
Chronic Occupational Exposure to Traffic Pollution Is Associated with Increased Carotid Intima-Media Thickness in Healthy Urban Traffic Control Police
 , and
, and
Abstract
:1. Introduction
2. Methods
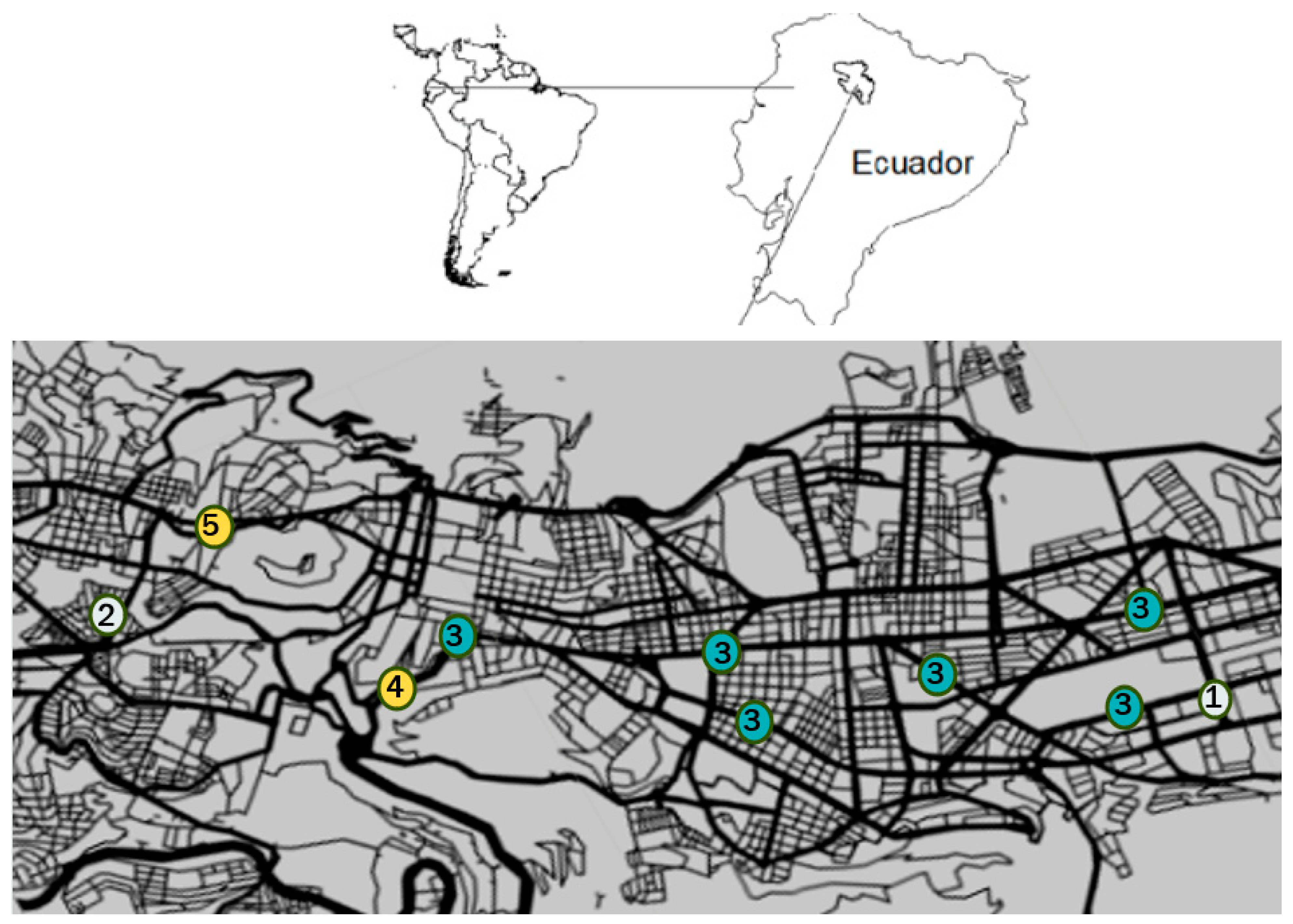
2.1. Study Site
2.2. Study Design and Participants
2.3. Exposure
2.4. Primary Outcome
2.5. Covariates
2.6. Data Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- HEI. HEI Panel on the Health Effects of Long-Term Exposure to Traffic-Related Air Pollution. In Systematic Review and Meta-Analysis of Selected Health Effects of Long-Term Exposure to Traffic-Related Air Pollution; Special Report 23; Health Effects Institute: Boston, MA, USA, 2022. [Google Scholar]
- Khreis, H.; Nieuwenhuijsen, M.; Zietsman, J.; Ramani, T. Emissions, human exposures, and health-The way forward. Traffic Relat. Air Pollut. 2020, 25, 597–620. [Google Scholar] [CrossRef]
- Heydari, S.; Tainio, M.; Woodcock, J.; de Nazelle, A. Estimating traffic contribution to particulate matter concentration in urban areas using a multilevel Bayesian meta-regression approach. Environ. Int. 2020, 141, 105800. [Google Scholar] [CrossRef] [PubMed]
- EPA 2020 Emissions Inventories. Available online: https://www.epa.gov/air-emissions-inventories/2020-national-emissions-inventory-nei-data (accessed on 11 August 2021).
