

Habitual Physical Activity and Dietary Profiles in Older Japanese Males with Normal-Weight Obesity
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
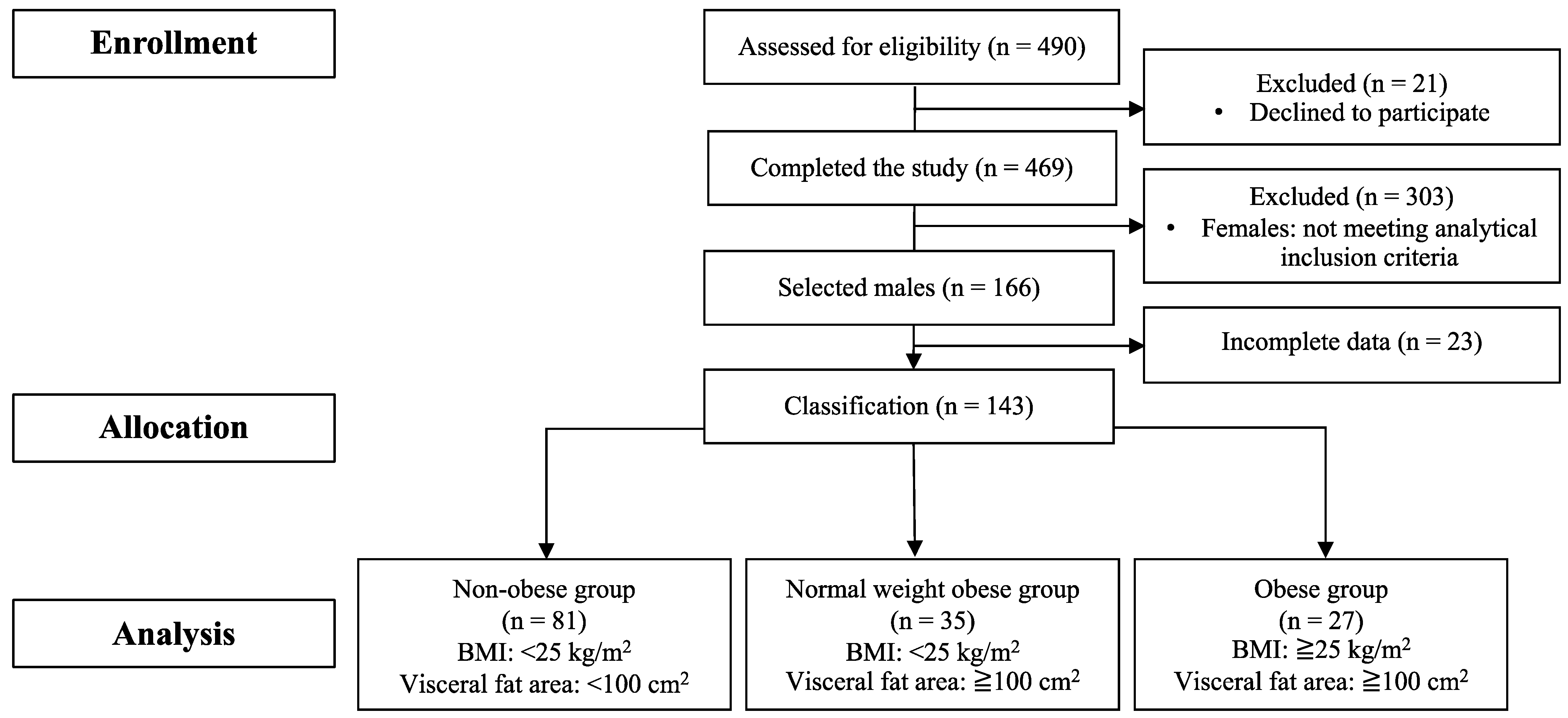
2.1. Participants
2.2. Anthropometric Measurements
2.3. Physical Activity Measurements
2.4. Physical Fitness Measurements
2.5. Dietary Record
2.6. Analytical Methods
2.7. Statistical Analyses
3. Results
3.1. Physical Characteristics
3.2. Blood Parameters
3.3. Physical Activity
3.4. Diet
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 11 April 2023).
