1. Introduction
The COVID-19 pandemic and subsequent nationwide lockdown have had a detrimental effect on people’s mental well-being. This has led to a drastic surge in mental health problems, affecting both previously healthy individuals and those with pre-existing mental health conditions [
1,
2,
3]. The impact of this surge has been quite substantial, with roughly 10 million people in England necessitating new or additional mental health assistance, accounting for approximately 20% of the population [
4]. People with pre-existing mental health conditions were especially vulnerable during this period, experiencing exacerbated symptoms, difficulties accessing necessary services and support, and an increased risk of relapse and suicidal behavior [
1]. As a consequence, there has been a higher demand for crucial mental health services and treatment, exceeding the capacity of these services.
The pandemic has also brought about significant disruptions to the usual practices of mental health services not only in the United Kingdom (UK) but also globally [
5,
6]. The UK government initiated national restrictions on 23 March 2020 to control the infection rate, forestall the National Health Service (NHS) from becoming overwhelmed, and lessen the number of COVID-19-associated fatalities. Nonetheless, recent studies have indicated that the adaptations necessary to provide mental healthcare services during this prolonged period of infection-control measures may have had an inequitable impact on individuals with pre-existing mental health conditions (e.g., autism [
7], obsessive compulsive disorder [
8], and substance use disorder [
9]).
Furthermore, the challenges of attending in-person review appointments and the closure of support services are likely to have had an impact on all individuals who were receiving or in need of active mental health treatment [
10]. For instance, initiating new medications with patients who are being seen virtually can be challenging, which may also impede their use. These challenges may have further worsened and deepened the existing structural health inequalities that were already being targeted by quality improvement initiatives before COVID-19 [
11]. Patients in higher health disparate areas may have experienced limited access to telehealth services during the pandemic, resulting in a reduced availability of psychiatric medications for them. Patients’ changing attitudes have also contributed to these challenges, as the fear of contracting the virus coupled with national lockdowns has led to a decrease in people seeking medical attention, especially in higher health disparate areas where individuals already faced significant challenges in accessing mental health services due to issues such as poverty, limited resources, and stigma.
Psychiatric medications, such as anxiolytics and hypnotics, are frequently prescribed to alleviate symptoms of anxiety, depression, and insomnia. Recent studies have reported a rise in prescriptions for psychiatric medication, which appears to coincide with an increase in psychological symptoms during the pandemic when compared to the preceding year [
12,
13,
14]. However, it is not well understood how the pandemic and the restrictions introduced to contain the infection spread have affected the use of psychiatric medication, particularly concerning those from higher health disparate areas. Given the widespread use of these medications and their potential impact on mental health outcomes, it is crucial to gather information to develop effective approaches to addressing the mental health needs of these communities. Therefore, in this study, we aim to examine the association between trends in psychiatric medication use among general practitioner (GP) practices located in regions with higher health disparity and the COVID-19 pandemic lockdown. This inquiry is important because learning from healthcare service changes is vital to understand whether and to what extent the pandemic and subsequent lockdown influenced medication use for individuals with the most significant needs, informing proactive planning for future pandemics.
2. Materials and Methods
We performed a retrospective cohort study at the practice level and conducted a multivariate analysis of psychiatric medication use from April 2019 to March 2021 using publicly available datasets.
2.1. Setting
This study was carried out in the North East of England, which has the lowest healthy life expectancy, with an average of 59 years for men and 61 years for women, compared to a national average of 64 years for men and 65 years for women [
15,
16]. Furthermore, previous research indicates that the North East region exhibits higher health disparities compared to the rest of England. Specifically, the region has elevated mortality rates from cancer, circulatory diseases, and respiratory diseases, as well as higher rates of hospital admissions for alcohol-related conditions and self-harm [
17,
18]. The findings from this study could aid in comprehending the impact of COVID-19 on higher health disparate areas in England and help direct the development of the region’s healthcare strategies.