- Boogaard, H.; Vienneau, D.; Weuve, J.; Lurmann, F.W.; Forastiere, F. Long-term exposure to traffic-related air pollution and selected health outcomes: A systematic review and meta-analysis. Environ. Int. 2022, 164, 107262. [Google Scholar] [CrossRef] [PubMed]
- WHO. Invisible Numbers: The True Extent of Noncommunicable Diseases and What to Do about Them; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]
- O’Leary, D.H.; Polak, J.F.; Kronmal, R.A.; Manolio, T.A.; Burke, G.L.; Wolfson, S.K. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. Cardiovascular Health Study Collaborative Research Group. N. Engl. J. Med. 1999, 340, 14–22. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A., III; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef]
- Bai, Y.; Sun, Q. Fine particulate matter air pollution and atherosclerosis: Mechanistic insights. Biochim. Biophys. Acta (BBA)-Gen. Subj. 2016, 1860, 2863–2868. [Google Scholar] [CrossRef]
- Alexeeff, S.E.; Coull, B.A.; Gryparis, A.; Suh, H.; Sparrow, D.; Vokonas, P.S.; Schwartz, J. Medium-term exposure to traffic-related air pollution and markers of inflammation and endothelial function. Environ. Health Perspect. 2011, 119, 481–486. [Google Scholar] [CrossRef]
- Pope, C.A., III; Bhatnagar, A.; McCracken, J.P.; Abplanalp, W.; Conklin, D.J.; O’Toole, T. Exposure to fine particulate air pollution is associated with endothelial injury and systemic inflammation. Circ. Res. 2016, 119, 1204–1214. [Google Scholar] [CrossRef]
- Liang, S.; Zhang, J.; Ning, R.; Du, Z.; Liu, J.; Batibawa JWa Duan, J.; Sun, Z. The critical role of endothelial function in fine particulate matter-induced atherosclerosis. Fibre Toxicol. 2020, 17, 61. [Google Scholar] [CrossRef]
- Geisel, M.H.; Bahuer, M.; Hernning, F.; Hoffmann, B.; Lehmann, N.; Mohlenkamp, S.; Kroger, K.; Kara, K.; Muller, T.; Moebus, S.; et al. Comparison of coronary artery calcification, carotid intima-media thickness and ankle-brachial index for predicting 10-year incident cardiovascular events in the general population. Eur. Heart J. 2017, 38, 1815–1822. [Google Scholar] [CrossRef]
- Künzli, N.; Jerrett, M.; Mack, W.J.; Beckerman, B.; LaBree, L.; Gilliland, F. Ambient air pollution and atherosclerosis in Los Angeles. Environ. Health Perspect. 2005, 113, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Künzli, N.; Jerret, M.; Garcia-Esteban, R.; Basagaña, X.; Beckermann, B.; Gilliland, F.; Medina, M.; Peters, J.; Hodis, H.N.; Mack, W.J. Ambient air pollution and the progression of atherosclerosis in adults. PLoS ONE 2010, 5, e9096. [Google Scholar] [CrossRef]
- Hoffmann, B.; Moebus, S.; Möhlenkamp, S.; Stang, A.; Lehmann, N.; Dragano, N. Residential exposure to traffic is associated with coronary atherosclerosis. Circulation 2007, 116, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Diez Roux, A.V.; Auchincloss, A.H.; Franklin, T.G.; Raghunathan, T.; Barr, R.G.; Kaufman, J.; Astor, B.; Keeler, J. Long-term exposure to ambient particulate matter and prevalence of subclinical atherosclerosis in the Multi-Ethnic Study of Atherosclerosis. Am. J. Epidemiol. 2008, 167, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Moebus, S.; Möhlenkamp, S.; Dragano, N.; Nonnemacher, M.; Fuchsluger, M.; Kessler, C.; Jakobs, H.; Memmesheimer, M.; Erbel, R.; et al. Urban particulate matter air pollution is associated with subclinical atherosclerosis: Results from the HNR (Heinz Nixdorf Recall) study. J. Am. Coll. Cardiol. 2010, 56, 1803–1808. [Google Scholar] [CrossRef]
