak, K.J.; Jaguszewski, M.; Ladny, J.R.; Smereka, J. COVID-19 challenge for modern medicine. Cardiol. J. 2020, 27, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Smereka, J.; Szarpak, L.; Filipiak, K.J. Modern medicine in COVID-19 era. Disaster Emerg. Med. J. 2020, 5, 103–105. [Google Scholar] [CrossRef] [Green Version]
- Machhi, J.; Herskovitz, J.; Senan, A.M.; Dutta, D.; Nath, B.; Oleynikov, M.D.; Blomberg, W.R.; Meigs, D.D.; Hasan, M.; Patel, M.; et al. The natural history, pathobiology, and clinical manifestations of SARS-CoV-2 infections. J. Neuroimmune Pharmacol. 2020, 15, 359–386. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization [WHO]. Archived: WHO Timeline-COVID-19. 2020. Available online: https://www.who.int/news-room/detail/27-04-2020-who-timeline---covid-19 (accessed on 24 September 2020).
- Stokes, E.K.; Zambrano, L.D.; Anderson, K.N.; Marder, E.P.; Raz, K.M.; El Burai, F.S.; Tie, Y.; Fullerton, K.E. Coronavirus Disease 2019 Case Surveillance-United States, January 22-May 30, 2020. MMWR Morb. Mortal. Wkly Rep. 2020, 69, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Resource Center: Maps and Trends. 2020. Available online: https://coronavirus.jhu.edu/data. (accessed on 21 October 2022).
- Scquizzato, T.; Landoni, G.; Paoli, A.; Lembo, R.; Fominskiy, E.; Kuzovlev, A.; Likhvantsev, V.; Zangrillo, A. Effects of COVID-19 pandemic on out-of-hospital cardiac arrests: A systematic review. Resuscitation 2020, 157, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Lim, Z.J.; Ponnapa Reddy, M.; Afroz, A.; Billah, B.; Shekar, K.; Subramaniam, A. Incidence and outcome of out-of-hospital cardiac arrests in the COVID-19 era: A systematic review and meta-analysis. Resuscitation 2020, 157, 248–258. [Google Scholar] [CrossRef] [PubMed]
- Jansen, G.; Ebeling, N.; Latka, E.; Krüger, S.; Scholz, S.S.; Trapp, S.; Grannemann, J.J.; Thaemel, D.; Chandwani, S.; Sauzet, O.; et al. Impact of COVID-19-adapted guidelines on resuscitation quality in out-of-hospital-cardiac-arrest: A manikin study. Minerva Anestesiol. 2021, 87, 1320–1329. [Google Scholar] [CrossRef]
- Law, A.K.; Ng, M.; Hon, K.; Graham, C.A. Out-of-hospital cardiac arrest in the pediatric population in Hong Kong: A 10-year review at a University Hospital. Pediatr. Emerg. Care 2018, 34, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Szary, J.; Jaguszewski, M.J.; Smereka, J.; Gasecka, A.; Emam, M.S.; John, I.; Rafique, Z.; Peacock, F.W.; Chirico, F.; Sagan, D.; et al. Impact of COVID-19 on pediatric out-of-hospital cardiac arrest in the Masovian region. Disaster Emerg. Med. J. 2021, 6, 183–185. [Google Scholar] [CrossRef]
- Jayaram, N.; McNally, B.; Tang, F.; Chan, P.S. Survival after out-of-hospital cardiac arrest in children. J. Am. Heart Assoc. 2015, 4, e002122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkins, D.L.; Everson-Stewart, S.; Sears, G.K.; Daya, M.; Osmond, M.H.; Warden, C.R.; Berg, R.A.; Resuscitation Outcomes Consortium Investigators. Epidemiology and outcomes from out-of-hospital cardiac arrest in children: The ROC Epistry-cardiac arrest. Circulation 2009, 119, 1484–1491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, Y.R.; Wu, H.P.; Huang, C.Y.; Chang, Y.J.; Lin, C.Y.; Chou, C.C. Significant factors in predicting sustained ROSC in paediatric patients with traumatic out-of hospital cardiac arrest admitted to the emergency department. Resuscitation 2007, 74, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.R.; Wu, H.P.; Chen, W.L.; Wu, K.H.; Teng, T.H.; Yang, M.C.; Chou, C.C.; Chang, C.F.; Li, C.J. Predictors of survival and neurologic outcomes in children with traumatic out-of-hospital cardiac arrest during the early postresuscitative period. J. Trauma Acute Care Surg. 2013, 75, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Tu, X.; Zhou, X.; Yu, J.; Luo, S.; Ma, L.; Liu, C.; Zhao, Y.; Jin, X. Wearing a N95 mask increases rescuer’s fatigue and decreases chest compression quality in simulated cardiopulmonary resuscitation. Am. J. Emerg. Med. 2021, 44, 434–438. [Google Scholar] [CrossRef]
