

Implementing Innovative Approaches to Improve Health Care Delivery Systems for Integrating Communicable and Non-Communicable Diseases Using Tuberculosis and Diabetes as a Model in Tanzania
 , ,
, ,  , , , , , and
, , , , , and
Abstract
:1. Background
2. Materials and Methods
2.1. Method Description
2.1.1. Design
2.1.2. Context
2.1.3. Target Sites and Sample Size
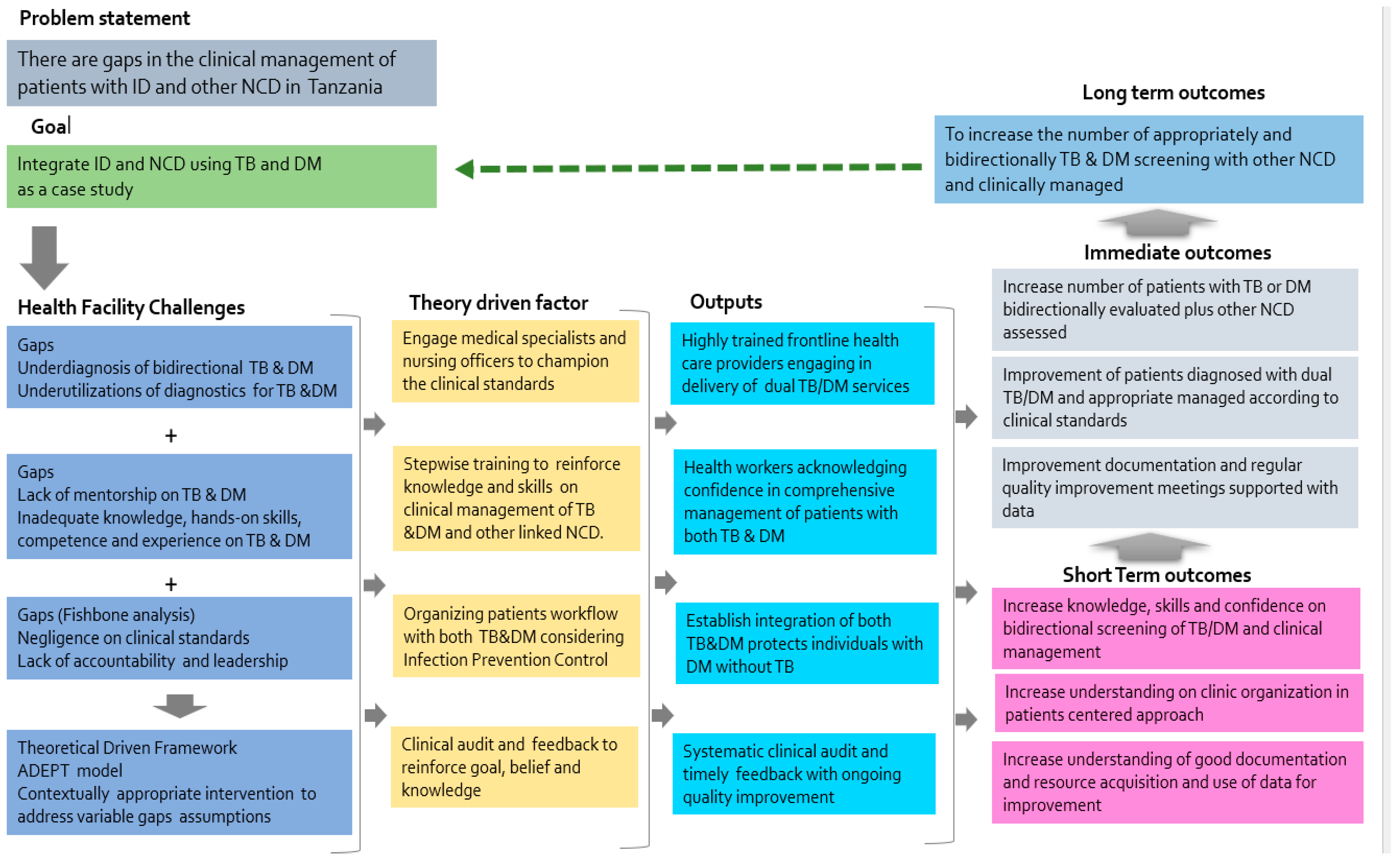
2.1.4. Description of the ADEPT Model Strategy
2.1.5. Phase 1: Training of Cluster One of the Health Care Providers
2.1.6. Phase 2: Training of Level 2 and Integration of the TB and DM Services
2.1.7. Phase 3: Clinical Audit of the TB and DM Clinical Standards
2.2. Method Evaluation
Statistical Analysis
3. Results
3.1. Stepwise Training ADEPT Intervention Sites
3.2. Comparison of Outcome Measures Using Clinical Audit Tools in Intervention and Control Health Facilities
3.3. Feasibility of the Stepwise Training
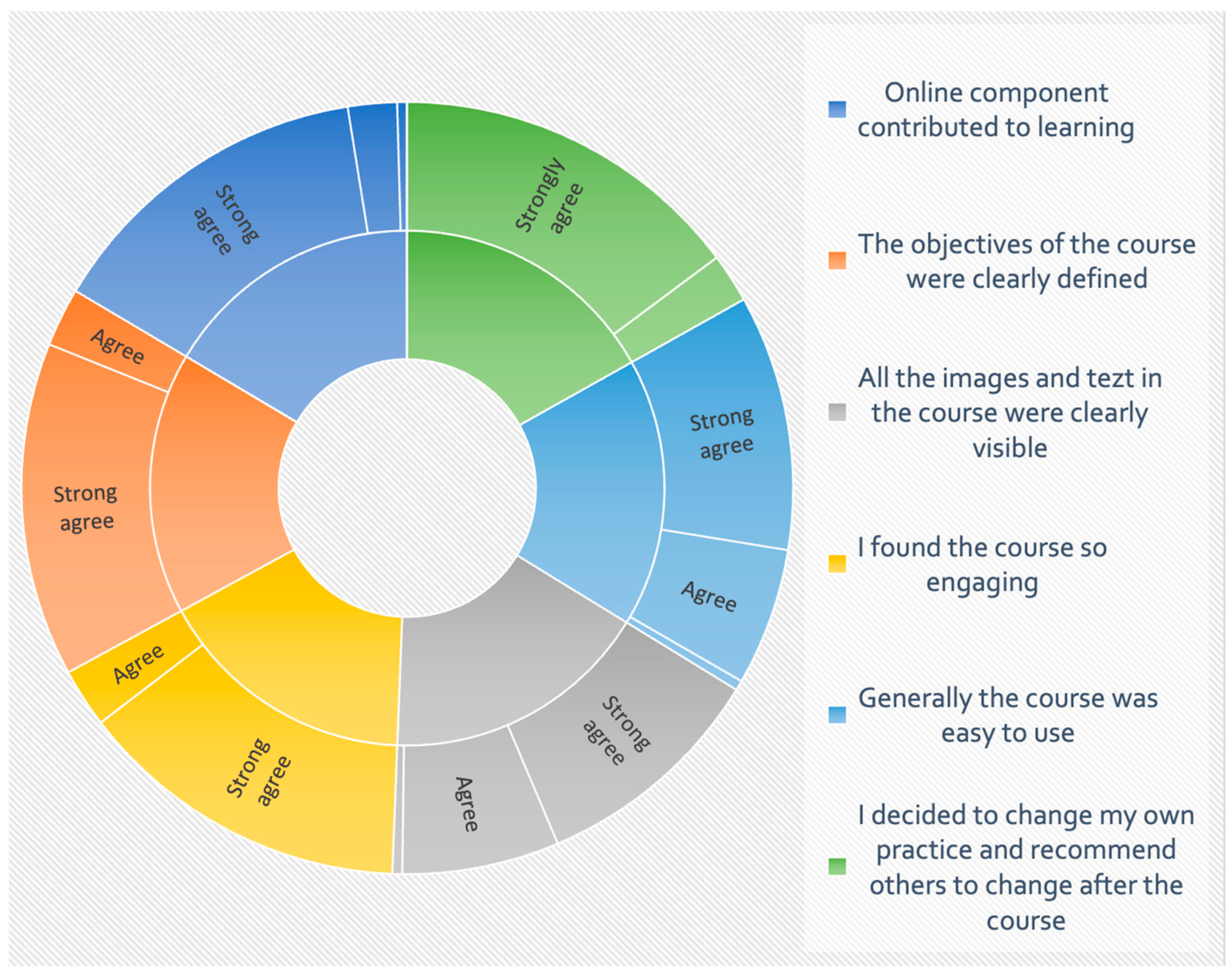
3.4. Acceptability of Web-Based Training in the Stepwise Training
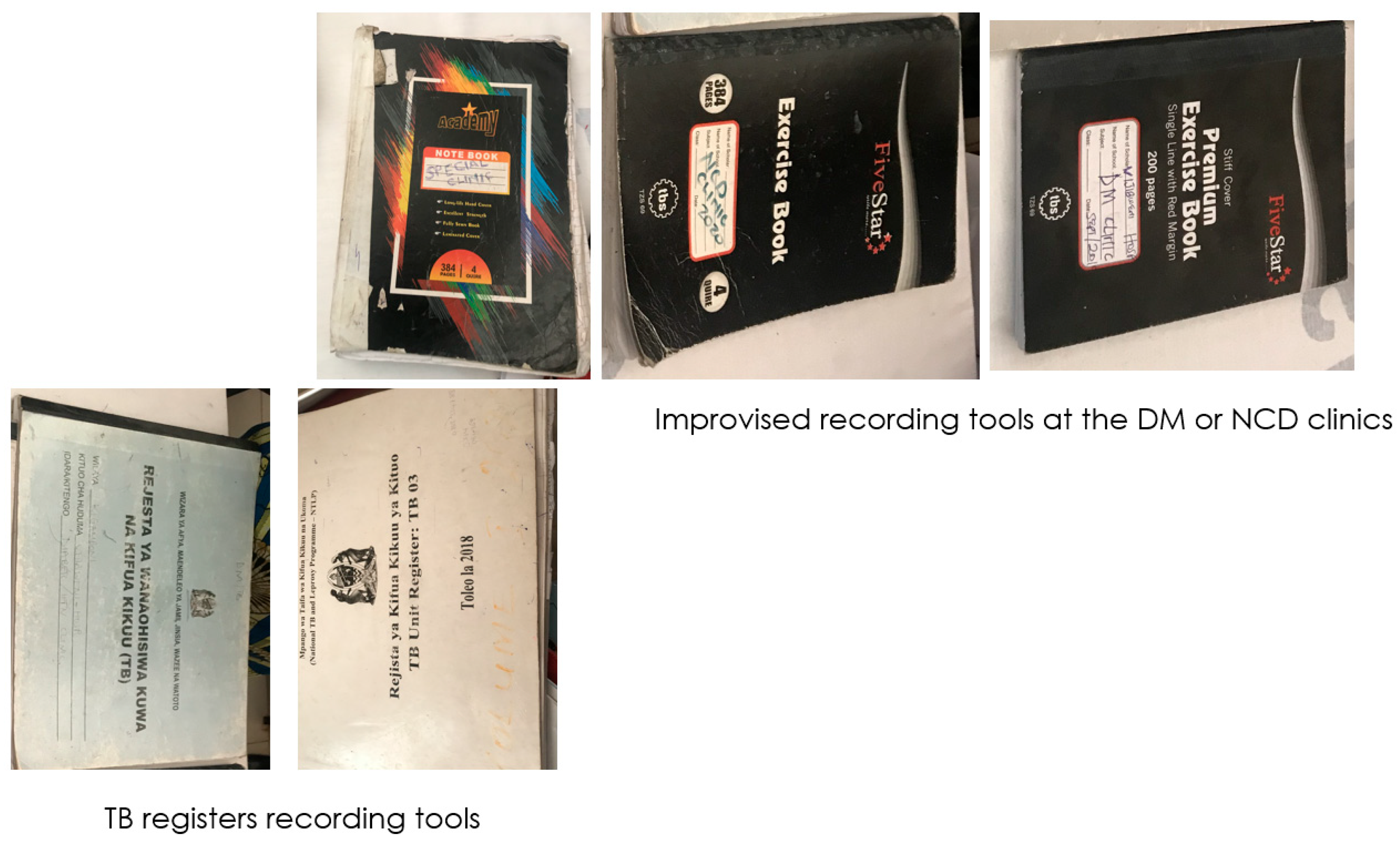
3.5. Other Observed Challenges during the Process of Implementation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tiberi, S.; Carvalho, A.C.C.; Sulis, G.; Vaghela, D.; Rendon, A.; Mello, F.C.; Rahman, A.; Matin, N.; Zumla, A.; Pontali, E. The cursed duet today: Tuberculosis and HIV-coinfection. Presse Med. 2017, 46 Pt 2, e23–e39. [Google Scholar] [CrossRef]