- Rivera, M.; Basagaña, X.; Aguilera, I.; Foraster, M.; Agis, D.; de Groot, E.; Perez, L.; Mendez, M.A.; Bouso, L.; Targa, J.; et al. Association between long-term exposure to traffic-related air pollution and subclinical atherosclerosis: The REGICOR study. Environ. Health Perspect. 2013, 121, 223–230. [Google Scholar] [CrossRef]
- Su, T.C.; Hwang, J.J.; Shen, Y.C.; Chan, C.C. Carotid intima-media thickness and long-term exposure to traffic-related air pollution in middle-aged residents of Taiwan: A cross-sectional study. Environ. Health Perspect. 2015, 123, 773–778. [Google Scholar] [CrossRef]
- Chen, S.-Y.; Hwang, J.-S.; Chan, C.-C.; Wu, C.-F.; Wu, C.; Su, T.-C. Urban Air Pollution and Subclinical Atherosclerosis in Adolescents and Young Adults. J. Adolesc. Health 2022, 71, 233–238. [Google Scholar] [CrossRef]
- Wang, Y.; Wellenius, G.A.; Hickson, D.A.; Gjelsvik, A.; Eaton, C.B.; Wyatt, S.B. Residential proximity to traffic-related atherosclerosis in 4 vascular beds among African-Americans adults. Am. J. Epidemiol. 2016, 15, 732–743. [Google Scholar] [CrossRef]
- Farzan, S.F.; Habre, R.; Danza, P.; Lurmann, F.; Gauderman, W.J.; Avol, E.; Bastain, T.; Hodis, H.N.; Breton, C. Childhood traffic-related air pollution and adverse changes in subclinical atherosclerosis measures from childhood to adulthood. Environ. Health 2021, 20, 44. [Google Scholar] [CrossRef]
- Lenters, V.; Uiterwaal, C.S.; Beelen, R.; Bots, M.L.; Fischer, P.; Brunekreef, B.; Hoek, G. Long-term exposure to air pollution and vascular damage in young adults. Epidemiology 2010, 21, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Perez, L.; Wolf, K.; Hennig, F.; Penell, J.; Basagaña, X.; Foraster, M.; Aguilera, I.; Agis, D.; Beelen, R.; Brunekreef, B.; et al. Air pollution and atherosclerosis: A cross-sectional analysis of four European cohort studies in the ESCAPE study. Environ. Health Perspect. 2015, 123, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Oikonomou, E.; Theofilis, P.; Vogiatzi, G.; Lazaros, G.; Tsalamandris, S.; Mystakidi, V.C.; Goliopoulou, A.; Anastasiou, M.; Fountoulakis, P.; Chasikidis, C.; et al. Tousoulis The impact of sleeping duration on atherosclerosis in the community: Insights from the Corinthia study. Sleep Breath 2021, 25, 1813–1819. [Google Scholar] [CrossRef] [PubMed]
- Gan, W.Q.; Allen, R.W.; Brauer, M.; Davies, H.W.; Mancini, G.J.; Lear, S.A. Long-term exposure to traffic-related air pollution and progression of carotid artery atherosclerosis: A prospective cohort study. BMJ Open 2014, 4, e004743. [Google Scholar] [CrossRef]
- Wongsurakiat, P.; Maranetra, K.N.; Nana, A.; Naruman, C.; Aksornint, M.; Chalermsanyakorn, T. Respiratory symptoms and pulmonary function of traffic policemen in Thonburi. J. Med. Assoc. Thail. Chotmaihet Thangphaet 1999, 8, 435–443. [Google Scholar]
- Karita, K.; Yano, E.; Jinsat, W.; Boudoung, D.; Tamura, K. Respiratory symptoms and pulmonary function among traffic police in Bangkok, Thailand. Arch. Environ. Health Int. J. 2001, 56, 467–470. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Mittal, S.; Kumar, A.; Singh, K.D. Respiratory effects of air pollutants among nonsmoking traffic policemen of Patiala, India. Lung India Off. Organ Indian Chest Soc. 2011, 28, 253. [Google Scholar] [CrossRef] [PubMed]
