
Parent and Carer Skills Groups in Dialectical Behaviour Therapy for High-Risk Adolescents with Severe Emotion Dysregulation: A Mixed-Methods Evaluation of Participants’ Outcomes and Experiences
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Intervention
2.3. Study Design
2.4. Participants
2.5. Therapists
2.6. Procedures
2.7. Measures
2.8. Data Analysis
2.9. Ethics
3. Results
3.1. Quantitative Findings
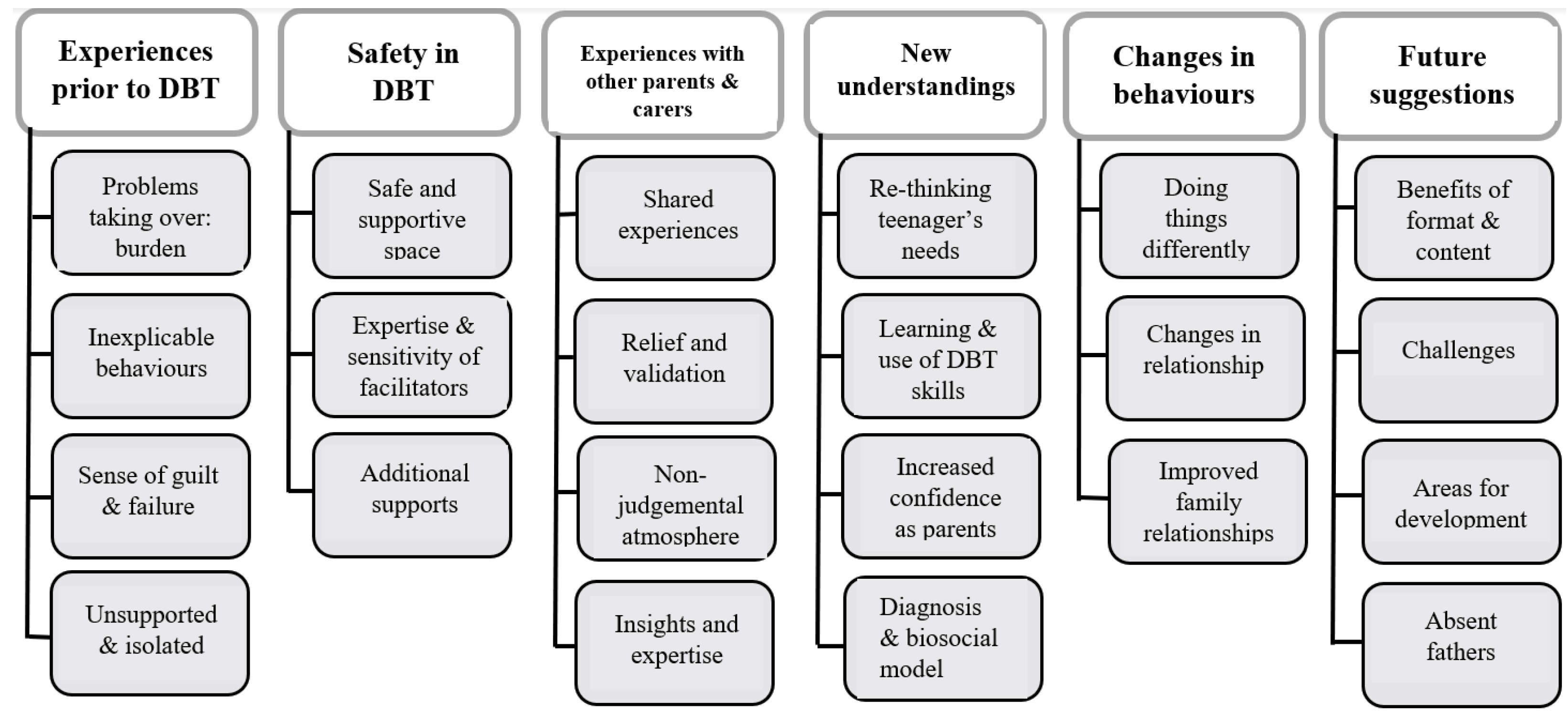
3.2. Qualitative Findings
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rathus, J.H.; Miller, A.L. Dialectical behavior therapy adapted for suicidal adolescents. Suicide Life-Threat. Behav. 2002, 32, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.L.; Rathus, J.H.; Linehan, M.M. Dialectical Behavior Therapy with Suicidal Adolescents; Guilford Press: New York, NY, USA, 2007. [Google Scholar]
- National Institute for Health and Care Excellence. Self-Harm: Assessment, Management and Preventing Recurrence; NICE Guideline NG 225; National Institute for Health and Care Excellence: London, UK, 2022; Available online: https://www.nice.org.uk/guidance/ng225 (accessed on 7 September 2022).