- Serin, S.; Caglar, B. The Effect of Different Personal Protective Equipment Masks on Health Care Workers’ Cardiopulmonary Resuscitation Performance During the Covid-19 Pandemic. J. Emerg. Med. 2021, 60, 292–298. [Google Scholar] [CrossRef]
- Shah, P.; Smith, H.; Olarewaju, A.; Jani, Y.; Cobb, A.; Owens, J.; Moore, J.; Chenna, A.; Hess, D. Is cardiopulmonary resuscitation futile in coronavirus disease 2019 patients experiencing in-hospital cardiac arrest? Crit. Care Med. 2021, 49, 201–208. [Google Scholar] [CrossRef]
- Miles, J.A.; Mejia, M.; Rios, S.; Sokol, S.I.; Langston, M.; Hahn, S.; Leiderman, E.; Salgunan, R.; Soghier, I.; Gulani, P.; et al. Characteristics and outcomes of inhospital cardiac arrest events during the COVID-19 pandemic: A single-center experience from a New York City Public Hospital. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e007303. [Google Scholar] [CrossRef]
- Chen, C.Y.; Lee, E.P.; Chang, Y.J.; Yang, W.C.; Lin, M.J.; Wu, H.P. Impact of Coronavirus Disease 2019 Pandemic on Pediatric Out-of-Hospital Cardiac Arrest in the Emergency Department. Front. Pediatr. 2022, 10, 846410. [Google Scholar] [CrossRef]
- El-Zein, R.S.; Chan, M.L.; Su, L.; Chan, P.S.; American Heart Association’s Get With the Guidelines®-Resuscitation Investigators. Outcomes of pediatric patients with COVID-19 and in-hospital cardiopulmonary resuscitation. Resuscitation 2022, 173, 71–75. [Google Scholar] [CrossRef]
- Morgan, R.W.; Wolfe, H.A.; Reeder, R.W.; Alvey, J.S.; Frazier, A.H.; Friess, S.H.; Maa, T.; McQuillen, P.S.; Meert, K.L.; Nadkarni, V.M.; et al. The Temporal Association of the COVID-19 Pandemic and Pediatric Cardiopulmonary Resuscitation Quality and Outcomes. Pediatr. Crit. Care Med. 2022, 23, 908–918. [Google Scholar] [CrossRef] [PubMed]
- Recher, M.; Baert, V.; Leteurtre, S.; Hubert, H. Consequences of coronavirus disease outbreak on paediatric out-of-hospital cardiac arrest in France. Resuscitation 2020, 155, 100–102. [Google Scholar] [CrossRef] [PubMed]
- Zha, L.; Hosomi, S.; Kiyohara, K.; Sobue, T.; Kitamura, T. Association of the COVID-19 Pandemic With Prehospital Characteristics and Outcomes of Pediatric Patients With Out-of-Hospital Cardiac Arrest in Japan, 2005–2020. JAMA Netw. Open 2022, 5, e2235401. [Google Scholar] [CrossRef]
- Shekerdemian, L.S.; Mahmood, N.R.; Wolfe, K.K.; Riggs, B.J.; Ross, C.E.; McKiernan, C.A.; Heidemann, S.M.; Kleinman, L.C.; Sen, A.I.; Hall, M.W.; et al. International COVID-19 PICU Collaborative. International COVID-19 PICU Collaborative: Characteristics and outcomes of children with coronavirus disease 2019 (COVID-19) infection admitted to US and canadian pediatric intensive care units. JAMA Pediatr. 2020, 174, 868–873. [Google Scholar] [CrossRef]
- Bhalala, U.S.; Gist, K.M.; Tripathi, S.; Boman, K.; Kumar, V.K.; Retford, L.; Chiotos, K.; Blatz, A.M.; Dapul, H.; Verma, S.; et al. Society of Critical Care Medicine Discovery Viral Infection and Respiratory Illness Universal Study (VIRUS): COVID-19 Registry Investigator Group. Characterization and outcomes of hospitalized children with coronavirus disease 2019: A report from a multicenter, viral infection and respiratory illness universal study (coronavirus disease 2019) registry. Crit. Care Med. 2022, 50, e40–e51. [Google Scholar] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Rev. Esp. Cardiol. 2021, 74, 790–799. [Google Scholar] [CrossRef]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. Newcastle-Ottawa Quality Assessment Scale Cohort Studies. 2014. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 12 October 2022).