- Estévez-García, J.A.; Rojas-Roa, N.Y.; Rodríguez-Pulido, A.I. Occupational exposure to air pollutants: Particulate matter and respiratory symptoms affecting traffic-police in Bogotá. Rev. Salud Publica 2013, 15, 889–902. [Google Scholar]
- Patil, R.; Chetlapally, S.; Bagavandas, M. Global review of studies on traffic police with special focus on environmental health effects. Int. J. Occup. Med. Environ. Health 2014, 27, 523–535. [Google Scholar] [CrossRef]
- Sharma, H.K.; Dandotiya, B.; Jadon, N. Exposure of Air pollution and its health effects in traffic police persons of Gwalior City, India. Environ. Claims J. 2017, 29, 305–315. [Google Scholar] [CrossRef]
- Villacis, D.F.; Piedra, J.P. Síntomas respiratorios en agentes civiles de tránsito expuestos a smog en Quito en el año 2021. Cambios Rev. Médica 2021, 20, 39–45. [Google Scholar]
- Crebelli, R.; Tomei, F.; Zijno, A.; Ghittori, S.; Imbriani, M.; Gamberale, D.; Martini, A.; Carere, A. Exposure to benzene in urban workers: Environmental and biological monitoring of traffic police in Rome. Occup. Environ. Med. 2001, 58, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Kamboj, S.S.; Sambyal, V. Increased chromosomal aberrations in peripheral blood lymphocytes of traffic policemen of Amritsar city. Int. J. Hum. Genet. 2006, 6, 125–131. [Google Scholar] [CrossRef]
- Arayasiri, M.; Mahidol, C.; Navasumrit, P.; Autrup, H.; Ruchirawat, M. Biomonitoring of benzene and 1, 3-butadiene exposure and early biological effects in traffic policemen. Sci. Total Environ. 2010, 408, 4855–4862. [Google Scholar] [CrossRef]
- Prasad, B.S.; Vidyullatha, P.; Venkata, R.P.; Tirumala, V.G.; Varre, S.; Penagaluru, U.R.; Grover, P.; Mundluru, H.P.; Penagaluru, P.R. Evaluation of oxidative stress and DNA damage in traffic policemen exposed to vehicle exhaust. Biomarkers 2013, 18, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.; Lu, S.; Wang, Y.; Zhu, Y.; Shi, T.; Lin, M.; Deng, Z.; Wang, Z.; Song, N.; Li, S.; et al. Long-term exposure to high air pollution induces cumulative DNA damages in traffic policemen. Sci. Total Environ. 2017, 594, 330–336. [Google Scholar] [CrossRef]
- Maffei, F.; Hrelia, P.; Angelini, S.; Carbone, F.; Forti, G.C.; Barbieri, A.; Sanguinetti, G.; Mattioli, S.; Violante, F.S. Effects of environmental benzene: Micronucleus frequencies and haematological values in traffic police working in an urban area. Mutat. Res. Genet. Toxicol. Environ. Mutagen. 2005, 583, 1–11. [Google Scholar] [CrossRef]
- Tomei, G.; Ciarrocca, M.; Capozzella, A.; Fiaschetti, M.; Tomao, E.; Cangemi, C.; Rosati, M.V.; Cerratti, D.; Anzani, M.F.; Pimpinella, B.; et al. Hemopoietic system in traffic police exposed to urban stressors. Ind. Health 2008, 46, 298–301. [Google Scholar] [CrossRef]
- Devi, V.S.; Rao, V.D.; Hara Gopal, V.V.; Prasad, B.S.; Devi, G.S.; Jyothy, A.; Reddy, P.P.; Prasad, M.H. Cytogenetic evaluation of traffic policemen occupationally exposed to vehicular exhaust. Indian J. Med. Res. 2009, 130, 520. [Google Scholar]
- Dai, Y.; Zhang, X.; Zhang, R.; Zhao, X.; Duan, H.; Niu, Y.; Huang, C.; Meng, T.; Ye, M.; Bin, P.; et al. Long-term exposure to diesel engine exhaust affects cytokine expression among occupational population. Toxicol. Res. 2016, 5, 674–681. [Google Scholar] [CrossRef]