- Kruk, M.E.; Gage, A.D.; Joseph, N.T.; Danaei, G.; García-Saisó, S.; Salomon, J.A. Mortality due to low-quality health systems in the universal health coverage era: A systematic analysis of amenable deaths in 137 countries. Lancet 2018, 392, 2203–2212. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine. Crossing the Global Quality Chasm: Improving Health Care Worldwide; The National Academies Collection: Reports funded by National Institutes of Health; National Academies of Sciences, Engineering, and Medicine: Washington, DC, USA, 2018. [Google Scholar]
- Motala, A.A.; Mbanya, J.C.; Ramaiya, K.; Pirie, F.J.; Ekoru, K. Type 2 diabetes mellitus in sub-Saharan Africa: Challenges and opportunities. Nat. Rev. Endocrinol. 2022, 18, 219–229. [Google Scholar] [CrossRef]
- Egere, U.; Shayo, E.; Ntinginya, N.; Osman, R.; Noory, B.; Mpagama, S.; Hussein, E.; Tolhurst, R.; Obasi, A.; Mortimer, K.; et al. Management of chronic lung diseases in Sudan and Tanzania: How ready are the country health systems? BMC Health Serv. Res. 2021, 21, 734. [Google Scholar] [CrossRef]
- WHO. Global Tuberculosis Report; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Munseri, P.J.; Kimambo, H.; Pallangyo, K. Diabetes mellitus among patients attending TB clinics in Dar es Salaam: A descriptive cross-sectional study. BMC Infect. Dis. 2019, 19, 915. [Google Scholar] [CrossRef] [PubMed]
- Faurholt-Jepsen, D.; Range, N.; PrayGod, G.; Jeremiah, K.; Faurholt-Jepsen, M.; Aabye, M.G.; Changalucha, J.; Christensen, D.L.; Pipper, C.B.; Krarup, H.; et al. Diabetes Is a Risk Factor for Pulmonary Tuberculosis: A Case-Control Study from Mwanza, Tanzania. PLoS ONE 2011, 6, e24215. [Google Scholar] [CrossRef] [PubMed]