- Linehan, M. Cognitive-Behavioral Treatment of Borderline Personality Disorder; Guildford Press: New York, NY, USA, 1993. [Google Scholar]
- Linehan, M.M.; Comtois, K.A.; Murray, A.M.; Brown, M.Z.; Gallop, R.J.; Heard, H.L.; Korslund, K.E.; Tutek, D.A.; Reynolds, S.K.; Lindenboim, N. Two-year randomized controlled trial and follow-up of dialectical behavior therapy vs therapy by experts for suicidal behaviors and borderline personality disorder. Arch. Gen. Psychiatry 2006, 63, 757–766, Erratum in Arch. Gen. Psychiatry 2007, 64, 1401. [Google Scholar] [CrossRef] [Green Version]
- McMain, S.F.; Links, P.S.; Gnam, W.H.; Guimond, T.; Cardish, R.J.; Korman, L.; Streiner, D.L. A randomized trial of dialectical behavior therapy versus general psychiatric management for borderline personality disorder. Am. J. Psychiatry 2009, 166, 1365–1374, Erratum in Am. J. Psychiatry 2010, 167, 1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehlum, L.; Tørmoen, A.J.; Ramberg, M.; Haga, E.; Diep, L.M.; Laberg, S.; Larsson, B.S.; Stanley, B.H.; Miller, A.L.; Sund, A.M.; et al. Dialectical behavior therapy for adolescents with repeated suicidal and self-harming behavior: A randomized trial. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 1082–1091. [Google Scholar] [CrossRef] [Green Version]
- McCauley, E.; Berk, M.S.; Asarnow, J.R.; Adrian, M.; Cohen, J.; Korslund, K.; Avina, C.; Hughes, J.; Harned, M.; Gallop, R.; et al. Efficacy of Dialectical Behavior Therapy for Adolescents at High Risk for Suicide: A Randomized Clinical Trial. JAMA Psychiatry 2018, 75, 777–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santamarina-Perez, P.; Mendez, I.; Singh, M.K.; Berk, M.; Picado, M.; Font, E.; Moreno, E.; Martínez, E.; Morer, A.; Borràs, R.; et al. Adapted Dialectical Behavior Therapy for Adolescents with a High Risk of Suicide in a Community Clinic: A Pragmatic Randomized Controlled Trial. Suicide Life Threat Behav. 2020, 50, 652–667. [Google Scholar] [CrossRef]
- Bahji, A.; Pierce, M.; Wong, J.; Roberge, J.N.; Ortega, I.; Patten, S. Comparative Efficacy and Acceptability of Psychotherapies for Self-harm and Suicidal Behavior Among Children and Adolescents: A Systematic Review and Network Meta-analysis. JAMA Netw. Open. 2021, 4, e216614. [Google Scholar] [CrossRef]
- Arbuthnott, A.E.; Lewis, S.P. Parents of youth who self-injure: A review of the literature and implications for mental health professionals. Child Adolesc. Psychiatry Ment. Health 2015, 9, 35. [Google Scholar] [CrossRef] [Green Version]
- Stepp, S.D.; Whalen, D.J.; Scott, L.N.; Zalewski, M.; Loeber, R.; Hipwell, A.E. Reciprocal-effects of parenting and borderline personality disorder symptoms in adolescent girls. Dev. Psychopathol. 2014, 26, 361–378. [Google Scholar] [CrossRef] [Green Version]
- Sutherland, R.; Baker, J.; Prince, S. Support, interventions and outcomes for families/carers of people with borderline personality disorder: A systematic review. Personal. Ment. Health 2020, 14, 199–214. [Google Scholar] [CrossRef]
- Reinelt, E.; Stopsack, M.; Aldinger, M.; Ulrich, I.; Grabe, H.J.; Barnow, S. Longitudinal transmission pathways of borderline personality disorder symptoms: From mother to child. Psychopathology 2013, 47, 10–16. [Google Scholar] [CrossRef]
- Carlson, E.A.; Egeland, B.; Sroufe, L.A. A prospective study of the development of borderline personality symptoms. Dev. Psychopathol. 2009, 21, 1311–1334. [Google Scholar] [CrossRef] [PubMed]