- Burgaz, S.; Demircigil, G.C.; Karahalil, B.; Karakaya, A.E. Chromosomal damage in peripheral blood lymphocytes of traffic policemen and taxi drivers exposed to urban air pollution. Chemosphere 2002, 47, 57–64. [Google Scholar] [CrossRef]
- Tomao, E.; Tiziana, P.B.; Rosati, V.; Marcellini, L.; Tomei, F. The effects of air pollution on the lipid balance of traffic police personnel. Ann. Saudi Med. 2002, 22, 287–290. [Google Scholar] [CrossRef]
- Tan, C.; Wang, Y.; Lin, M.; Wang, Z.; He, L.; Li, Z.; Li, Y.; Xu, K. Long-term high air pollution exposure induced metabolic adaptations in traffic policemen. Environ. Toxicol. Pharmacol. 2018, 58, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Gao, Z.; Tian, Z.; Xie, Y.; Xin, F.; Jiang, R.; Kan, H.; Song, W. The biological effects of individual-level PM(2.5) exposure on systemic immunity and inflammatory response in traffic policemen. Occup. Environ. Med. 2013, 70, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Shakya, K.M.; Peltier, R.E.; Zhang, Y.; Pandey, B.D. Roadside Exposure and Inflammation Biomarkers among a Cohort of Traffic Police in Kathmandu, Nepal. Int. J. Environ. Res. Public Health 2019, 16, 377. [Google Scholar] [CrossRef] [PubMed]
- Riediker, M. Cardiovascular effects of fine particulate matter components in highway patrol officers. Inhal. Toxicol. 2007, 19 (Suppl. S1), 99–105. [Google Scholar] [CrossRef]
- Bajaj, N.; Sharma, T.; Suneja, D.; Jain, S.; Kumar, P. Determinants of respiratory and cardiovascular health effects in traffic policemen: A perception-based comparative analysis. J. Transp. Health 2017, 4, 30–39. [Google Scholar] [CrossRef]
- Mortada, W.I.; Sobh, M.A.; El-Defrawy, M.M.; Farahat, S.E. Study of lead exposure from automobile exhaust as a risk for nephrotoxicity among traffic policemen. Am. J. Nephrol. 2001, 21, 274–279. [Google Scholar] [CrossRef]
- Kamal, A.A.M.; Eldamaty, S.E.; Faris, R. Blood lead level of Cairo traffic policeman. Sci. Total Environ. 1991, 105, 165–170. [Google Scholar] [CrossRef]
- Pala, K.; Akiş, N.; İzgi, B.; Gücer, Ş.; Aydin, N.; Aytekin, H. Blood lead levels of traffic policemen in Bursa, Turkey. Int. J. Hyg. Environ. Health 2002, 205, 361–365. [Google Scholar] [CrossRef]
- Liu, X.; Liang, Y.; Guo, J. Heavy metal pollution in Nanchang City and its health implication on traffic policemen. Environ. Sci. Pollut. Res. Int. 2019, 26, 17885–17890. [Google Scholar] [CrossRef] [PubMed]
- Jazani, R.K.; Saremi, M.; Rezapour, T.; Kavousi, A.; Shirzad, H. Influence of traffic-related noise and air pollution on self-reported fatigue. Int. J. Occup. Saf. Ergon. 2015, 21, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Mohamad Jamil, P.A.S.; Karuppiah, K.; Rasdi, I.; How, V.; Mohd Tamrin, S.B.; Mani, K.K.C.; Sambasivam, S.; Naeini, H.S.; Mohammad Yusof, N.A.D.; Hashim, N.M. Occupational hazard in Malaysian traffic police: Special focus on air pollutants. Rev. Environ. Health 2021, 36, 167–176. [Google Scholar] [CrossRef] [PubMed]
- United Nations Educational, Scientific and Cultural Organization (UNESCO). World Heritage Convention. City of Quito. UNESCO, 1992–2023. City of Quito–UNESCO World Heritage Centre. Available online: https://whc.unesco.org/en/list/2/ (accessed on 16 March 2023).