- Mpagama, S.G.; Ezekiel, M.J.; Mbelele, P.M.; Chongolo, A.M.; Kibiki, G.S.; de Guex, K.P.; Heysell, S.K. Gridlock from diagnosis to treatment of multidrug resistant tuberculosis (MDR-TB) in Tanzania: Patients’ perspectives from a focus group discussion. BMC Public Health 2020, 20, 1667. [Google Scholar] [CrossRef]
- Mpagama, S.G.; Mbelele, P.M.; Chongolo, A.M.; Lekule, I.A.; Lyimo, J.J.; Kibiki, G.S.; Heysell, S.K. Gridlock from diagnosis to treatment of multidrug-resistant tuberculosis in Tanzania: Low accessibility of molecular diagnostic services and lack of healthcare worker empowerment in 28 districts of 5 high burden TB regions with mixed methods evaluation. BMC Public Health 2019, 19, 395. [Google Scholar] [CrossRef]
- Adeyemi, O.; Lyons, M.; Njim, T.; Okebe, J.; Birungi, J.; Nana, K.; Mbanya, J.C.; Mfinanga, S.; Ramaiya, K.; Jaffar, S.; et al. Integration of non-communicable disease and HIV/AIDS management: A review of healthcare policies and plans in East Africa. BMJ Glob. Health 2021, 6, e004669. [Google Scholar] [CrossRef]
- Maokola, W.; Ngowi, B.; Lawson, L.; Robert, M.; Mahande, M.; Todd, J.; Msuya, S. Coverage of isoniazid preventive therapy among people living with HIV; A retrospective cohort study in Tanzania (2012–2016). Int. J. Infect. Dis. 2021, 103, 562–567. [Google Scholar] [CrossRef]