2.2. Time Periods of the COVID-19 Lockdown in England
The time periods [
19] studied were
Pre-lockdown (23 March 2019–22 March 2020);
First national lockdown (23 March–3 July 2020);
Minimal lockdown restrictions (4 July–13 September 2020);
Reimposing restrictions (14 September–4 November 2020);
Second and third lockdowns (Lockdowns 2 and 3 were combined because of a short interval between them) (5 November–7 March 2021).
For our regression analysis, we defined the post-lockdown period as the last four periods.
2.3. Medication Use Data
The OpenPrescribing database (OpenPrescibing.net, Bennett Institute for Applied Data Science, University of Oxford, 2022) was used to collect prescription information in the North East of England between April 2019 and March 2021. The database is derived from claims data for prescriptions that community pharmacies submit for reimbursement from the NHS in England. It contains anonymized data on medicines prescribed as prescription items, quantity and cost incurred. The data encompasses prescriptions written by GPs and other non-medical prescribers who are attached to practices, but it does not include private prescriptions.
The primary focus of this study was on the usage of anxiolytics and hypnotics, with the volume of their standardized average daily quantities (ADQs) per 1000 patients serving as the primary outcome measure. The use of standardized ADQs facilitates comparisons between different medications or populations by accounting for the size of the population being analyzed [
20]. This approach can help detect patterns and trends in medication use and inform decision-making regarding resource allocation, formulary management, and public health planning.
The ADQ is calculated by dividing the total number of dispensed doses of a specific medication by the number of patients who take that medication and then multiplying it by the number of days for which the medication was dispensed. The resulting value is then standardized by dividing it by 1000 to account for differences in the size of the population being studied. Monthly practice-level ADQ of anxiolytics and hypnotics data were downloaded for the study period.
2.4. GP Practice Characteristics
We obtained GP practice characteristics indicators for all practices in the North East of England from the Fingertips data (2020/21) to identify population characteristics attributed to each GP practice that may contribute to differences in psychiatric medication use. Fingertips data is a public health data analysis and visualization tool developed by Public Health England [
21]. It provides access to a wide range of health and well-being indicators at national, regional, and local levels in England.
To assess the influence of socioeconomic factors on psychiatric medication use, we used the index of multiple deprivations (IMD) 2019 provided for geographic areas (lower-level super output areas or LSOAs). LSOAs are geographic areas used in the United Kingdom for statistical purposes, and they are smaller than local authorities but larger than individual postcodes. The IMD measures deprivation across dimensions such as income, employment, education, health, crime, access to housing and services, and living environment. The higher value of the IMD score is indicative of a greater degree of area-based deprivation in comparison to other areas, which is related to spatial inequalities in health. We also used proportions of registered patients aged 75 or over in each practice as a proxy measure for the intensity of GP practice workload, with older people accounting for a relatively large proportion of GP consultations and prescriptions [
22].
To evaluate the patient experience of and access to their GP services, we employed measures such as the proportion of patients reporting positive experiences, satisfaction with phone access and practice appointment times, and overall experience of making an appointment. We also examined the demand for GP services through long-term health conditions prevalence rates, as people with long-term physical health conditions commonly experience mental health problems and have high healthcare needs (50% of all GP appointments) [
23]. Lifestyle indicators, such as the percentage of patients with caring responsibility, those in paid work or full-time education, and those who are unemployed, were also taken into account.
Finally, mental health indicators were assessed, including the quality and outcomes framework (QOF) prevalence of mental health and the percentage of patients with a new diagnosis of depression. By considering these various factors, we provided a picture of the characteristics of these GP practices and their patients that may impact the use of psychiatric medications in the North East of England.
