
Effects of Transitional Care after Hospital Discharge in Patients with Chronic Obstructive Pulmonary Disease: An Updated Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Study Selection
2.4. Data Extraction and Quality Appraisal
2.5. Data Analysis
3. Results
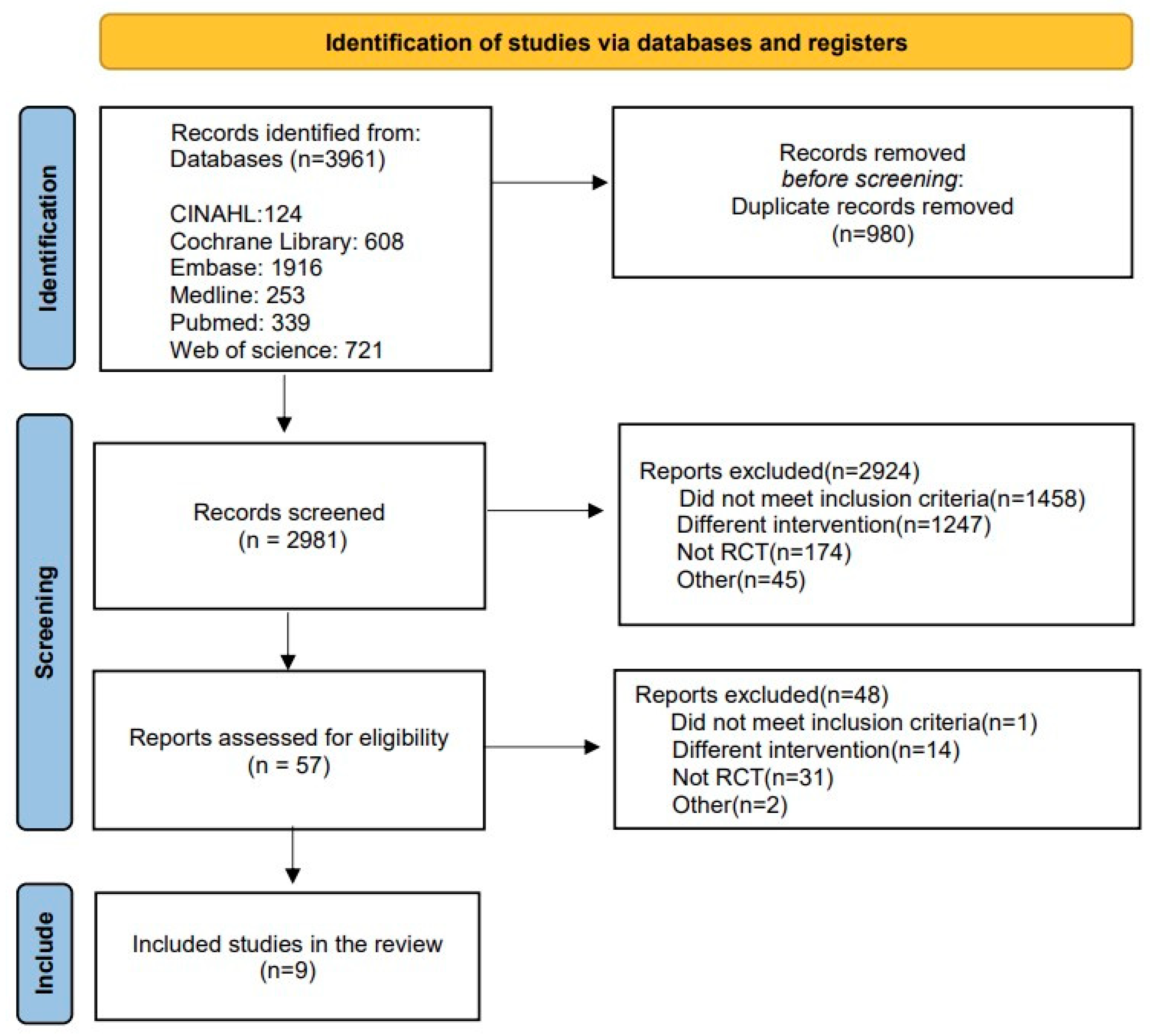
3.1. Study Selection
3.2. Study Characteristics
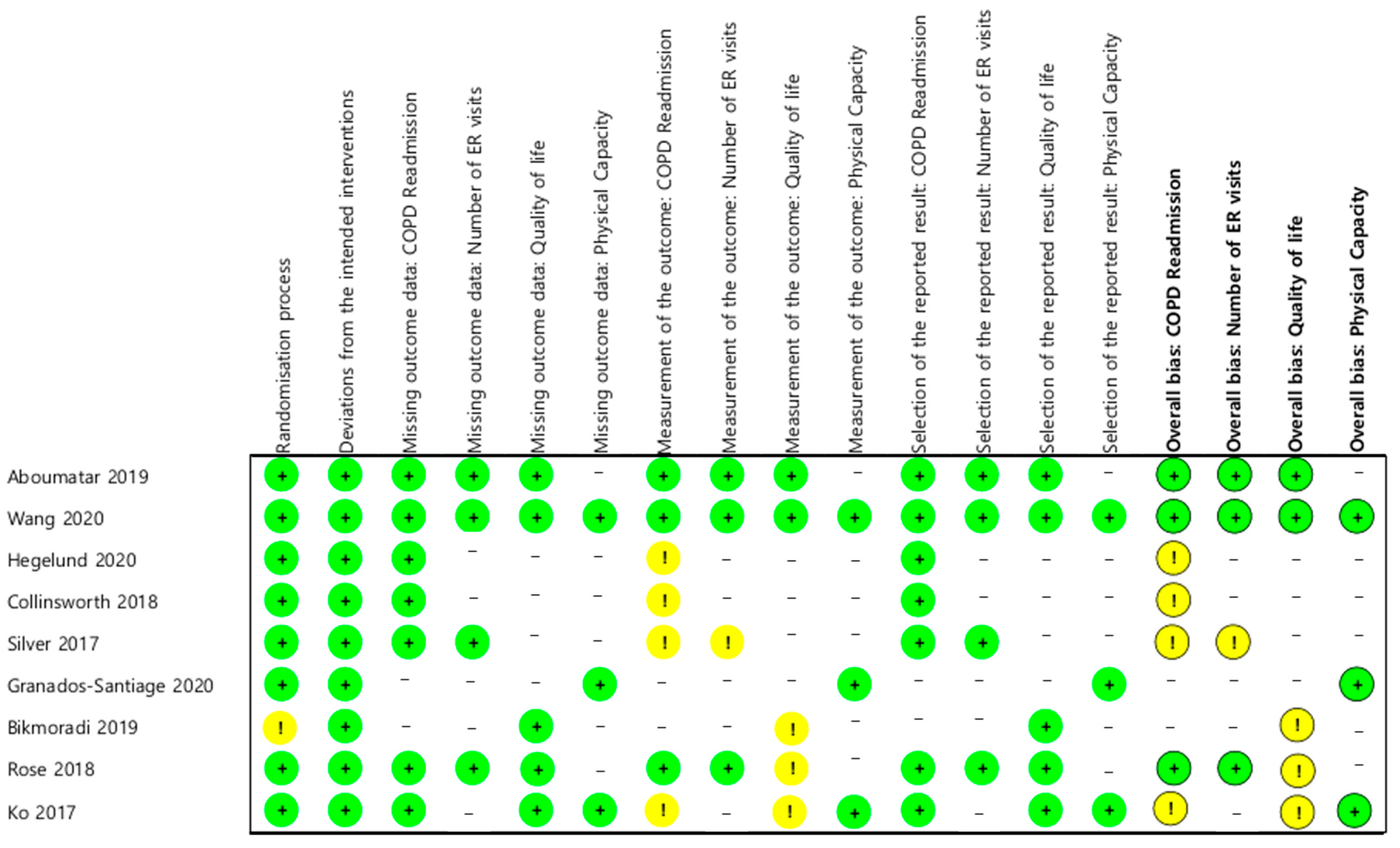
3.3. Risk of Bias
3.4. Meta-Analysis Results
3.4.1. Effect on Healthcare Utilization: Readmission and Number of ER Visits for COPD
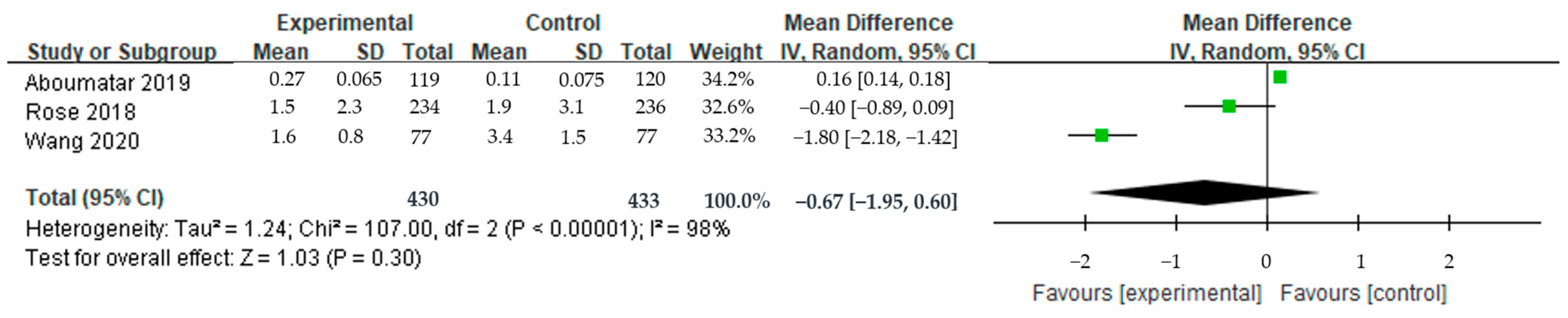
3.4.2. Effect on Health and Quality of Life: SGRQ Total Score, Physical Capacity
3.5. Sensitivity Analysis
3.6. Systematic Review of Other Outcomes and Related Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Fabbri, L.M.; Frith, P.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Bhutta, Z.A. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- López-Campos, J.L.; Ruiz-Ramos, M.; Soriano, J.B. Mortality trends in chronic obstructive pulmonary disease in Europe, 1994–2010: A joinpoint regression analysis. Lancet Respir. Med. 2014, 2, 54–62. [Google Scholar] [CrossRef]
- Mei, F.; Dalmartello, M.; Bonifazi, M.; Bertuccio, P.; Levi, F.; Boffetta, P.; Negri, E.; Vecchia, C.L.; Malvezzi, M. Chronic Obstructive Pulmonary Disease (COPD) mortality trends worldwide: An update to 2019. Respirology 2022, 27, 941–950. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Available online: http://goldcopd.org (accessed on 20 May 2023).
- Soriano, J.B.; Abajobir, A.A.; Abate, K.H.; Abera, S.F.; Agrawal, A.; Ahmed, M.B.; Vos, T. Global, Regional, and National Deaths, Prevalence, Disability-Adjusted Life Years, and Years Lived with Disability for Chronic Obstructive Pulmonary Disease and Asthma, 1990-2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, C.J.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Borzouei, S. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.J.; Park, K.M. Analysis of Research about Pulmonary Rehabilitation of Patients with COPD. J. Korean Community Nurs. 2003, 14, 312–322. [Google Scholar]
- Jo, H.S.; Jeong, S.; Kim, W.J.; Park, S.; Yu, S.A. Development of a transitional care model program for patients with pneumonia, asthma, and chronic obstructive pulmonary disease: In-depth interviews with readmitted patients. J. Korean Med. Sci. 2020, 35, e352. [Google Scholar] [CrossRef]
- Birtwell, K.; Planner, C.; Hodkinson, A.; Hall, A.; Giles, S.; Campbell, S.; Daker-White, G. Transitional Care Interventions for Older Residents of Long-Term Care Facilities: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2210192. [Google Scholar] [CrossRef]