- Neeland, I.J.; Turer, A.T.; Ayers, C.R.; Powell-Wiley, T.M.; Vega, G.L.; Farzaneh-Far, R.; Grundy, S.M.; Khera, A.; McGuire, D.K.; de Lemos, J.A. Dysfunctional adiposity and the risk of prediabetes and type 2 diabetes in obese adults. JAMA 2012, 308, 1150–1159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, Y.C.; Fujimoto, W.Y.; Hayashi, T.; Kahn, S.E.; Leonetti, D.L.; Boyko, E.J. Increased visceral adipose tissue is an independent predictor for future development of atherogenic dyslipidemia. J. Clin. Endocrinol. Metab. 2016, 101, 678–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, C.S.; Massaro, J.M.; Hoffmann, U.; Pou, K.M.; Maurovich-Horvat, P.; Liu, C.Y.; Vasan, R.S.; Murabito, J.M.; Meigs, J.B.; Cupples, L.A.; et al. Abdominal visceral and subcutaneous adipose tissue compartments: Association with metabolic risk factors in the Framingham Heart Study. Circulation 2007, 116, 39–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swainson, M.G.; Batterham, A.M.; Tsakirides, C.; Rutherford, Z.H.; Hind, K. Prediction of whole-body fat percentage and visceral adipose tissue mass from five anthrometric variable. PLoS ONE 2017, 12, e0177175. [Google Scholar] [CrossRef]
- Camhi, S.M.; Bray, G.A.; Bouchard, C.; Greenway, F.L.; Johnson, W.D.; Newton, R.L.; Ravussin, E.; Ryan, D.H.; Smith, S.R.; Katzmarzyk, P.T. The relationship of waist circumference and BMI to visceral, subcutaneous, and total body fat: Sex and race differences. Obesity 2011, 19, 402–408. [Google Scholar] [CrossRef]
- Examination Committee of Criteria for ‘Obesity Disease’ in Japan; Japan Society for the Study of Obesity. New criteria for ‘obesity disease’ in Japan. Circ. J. 2002, 66, 987–992. [Google Scholar] [CrossRef] [Green Version]
- De Lorenzo, A.; Soldati, L.; Sarlo, F.; Calvani, M.; Di Lorenzo, N.; Di Renzo, L. New obesity classification criteria as a tool for bariatric surgery indication. World J. Gastroenterol. 2016, 22, 681–703. [Google Scholar] [CrossRef]
- Franco, L.P.; Morais, C.C.; Cominetti, C. Normal-weight obesity syndrome: Diagnosis, prevalence, and clinical implications. Nutr. Rev. 2016, 74, 558–570. [Google Scholar] [CrossRef]
- Lemieux, S.; Prud’homme, D.; Bouchard, C.; Tremblay, A.; Després, J.P. Sex differences in the relation of visceral adipose tissue accumulation to total body fatness. Am. J. Clin. Nutr. 1993, 58, 463–467. [Google Scholar] [CrossRef]
- Kuk, J.L.; Lee, S.; Heymsfield, S.B.; Ross, R. Waist circumference and abdominal adipose tissue distribution: Influence of age and sex. Am. J. Clin. Nutr. 2005, 81, 1330–1334. [Google Scholar] [CrossRef] [Green Version]