- Bravo Alvarez, H.; Sosa Echeverria, R.; Sanchez Alvarez, P.; Krupa, S. Air quality standards for particulate matter (PM) at high altitude cities. Environ. Pollut. 2013, 173, 255–256. [Google Scholar] [CrossRef]
- World Health Organization. Air Quality Guidelines for Europe, 2nd ed.; 2000; Available online: https://www.who.int/publications/i/item/9789289013581 (accessed on 16 March 2023).
- CORPAIRE. Informe Anual 2009, la Calidad del Aire en Quito; CORPAIRE: Quito, Ecuador, 2010. [Google Scholar]
- Armijos, R.X.; Weigel, M.M.; Myers, O.; Li, W.W.; Racines, M.; Berwick, M. Residential exposure to urban traffic is associated with increased carotid intima-media thickness in children. J. Environ. Public Health 2015, 2015, 713540. [Google Scholar] [CrossRef]
- EPMMOP-Q Gerencia de Planificacion de la Mobilidad, 2007–2010; Municipio Metropolitano de Quito: Quito, Ecuador, 2011.
- Raysoni, A.U.; Armijos, R.X.; Weigel, M.M.; Montoya, T.; Eschanique, P.; Racines, M.; Li, W.W. Assessment of indoor and outdoor PM species at sch 8ools and residences in a high-altitude Ecuadorian urban center. Environ. Pollut. 2016, 214, 668–679. [Google Scholar] [CrossRef]
- United Nations Environmental Programme (UNEP). Environment Climate Change Outlook: ECCO Metropolitan District of Quito, Regional Office for Latin America and the Caribbean, Division of Early Warning and Assessment; United Nations Environmental Programme (UNEP): Nairobi, Kenya, 2011. [Google Scholar]
- Secretaria del Ambiente. NORMA ECUATORIANA DE CALIDAD DEL AIRE 2011.El Martes 7 de Junio de 2011, se Publicó en el Registro Oficial, la Reformar a la Norma de Calidad del Aire Ambiente o Nivel de Inmisión, Constante en el Anexo 4 del Libro VI del Texto Unificado de Legislación Secundaria del Ministerio del Ambiente, y que Forma Parte del Conjunto de Normas Técnicas Ambientales para la Prevención y Control de la Contaminación, Citadas en la Disposición General Primera del Título IV del Libro VI del Texto Unificado de Legislación Secundaria del Ministerio del Ambiente. Available online: www.quitoambiente.gob.ec (accessed on 8 June 2021).
- Romero Quinchuela, G.I.; Zambrano Arciniega, J.M. Estudio y Alternativas de Solución al Tráfico en las Avenidas Ladrón de Guevara, Patria, Pérez Guerrero y América, en el Tramo Comprendido Desde el Coliseo Rumiñahui Hasta la Intersección de la Avenida América con la Avenida La Gasca, en la Ciudad de Quito. Quito: Universidad Central del Ecuador. 2022. Available online: www.uce.edu.ec (accessed on 20 April 2023).
- Vega, D.; Parra, R. Characterization the average daily intensity and the vehicular traffic profiles in Distrito Metropolitano de Quito Caracterización de la intensidad media diaria y de los perfiles horarios del tráfico vehicular del Distrito Metropolitano de Quito. Av. Cienc. E Ing. 2014, 6, C40–C45. [Google Scholar]
- Touboul, P.-J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, H.; Desvarieux, M.; Ebrahim, S.; Fatar, M.; Hernandez Hernandez, R.; Kownator, S.; et al. Mannheim intima-media thickness consensus. Cerebrovasc. Dis. 2004, 18, 346–349. [Google Scholar] [CrossRef]
- Krishnaveni, P.; Gowda, V.M.N. Assessing the Validity of Friedewald’s Formula for Serum LDL-Cholesterol Calculation. J. Clin. Diagn. Res. 2015, 9, BC01–BC04. [Google Scholar] [CrossRef]
- Dupuy, A.M.; Badiou, S.; Descomps, B.; Criltol, J.P. Immunoturbidimetric determination of C-reactive protein (CRP) and high-sensitivity CRP on heparin plasma. Comparison with serum determination. Clin. Chem. Lab. Med. 2003, 41, 948–949. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. 2020. Available online: www.who.int (accessed on 22 September 2021).