- Liyoyo, A.A.; Heysell, S.K.; Kisonga, R.M.; Lyimo, J.J.; Mleoh, L.J.; Mutayoba, B.K.; Lekule, I.A.; Mmbaga, B.T.; Kibiki, G.S.; Mpagama, S.G. Gridlock from diagnosis to treatment of Multidrug-Resistant Tuberculosis (MDR-TB) in Tanzania: Illuminating Potential Factors for Possible Intervention. East Afr. Health Res. J. 2017, 1, 31. [Google Scholar] [CrossRef] [PubMed]
- Dudley, L.; Garner, P. Strategies for integrating primary health services in low- and middle-income countries at the point of delivery. Cochrane Database Syst. Rev. 2011, 2019, CD003318. [Google Scholar] [CrossRef] [PubMed]
- Mpagama, S.G.; Ramaiya, K.; Lillebæk, T.; Mmbaga, B.T.; Boer, M.S.-D.; Ntinginya, N.E.; Alffenaar, J.-W.; Heysell, S.K.; Bygbjerg, I.C.; Christensen, D.L. Protocol for establishing an Adaptive Diseases control Expert Programme in Tanzania (ADEPT) for integrating care of communicable and non-communicable diseases using tuberculosis and diabetes as a case study. BMJ Open 2021, 11, e041521. [Google Scholar] [CrossRef] [PubMed]
- Potter, C.; Brough, R. Systemic capacity building: A hierarchy of needs. Health Policy Plan. 2004, 19, 336–345. [Google Scholar] [CrossRef]
- Curran, G.M.; Bauer, M.; Mittman, B.; Pyne, J.M.; Stetler, C. Effectiveness-implementation hybrid designs: Combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care 2012, 50, 217–226. [Google Scholar] [CrossRef]
- Gandhi, N.R.; Weissman, D.; Moodley, P.; Ramathal, M.; Elson, I.; Kreiswirth, B.N.; Mathema, B.; Shashkina, E.; Rothenberg, R.; Moll, A.P.; et al. Nosocomial Transmission of Extensively Drug-Resistant Tuberculosis in a Rural Hospital in South Africa. J. Infect. Dis. 2013, 207, 9–17. [Google Scholar] [CrossRef]