2.5. Statistical Methods
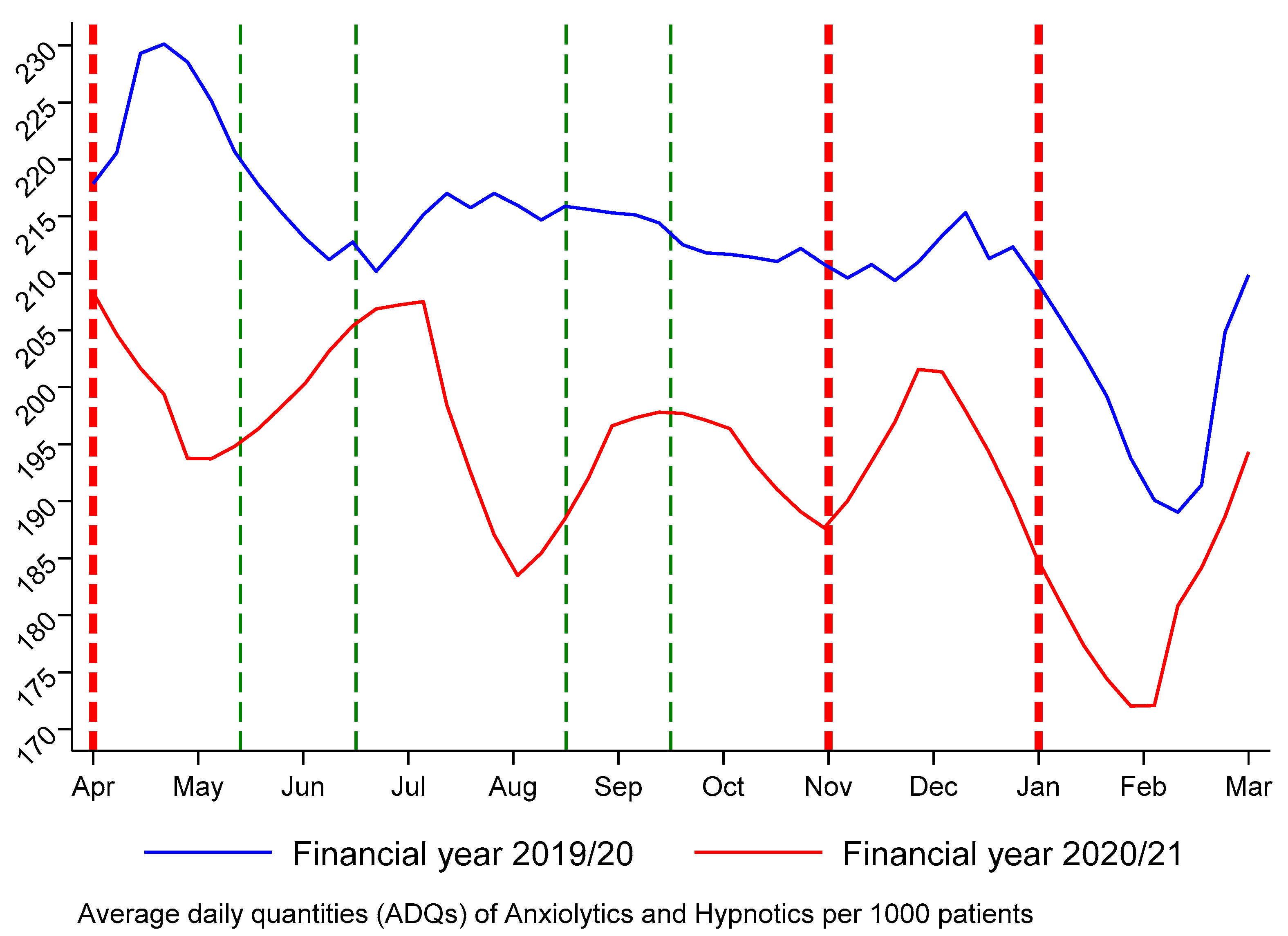
A descriptive analysis was performed to examine potential regional disparities in these prescribing GP practices. The region-level data was compared with the national average in England to provide a broader context and enhance the comprehension of medication usage in the North East region. This comparison can be useful for policymakers and healthcare providers who seek valuable information for decision-making purposes. Temporal trends in the monthly ADQs of anxiolytics and hypnotics use in practice before and after the onset of the COVID lockdown are illustrated in
Figure 1.