- Tchernof, A.; Després, J.P. Pathophysiology of human visceral obesity: An update. Physiol. Rev. 2013, 93, 359–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seidell, J.C.; Björntorp, P.; Sjöström, L.; Kvist, H.; Sannerstedt, R. Visceral fat accumulation in men is positively associated with insulin, glucose, and C-peptide levels, but negatively with testosterone levels. Metabolism 1990, 39, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Lear, S.A.; Humphries, K.H.; Kohli, S.; Chockalingam, A.; Frohlich, J.J.; Birmingham, C.L. Visceral adipose tissue accumulation differs according to ethnic background: Results of the Multicultural Community Health Assessment Trial (M-CHAT). Am. J. Clin. Nutr. 2007, 86, 353–359. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, S.; Horimai, C.; Katsukawa, F. Ethnic differences in abdominal visceral fat accumulation between Japanese, African-Americans, and Caucasians: A meta-analysis. Acta Diabetol. 2003, 40, S302–S304. [Google Scholar] [CrossRef] [PubMed]
- Usui, I.; Tonabe, K. Role of organs in the development of diabetes. 4. Adipose tissue. Diabetol. Int. 2013, 56, 417–419. (In Japanese) [Google Scholar]
- Verheggen, R.J.; Maessen, M.F.; Green, D.J.; Hermus, A.R.; Hopman, M.T.; Thijssen, D.H. A systematic review and meta-analysis on the effects of exercise training versus hypocaloric diet: Distinct effects on body weight and visceral adipose tissue. Obes. Rev. 2016, 17, 664–690. [Google Scholar] [CrossRef]
- Leskinen, T.; Sipilä, S.; Alen, M.; Cheng, S.; Pietiläinen, K.H.; Usenius, J.P.; Suominen, H.; Kovanen, V.; Kainulainen, H.; Kaprio, J.; et al. Leisure-time physical activity and high-risk fat: A longitudinal population-based twin study. Int. J. Obes. 2009, 33, 1211–1218. [Google Scholar] [CrossRef] [Green Version]
- Fischer, K.; Pick, J.A.; Moewes, D.; Nöthlings, U. Qualitative aspects of diet affecting visceral and subcutaneous abdominal adipose tissue: A systematic review of observational and controlled intervention studies. Nutr. Rev. 2015, 73, 191–215. [Google Scholar] [CrossRef]
- Wijayatunga, N.N.; Dhurandhar, E.J. Normal weight obesity and unaddressed cardiometabolic health risk-a narrative review. Int. J. Obes. 2021, 45, 2141–2155. [Google Scholar] [CrossRef]
- Cassidy, S.; Chau, J.Y.; Catt, M.; Bauman, A.; Trenell, M.I. Low physical activity, high television viewing and poor sleep duration cluster in overweight and obese adults; a cross-sectional study of 398,984 participants from the UK Biobank. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 57. [Google Scholar] [CrossRef] [Green Version]
- Bell, J.A.; Hamer, M.; van Hees, V.T.; Singh-Manoux, A.; Kivimäki, M.; Sabia, S. Healthy obesity and objective physical activity. Am. J. Clin. Nutr. 2015, 102, 268–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Church, T.; Martin, C.K. The Obesity epidemic: A consequence of reduced energy expenditure and the uncoupling of energy intake? Obesity 2018, 26, 14–16. [Google Scholar] [CrossRef] [Green Version]
- Brook, J.S.; Lee, J.Y.; Finch, S.J.; Balka, E.B.; Brook, D.W. Physical factors, personal characteristics, and substance use: Associations with obesity. Subst. Abus. 2013, 34, 273–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeon, K.J.; Lee, O.; Kim, H.K.; Han, S.N. Comparison of the dietary intake and clinical characteristics of obese and normal weight adults. Nutr. Res. Pract. 2011, 5, 329–336. [Google Scholar] [CrossRef] [Green Version]