- Aboumatar, H.; Naqibuddin, M.; Chung, S.; Adebowale, H.; Bone, L.; Brown, T.; Pronovost, P. Better Respiratory Education and Treatment Help Empower (BREATHE) study: Methodology and baseline characteristics of a randomized controlled trial testing a transitional care program to improve patient-centered care delivery among chronic obstructive pulmonary disease patients. Contemp. Clin. Trials 2017, 62, 159–167. [Google Scholar] [CrossRef]
- Kim, Y.S.; Shin, J.Y.; Kim, K.J.; Lee, J.M.; Lee, K.S.; Choi, J.K.; Han, S.H. Clinical Practice Guideline for Care Transition. Korean J. Clin. Geriatr. 2018, 19, 27–37. [Google Scholar] [CrossRef]
- Dronina, Y.; Kim, S.K.; Jo, H.S. Predictors of the need for post-discharge transitional care services in older adults: A cross-sectional analysis. J. Korean Gerontol. Soc. 2022, 42, 787–803. [Google Scholar] [CrossRef]
- Naylor, M.D. Transitional care of older adults. Annu. Rev. Nurs. Res. 2002, 20, 127–147. [Google Scholar] [CrossRef] [PubMed]
- Graham, C.L.; Ivey, S.L.; Neuhauser, L. From hospital to home: Assessing the transitional care needs of vulnerable seniors. Gerontologist 2009, 49, 23–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benzo, R.; Vickers, K.; Novotny, P.J.; Tucker, S.; Hoult, J.; Neuenfeldt, P.; Connett, J.; Lorig, K.; McEvoy, C. Health coaching and chronic obstructive pulmonary disease rehospitalization. A randomized study. Am. J. Respir. Crit. Care Med. 2016, 194, 672–680. [Google Scholar] [CrossRef] [Green Version]
- Ko, F.W.; Cheung, N.K.; Rainer, T.H.; Lum, C.; Wong, I.; Hui, D.S. Comprehensive care programme for patients with chronic obstructive pulmonary disease: A randomised controlled trial. Thorax 2017, 72, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Cotton, M.M.; Bucknall, C.E.; Dagg, K.D.; Johnson, M.K.; MacGregor, G.; Stewart, C.; Stevenson, R.D. Early discharge for patients with exacerbations of chronic obstructive pulmonary disease: A randomised controlled trial. Thorax 2000, 55, 902–906. [Google Scholar] [CrossRef] [Green Version]
- Majothi, S.; Jolly, K.; Heneghan, N.R.; Price, M.J.; Riley, R.D.; Turner, A.M.; Bayliss, S.E.; Moore, D.J.; Singh, S.J.; Adab, P.; et al. Supported self-management for patients with COPD who have recently been discharged from hospital: A systematic review and meta-analysis. Int. J. Chron. Obstr. Pulm. Dis. 2015, 10, 853–867. [Google Scholar] [CrossRef] [Green Version]