- Mfinanga, S.G.; Mnyambwa, N.P.; Minja, D.T.; Ntinginya, N.E.; Ngadaya, E.; Makani, J.; Makubi, A.N. Tanzania’s position on the COVID-19 pandemic. Lancet 2021, 397, 1542–1543. [Google Scholar] [CrossRef]
- Pinnock, H.; Barwick, M.; Carpenter, C.R.; Eldridge, S.; Grandes, G.; Griffiths, C.J.; Rycroft-Malone, J.; Meissner, P.; Murray, E.; Patel, A.; et al. Standards for Reporting Implementation Studies (StaRI) Statement. BMJ 2017, 356, i6795. [Google Scholar] [CrossRef]
- Kagaruki, G.B.; Mayige, M.T. Tanzania Steps Survey Report; Technical Report; National Institute of Medical Research: Dar es Salaam, Tanzania, 2013. [Google Scholar]
- Mabula, P.L.; Kazinyingi, K.I.; Chavala, E.C.; Mosha, V.; Msuya, S.E.; Leyaro, B.J. Prevalence and risk factors for diabetes mellitus among tuberculosis patients in Moshi Municipal Council, Kilimanjaro Tanzania. East Afr. Health Res. J. 2021, 5, 69–74. [Google Scholar] [CrossRef]
- Byashalira, K.C.; Chamba, N.G.; Alkabab, Y.; Mbelele, P.M.; Ntinginya, N.E.; Ramaiya, K.L.; Alimohamed, M.Z.; Heysell, S.K.; Mmbaga, B.T.; Bygbjerg, I.C.; et al. Clinical-demographic markers for improving diabetes mellitus diagnosis in people with tuberculosis in Tanzania. BMC Infect. Dis. 2022, 22, 260. [Google Scholar] [CrossRef]
- NTLP. TB Prevalence in Tanzania National Tuberculosis & Leprosy Programme. 2022. Available online: https://ntlp.go.tz/tuberculosis/tb-prevalence-in-tanzania/ (accessed on 8 April 2023).
