
Risk Factors for Falls and Fall-Related Fractures in Community-Living Older People with Pain: A Prospective Cohort Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
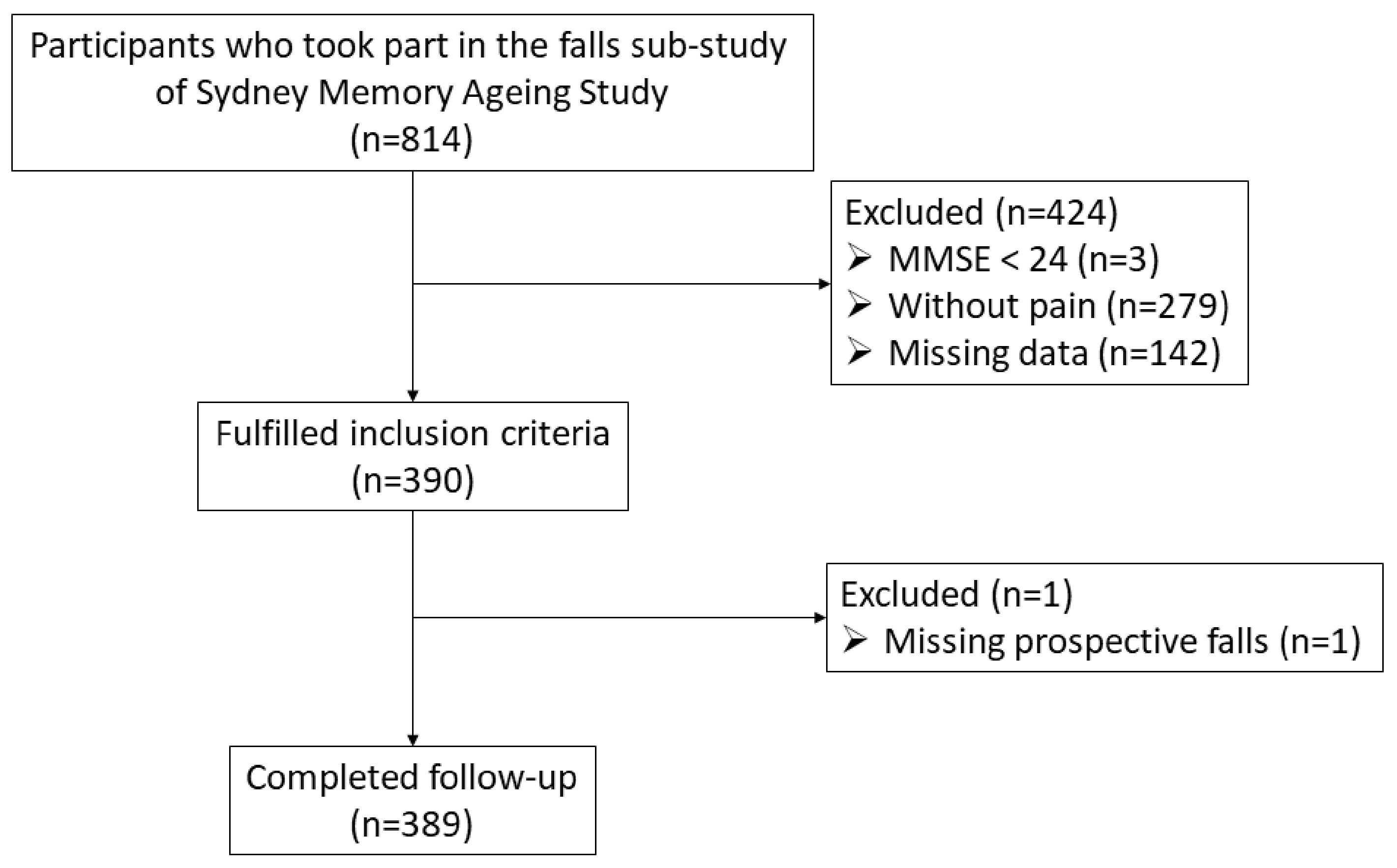
2.1. Participants and Study Design
2.2. Assessments
2.2.1. Falls
2.2.2. Demographics
2.2.3. Physical Function
2.2.4. Cognitive Function and Psychological Status
2.2.5. Physical Activity
2.3. Statistical Analysis
3. Results
3.1. Baseline Participant Characteristics
3.2. Logistic Regression Analyses to Determine Predictors of Falls and Fall-Related Fractures
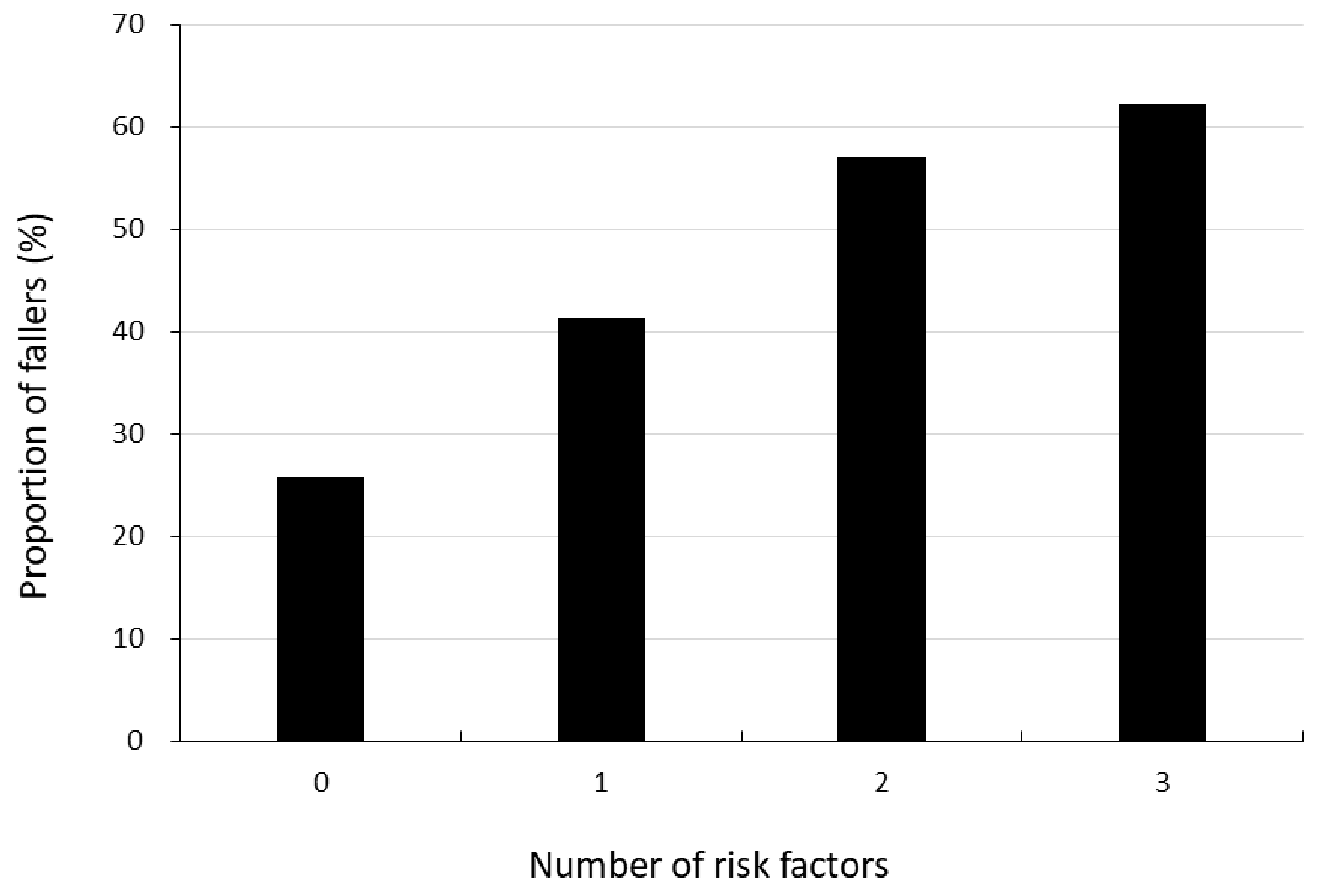
3.3. Proportion of Fallers in Relation to Number of Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nevitt, M.C.; Cummings, S.R.; Kidd, S.; Black, D. Risk factors for recurrent nonsyncopal falls. A prospective study. JAMA 1989, 261, 2663–2668. [Google Scholar] [CrossRef]
- Tinetti, M.E.; Speechley, M.; Ginter, S.F. Risk factors for falls among elderly persons living in the community. N. Engl. J. Med. 1988, 319, 1701–1707. [Google Scholar] [CrossRef]
- Sterling, D.A.; O’Connor, J.A.; Bonadies, J. Geriatric falls: Injury severity is high and disproportionate to mechanism. J. Trauma 2001, 50, 116–119. [Google Scholar] [CrossRef]
- Stevens, J.A.; Corso, P.S.; Finkelstein, E.A.; Miller, T.R. The costs of fatal and non-fatal falls among older adults. Inj. Prev. J. Int. Soc. Child Adolesc. Inj. Prev. 2006, 12, 290–295. [Google Scholar] [CrossRef] [Green Version]
- Florence, C.S.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. Medical Costs of Fatal and Nonfatal Falls in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef] [Green Version]
- Patel, K.V.; Guralnik, J.M.; Dansie, E.J.; Turk, D.C. Prevalence and impact of pain among older adults in the United States: Findings from the 2011 National Health and Aging Trends Study. Pain 2013, 154, 2649–2657. [Google Scholar] [CrossRef] [Green Version]
- Shah, R.C.; Buchman, A.S.; Boyle, P.A.; Leurgans, S.E.; Wilson, R.S.; Andersson, G.B.; Bennett, D.A. Musculoskeletal pain is associated with incident mobility disability in community-dwelling elders. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2011, 66, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Suka, M.; Yoshida, K. The national burden of musculoskeletal pain in Japan: Projections to the year 2055. Clin. J. Pain 2009, 25, 313–319. [Google Scholar] [CrossRef]
- Stubbs, B.; Binnekade, T.; Eggermont, L.; Sepehry, A.A.; Patchay, S.; Schofield, P. Pain and the risk for falls in community-dwelling older adults: Systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2014, 95, 175–187.e9. [Google Scholar] [CrossRef]