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Morgan, R.W.; Atkins, D.L.; Hsu, A.; Kamath-Rayne, B.D.; Aziz, K.; Berg, R.A.; Bhanji, F.; Chan, M.; Cheng, A.; Chiotos, K.; et al. American Heart Association Emergency Cardiovascular Committee and Get with the Guidelines-Resuscitation Pediatric Task Force in Collaboration with the American Academy of Pediatrics, American Association for Respiratory Care, and American Society of Anesthesiologists. Guidance for Cardiopulmonary Resuscitation of Children With Suspected or Confirmed COVID-19. Pediatrics 2022, 150, e2021056043. [Google Scholar]
- Chojecka, D.; Pytlos, J.; Zawadka, M.; Andruszkiewicz, P.; Szarpak, Ł.; Dzieciątkowski, T.; Jaguszewski, M.J.; Filipiak, K.J.; Gąsecka, A. How to Maintain Safety and Maximize the Efficacy of Cardiopulmonary Resuscitation in COVID-19 Patients: Insights from the Recent Guidelines. J. Clin. Med. 2021, 10, 5667. [Google Scholar] [CrossRef]
- Borkowska, M.J.; Smereka, J.; Safiejko, K.; Nadolny, K.; Maslanka, M.; Filipiak, K.J.; Jaguszewski, M.J.; Szarpak, L. Out-of-hospital cardiac arrest treated by emergency medical service teams during COVID-19 pandemic: A retrospective cohort study. Cardiol. J. 2021, 28, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Bielski, K.; Szarpak, A.; Jaguszewski, M.J.; Kopiec, T.; Smereka, J.; Gasecka, A.; Wolak, P.; Nowak-Starz, G.; Chmielewski, J.; Rafique, Z.; et al. The Influence of COVID-19 on Out-Hospital Cardiac Arrest Survival Outcomes: An Updated Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 5573. [Google Scholar] [CrossRef] [PubMed]
- Wyckoff, M.H.; Singletary, E.M.; Soar, J.; Olasveengen, T.M.; Greif, R.; Liley, H.G.; Zideman, D.; Bhanji, F.; Andersen, L.W.; Avis, S.R.; et al. 2021 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations: Summary From the Basic Life Support; Advanced Life Support; Neonatal Life Support; Education, Implementation, and Teams; First Aid Task Forces; and the COVID-19 Working Group. Resuscitation 2021, 169, 229–311. [Google Scholar] [PubMed]


{kind=link}
| Study | Country | Cardiac Arrest Setting | COVID-19 Period | Pre-COVID-19 Period | NOS Score | ||||
|---|---|---|---|---|---|---|---|---|---|
| No. | Age, Years | Sex, Male | No. | AGE, YEARS | Sex, Male | ||||
| Chen et al., 2022 [21] | Taiwan | OHCA | 37 | NS | 23 (62.2%) | 60 | NS | 45 (75.0%) | 8 |
| Meyer-Szary et al., 2021 [12] | Poland | OHCA | 29 | 6.7 (6.2) | 15 (57.1%) | 18 | 5.1 (6.5) | 13 (72.2%) | 8 |
| Recher et al., 2020 [24] | France | OHCA | 32 | 6 (0–14) | 19 (59.4%) | 53 | 9 (1–15) | 32 (68.1%) | 8 |
| Zha et al., 2022 [25] | Japan | OHCA | 1160 | NS | 671 (57.8%) | 6443 | NS | 3896 (60.5%) | 9 |
| El-Zein et al., 2020 [22] | USA | IHCA | 46 | NS | 23 (50.0%) | 1282 | NS | 713 (55.6%) | 9 |
| Morgan et al., 2022 [23] | USA | IHCA | 195 | NS | 93 (47.7%) | 234 | NS | 133 (56.8%) | 8 |