- WHO. How to Investigate Drug Use in Health Facilities> Selected Drug Use Indicators. 1993. Available online: https://apps.who.int/iris/bitstream/handle/10665/60519/WHO_DAP_93.1.pdf (accessed on 8 April 2023).
- Paterson, C.; Chapman, J. Enhancing skills of critical reflection to evidence learning in professional practice. Phys. Ther. Sport 2013, 14, 133–138. [Google Scholar] [CrossRef] [PubMed]
- WHO/IUATLD. Collaborative Framework for Care and Control of Tuberculosis and Diabetes. Stop TB Department and Department of Chronic Diseases and Health Promotion World Health Organization, Geneva, Switzerland and The International Union Against Tuberculosis and Lung Disease, Paris, France; WHO/HTM/TB/2011.15. 2010. Available online: https://apps.who.int/iris/bitstream/handle/10665/44698/9789241502252_eng.pdf (accessed on 8 April 2023).
- Boillat-Blanco, N.; Ramaiya, K.L.; Mganga, M.; Minja, L.T.; Bovet, P.; Schindler, C.; Von Eckardstein, A.; Gagneux, S.; Daubenberger, C.; Reither, K.; et al. Transient Hyperglycemia in Patients With Tuberculosis in Tanzania: Implications for Diabetes Screening Algorithms. J. Infect. Dis. 2015, 213, 1163–1172. [Google Scholar] [CrossRef]
- UNION. Management of Diabetes Mellitus-Tuberculosis. A Guide to the Essential Practice, 1st ed.; 2022. Licence: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Foy, R.; Skrypak, M.; Alderson, S.; Ivers, N.M.; McInerney, B.; Stoddart, J.; Ingham, J.; Keenan, D. Revitalising audit and feedback to improve patient care. BMJ 2020, 368, m213. [Google Scholar] [CrossRef]
- Hut-Mossel, L.; Ahaus, K.; Welker, G.; Gans, R. Understanding how and why audits work in improving the quality of hospital care: A systematic realist review. PLoS ONE 2021, 16, e0248677. [Google Scholar] [CrossRef] [PubMed]
- Johnston, G.; Crombie, I.K.; Alder, E.M.; Davies, H.T.O.; Millard, A. Reviewing audit: Barriers and facilitating factors for effective clinical audit. BMJ Qual. Saf. 2000, 9, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Mormina, M.; Pinder, S. A conceptual framework for training of trainers (ToT) interventions in global health. Glob. Health 2018, 14, 100. [Google Scholar] [CrossRef]
- Feldacker, C.; Jacob, S.; Chung, M.H.; Nartker, A.; Kim, H.N. Experiences and perceptions of online continuing professional development among clinicians in sub-Saharan Africa. Hum. Resour. Health 2017, 15, 89. [Google Scholar] [CrossRef]
- Koumamba, A.P.; Bisvigou, U.J.; Ngoungou, E.B.; Diallo, G. Health information systems in developing countries: Case of African countries. BMC Med. Inform. Decis. Mak. 2021, 21, 232. [Google Scholar] [CrossRef]
- Birungi, J.; Kivuyo, S.; Garrib, A.; Mugenyi, L.; Mutungi, G.; Namakoola, I.; Mghamba, J.; Ramaiya, K.; Wang, D.; Maongezi, S.; et al. Integrating health services for HIV infection, diabetes and hypertension in sub-Saharan Africa: A cohort study. BMJ Open 2021, 11, e053412. [Google Scholar] [CrossRef]