- Fruzzetti, A.E.; Iverson, K.M. Intervening With Couples and Families to Treat Emotion Dysregulation and Psychopathology. In Emotion Regulation in Couples and Families: Pathways to Dysfunction and Health; Snyder, D.K., Simpson, J., Hughes, J.N., Eds.; American Psychological Association: Washington, DC, USA, 2006; pp. 249–267. [Google Scholar] [CrossRef]
- Hoffman, P.D.; Fruzzetti, A.E.; Buteau, E.; Neiditch, E.R.; Penney, D.; Bruce, M.L.; Hellman, F.; Struening, E. Family connections: A program for relatives of persons with borderline personality disorder. Fam. Process. 2005, 44, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Flynn, D.; Kells, M.; Joyce, M.; Corcoran, P.; Herley, S.; Suarez, C.; Cotter, P.; Hurley, J.; Weihrauch, M.; Groeger, J. Family Connections versus optimised treatment-as-usual for family members of individuals with borderline personality disorder: Non-randomised controlled study. Borderline Pers. Disord Emot. Dysregul. 2017, 4, 18. [Google Scholar] [CrossRef] [PubMed]
- Boritz, T.Z.; Sheikhan, N.Y.; Hawke, L.D.; McMain, S.F.; Henderson, J. Evaluating the effectiveness of the Family Connections program for caregivers of youth with mental health challenges, part I: A quantitative analysis. Health Expect. 2021, 24, 578–588. [Google Scholar] [CrossRef] [PubMed]
- Woodberry, K.; Popenoe, E. Implementing Dialectical Behavior Therapy With Adolescents and Their Families in a Community Outpatient Clinic. Cogn. Behav. Pract. 2008, 15, 277–286. [Google Scholar] [CrossRef]
- Scheirs, J.G.; Bok, S. Psychological distress in caretakers or relatives of patients with borderline personality disorder. Int. J. Soc. Psychiatry 2007, 53, 195–203. [Google Scholar] [CrossRef]
- Rizvi, S.L.; Steffel, L.M.; Carson-Wong, A. An overview of dialectical behaviour therapy for professional psychologists. Prof. Psychol. Res. Pract. 2013, 44, 73–80. [Google Scholar] [CrossRef]
- Ekdahl, S.; Idvall, E.; Samuelsson, M.; Perseius, K.-I. A life tiptoeing: Being a significant other to persons with borderline personality disorder. Arch. Psychiatr. Nurs. 2011, 25, 69–76. [Google Scholar] [CrossRef]
- Byrne, S.; Morgan, S.; Fitzpatrick, C.; Boylan, C.; Crowley, S.; Gahan, H.; Howley, J.; Staunton, D.; Guerin, S. Deliberate self-harm in children and adolescents: A qualitative study exploring the needs of parents and carers. Clin. Child Psychol. Psychiatry 2008, 13, 493–504. [Google Scholar] [CrossRef]
- Oldershaw, A.; Richards, C.; Simic, M.; Schmidt, U. Parents’ perspectives on adolescent self-harm: Qualitative study. Br. J. Psychiatry 2008, 193, 140–144. [Google Scholar] [CrossRef]
- Flynn, D.; Gillespie, C.; Joyce, M.; Spillane, A. An evaluation of the skills group component of DBT-A for parent/guardians: A mixed methods study. Ir. J. Psychol. Med. 2020, 40, 143–151. [Google Scholar] [CrossRef] [PubMed]
- First, M.B.; Spitzer, R.L.; Gibbon, M.; Williams, J.B.W. Structured Clinical Interview for DSM-IV Personality Disorders, (SCID-II); American Psychiatric Press, Inc.: Washington, DC, USA, 1997. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cramm, J.M.; Nieboer, A.P. Psychological well-being of caregivers of children with intellectual disabilities: Using parental stress as a mediating factor. J. Intellect. Disabil. 2011, 15, 101–113. [Google Scholar] [CrossRef]
- Olson, D. Family Inventories: Inventories Used in a National Survey of Families Across the Life Cycle; Family Social Science: Minneapolis, MN, USA, 1985. [Google Scholar]