- Stubbs, B.; Schofield, P.; Binnekade, T.; Patchay, S.; Sepehry, A.; Eggermont, L. Pain is associated with recurrent falls in community-dwelling older adults: Evidence from a systematic review and meta-analysis. Pain Med. 2014, 15, 1115–1128. [Google Scholar] [CrossRef] [Green Version]
- Peeters, G.; van Schoor, N.M.; Lips, P. Fall risk: The clinical relevance of falls and how to integrate fall risk with fracture risk. Best Pract. Res. Clin. Rheumatol. 2009, 23, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; van der Velde, N.; Martin, F.C.; Petrovic, M.; Tan, M.P.; Ryg, J.; Aguilar-Navarro, S.; Alexander, N.B.; Becker, C.; Blain, H.; et al. World guidelines for falls prevention and management for older adults: A global initiative. Age Ageing 2022, 51, afac205. [Google Scholar] [CrossRef] [PubMed]
- Hicks, C.; Levinger, P.; Menant, J.C.; Lord, S.R.; Sachdev, P.S.; Brodaty, H.; Sturnieks, D.L. Reduced strength, poor balance and concern about falls mediate the relationship between knee pain and fall risk in older people. BMC Geriatr. 2020, 20, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirase, T.; Okubo, Y.; Sturnieks, D.L.; Lord, S.R. Pain Is Associated With Poor Balance in Community-Dwelling Older Adults: A Systematic Review and Meta-analysis. J. Am. Med. Dir. Assoc. 2020, 21, 597–603.e8. [Google Scholar] [CrossRef] [PubMed]
- Bair, M.J.; Robinson, R.L.; Katon, W.; Kroenke, K. Depression and pain comorbidity: A literature review. Arch. Intern. Med. 2003, 163, 2433–2445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Leeuw, G.; Eggermont, L.H.; Shi, L.; Milberg, W.P.; Gross, A.L.; Hausdorff, J.M.; Bean, J.F.; Leveille, S.G. Pain and Cognitive Function Among Older Adults Living in the Community. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 398–405. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, B.; Binnekade, T.T.; Soundy, A.; Schofield, P.; Huijnen, I.P.; Eggermont, L.H. Are older adults with chronic musculoskeletal pain less active than older adults without pain? A systematic review and meta-analysis. Pain Med. 2013, 14, 1316–1331. [Google Scholar] [CrossRef] [Green Version]
- Sachdev, P.S.; Brodaty, H.; Reppermund, S.; Kochan, N.A.; Trollor, J.N.; Draper, B.; Slavin, M.J.; Crawford, J.; Kang, K.; Broe, G.A.; et al. The Sydney Memory and Ageing Study (MAS): Methodology and baseline medical and neuropsychiatric characteristics of an elderly epidemiological non-demented cohort of Australians aged 70–90 years. Int. Psychogeriatr. 2010, 22, 1248–1264. [Google Scholar] [CrossRef]