- Johnson-Warrington, V.; Rees, K.; Gelder, C.; Morgan, M.D.; Singh, S.J. Can a supported self-management program for COPD upon hospital discharge reduce readmissions? A randomized controlled trial. Int. J. Chron. Obstr. Pulm. Dis. 2016, 11, 1161–1169. [Google Scholar] [CrossRef] [Green Version]
- Hermiz, O.; Comino, E.; Marks, G.; Daffurn, K.; Wilson, S.; Harris, M. Randomised controlled trial of home based care of patients with chronic obstructive pulmonary disease. BMJ 2002, 325, 938. [Google Scholar] [CrossRef] [Green Version]
- Abad-Corpa, E.; Royo-Morales, T.; Iniesta-Sánchez, J.; Carrillo-Alcaraz, A.; Rodríguez-Mondejar, J.J.; Saez-Soto, Á.R.; Vivo-Molina, M.C. Evaluation of the effectiveness of hospital discharge planning and follow-up in the primary care of patients with chronic obstructive pulmonary disease. J. Clin. Nurs. 2013, 22, 669–680. [Google Scholar] [CrossRef]
- Fonarow, G.C.; Konstam, M.A.; Yancy, C.W. The hospital readmission reduction program is associated with fewer readmissions, more deaths: Time to reconsider. J. Am. Coll. Cardiol. 2017, 70, 1931–1934. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, P.; Werner, R.M. The hospital readmission reduction program and social risk. Health Serv. Res. 2019, 54, 324. [Google Scholar] [CrossRef] [PubMed]
- Naylor, M.D.; Hirschman, K.B.; McCauley, K.; Shaid, E.C.; Hanlon, A.L.; Whitehouse, C.R.; Ghosh, A.; Browm, R.; Sullivan, B.; Pauly, M.V. MIRROR-TCM: Multisite replication of a randomized controlled trial-Transitional care model. Contemp. Clin. Trials 2022, 112, 106620. [Google Scholar] [CrossRef] [PubMed]
- Hunt, M.R. Implementation of a Nurse-Led Transitional Care Model for Older Adults with COPD Admitted to Home Health. Dr. Nurs. Pract. Proj. 2019, 26, 1–111. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis, 1st ed.; John Wiley & Sons: New York, NY, USA, 2021; pp. 69–75. [Google Scholar]
- Shin, W.J. An Introduction of the Systematic Review and Meta-Analysis. Hanyang Med. Rev. 2015, 35, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Kang, H. Statistical Considerations in Meta-Analysis. Hanyang Med. Rev. 2015, 35, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Aboumatar, H.; Naqibuddin, M.; Chung, S.; Chaudhry, H.; Kim, S.W.; Saunders, J.; Wise, R.A. Effect of a hospital-initiated program combining transitional care and long-term self-management support on outcomes of patients hospitalized with chronic obstructive pulmonary disease: A randomized clinical trial. JAMA 2019, 322, 1371–1380. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.H.; Zhao, Y.; Chen, L.Y.; Zhang, L.; Zhang, Y.M. The effect of a nurse-led self-management program on outcomes of patients with chronic obstructive pulmonary disease. J. Clin. Respir. Med. 2020, 14, 148–157. [Google Scholar] [CrossRef]