- Pickering, T.G.; Hall, J.E.; Appel, L.J.; Falkner, B.E.; Graves, J.W.; Hill, M.N.; Jones, D.H.; Kurtz, T.; Sheps, S.G.; Rocella, E.J. Recommendations for blood pressure measurement in humans: An AHA scientific statement from the Council on High Blood Pressure Research Professional and Public Education Subcommittee. J. Clin. Hypertens. 2005, 7, 102–109. [Google Scholar] [CrossRef]
- Nicolas, J.P. Analyzing road traffic influences on air pollution: How to achieve sustainable urban development. Transp. Rev. 2000, 20, 219–232. [Google Scholar] [CrossRef]
- United Nations Environment Program. Quito, Ecuador Is Taking Strong Actions to Improve Air Quality. Available online: www.cleanairblueskies.org (accessed on 9 June 2020).
- Khreis, H.; Sanchez, K.A.; Foster, M.; Burns, J.; Nieuwenhuijsen, M.J.; Jaikumar, R.; Ramani, T.; Zietsman, J. Urban policy interventions to reduce traffic-related emissions and air pollution: A systematic evidence map. Environ. Int. 2023, 172, 107805. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.L.; Tian, H.Y. Air pollution and risk of chronic obstructed pulmonary disease: The modifying effect of genetic susceptibility and lifestyle. E BioMedicine 2022, 79, 103994. [Google Scholar] [CrossRef]
- Gehring, U.; Wiiga, A.H.; Koppelman, G.H.; Vonk, J.M.; Smit, H.A.; Brunekreef, B. Air pollution and the development of asthma from birth until young adulthood. Eur. Respir. J. 2020, 56, 2000147. [Google Scholar] [CrossRef] [PubMed]
- Peeters, S.; Wang, C.; Bijnens, E.M.; Bullens, D.M.A.; Fokkens, W.J.; Bachert, C.; Hellings, P.W.; Nawrot, T.S.; Seys, S.F. Association between outdoor air pollution and chronic rhinosinusitis patient reported outcomes. Environ. Health 2022, 21, 134. [Google Scholar] [CrossRef]
- Chen, Y.; Cao, F.; Xiao, J.P.; Fang, X.Y.; Wang, X.R.; Ding, L.H.; Wang, D.G.; Pan, H.F. Emerging role of air pollution in chronic kidney disease. Environ. Sci. Pollut. Res. Int. 2021, 28, 52610–52624. [Google Scholar] [CrossRef]
- Raju, S.; Woo, H.; Koehler, K.; Fawzy, A.; Liu, C.; Putcha, N.; Balasubramanian, A.; Peng, R.D.; Lin, C.T.; Lemoine, C.; et al. Indoor Air Pollution and Impaired Cardiac Autonomic Function in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2023, 207, 721–730. [Google Scholar] [CrossRef]
- Poursafa, P.; Kamali, Z.; Fraszczyk, E.; Boezen, H.M.; Vaez, A.; Snieder, H. DNA methylation: A potential mediator between air pollution and metabolic syndrome. Clin. Epigenetics 2022, 14, 82. [Google Scholar] [CrossRef]
- GBD 2019 Diabetes and Air Pollution Collaborators. Estimates, trends, and drivers of the global burden of type 2 diabetes attributable to PM2·5 air pollution, 1990–2019: An analysis of data from the Global Burden of Disease. Lancet Planet Health 2022, 6, e586–e600. [Google Scholar] [CrossRef]
- Colao, A.; Muscogiuri, G.; Piscitelli, P. Environment and Health: Not Only Cancer. Int. J. Environ. Res. Public Health 2016, 13, 724. [Google Scholar] [CrossRef] [PubMed]
- Münzel, T.; Sørensen, M.; Daiber, A. Transportation noise pollution and cardiovascular disease. Nat. Rev. Cardiol. 2021, 18, 619–636. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Cavallero, S.; Hsiai, T.; Li, R. Impact of air pollution on intestinal redox lipidome and microbiome. Free Radic. Biol. Med. 2020, 151, 99–110. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total Sample (n = 115) Mean ± SD or No. (%) | High Exposure Group Road Traffic-Police Personnel (n= 61) Mean ± SD or No. (%) | Control Group Administrative-Duty Police Personnel (n= 54) Mean ± SD or No. (%) | |