- Tombaugh, T.N.; McIntyre, N.J. The mini-mental state examination: A comprehensive review. J. Am. Geriatr. Soc. 1992, 40, 922–935. [Google Scholar] [CrossRef]
- Lamb, S.E.; Jorstad-Stein, E.C.; Hauer, K.; Becker, C. Development of a common outcome data set for fall injury prevention trials: The Prevention of Falls Network Europe consensus. J. Am. Geriatr. Soc. 2005, 53, 1618–1622. [Google Scholar] [CrossRef]
- Lord, S.R.; Menz, H.B.; Tiedemann, A. A physiological profile approach to falls risk assessment and prevention. Phys. Ther. 2003, 83, 237–252. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.R.; Murray, S.M.; Chapman, K.; Munro, B.; Tiedemann, A. Sit-to-stand performance depends on sensation, speed, balance, and psychological status in addition to strength in older people. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2002, 57, M539–M543. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Waite, L.M.; Broe, G.A.; Grayson, D.A.; Creasey, H. Preclinical syndromes predict dementia: The Sydney older persons study. J. Neurol. Neurosurg. Psychiatry 2001, 71, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, D. Wechsler Adult Intelligence Scale-Revised; Harcourt Brace Jovanovich: New York, NY, USA, 1981. [Google Scholar]
- Wechsler, D. Wechsler Adult Intelligence Scale-III; The Psychological Corporation: San Antonio, TX, USA, 1997. [Google Scholar]
- Yesavage, J.A.; Sheikh, J.I. Geriatric Depression Scale (GDS). Clin. Gerontol. 1986, 5, 165–173. [Google Scholar] [CrossRef]
- Yardley, L.; Beyer, N.; Hauer, K.; Kempen, G.; Piot-Ziegler, C.; Todd, C. Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing 2005, 34, 614–619. [Google Scholar] [CrossRef] [Green Version]
- Delbaere, K.; Hauer, K.; Lord, S.R. Evaluation of the incidental and planned activity questionnaire (IPEQ) for older people. Br. J. Sport. Med. 2010, 44, 1029–1034. [Google Scholar] [CrossRef]
- Brumagne, S.; Cordo, P.; Lysens, R.; Verschueren, S.; Swinnen, S. The role of paraspinal muscle spindles in lumbosacral position sense in individuals with and without low back pain. Spine 2000, 25, 989–994. [Google Scholar] [CrossRef]
- Lihavainen, K.; Sipilä, S.; Rantanen, T.; Sihvonen, S.; Sulkava, R.; Hartikainen, S. Contribution of musculoskeletal pain to postural balance in community-dwelling people aged 75 years and older. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2010, 65, 990–996. [Google Scholar] [CrossRef]
- McIlroy, W.E.; Bishop, D.C.; Staines, W.R.; Nelson, A.J.; Maki, B.E.; Brooke, J.D. Modulation of afferent inflow during the control of balancing tasks using the lower limbs. Brain Res. 2003, 961, 73–80. [Google Scholar] [CrossRef]