- Hegelund, A.; Andersen, I.C.; Andersen, M.N.; Bodtger, U. The impact of a personalised action plan delivered at discharge to patients with COPD on readmissions: A pilot study. Scand. J. Caring Sci. 2020, 34, 909–918. [Google Scholar] [CrossRef] [Green Version]
- Collinsworth, A.W.; Brown, R.M.; James, C.S.; Stanford, R.H.; Alemayehu, D.; Priest, E.L. The impact of patient education and shared decision making on hospital readmissions for COPD. Int. J. Chron. Obstr. Pulm. Dis. 2018, 13, 1325. [Google Scholar] [CrossRef] [Green Version]
- Silver, P.C.; Kollef, M.H.; Clinkscale, D.; Watts, P.; Kidder, R.; Eads, B.; Quartaro, M. A respiratory therapist disease management program for subjects hospitalized with COPD. Respir. Care 2017, 62, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granados-Santiago, M.; Valenza, M.C.; López-López, L.; Prados-Román, E.; Rodríguez-Torres, J.; Cabrera-Martos, I. Shared decision-making and patient engagement program during acute exacerbation of COPD hospitalization: A randomized control trial. Patient Educ. Couns. 2020, 103, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Bikmoradi, A.; Jalalinasab, A.; Salvati, M.; Ahmadpanah, M.; Divani, F.; Roshanaei, G. Impact of continuity of care on quality of life in patients with chronic obstructive pulmonary disease: A quasi-experimental study. J. Integr. Care 2018, 27, 26–36. [Google Scholar] [CrossRef]
- Rose, L.; Istanboulian, L.; Carriere, L.; Thomas, A.; Lee, H.B.; Rezaie, S.; Shafari, R.; Fraser, I. Program of integrated care for patients with chronic obstructive pulmonary disease and multiple comorbidities (PIC COPD+): A randomised controlled trial. Eur. Respir. J. 2018, 51, 1701567. [Google Scholar] [CrossRef] [Green Version]
- Xu, W.; Hu, H.; Mao, Y. Questionnaire Survey-Based Quantitative Assessment of the Impact of Transitional Care on Self-Management of Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Comput. Math. Methods Med. 2021, 13, 3634548. [Google Scholar] [CrossRef]
- Vegda, K.; Nie, J.X.; Wang, L.; Tracy, C.S.; Moineddin, R.; Upshur, R.E. Trends in health services utilization, medication use, and health conditions among older adults: A 2-year retrospective chart review in a primary care practice. BMC Health Serv. Res. 2009, 9, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Pinkhasov, R.M.; Wong, J.; Kashanian, J.; Lee, M.; Samadi, D.B.; Pinkhasov, M.M.; Shabsigh, R. Are men shortchanged on health? Perspective on health care utilization and health risk behavior in men and women in the United States. Int. J. Clin. Pract. 2010, 64, 475–487. [Google Scholar] [CrossRef]