- Aballay, L.R.; Osella, A.R.; De La Quintana, A.G.; Diaz, M.D.P. Nutritional profile and obesity: Results from a random-sample population-based study in Córdoba, Argentina. Eur. J. Nutr. 2016, 55, 675–685. [Google Scholar] [CrossRef]
- Moradi, S.; Entezari, M.H.; Mohammadi, H.; Jayedi, A.; Lazaridi, A.V.; Kermani, M.A.H.; Miraghajani, M. Ultra-processed food consumption and adult obesity risk: A systematic review and dose-response meta-analysis. Crit. Rev. Food Sci. Nutr. 2023, 63, 249–260. [Google Scholar] [CrossRef]
- Fushimi, T.; Fujihira, K.; Takase, H.; Miyashita, M. Relationships among physical activity, physical function, and food intake in older Japanese adults living in urban areas: A cross-sectional study. Geriatrics 2023, 8, 41. [Google Scholar] [CrossRef] [PubMed]
- Ryo, M.; Maeda, K.; Onda, T.; Katashima, M.; Okumiya, A.; Nishida, M.; Yamaguchi, T.; Funahashi, T.; Matsuzawa, Y.; Nakamura, T.; et al. A new simple method for the measurement of visceral fat accumulation by bioelectrical impedance. Diabetes Care 2005, 28, 451–453. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, T.; Ozato, N.; Katashima, M.; Sawada, K.; Katsuragi, Y.; Ihara, K.; Nakaji, S. A novel method to visualize the dietary macronutrient composition of smaller visceral fat accumulation. Front. Nutr. 2020, 6, 194. [Google Scholar] [CrossRef] [PubMed]
- Kumahara, H.; Schutz, Y.; Ayabe, M.; Yoshioka, M.; Yoshitake, Y.; Shindo, M.; Ishii, K.; Tanaka, H. The use of uniaxial accelerometry for the assessment of physical-activity-related energy expenditure: A validation study against whole-body indirect calorimetry. Br. J. Nut. 2004, 91, 235–243. [Google Scholar] [CrossRef]
- Healy, G.N.; Clark, B.K.; Winkler, E.A.; Gardiner, P.A.; Brown, W.J.; Matthews, C.E. Measurement of adults’ sedentary time in population-based studies. Am. J. Prev. Med. 2011, 41, 216–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takase, H.; Sakane, N.; Morimoto, T.; Uchida, T.; Mori, K.; Katashima, M.; Katsuragi, Y. Development of a dietary factor assessment tool for evaluating associations between visceral fat accumulation and major nutrients in Japanese adults. J. Obes. 2019, 2019, 9497861. [Google Scholar] [CrossRef] [Green Version]
- The Council for Science and Technology, Ministry of Education, Culture, Sports, Science and Technology. 2015. Standard Tables of Food Composition in Japan. 2015. Available online: https://www.mext.go.jp/en/policy/science_technology/policy/title01/detail01/1374030.htm (accessed on 12 January 2023).
- Turner, R.C.; Holman, R.R.; Matthews, D.; Hockaday, T.D.; Peto, J. Insulin deficiency and insulin resistance interaction in diabetes: Estimation of their relative contribution by feedback analysis from basal plasma insulin and glucose concentrations. Metabolism 1979, 28, 1086–1096. [Google Scholar] [CrossRef]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and abuse of HOMA modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef] [Green Version]