- Kato, S.; Murakami, H.; Demura, S.; Yoshioka, K.; Shinmura, K.; Yokogawa, N.; Igarashi, T.; Yonezawa, N.; Shimizu, T.; Tsuchiya, H. Abdominal trunk muscle weakness and its association with chronic low back pain and risk of falling in older women. BMC Musculoskelet. Disord. 2019, 20, 273. [Google Scholar] [CrossRef]
- Balogun, S.; Aitken, D.; Winzenberg, T.; Wills, K.; Scott, D.; Callisaya, M.; Jones, G. Longitudinal Associations of Serum 25-hydroxyvitamin D, Physical Activity, and Knee Pain and Dysfunction with Muscle Loss in Community-dwelling Older Adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2018, 73, 526–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orr, R. Contribution of muscle weakness to postural instability in the elderly. A systematic review. Eur. J. Phys. Rehabil. Med. 2010, 46, 183–220. [Google Scholar] [PubMed]
- Horlings, C.G.; van Engelen, B.G.; Allum, J.H.; Bloem, B.R. A weak balance: The contribution of muscle weakness to postural instability and falls. Nat. Clin. Pract. Neurol. 2008, 4, 504–515. [Google Scholar] [CrossRef] [PubMed]
- Okubo, Y.; Duran, L.; Delbaere, K.; Sturnieks, D.L.; Richardson, J.K.; Pijnappels, M.; Lord, S.R. Rapid Inhibition Accuracy and Leg Strength Are Required for Community-Dwelling Older People to Recover Balance From Induced Trips and Slips: An Experimental Prospective Study. J. Geriatr. Phys. Ther. 2022, 45, 160–166. [Google Scholar] [CrossRef]
- McMullan, I.I.; Bunting, B.P.; McDonough, S.M.; Tully, M.A.; Casson, K. Changes in physical activity predict changes in a comprehensive model of balance in older community-dwelling adults. A longitudinal analysis of the TILDA study. J. Frailty Sarcopenia Falls 2019, 4, 102–110. [Google Scholar] [CrossRef]
- Lee, H.; Lee, J.A.; Brar, J.S.; Rush, E.B.; Jolley, C.J. Physical activity and depressive symptoms in older adults. Geriatr. Nurs. 2014, 35, 37–41. [Google Scholar] [CrossRef] [Green Version]
- Hirase, T.; Okubo, Y.; Menant, J.; Lord, S.R.; Sturnieks, D.L. Impact of pain on reactive balance and falls in community-dwelling older adults: A prospective cohort study. Age Ageing 2020, 49, 982–988. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.; Linton, S.J. Fear-avoidance and its consequences in chronic musculoskeletal pain: A state of the art. Pain 2000, 85, 317–332. [Google Scholar] [CrossRef] [Green Version]
- Delbaere, K.; Close, J.C.; Heim, J.; Sachdev, P.S.; Brodaty, H.; Slavin, M.J.; Kochan, N.A.; Lord, S.R. A multifactorial approach to understanding fall risk in older people. J. Am. Geriatr. Soc. 2010, 58, 1679–1685. [Google Scholar] [CrossRef]