- Sohrabi, C.; Alsafi, Z.; O’neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef] [PubMed]
- DeVita, T.; Brett-Major, D.; Katz, R. How are healthcare provider systems preparing for health emergency situations? World Med. Health Policy 2021, 14, 102–120. [Google Scholar] [CrossRef] [PubMed]
- Hogan, A.B.; Jewell, B.L.; Sherrard-Smith, E.; Vesga, J.F.; Watson, O.J.; Whittaker, C.; Hamlet, A.; Smith, J.A.; Winskill, P.; Verity, R.; et al. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, e1132–e1141. [Google Scholar] [CrossRef] [PubMed]
- Czeisler, M.É.; Barrett, C.E.; Siegel, K.R.; Weaver, M.D.; Czeisler, C.A.; Rajaratnam, S.M.; Howard, M.E.; Bullard, K.M. Health Care Access and Use Among Adults with Diabetes During the COVID-19 Pandemic—United States, February-March 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1597–1602. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Sub-Category | Total | Intervention Health Facilities Median Percentage Score in n% (25/75) * | Control Health Facilities Median Score in n% (25/75) | p-Value |
|---|---|---|---|---|---|
| Standard # 1: All new TB patients should be screened for diabetes (DM) at the start of TB treatment using the DM screening questionnaire to identify those with symptoms and signs of DM. Random blood glucose (RBG) and fasting blood glucose (FBG) tests should be performed per the algorithm for diagnosis of DM among TB patients. | |||||
| DM screening in TB, median (IQR) | Hospitals | 10 (0–69) | 90 (60–100) | 0 | 0.00 |
| Health Centres | 25 (0–95) | 69 (35–70) | 0 | ||
| Hypertension screening in TB, median (IQR) | Hospitals | 0 | 0 | 0 | 0.24 |
| Health Centres | 0 | 0 (0–10) | 0 | ||
| Malnutrition screening in TB median (IQR) | Hospitals | 23(10–30) | 25 (23–30) | 14 (5–28) | 0.31 |
| Health Centres | 12 (5–27) | 5 (5–30) | 15 (4–25) | ||
| General implementation of the standard, median (IQR) | Hospitals | 23 (8–46) | 46 (45–48) | 7 (3–8) | 0.00 |
| Health Centre | 10 (2–52) | 48 (13–62) | 2 (0–6) | ||
| Standard # 2: All DM patients should be screened for TB at the time of diagnosis and at follow-up visits. | |||||
| TB screening in DM, median (IQR) | Hospitals | 0 (0–67) | 0 (0–69) | 0 (0–50) | 0.05 |
| Health Centres | 0 (0–75) | 75(29–100) | 0 | ||
| Hypertension screening in DM, median (IQR) | Hospitals | 10 (0–100) | 0 (0–10) | 100 (50–100) | 0.81 |
| Health Centres | 0 (0–12) | 12 (0–95) | 0 | ||
| Malnutrition screening in DM, median (IQR) | Hospitals | 0 | 0 | 34(0–84) | 0.86 |
| Health Centres | 0 | 0 (0–3) | 0 | ||
| General implementation of the standard, median (IQR) | Hospitals | 19 (0–32) | 0 (0–19) | 39 (12–56) | 0.60 |
| Health Centres | 0 (0–19) | 19 (14–32) | 0 | ||
| Standard # 3: Management of patient with dual TB and DM either co-infected with HIV or not; the treatment will follow the standard TB treatment guideline and DM management will be in accordance with HbA1c glycaemic levels. | |||||
| HbA1c testing | Hospital | 27 (0–50) | 45 (27–50) | 0 | 0.04 |