- Bonora, E.; Targher, G.; Alberiche, M.; Bonadonna, R.C.; Saggiani, F.; Zenere, M.B.; Monauni, T.; Muggeo, M. Homeostasis model assessment closely mirrors the glucose clamp technique in the assessment of insulin sensitivity: Studies in subjects with various degrees of glucose tolerance and insulin sensitivity. Diabetes Care 2000, 23, 57–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L.Erlbaum Associates: Hillsdale, NJ, USA, 1998. [Google Scholar]
- Mochizuki, K.; Miyauchi, R.; Misaki, Y.; Shiamada, M.; Kasezawa, T.; Tohyama, K.; Goda, T. Accumulation of visceral fat is positively associated with serum ALT and γ-GTP activities in healthy and preclinical middle-aged Japanese men. J. Nutr. Sci. Vitaminol. 2011, 57, 65–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reaven, G.M. Syndrome X: 6 years later. J. Intern. Med. 1994, 736, 13–22. [Google Scholar]
- Hanley, A.J.; Wagenknecht, L.E.; Festa, A.; D’Agostino, R.B., Jr.; Haffner, S.M. Alanine aminotransferase and directly measured insulin sensitivity in a multiethnic cohort: The Insulin Resistance Atherosclerosis Study. Diabetes Care 2007, 30, 1819–1827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; Hu, T.; Zhang, S.; Zhou, L. Associations of different adipose tissue depots with insulin resistance: A systematic review and meta-analysis of observational studies. Sci. Rep. 2015, 5, 18495. [Google Scholar] [CrossRef] [Green Version]
- Okauchi, Y.; Nishizawa, H.; Funahashi, T.; Ogawa, T.; Noguchi, M.; Ryo, M.; Kihara, S.; Iwahashi, H.; Yamagata, K.; Nakamura, T.; et al. Reduction of visceral fat is associated with decrease in the number of metabolic risk factors in Japanese men. Diabetes Care 2007, 30, 2392–2394. [Google Scholar] [CrossRef] [Green Version]
- Ando, S.; Koyama, T.; Kuriyama, N.; Ozaki, E.; Uehara, R. The Association of daily physical activity behaviors with visceral fat. Obes. Res. Clin. Prac. 2020, 14, 531–535. [Google Scholar] [CrossRef] [PubMed]
- Winters-VAN Eekelen, E.; van der Velde, J.; Boone, S.C.; Westgate, K.; Brage, S.; Lamb, H.J.; Rosendaal, F.R.; de Mutsert, R. Objectively measured physical activity and body fatness: Associations with total body fat, visceral fat, and liver fat. Med. Sci. Sports Exerc. 2021, 53, 2309–2317. [Google Scholar] [CrossRef] [PubMed]
- Iliodromiti, S.; Ghouri, N.; Celis-Morales, C.A.; Sattar, N.; Lumsden, M.A.; Gill, J.M. Should physical activity recommendations for South Asian adults be ethnicity-specific? Evidence from a cross-sectional study of South Asian and White European men and Women. PLoS ONE 2016, 11, e0160024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagayama, C.; Burns, S.F.; Thackray, A.E.; Stensel, D.J.; Miyashita, M. Postprandial metabolism and physical activity in Asians: A narrative review. Int. J. Sports Med. 2021, 42, 953–966. [Google Scholar] [CrossRef] [PubMed]
- Ozato, N.; Saito, S.; Yamaguchi, T.; Katashima, M.; Tokuda, I.; Sawada, K.; Katsuragi, Y.; Imoto, S.; Ihara, K.; Nakaji, S. Association between nutrients and visceral fat in healthy Japanese adults: A 2-year longitudinal study. Nutrients 2019, 11, 2698. [Google Scholar] [CrossRef] [Green Version]