- Abellan van Kan, G.; Rolland, Y.; Andrieu, S.; Bauer, J.; Beauchet, O.; Bonnefoy, M.; Cesari, M.; Donini, L.M.; Gillette Guyonnet, S.; Inzitari, M.; et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J. Nutr. Health Aging 2009, 13, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Gouveia, É.; Blimkie, C.J.; Maia, J.A.; Lopes, C.; Gouveia, B.R.; Freitas, D.L. Multivariate analysis of lifestyle, constitutive and body composition factors influencing bone health in community-dwelling older adults from Madeira, Portugal. Arch. Gerontol. Geriatr. 2014, 59, 83–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Jameson, K.; Sayer, A.A.; Robinson, S.; Cooper, C.; Dennison, E. Accumulation of risk factors associated with poor bone health in older adults. Arch. Osteoporos. 2016, 11, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakazaki, T.; Koike, T.; Yanagimoto, Y.; Oshida, Y. Association between gait speed and bone strength in community-dwelling postmenopausal Japanese women. Environ. Health Prev. Med. 2012, 17, 394–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, W.; Watanabe, M.; Tanimoto, Y.; Shibutani, T.; Saito, M.; Usuda, K.; Kono, K. Ultrasound parameters of bone health and related physical measurement indicators for the community-dwelling elderly in Japan. Geriatr. Gerontol. Int. 2007, 7, 154–159. [Google Scholar] [CrossRef]
- Kwon, J.; Suzuki, T.; Yoshida, H.; Kim, H.; Yoshida, Y.; Iwasa, H.; Sugiura, M.; Furuna, T. Association between change in bone mineral density and decline in usual walking speed in elderly community-dwelling Japanese women during 2 years of follow-up. J. Am. Geriatr. Soc. 2007, 55, 240–244. [Google Scholar] [CrossRef]
- Lord, S.R.; Ward, J.A.; Williams, P.; Anstey, K.J. An epidemiological study of falls in older community-dwelling women: The Randwick falls and fractures study. Aust. J. Public Health 1993, 17, 240–245. [Google Scholar] [CrossRef]
- Lord, S.R.; Ward, J.A.; Williams, P.; Strudwick, M. The effect of a 12-month exercise trial on balance, strength, and falls in older women: A randomized controlled trial. J. Am. Geriatr. Soc. 1995, 43, 1198–1206. [Google Scholar] [CrossRef]
- Day, L.; Fildes, B.; Gordon, I.; Fitzharris, M.; Flamer, H.; Lord, S. Randomised factorial trial of falls prevention among older people living in their own homes. BMJ (Clin. Res. Ed.) 2002, 325, 128. [Google Scholar] [CrossRef] [Green Version]