| Health centre | 80 (42–100) | 80 (42–100) | 0 | ||
| Clinical management according to HbA1c results and antiretroviral therapy | Hospital | 45 (38–50) | 45 (41–58) | 25 (0–50) | 0.55 |
| Health centre | 50 (0–82) | 50 (0–82) | 0 | ||
| Assessment of complications | Hospital | 0 (0–20) | 20 (0–58) | 0 | 0.19 |
| Health centre | 0 (0–31) | 0 (0–35) | 0 | ||
| Management of comorbidities | Hospital | 0 (0–58) | 29 (0–69) | 0 | 0.35 |
| Health centre | 25 (0–71) | 25 (0–71) | 0 | ||
| Recording and reporting adverse drug reactions | Hospital | 0 | 0 (0–4) | 0 | 0.35 |
| Health centre | 8 (0–100) | 8 (0–100) | 0 | ||
| Linkage to the DM or DM/HIV clinic after TB treatment | Hospital | 0(0–80) | 40 (0–90) | 0 | 0.19 |
| Health centre | 100 (50–100) | 100 (50–100) | 0 | ||
| General implementation of the standard, median (IQR) | Hospital | 25 (8–38) | 32 (25–46) | 4 (0–8) | 0.04 |
| Health centre | 49 (22–70) | 49 (22–70) | 0 | ||
| Characteristics | Subcategory | All n% | Dar n% | Iringa n% | Kilimanjaro n% | p-Value |
|---|---|---|---|---|---|---|
| Health care provider scores 1 | Nurses | 65.2 | 65.0 | 76.3 | 54.0 | 0.001 |
| Doctors/specialists | 55.0 | 67.2 | 49.0 | 55.0 | 0.665 | |
| Health facility score 2 | Cluster 1 | 76.2 | 61.9 | 73.3 | 76.2 | 0.966 |
| Cluster 2 | 57.1 | 81.0 | 53.3 | 57.1 | 0.091 | |
| Type of health facility score | Hospitals | 64.8 | 74.6 | 58.7 | 61.9 | 0.294 |
| Health centres | 69.7 | 72.2 | 68.6 | 69.2 | 0.795 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mpagama, S.G.; Byashalira, K.C.; Chamba, N.G.; Heysell, S.K.; Alimohamed, M.Z.; Shayo, P.J.; Kalolo, A.; Chongolo, A.M.; Gitige, C.G.; Mmbaga, B.T.; et al. Implementing Innovative Approaches to Improve Health Care Delivery Systems for Integrating Communicable and Non-Communicable Diseases Using Tuberculosis and Diabetes as a Model in Tanzania. Int. J. Environ. Res. Public Health 2023, 20, 6670. https://doi.org/10.3390/ijerph20176670
Mpagama SG, Byashalira KC, Chamba NG, Heysell SK, Alimohamed MZ, Shayo PJ, Kalolo A, Chongolo AM, Gitige CG, Mmbaga BT, et al. Implementing Innovative Approaches to Improve Health Care Delivery Systems for Integrating Communicable and Non-Communicable Diseases Using Tuberculosis and Diabetes as a Model in Tanzania. International Journal of Environmental Research and Public Health. 2023; 20(17):6670. https://doi.org/10.3390/ijerph20176670
Chicago/Turabian StyleMpagama, Stellah G., Kenneth C. Byashalira, Nyasatu G. Chamba, Scott K. Heysell, Mohamed Z. Alimohamed, Pendomartha J. Shayo, Albino Kalolo, Anna M. Chongolo, Catherine G. Gitige, Blandina T. Mmbaga, and et al. 2023. "Implementing Innovative Approaches to Improve Health Care Delivery Systems for Integrating Communicable and Non-Communicable Diseases Using Tuberculosis and Diabetes as a Model in Tanzania" International Journal of Environmental Research and Public Health 20, no. 17: 6670. https://doi.org/10.3390/ijerph20176670