The IMD score for 2019 was divided into quartiles prior to conducting the multivariable regression model analysis in order to enable easy interpretation of the results. A random-effects model was used to examine the relationship between the COVID-19 lockdown and the use of anxiolytics and hypnotics. We included calendar months as covariates to account for seasonal variations in the data. Specifically, we added 11 binary variables to represent each month, with one month (April) serving as the reference category. The significance of each month suggests that there may be certain months that have a significant impact on anxiolytics and hypnotics use, even after accounting for the effect of the lockdown. To account for pre-existing differences across practices, the model included a range of baseline practice characteristic covariates, as listed previously. In order to minimize bias resulting from unobserved time-invariant factors that were correlated with the use of anxiolytics and hypnotics, we estimated models with random practice effects. The random effects specification was assumed to be valid as it is more efficient than the fixed effects specification and makes use of both within- and between-practice variation in the data, given that the time-varying explanators are uncorrelated with unobserved time-invariant practice factors.
Data statistics were presented as mean, standard deviation (SD), median, and range. p < 0.05 was considered to be statistically significant. All analyses were conducted using Stata 17 (StataCorp LLC, College Station, TX, USA). We reported robust standard errors clustered at the practice level.
3. Results
3.1. Health Disparities
The study collected monthly data on anxiolytics and hypnotics use from 322 GP practices in the North East of England over two financial years from 2019/20 to 2020/21, resulting in 7728 practice-month observations.
The study compared the characteristics of these practices to England’s average (as displayed in
Table 1). It was found that GPs in the North East of England had a heavier workload than England’s average, with a higher proportion of elderly patients (8.7% vs. 7.9%). Furthermore, within the North East of England, GP practices located in higher health disparate areas exhibited a lower workload on average than those in less health disparate areas, with a significantly lower proportion of patients aged over 75 (7.6% vs. 9.8%).
Patients in the North East of England reported higher levels of satisfaction with healthcare services provided by their local GP practices compared to the average in England. Specifically, patients reported higher satisfaction rates in terms of the quality of care received (86.8% vs. 83.0%), the experience of phone access (75.6% vs. 67.6%), appointment times (67.3% vs. 62.7%), and making appointments (75.6% vs. 70.6%). However, patients living in higher health disparate areas were found to be less satisfied with their GP practices (85.4% vs. 88.2%), phone access (73.4% vs. 77.8%), appointment times (66.6% vs. 68.0%), and making appointments (73.9% vs. 77.3%), compared to those living in less health disparate areas. In the North East of England, the prevalence of long-term conditions among registered patients in GP practices exceeded the English average, with a percentage of more than 5% (56.3% vs. 51.1%). Patients living in higher health disparate areas were found to have a higher prevalence of long-term conditions compared to those living in less health disparate areas (57.4% vs. 55.2%).
There was a negligible contrast in the percentage of individuals in higher health disparate areas versus less health disparate areas who reported responsibilities for care (19.9% vs. 20.0%). However, it was observed that a larger proportion of patients in the North East of England had the responsibility of caring for someone compared to the English average (20.0% vs. 18.2%).
A lower percentage of individuals in the North East of England were engaged in paid work or full-time education compared to England’s average (57.0%% vs. 61.8%). Conversely, a slightly higher percentage of people in the region were unemployed compared to England’s average (6.2% vs. 5.5%). Additionally, the data show that in higher health disparate areas, there were lower proportions of people registered with practices who were engaged in paid work or full-time education compared to less health disparate areas (with a difference of 2.6%). Conversely, there were higher proportions of unemployed individuals in higher health disparate areas compared to less health disparate areas (with a difference of 4.9%).
The data reveal that there was no significant difference in the reported prevalence of mental illness in the QOF between the North East of England and England average. However, the proportion of individuals who received a new diagnosis of depression in the North East of England was slightly higher than England’s average, with a figure of 1.5% compared to 1.4% in the whole of England. Moreover, the QOF reported prevalence of mental illness in higher health disparate areas was 1.1% compared to 0.9% in less health disparate areas. The proportion of individuals who received a new diagnosis of depression was higher in higher health disparate areas at 1.6% compared to 1.4% in less health disparate areas.