- Gay, E.; Desai, S.; McNeil, D. A multidisciplinary intervention to improve care for high-risk COPD patients. Am. J. Med. Qual. 2020, 35, 231–235. [Google Scholar] [CrossRef]
- Sridhar, M.; Taylor, R.; Dawson, S.; Roberts, N.H.; Patridge, M.R. A nurse led intermediate care package in patients who have been hospitalised with an acute exacerbation of chronic obstructive pulmonary disease. Thorax 2008, 63, 194–200. [Google Scholar] [CrossRef] [Green Version]
- Ridwan, E.S.; Hadi, H.; Wu, Y.L.; Tsai, P.S. Effects of transitional care on hospital readmission and mortality rate in subjects with COPD: A systematic review and meta-analysis. Respir. Care 2019, 64, 1146–1156. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Zhang, Y.; Li, D.D.; Sun, J. Transitional care interventions to reduce readmission in patients with chronic obstructive pulmonary disease: A meta-analysis of randomized controlled trials. Chin. Nurs. Res. 2017, 4, 84–91. [Google Scholar] [CrossRef]
- Ryrsø, C.K.; Godtfredsen, N.S.; Kofod, L.M.; Lavesen, M.; Mogensen, L.; Tobberup, R.; Farver-Vestergaard, I.; Callesen, H.E.; Tendal, B.; Lange, P.; et al. Lower mortality after early supervised pulmonary rehabilitation following COPD-exacerbations: A systematic review and meta-analysis. BMC Pulm. Med. 2018, 18, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, S.L.; Robertson, N.; Graham, C.D.; Williams, J.; Steiner, M.C.; Morgan, M.D.L.; Singh, S.J. Can we identify patients with different illness schema following an acute exacerbation of COPD: A cluster analysis. Respir. Med. 2014, 108, 319–328. [Google Scholar] [CrossRef] [Green Version]
- Maddocks, M.; Kon, S.S.; Singh, S.J.; Man, W.D.C. Rehabilitation following hospitalization in patients with COPD: Can it reduce readmissions? Respirology 2015, 20, 395–404. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) Country | Study Design | Participants | Intervention Group | Control Group | Components of the Intervention | Duration of Intervention | Coordinator | Main Outcome |
|---|---|---|---|---|---|---|---|---|
| Aboumatar et al. (2019) USA [30] | RCT (blinded data collectors and outcome assessors) | 240 IG: 120 CG: 120 | Combined transitional care and long-term self-management Support | Usual transitional care | (i) Customized transition support services (ii) Self-management training and support (iii) Community programs and treatment service support (Patient-centered partnership approach) | From hospitalization to 6 months after discharge | COPD nurse | Readmission, emergency department visits, quality of life, death |