- Ramsey, K.A.; Rojer, A.G.M.; D’Andrea, L.; Otten, R.H.J.; Heymans, M.W.; Trappenburg, M.C.; Verlaan, S.; Whittaker, A.C.; Meskers, C.G.M.; Maier, A.B. The association of objectively measured physical activity and sedentary behavior with skeletal muscle strength and muscle power in older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2021, 67, 101266. [Google Scholar] [CrossRef]
- Fung, T.T.; Rimm, E.B.; Spiegelman, D.; Rifai, N.; Tofler, G.H.; Willett, W.C.; Hu, F.B. Association between dietary patterns and plasma biomarkers of obesity and cardiovascular disease risk. Am. J. Clin. Nutr. 2001, 73, 61–67. [Google Scholar] [CrossRef] [Green Version]
- Dhurandhar, N.V.; Schoeller, D.; Brown, A.W.; Heymsfield, S.B.; Thomas, D.; Sørensen, T.I.; Speakman, J.R.; Jeansonne, M.; Allison, D.B.; Energy Balance Measurement Working Group. Energy balance measurement working group. Energy balance measurement: When something is not better than nothing. Int. J. Obes. 2015, 39, 1109–1113. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Obese Group (n = 27) | Normal-Weight Obese Group (n = 35) | Non-Obese Group (n = 81) | Main Effect of Group (p Value) | |
|---|---|---|---|---|
| Age (year) | 70.0 (3.3) | 70.0 (2.9) | 70.4 (2.9) | NS |
| Height (m) | 1.66 (0.07) | 1.68 (0.05) | 1.67 (0.05) | NS |
| Body mass (kg) | 75.6 (7.9) *,† | 65.0 (5.2) * | 61.1 (5.3) | <0.05 |
| Body mass index (kg/m2) | 27.3 (2.0) *,† | 23.1 (1.3) * | 21.9 (1.6) | <0.05 |
| Visceral fat area (cm2) | 149.7 (36.8) *,† | 125.9 (20.8) * | 63.8 (22.0) | <0.05 |
| Systolic blood pressure (mmHg) | 146 (21) | 143 (28) | 141 (22) | NS |
| Diastolic blood pressure (mmHg) | 83 (12) | 84 (13) | 82 (12) | NS |
| Grip strength (kg) | 36.2 (7.6) | 33.2 (8.6) | 34.1 (7.0) | NS |
| Functional Reach Test (cm) | 35.4 (6.7) | 35.4 (6.2) | 35.5 (6.4) | NS |
| OCS-20 (count) | 29 (6) | 29 (5) | 30 (5) | NS |
| Knee strength (kgf/kg) | 0.41 (0.12) | 0.40 (0.15) | 0.40 (0.10) | NS |
| One-leg standing with vision (s) | 57 (40) * | 50 (44) * | 81 (46) | <0.05 |
| Timed Up and Go Test (s) | 5.59 (1.10) | 5.61 (0.89) | 5.64 (0.83) | NS |
| Obese Group (n = 27) | Normal-Weight Obese Group (n = 35) | Non-Obese Group (n = 81) | Main Effect of Group (p Value) | |
|---|---|---|---|---|
| Glucose (mmol/L) | 6.2 (1.1) * | 5.8 (1.0) | 5.6 (0.8) | <0.05 |
| HbA1c (%) | 5.9 (0.7) * | 5.7 (0.5) | 5.6 (0.4) | <0.05 |
| Insulin (pmol/L) | 58.3 (54.6) * | 35.6 (16.8) | 31.9 (25.5) | <0.05 |
| HOMA-IR | 2.4 (2.5) *,† | 1.3 (0.6) | 1.1 (1.0) | <0.05 |
| HOMA-β | 61.1 (44.4) | 46.8 (21.3) | 43.8 (34.1) | NS |
| GIP (pmol/L) | 132.3 (150.0) | 95.3 (87.3) | 122.2 (147.6) | NS |
| Triglyceride (mmol/L) | 1.4 (0.6) | 1.6 (0.8) * | 1.1 (1.0) | <0.05 |
| NEFA (mmol/L) | 0.63 (0.29) | 0.64 (0.23) | 0.60 (0.26) | NS |
| HDL-C (mmol/L) | 1.5 (0.4) | 1.4 (0.3) * | 1.7 (0.4) | <0.05 |
| LDL-C (mmol/L) | 3.3 (0.8) | 3.3 (0.7) | 3.1 (0.7) | NS |
| AST (U/L) | 25.5 (8.8) | 24.8 (6.3) | 24.4 (8.0) | NS |
| ALT (U/L) | 24.9 (10.2) * | 22.5 (9.4) * | 18.3 (6.3) | <0.05 |
| γ-GTP (U/L) | 50.9 (69.9) | 40.0 (19.3) | 36.5 (40.7) | NS |
| Obese Group (n = 27) | Normal-Weight Obese Group (n = 35) | Non-Obese Group (n = 81) | Main Effect of Group (p Value) | |