- Sundermann, E.E.; Katz, M.J.; Lipton, R.B. Sex Differences in the Relationship between Depressive Symptoms and Risk of Amnestic Mild Cognitive Impairment. Am. J. Geriatr. Psychiatry Off. J. Am. Assoc. Geriatr. Psychiatry 2017, 25, 13–22. [Google Scholar] [CrossRef] [Green Version]
- Buchner, D.M.; Rillamas-Sun, E.; Di, C.; LaMonte, M.J.; Marshall, S.W.; Hunt, J.; Zhang, Y.; Rosenberg, D.E.; Lee, I.M.; Evenson, K.R.; et al. Accelerometer-Measured Moderate to Vigorous Physical Activity and Incidence Rates of Falls in Older Women. J. Am. Geriatr. Soc. 2017, 65, 2480–2487. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, D.E.; Rillamas-Sun, E.; Bellettiere, J.; LaMonte, M.; Buchner, D.M.; Di, C.; Hunt, J.; Marshall, S.; Stefanick, M.; Zhang, Y.; et al. Accelerometer-Measured Sedentary Patterns are Associated with Incident Falls in Older Women. J. Am. Geriatr. Soc. 2021, 69, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Jadczak, A.D.; Makwana, N.; Luscombe-Marsh, N.; Visvanathan, R.; Schultz, T.J. Effectiveness of exercise interventions on physical function in community-dwelling frail older people: An umbrella review of systematic reviews. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 752–775. [Google Scholar] [CrossRef]
- Seo, J.Y.; Chao, Y.Y. Effects of Exercise Interventions on Depressive Symptoms Among Community-Dwelling Older Adults in the United States: A Systematic Review. J. Gerontol. Nurs. 2018, 44, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Michaleff, Z.A.; Fairhall, N.; Paul, S.S.; Tiedemann, A.; Whitney, J.; Cumming, R.G.; Herbert, R.D.; Close, J.C.T.; Lord, S.R. Exercise to prevent falls in older adults: An updated systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1750–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherrington, C.; Whitney, J.C.; Lord, S.R.; Herbert, R.D.; Cumming, R.G.; Close, J.C. Effective exercise for the prevention of falls: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 2008, 56, 2234–2243. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, M.; Yamazaki, S.; Kimura, M.; Nakano, K.; Yasumura, S. Community-based exercise program reduces chronic knee pain in elderly Japanese women at high risk of requiring long-term care: A non-randomized controlled trial. Geriatr. Gerontol. Int. 2013, 13, 167–174. [Google Scholar] [CrossRef]
- Hirase, T.; Kataoka, H.; Nakano, J.; Inokuchi, S.; Sakamoto, J.; Okita, M. Effects of a psychosocial intervention programme combined with exercise in community-dwelling older adults with chronic pain: A randomized controlled trial. Eur. J. Pain 2018, 22, 592–600. [Google Scholar] [CrossRef]