3.2. Trends in Psychiatric Medication Use
Our observation revealed a monthly variation during the 2019/20 financial year, with the highest medication usage in the months of March and April and consistently lowest numbers in January and February. The first UK lockdown that commenced on 23 March 2020, which required people to stay at home, resulted in a sharp drop in ADQs of medication use. Although the volumes were gradually recovering as restrictions eased, the ADQs remained below pre-lockdown levels until the end of the study period. The second lockdown, which commenced on 5 November 2020, was associated with a further reduction in the monthly ADOs of prescriptions and a bigger gap in the same month between the 2019/20 and 2020/21 financial years compared to the first lockdown. However, no wider gap was found from the second lockdown to the third lockdown, which began in January 2021. The partial removal of restrictions associated with each lockdown, as indicated by the green dashed lines, resulted in an immediate increase in medication use. We noted a peak increase when all non-essential retailers were allowed to reopen in England from 15 June 2020 and a second peak increase when the second lockdown ended on 2 December 2020.
3.3. The Impact of COVID Lockdown
Table 2 presents the adjusted regression coefficients that exhibit the relationship between anxiolytics and hypnotics use and the pandemic lockdown, the interaction between socioeconomic status and the lockdown, seasonal variation, and GP practice characteristics. The lockdown was found to have a significant negative association with the volume of anxiolytics and hypnotics used. From April 2020 to March 2021, there was an average of 14 fewer ADQs (
p < 0.001) compared to the 2019/20 financial year average for the same period. Furthermore, on average, 50 more ADQs of anxiolytics and hypnotics (
p = 0.011) were used in GP practices serving higher health disparate populations compared to those serving less health disparate populations.
We also observed a noteworthy and adverse interaction effect between higher health disparities and pandemic lockdown on anxiolytics and hypnotics use (β = −9.09, p = 0.007), suggesting that patients living in higher health disparate areas had even more limited access to these medications during the lockdown than those in less health disparate areas. This may be due to a variety of factors, such as reduced access to healthcare services, financial constraints, or greater levels of stress and anxiety related to the pandemic. The adverse effect highlights the unequal effect of the pandemic lockdown, which may worsen the already-existing health inequalities in mental health service utilization among higher health disparate areas.
Monthly variation was seen in daily medication use, with the highest medication usage in April and consistently lowest numbers in February, representing a reduction of 31 items per 1000 per day compared to April. In addition, we found that practices with a higher workload, as indicated by a greater proportion of patients aged over 75 years, had a higher prescription volume, with an average of over 14 prescriptions more per 1000 per day. Medication use volume also appeared to be based on the morbidity needs of the practice population, with higher medication use volumes in practices reporting a higher prevalence of long-term health conditions.
4. Discussion
4.1. Health Disparities
This study conducted in the North East of England revealed important findings regarding healthcare services and socioeconomic inequalities in health. Firstly, the workload of GP practices in the region was higher than the average workload in England, which is in line with previous studies [
24,
25]. However, within the region, GP practices in higher health disparate areas had a lower workload as compared to those in less health disparate areas. This observation could be attributed to the fact that patients living in less health disparate areas are more willing to access healthcare. Extensive research supports the strong relationship between socioeconomic status, healthcare utilization, and healthy aging [
26,
27,
28,
29,
30,
31]. These disparities may impact equitable access to high-quality healthcare services. Secondly, patients in the region reported higher levels of satisfaction with their healthcare services than the England average. This may be because people in the North East of England have low expectations of the healthcare system, or they are grateful for any care that they are able to receive, despite the challenges they face in accessing care [
32,
33]. Within the region, there were differences among patients living in higher health disparate areas versus less health disparate areas. The findings suggest that further efforts may be necessary to raise people’s expectations of healthcare quality to ensure equitable access to high-quality healthcare services for patients living in higher health disparate areas. Thirdly, there may be a greater need for healthcare services that focus on managing long-term conditions in the North East of England, particularly in higher health disparate areas. As such, it may be beneficial to implement targeted interventions aimed at improving the health outcomes of patients living with long-term conditions in these areas. Fourthly, disparities in paid work and full-time education were observed between higher and less health disparate areas. This disparity can have negative consequences on overall health and well-being, as employment and education are important determinants of health. This highlights the need for targeted interventions and policies to address these disparities and promote equal access to employment and education opportunities, particularly in higher health disparate areas. The study also highlighted higher rates of mental health issues in higher health disparate areas, indicating the need for improving access to mental health services and resources in these areas. It is also important to increase awareness and understanding of mental health issues in these areas and to provide support and education to individuals who may be at risk. Additionally, efforts should be made to address the root causes of mental health disparities, such as poverty and social inequality.