|---|---|---|---|---|
| Steps (steps/day) | 7431 (3015) * | 8286 (2766) | 9562 (3438) | <0.05 |
| Total physical activity (min/day) | 78 (31) * | 86 (27) | 98 (33) | <0.05 |
| Light-intensity physical activity (min/day) | 56 (23) | 59 (19) | 66 (23) | NS |
| Moderate-intensity physical activity (min/day) | 21 (17) | 26 (16) | 31 (21) | NS |
| Vigorous-intensity physical activity (min/day) | 1 (1) * | 1 (1) * | 2 (4) | <0.05 |
| Obese Group (n = 27) | Normal-Weight Obese Group (n = 35) | Non-Obese Group (n = 81) | Main Effect of Group (p Value) | |
|---|---|---|---|---|
| Energy intake (kJ/day) | ||||
| Total energy intake | 9062 (1278) | 9101 (1432) | 9357 (1539) | NS |
| Breakfast | 2226 (513) | 2546 (712) | 2356 (667) | NS |
| Lunch | 2531 (614) | 2549 (770) | 2520 (700) | NS |
| Dinner | 3192 (594) | 3527 (993) | 3479 (922) | NS |
| Snacks | 910 (793) | 702 (736) | 966 (845) | NS |
| Food group (kJ/day) | ||||
| Cereals | 3020 (621) | 3008 (577) | 3017 (662) | NS |
| Potatoes and starches | 133 (128) | 130 (101) | 152 (124) | NS |
| Sugars and sweeteners | 106 (60) | 116 (79) | 106 (81) | NS |
| Pulses | 394 (321) | 299 (234) | 354 (275) | NS |
| Nuts and seeds | 81 (29) *,† | 102 (32) | 104 (42) | <0.05 |
| Vegetables | 340 (121) *,† | 427 (133) | 436 (176) | <0.05 |
| Fruits | 391 (288) | 347 (217) | 371 (254) | NS |
| Mushrooms | 6 (5) | 9 (12) | 9 (13) | NS |
| Algae | 16 (23) | 16 (40) | 12 (15) | NS |
| Fish, mollusks and crustaceans | 511 (347) | 610 (400) | 554 (303) | NS |
| Meat | 898 (440) | 984 (436) | 985 (499) | NS |
| Eggs | 340 (154) | 289 (167) | 273 (152) | NS |
| Milk and milk products | 499 (407) | 641 (481) | 632 (448) | NS |
| Fats and oils | 520 (246) | 588 (277) | 553 (247) | NS |
| Confectionaries | 539 (539) | 280 (346) | 349 (416) | NS |
| Beverages | 696 (535) | 684 (712) | 800 (864) | NS |
| Seasonings and spices | 362 (161) | 453 (239) | 437 (220) | NS |
| Prepared foods | 30 (78) | 0 (0) | 18 (73) | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tataka, Y.; Hiratsu, A.; Fujihira, K.; Nagayama, C.; Kamemoto, K.; Fushimi, T.; Takase, H.; Miyashita, M. Habitual Physical Activity and Dietary Profiles in Older Japanese Males with Normal-Weight Obesity. Int. J. Environ. Res. Public Health 2023, 20, 6408. https://doi.org/10.3390/ijerph20146408
Tataka Y, Hiratsu A, Fujihira K, Nagayama C, Kamemoto K, Fushimi T, Takase H, Miyashita M. Habitual Physical Activity and Dietary Profiles in Older Japanese Males with Normal-Weight Obesity. International Journal of Environmental Research and Public Health. 2023; 20(14):6408. https://doi.org/10.3390/ijerph20146408
Chicago/Turabian StyleTataka, Yusei, Ayano Hiratsu, Kyoko Fujihira, Chihiro Nagayama, Kayoko Kamemoto, Takashi Fushimi, Hideto Takase, and Masashi Miyashita. 2023. "Habitual Physical Activity and Dietary Profiles in Older Japanese Males with Normal-Weight Obesity" International Journal of Environmental Research and Public Health 20, no. 14: 6408. https://doi.org/10.3390/ijerph20146408