- Okubo, Y.; Schoene, D.; Lord, S.R. Step training improves reaction time, gait and balance and reduces falls in older people: A systematic review and meta-analysis. Br. J. Sport. Med. 2017, 51, 586–593. [Google Scholar] [CrossRef]
- Fiori, K.L.; Antonucci, T.C.; Cortina, K.S. Social network typologies and mental health among older adults. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2006, 61, P25–P32. [Google Scholar] [CrossRef] [Green Version]
- Lo, C.W.T.; Tsang, W.W.N.; Yan, C.H.; Lord, S.R.; Hill, K.D.; Wong, A.Y.L. Risk factors for falls in patients with total hip arthroplasty and total knee arthroplasty: A systematic review and meta-analysis. Osteoarthr. Cartil. 2019, 27, 979–993. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.W.T.; Brodie, M.A.; Tsang, W.W.N.; Lord, S.R.; Yan, C.H.; Wong, A.Y.L. Pain, balance, and mobility in people 1 year after total knee arthroplasty: A non-randomized cross-sectional pilot study contrasting posterior-stabilized and medial-pivot designs. Pilot Feasibility Stud. 2022, 8, 131. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 12-Month Follow-Up | ||||||
|---|---|---|---|---|---|---|
| Falls | Fall-Related Fractures | |||||
| Yes (n = 175) | No (n = 214) | p-Value | Yes (n = 20) | No (n = 369) | p-Value | |
| Age (years) | 79 (4.8) | 78.8 (4.8) | 0.638 | 81 (6.4) | 78.8 (4.7) | 0.132 |
| Female, n (%) | 98 (56.0) | 114 (53.3) | 0.591 | 14 (70.0) | 198 (53.7) | 0.153 |
| Height (cm) | 163.7 (9.3) | 164.0 (9.5) | 0.772 | 159.8 (8.7) | 164.1 (9.4) | 0.043 |
| Weight (kg) | 75.6 (15.8) | 73.3 (14.2) | 0.129 | 69.0 (11.5) | 74.7 (15.1) | 0.100 |
| BMI (kg/m2) | 28.2 (5.3) | 27.1 (4.1) | 0.040 | 27.0 (3.4) | 27.6 (4.7) | 0.540 |
| Comorbidity (yes) | 11 (6.3) | 11 (5.1) | 0.658 | 2 (10.0) | 20 (5.4) | 0.401 |
| Stroke | 1 (0.6) | 9 (4.2) | 0.024 | 1 (5.0) | 9 (2.4) | 0.483 |
| Parkinson’s disease | 1 (0.6) | 1 (0.6) | 0.886 | 0 (0) | 2 (0.5) | 0.741 |
| Diatebes mellitus (type 1 or type 2) | 26 (14.9) | 23 (10.8) | 0.223 | 4 (20.0) | 45 (12.3) | 0.311 |
| Chronic obstructive pulmonary disease | 3 (1.7) | 2 (0.9) | 0.504 | 0 (0) | 5 (1.4) | 0.599 |
| Heart disease | 41 (23.4) | 47 (22.1) | 0.750 | 4 (20.0) | 84 (22.8) | 0.769 |
| Use of 4 or more medications (yes) | 110 (62.9) | 149 (69.6) | 0.183 | 13 (65.0) | 246 (66.7) | 0.874 |
| Physical function | ||||||
| Proprioception (deg) | 2.3 (1.4) | 2.4 (1.5) | 0.842 | 2.5 (1.2) | 2.3 (1.5) | 0.419 |
| Lower limb muscle strength (kg) | 27.5 (11.2) | 28.4 (12.9) | 0.464 | 25.7 (11.6) | 28.1 (12.2) | 0.267 |
| Hand reaction time (ms) | 235 (37.5) | 237 (47.8) | 0.932 | 245 (31.7) | 236 (43.9) | 0.126 |