| Wang et al. (2020) China [31] | RCT (blinded interventionists) | 154 IG: 77 CG: 77 | Nurse-led self-management program | Usual care, health education for COPD | (i) Comprehensive patient assessment (ii) Five or six face-to-face education sessions before discharge (individually tailored) (iii) Discharge planning for each participant (iv) Three-month follow-up intervention | From approximately 6–7 days before discharge to 3 months after discharge | Advanced respiratory nurse | Readmission, emergency department visits, quality of life, physical capacity |
| Hegelund et al. (2020) Denmark [32] | RCT (not blinded) | 99 IG: 49 CG: 50 | Personalized action plan | Usual care and treatment | (i) Personalized action plan (check status according to the CAT value measured periodically and suggest actions to be taken) (ii) Self-management dialogue, including short instruction and the possibility for subsequent support | From hospitalization to 3 months after discharge | Respiratory-educated study nurses | Readmission, symptoms assessed, anxiety and depression |
| Collinsworth et al. (2018) USA [33] | RCT (waiver of patient consent for blinding) | 308 IG: 141 CG: 167 | Patient education and shared decision-making | - | (i) Baseline assessment (ii) Pragmatic COPD Chronic Care education program (iii) Shared decision-making-based self-management planning (iv) Telephone follow-up (1 wk, 1, 2, 6 mo) using a structured checklist | From hospitalization to 6 months after discharge | Registered respiratory therapist | Readmission, symptoms assessed, patient activation measure |
| Silver et al. (2017) USA [34] | RCT (blocked randomization) | 428 IG: 214 CG: 214 | Disease management program | - | (i) Education based on Global initiative for chronic obstructive lung diseases(GOLD) guidelines (ii) Individualized written action plan (iii) Scheduled telephone monitoring (Q&A and consultation) | From hospitalization to 6 months after discharge | Respiratory therapist | Readmission, emergency department visits, all-cause mortality |
| Granados-Santia go et al. (2020) Spain [35] | RCT | 42 IG: 21 CG: 21 | Shared decision-making and patient engagement program | Standard treatment | Personalized shared decision-making patient engagement program | From hospitalization to 3 months after discharge | - | Physical capacity, health status, knowledge of the disease, pharmacological management, general functionality, nutritional status |