| Characteristic | No. of Studies | Event/Participants or Mean ± SD | Events | Heterogeneity between Trials | p-Value for Differences across Groups | |||
|---|---|---|---|---|---|---|---|---|
| COVID-19 Period | Pre-COVID-19 Period | OR or MD | 95% CI | p-Value | I2 Statistics | |||
| Age | 3 | 6.6 (5.5) | 6.1 (5.4) | 0.43 | −2.73 to 3.58 | 0.008 | 79% | 0.79 |
| Sex, male | 4 | 728/1258 (57.9%) | 3988/6574 (60.7%) | 0.88 | 0.78 to 1.00 | 0.46 | 0% | 0.04 |
| OHCA at home | 1 | 27/31 87.1%) | 32/47 (68.1%) | 3.16 | 0.94 to 10.68 | NA | NA | 0.06 |
| Cause of OHCA | ||||||||
| 3 | 465/1221 (38.1%) | 2338/6514 (35.9%) | 1.02 | 0.90 to 1.16 | 0.43 | 0% | 0.75 |
| 3 | 12/98 (12.2%) | 20/131 (15.3%) | 0.78 | 0.35 to 1.72 | 0.14 | 48% | 0.54 |
| Witnessed cardiac arrest | 2 | 343/1197 (28.7%) | 1852/6503 (28.5%) | 0.99 | 0.87 to 1.14 | 0.55 | 0% | 0.93 |
| Bystander CPR | 3 | 782/1229 (63.6%) | 4035/6556 (61.5%) | 1.11 | 0.98 to 1.26 | 0.52 | 0% | 0.11 |
| Bystander AED | 2 | 33/1192 (2.8%) | 183/6496 (2.8%) | 1.00 | 0.69 to 1.45 | 0.71 | 0% | 0.99 |
| The first recorded cardiac rhythm | ||||||||
| Shockable | 4 | 71/1258 (5.6%) | 383/6568 (5.8%) | 0.98 | 0.75 to 1.27 | 0.85 | 0% | 0.88 |
| Non-shockable | 4 | 1184/1258 (94.4%) | 6183/6568 (94.2%) | 1.00 | 0.77 to 1.30 | 0.60 | 0% | 1.00 |
| Airway management procedures | ||||||||
| ETI | 2 | 40/57 (70.2%) | 39/55 (70.9%) | 1.30 | 0.11 to 15.53 | 0.03 | 80% | 0.83 |
| SADs | 1 | 6/29 (20.7%) | 8/18 (44.4%) | 0.33 | 0.09 to 1.19 | NA | NA | 0.09 |
| Outcomes | ||||||||
| ROSC | 3 | 109/1221 (8.9%) | 550/6514 (8.4%) | 0.93 | 0.47 to 1.88 | 0.11 | 54% | 0.85 |
| Survival to hospital admission | 4 | 128/1258 (10.2%) | 590/6570 (9.0%) | 0.81 | 0.45 to 1.44 | 0.09 | 54% | 0.47 |
| Survival to hospital discharge | 2 | 148/1197 (12.4%) | 872/6503 (13.4%) | 0.62 | 0.22 to 1.72 | 0.05 | 73% | 0.35 |
| SHD with CPC 1–2 | 1 | 59/1160 (5.1%) | 331/6443 (5.1%) | 0.99 | 0.74 to 1.31 | NA | NA | 0.94 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navolokina, A.; Smereka, J.; Böttiger, B.W.; Pruc, M.; Juárez-Vela, R.; Rahnama-Hezavah, M.; Rafique, Z.; Peacock, F.W.; Safiejko, K.; Szarpak, L. The Impact of COVID-19 on Pediatric Cardiac Arrest Outcomes: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 1104. https://doi.org/10.3390/ijerph20021104
Navolokina A, Smereka J, Böttiger BW, Pruc M, Juárez-Vela R, Rahnama-Hezavah M, Rafique Z, Peacock FW, Safiejko K, Szarpak L. The Impact of COVID-19 on Pediatric Cardiac Arrest Outcomes: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(2):1104. https://doi.org/10.3390/ijerph20021104
Chicago/Turabian StyleNavolokina, Alla, Jacek Smereka, Bernd W. Böttiger, Michal Pruc, Raúl Juárez-Vela, Mansur Rahnama-Hezavah, Zubaid Rafique, Frank W. Peacock, Kamil Safiejko, and Lukasz Szarpak. 2023. "The Impact of COVID-19 on Pediatric Cardiac Arrest Outcomes: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 2: 1104. https://doi.org/10.3390/ijerph20021104