| Postural sway on a foam rubber pad (mm/30 s) | 214 (117.0) | 184 (107.0) | 0.011 | 258 (143.8) | 194 (109.9) | 0.017 |
| STS (s) | 15.8 (4.5) | 16.0 (5.8) | 0.735 | 17.4 (5.8) | 15.9 (5.2) | 0.237 |
| TUG (s) | 9.9 (3.6) | 10.1 (3.9) | 0.586 | 11.2 (4.0) | 9.9 (3.8) | 0.174 |
| 6 m walking time (s) | 9.4 (3.5) | 9.4 (3.3) | 0.516 | 12.3 (5.5) | 9.3 (3.2) | 0.012 |
| Cognitive function | ||||||
| TMT B-A (s) | 72.5 (47.4) | 71.5 (45.7) | 0.842 | 83.8 (60.1) | 71.4 (45.7) | 0.284 |
| DSST (score) | 49.0 (11.3) | 47.9 (12.4) | 0.381 | 44.6 (13.6) | 48.6 (11.9) | 0.153 |
| Psychological status | ||||||
| GDS-15 (score) | 2.6 (2.2) | 2.2 (1.9) | 0.034 | 2.8 (2.5) | 2.3 (2.0) | 0.333 |
| FES-I (score) | 24.6 (7.3) | 23.1 (7.1) | 0.019 | 26.9 (7.8) | 23.6 (7.2) | 0.077 |
| Physical activity | ||||||
| IPEQ-total (hours/week) | 29.9 (15.1) | 32.7 (16.3) | 0.018 | 28.6 (16.3) | 30.7 (15.9) | 0.634 |
| Dependent Variables Any Falls | ||||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | |||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Postural sway on a foam rubber pad | 1.29 | 1.06–1.57 | 0.012 | 1.38 | 1.10–1.73 | 0.005 |
| GDS-15 | 1.23 | 1.01–1.50 | 0.037 | 1.26 | 1.02–1.55 | 0.034 |
| FES-I | 1.21 | 1.00–1.46 | 0.041 | 1.18 | 0.96–1.45 | 0.109 |
| IPEQ-total | 0.72 | 0.58–0.90 | 0.004 | 0.72 | 0.57–0.91 | 0.006 |
| Dependent Variable: At Least One Fall with Fracture | ||||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | |||||
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Postural sway on a foam rubber pad | 1.41 | 1.05–1.90 | 0.024 | 1.40 | 0.99–1.97 | 0.059 |
| 6 m walking time | 1.67 | 1.24–2.23 | 0.001 | 1.58 | 1.14–2.19 | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hirase, T.; Okubo, Y.; Delbaere, K.; Menant, J.C.; Lord, S.R.; Sturnieks, D.L. Risk Factors for Falls and Fall-Related Fractures in Community-Living Older People with Pain: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2023, 20, 6040. https://doi.org/10.3390/ijerph20116040
Hirase T, Okubo Y, Delbaere K, Menant JC, Lord SR, Sturnieks DL. Risk Factors for Falls and Fall-Related Fractures in Community-Living Older People with Pain: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2023; 20(11):6040. https://doi.org/10.3390/ijerph20116040
Chicago/Turabian StyleHirase, Tatsuya, Yoshiro Okubo, Kim Delbaere, Jasmine C. Menant, Stephen R. Lord, and Daina L. Sturnieks. 2023. "Risk Factors for Falls and Fall-Related Fractures in Community-Living Older People with Pain: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 20, no. 11: 6040. https://doi.org/10.3390/ijerph20116040