4.2. Psychiatric Medication Use
This study found a substantial drop in psychiatric medication use following the lockdown, particularly in higher health disparate areas. This is consistent with previous studies that have shown that disadvantaged individuals are more likely to experience barriers to accessing mental health care and are less likely to receive appropriate treatment for their mental health conditions [
34,
35]. The pandemic and subsequent lockdown may have exacerbated these existing disparities by limiting access to mental health services and increasing stressors such as job loss, financial instability, and social isolation, which can negatively impact mental health [
6,
36].
The study also highlighted that during the pandemic, patients may not be able to access psychiatric medications, which can impact the continuity of care for them in managing their mental health. Proper dose titration is crucial for individuals taking psychiatric medication, as abruptly stopping or restarting a high-dose prescription can lead to dangerous side effects and withdrawal symptoms [
37]. The disruption of medication access during the pandemic may have contributed to medication nonadherence and treatment discontinuation, which can increase the risk of relapse and worsen mental health outcomes.
In sum, the study’s findings align with previous research in the UK and internationally into the uneven regional impact of the pandemic and its implications for socioeconomic inequalities in health. They provide preliminary support to the concerns that the pandemic and subsequent lockdown have increased inequality in healthcare [
11,
38], particularly in higher health disparate areas [
39,
40]. These findings have important implications for future crises, and there is a need to assess the strengths and weaknesses of healthcare services to better plan and support mental health in disadvantaged communities. Targeting resources, such as introducing new models of mental healthcare and increasing the provision of mental health services, may help to alleviate some of the health consequences of the pandemic in vulnerable areas.
5. Strengths and Limitations
This study provides valuable insights into the impact of the COVID-19 pandemic and subsequent lockdown on psychiatric medication use, particularly in higher health disparate areas. The use of a random-effect model enabled us to account for medication use patterns that are associated with the local GP practice of residence. The study also utilized high-quality medication use data sourced from pharmacy claims, which ensured a high level of completeness and eliminated the possibility of recall bias. The large sample size and large effect size obtained in this study resulted in a high level of statistical significance in many of the observed associations.
However, it is important to acknowledge the limitations of the study. One of the major limitations is the lack of patient socioeconomic and demographic data included in the dataset. The numbers of medication use are given as aggregate data per GP practice for each month, and thus, potential biases relating to patient socioeconomics and demographics could not be controlled for. Additionally, there is a lack of data on the diagnosis of depression, meaning that some of the medication use may not be for mental illness. Finally, the unexplained variance in the model could be related to other individual and practice changes that occurred during the study period.
To address these limitations and to further explore the impact of the pandemic on mental health, future analyses could integrate multiple individuals and practice time-varying variables. These variables could help to control for potential biases relating to patient demographics and provide a more nuanced understanding of the impact of the pandemic on mental health in higher health disparate areas. Despite these limitations, the findings of this study are significant and provide preliminary support for concerns that inequality in healthcare increased during the pandemic lockdown, particularly in higher health disparate areas. As such, the study highlights the need for targeted interventions and increased provision of mental health services in vulnerable areas to help alleviate some of the health consequences of the pandemic.
6. Conclusions
Our study has provided important insights into the impact of the COVID-19 pandemic and subsequent lockdown on mental health service utilizations in higher health disparate areas. Our findings demonstrate a decrease in psychiatric medication use during the period of national lockdown, particularly among those living in higher health disparate areas. These results suggest that the pandemic has exacerbated existing socioeconomic inequalities in healthcare service use, highlighting the need for targeted support in these areas. Our study underscores the importance of addressing the regional disparities in the long-term impacts of COVID-19-related changes on mental health service providers, who need to ensure that patients in higher health disparate areas receive adequate support during and after the pandemic. However, we recognized that future research should delve deeper into the underlying reasons for this decline in psychiatric medication use and identify potential strategies to address this issue. In conclusion, our study emphasized the urgent need for targeted interventions to support mental health services in higher health disparate areas during times of crisis.