- Gubert, F.D.A.; Vieira, N.F.C.; Pinheiro, P.N.D.C.; Oriá, M.O.B.; Almeida, P.C.D.; Araújo, T.S.D. Translation and validation of the Parent-adolescent Communication Scale: Technology for DST/HIV prevention. Rev. Lat. Am. Enferm. 2013, 21, 851–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sales, J.M.; Milhausen, R.R.; Wingood, G.M.; DiClemente, R.J.; Salazar, L.F.; Crosby, R.A. Validation of a Parent-Adolescent Communication Scale for Use in STD/HIV Prevention Interventions. Health Educ. Behav. 2008, 35, 332–345. [Google Scholar] [CrossRef] [PubMed]
- Stratton, P.; Bland, J.; Janes, E.; Lask, J. Developing an indicator of family function and a practicable outcome measure for systemic family and couple therapy: The SCORE. J. Fam. Ther. 2010, 32, 232–258. [Google Scholar] [CrossRef]
- Hamilton, E.; Carr, A. Systematic Review of Self-Report Family Assessment Measures. Fam. Process 2016, 55, 16–30. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988. [Google Scholar]
- SPSS. IBM Corp. IBM SPSS Statistics for Windows; Version 22.0; Released 2013; IBM Corp.: Armonk, NY, USA, 2013. [Google Scholar]
- Braun, V.; Clarke, V. Successful Qualitative Research: A Practical Guide for Beginners; SAGE Publications: London, UK, 2013. [Google Scholar]
- Fruzzetti, A.E. Dialectical behaviour therapy with parents, couples, and families to augment Stage 1 outcome. In The Oxford Handbook of Dialectical Behaviour Therapy; Swales, M.A., Ed.; Oxford University Press: Oxford, UK, 2019; pp. 389–411. [Google Scholar]
- Ferrey, A.E.; Hughes, N.D.; Simkin, S.; Locock, L.; Stewart, A.; Kapur, N.; Gunnell, D.; Hawton, K. The impact of self-harm by young people on parents and families: A qualitative study. BMJ Open 2016, 6, e009631. [Google Scholar] [CrossRef] [Green Version]
- Nixon, M.K.; McLagan, L.; Landell, S.; Carter, A.; Deshaw, M. Developing and Piloting Community-Based Self-Injury Treatment Groups for Adolescents and Their Parents. Can. Child Adolesc. Psychiatry Rev. 2004, 13, 62–67. [Google Scholar]
- Linehan, M.M.; Korslund, K.E.; Harned, M.S.; Gallop, R.J.; Lungu, A.; Neacsiu, A.D.; McDavid, J.; Comtois, K.A.; Murray-Gregory, A.M. Dialectical behavior therapy for high suicide risk in individuals with borderline personality disorder: A randomized clinical trial and component analysis. JAMA Psychiatry 2015, 72, 475–482, Erratum in JAMA Psychiatry 2015, 72, 951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilks, C.R.; Valenstein-Mah, H.; Tran, H.; King, A.M.M.; Lungu, A.; Linehan, M.M. Dialectical behavior therapy skills for families of individuals with behavioral disorders: Initial feasibility and outcomes. Cogn. Behav. Pract. 2017, 24, 288–295. [Google Scholar] [CrossRef]
- Fruzzetti, A.E.; Shenk, C.; Hoffman, P.D. Family interaction and the development of borderline personality disorder: A transactional model. Dev. Psychopathol. 2005, 17, 1007–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fruzzetti, A.; Worrall, J. Accurate Expression and Validating Responses: A Transactional Model for Understanding Individual and Relationship Distress. Support Process. Intim. Relatsh. 2010, 11, 121–150. [Google Scholar] [CrossRef]
- Panter-Brick, C.; Burgess, A.; Eggerman, M.; McAllister, F.; Pruett, K.; Leckman, J.F. Practitioner review: Engaging fathers–recommendations for a game change in parenting interventions based on a systematic review of the global evidence. J. Child Psychol. Psychiatry 2014, 55, 1187–1212. [Google Scholar] [CrossRef]
- Tiano, J.D.; McNeil, C.B. The inclusion of fathers in behavioral parent training: A critical evaluation. Child Fam. Behav. Ther. 2005, 27, 1–28. [Google Scholar] [CrossRef]