|---|---|---|---|
| Age (years) | 31.6 ± 7.3 | 30.9 ± 8.4 | 32.4 ± 5.7 |
| Sex/gender (male) | 89 (77.4) | 51 (83.6) | 38 (70.4) |
| Body mass index | 25.9 ± 3.5 | 25.9 ± 3.3 | 25.9 ± 3.7 |
| Overweight | 57 (49.6) | 29 (47.6) | 28 (51.9) |
| Obesity | 13 (11.3) | 8 (13.1) | 5 (9.3) |
| Blood pressure | |||
| Systolic BP (mmHg) | 112 ± 12 | 110 ± 13 | 114 ± 10 * |
| Diastolic BP (mmHg) | 73 ± 8 | 73 ± 9 | 74 ± 7 |
| Blood lipid profile | |||
| Total cholesterol (mg/dL) | 210 ± 39 | 208 ± 39 | 212 ± 39 |
| Triglycerides(mg/dL) | 171 ± 103 | 178 ± 108 | 164 ± 98 |
| HDLc (mg/dL) | 49 ± 14 | 48 ± 11 | 51 ± 16 |
| LDLc (mg/dL) | 122 ± 29 | 124 ± 29 | 121 ± 29 |
| VLDLc (mg/dL) | 34 ± 21 | 36 ± 21 | 33 ± 20 |
| C-reactive protein (mg/dL) | 2.3 ± 3.2 | 1.9 ± 2.3 | 2.7 ± 4 |
| Any current smoking | 22 (19.1) | 16 (26.2) | 6 (11.1) |
| Any current alcohol consumption | 35 (30.4) | 20 (32.8) | 15 (27.8) |
| Positive family history for cardiovascular disease | 11 (9.6) | 7 (11.5) | 4 (7.4) |
| High Exposure Group Traffic-Duty Police Personnel (n = 61) | Control Group Administrative-Duty Police Personnel (n = 54) | |||
|---|---|---|---|---|
| Unadjusted Mean (95% CI) | Adjusted mean (95% CI) 1 | Unadjusted Mean (95% CI) | Adjusted mean (95% CI) 1 | |
| Mean CIMT (mm) | 0.537 (0.513, 0.561) | 0.535 (0.513, 0.557) | 0.472 (0.446, 0.497) * | 0.474 (0.450, 0.497) * |
| Mean Right CIMT (mm) | 0.546 (0.516, 0.575) | 0.538 (0.510, 0.566) | 0.459 (0.428, 0.490) * | 0.467 (0.438, 0.497) ** |
| Mean Left CIMT (mm) | 0.528 (0.497, 0.559) | 0.532 (0.501, 0.563) | 0.484 (0.451, 0.517) | 0.480 (0.447, 0.512) # |
| Maximum CIMT (mm) | 0.695 (0.669, 0.721) | 0.693 (0.668, 0.718) | 0.620 (0.592, 0.647) * | 0.622 (0.595, 0.649) * |
| Maximum Right CIMT (mm) | 0.705 (0.674,0.737) | 0.696 (0.666, 0.727) | 0.628 (0.594, 0.661) ** | 0.638 (0.605, 0.671) ## |
| Maximum Left CIMT (mm) | 0.685 (0.652, 0.719) | 0.690 (0.656, 0.724) | 0.612 (0.576, 0.647) ^ | 0.606 (0.570, 0.642) ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balogun, A.O.; Weigel, M.M.; Estévez, E.; Armijos, R.X. Chronic Occupational Exposure to Traffic Pollution Is Associated with Increased Carotid Intima-Media Thickness in Healthy Urban Traffic Control Police. Int. J. Environ. Res. Public Health 2023, 20, 6701. https://doi.org/10.3390/ijerph20176701
Balogun AO, Weigel MM, Estévez E, Armijos RX. Chronic Occupational Exposure to Traffic Pollution Is Associated with Increased Carotid Intima-Media Thickness in Healthy Urban Traffic Control Police. International Journal of Environmental Research and Public Health. 2023; 20(17):6701. https://doi.org/10.3390/ijerph20176701
Chicago/Turabian StyleBalogun, Abdulrazak O., M. Margaret Weigel, Edmundo Estévez, and Rodrigo X. Armijos. 2023. "Chronic Occupational Exposure to Traffic Pollution Is Associated with Increased Carotid Intima-Media Thickness in Healthy Urban Traffic Control Police" International Journal of Environmental Research and Public Health 20, no. 17: 6701. https://doi.org/10.3390/ijerph20176701