| Bikmoradi et al. (2019) Iran [36] | RCT | 80 IG: 40 CG: 40 | Continuous care | Usual care | (i) Four intervention sessions (awareness, sensitization, control, and evaluation) with education package (ii) Telephone follow-up (iii) Invite to LDBE Hospital education orientation for continuous care | From hospitalization to 2 months after discharge | Researchers’ assistants, Hospital Respiratory Center | Quality of life |
| Rose et al. (2018) Canada [37] | RCT (blinded inspection research assistant) | 470 IG: 234 CG: 236 | Program of integrated care | Usual care | (i) Standardized education session (ii) Individualized care and action plans (iii) Telephone consultations, action plan, teach-back sessions (iv) Ongoing case manager communication with family physicians and hospital specialists, including respirologists (v) Priority access to ambulatory outpatient clinics and exacerbation management prescriptions | From hospitalization to 3 months after discharge | Case manager | Readmission, emergency department visits, mortality rate, quality of life, anxiety and depression, self-efficacy |
| Ko et al. (2017) Hong Kong [17] | RCT (blinded examination and investigation research assistants) | 180 IG: 90 CG: 90 | Comprehensive care program | Usual care | (i) Two educational sessions by a respiratory nurse (ii) The physiotherapist provided every patient with an individualized physical training program (iii) Respiratory physician prescribed medications (iv) Provided consultation phone number available during work hours (v) Follow-up at respiration center every three months | From hospitalization to 12 months after discharge | Respiratory nurse, physiotherapist, respiratory physician | Readmission, quality of life, mortality rate, physical capacity, lung function |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, Y.; Kim, J.; Kim, S.; Moon, D.; Jo, H. Effects of Transitional Care after Hospital Discharge in Patients with Chronic Obstructive Pulmonary Disease: An Updated Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 6053. https://doi.org/10.3390/ijerph20116053
Park Y, Kim J, Kim S, Moon D, Jo H. Effects of Transitional Care after Hospital Discharge in Patients with Chronic Obstructive Pulmonary Disease: An Updated Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(11):6053. https://doi.org/10.3390/ijerph20116053
Chicago/Turabian StylePark, Yukyung, Jiwon Kim, Sukyoung Kim, Dahae Moon, and Heuisug Jo. 2023. "Effects of Transitional Care after Hospital Discharge in Patients with Chronic Obstructive Pulmonary Disease: An Updated Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 11: 6053. https://doi.org/10.3390/ijerph20116053