- Bögels, S.; Phares, V. Fathers’ role in the etiology, prevention and treatment of child anxiety: A review and new model. Clin. Psychol. Rev. 2008, 28, 539–558. [Google Scholar] [CrossRef]
- Tully, L.A.; Piotrowska, P.J.; Collins, D.A.J.; Mairet, K.S.; Black, N.; Kimonis, E.R.; Hawes, D.J.; Moul, C.; Lenroot, R.K.; Frick, P.J.; et al. Optimising child outcomes from parenting interventions: Fathers’ experiences, preferences and barriers to participation. BMC Public Health 2017, 17, 550. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Thematic Analysis: A Practical Guide; SAGE Publications: London, UK, 2022. [Google Scholar]


{kind=link}
| Round | Week | Topic |
|---|---|---|
| 1 | 1–2 | Orientation/Biosocial Theory |
| 3–4 | Understanding and Responding to Self-Harm and Suicidal Behaviour | |
| 5–7 | Distress Tolerance | |
| 2 | 8 | Validation (1) (+mini-orientation) |
| 9–11 | Interpersonal Effectiveness | |
| 12–14 | Emotion Regulation | |
| 3 | 15–17 | Ways to Increase & Decrease Behaviours (+mini-orientation) |
| 18 | Validation (2) | |
| 19–21 | Walking the Middle Path |
| Characteristics | Quantitative Study %, (N = 41) | Qualitative Study %, (N = 8) |
|---|---|---|
| Gender of parent/carer: | ||
| Female | 76 | 75 |
| Male | 24 | 25 |
| Gender of adolescent: | ||
| Female | 93 | 88 |
| Kinship to adolescent: | ||
| Mother | 76 | |
| Father | 22 | |
| Other family member | 2 | |
| Ethnicity: | ||
| White British | 68 | 88 |
| White European | 15 | 12 |
| Black British/Black Caribbean | 5 | |
| Black African | 5 | |
| Asian | 5 | |
| Arabic | 2 | |
| Age range | ||
| 35–44 | - | 50 (4) |
| 45–54 | - | 25 (2) |
| 55–64 | - | 25 (2) |
| Measure | Group Mean (SD) | t Value | Cohen’s d | |
|---|---|---|---|---|
| Time 1 (N = 41) | Time 2 (N = 41) | |||
| HADS Depression | 7.44 (4.34) | 5.39 (3.49) | 3.80 *** | 0.59 |
| HADS Anxiety | 10.71 (4.09) | 8.49 (3.08) | 4.30 *** | 0.67 |
| PACS Total | 58.52 (12.51) | 63.46 (13.19) | −3.55 ** | −0.56 |
| PACS Problems in Family Communication | 27.21 (6.62) | 29.15 (6.60) | −2.09 * | −0.33 |
| PACS Open Family Communication | 31.32 (8.23) | 34.32 (8.09) | −4.10 *** | −0.64 |
| SCORE-15 Strengths and Adaptability | 2.45 (0.82) | 2.22 (0.69) | 2.19 * | 0.34 |
| SCORE-15 Overwhelmed by Difficulties | 2.61 (0.93) | 2.53 (0.78) | 0.67 | 0.10 |
| SCORE-15 Disrupted Communication | 2.42 (0.78) | 2.29 (0.56) | 1.26 | 0.20 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, L.; Hunt, K.; Parker, S.; Camp, J.; Stewart, C.; Morris, A. Parent and Carer Skills Groups in Dialectical Behaviour Therapy for High-Risk Adolescents with Severe Emotion Dysregulation: A Mixed-Methods Evaluation of Participants’ Outcomes and Experiences. Int. J. Environ. Res. Public Health 2023, 20, 6334. https://doi.org/10.3390/ijerph20146334
Smith L, Hunt K, Parker S, Camp J, Stewart C, Morris A. Parent and Carer Skills Groups in Dialectical Behaviour Therapy for High-Risk Adolescents with Severe Emotion Dysregulation: A Mixed-Methods Evaluation of Participants’ Outcomes and Experiences. International Journal of Environmental Research and Public Health. 2023; 20(14):6334. https://doi.org/10.3390/ijerph20146334
Chicago/Turabian StyleSmith, Lindsay, Katrina Hunt, Sam Parker, Jake Camp, Catherine Stewart, and Andre Morris. 2023. "Parent and Carer Skills Groups in Dialectical Behaviour Therapy for High-Risk Adolescents with Severe Emotion Dysregulation: A Mixed-Methods Evaluation of Participants’ Outcomes and Experiences" International Journal of Environmental Research and Public Health 20, no. 14: 6334. https://doi.org/10.3390/ijerph20146334