Author Contributions
Conceptualization, Y.F.; methodology, G.Y.; validation, E.Y.H.T.; formal analysis G.Y.; resources, Y.F.; writing—original draft preparation, G.Y. and Y.F.; writing—review and editing, E.Y.H.T. All authors have read and agreed to the published version of the manuscript.
Funding
This publication presents independent research funded by the National Institute of Health and Care Research (NIHR) School for Primary Care Research as part of the Three NIHR Research Schools Mental Health Programme (award number MH027) and also supported by the NIHR [Applied Research Collaboration North East and North Cumbria (NIHR200173)]. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Informed Consent Statement
As this study used publicly available data aggregated at the general practitioner practice level, ethical approval and consent were not required.
Data Availability Statement
All data are fully available without restriction.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef] [PubMed]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef] [PubMed]
- Banks, J.; Xu, X. The mental health effects of the first two months of lockdown during the COVID-19 pandemic in the UK. Fisc. Stud. 2020, 41, 685–708. [Google Scholar] [CrossRef]
- O’Shea, N. COVID-19 and the Nation’s Mental Health: Forecasting Needs and Risks in the UK; Centre for Mental Health: London, UK, 2020. [Google Scholar]
- Amerio, A.; Aguglia, A.; Odone, A.; Gianfredi, V.; Serafini, G.; Signorelli, C.; Amore, M. COVID-19 pandemic impact on mental health of vulnerable populations. Acta Bio Med. Atenei Parm. 2020, 91, 95–96. [Google Scholar]
- Cullen, W.; Gulati, G.; Kelly, B.D. Mental health in the COVID-19 pandemic. QJM Int. J. Med. 2020, 113, 311–312. [Google Scholar] [CrossRef]
- Halstead, E.J.; Sullivan, E.C.; Dimitriou, D. The Impact of COVID-19 on Sleep in Autistic Adults: Longitudinal Comparisons pre and During Lockdown. Front. Psychiatry 2021, 1608, 708339. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G.; Frank, J.W.; Naylor, C.D.; Wodchis, W.; Feng, P. Using socioeconomics to counter health disparities arising from the COVID-19 pandemic. BMJ 2020, 369, m2149. [Google Scholar] [CrossRef]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 pandemic and health inequalities. J. Epidemiol. Community Health 2020, 74, 964–968. [Google Scholar] [CrossRef]
- Hirschtritt, M.E.; Slama, N.; Sterling, S.A.; Olfson, M.; Iturralde, E. Psychotropic medication prescribing during the COVID-19 pandemic. Medicine 2021, 100, e27664. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.J.; Roberts, G. Psychotropic medication prescribing trends in a developmental–behavioural clinic during the COVID-19 pandemic. J. Paediatr. Child Health 2022, 58, 1359–1365. [Google Scholar] [CrossRef] [PubMed]
- Waheed, U.; Stedman, M.; Davies, M.; Walther, A.; Solomon, E.O.; Ollier, B.; Heald, A.H. National level prescribing of psychotropic medication in primary care during the COVID-19 pandemic in England: Potential implications for cardiometabolic health. Cardiovasc. Endocrinol. Metab. 2022, 11, e0270. [Google Scholar] [CrossRef] [PubMed]
- Ly, M. Health Profile for England; Public Health England: London, UK, 2020; Volume 3. Available online: https://ukhsa.blog.gov.uk/2019/03/11/why-are-musculoskeletal-conditions-the-biggest-contributor-to-morbidity/ (accessed on 1 May 2023).
- Marmot, M. Health equity in England: The Marmot review 10 years on. BMJ 2020, 368, m693. [Google Scholar] [CrossRef]
- Bambra, C.L.; Munford, L.; Brown, H.; Wilding, A.; Robinson, T.; Holland, P.; Barr, B.; Hill, H.; Regan, M.; Rice, N. Health for Wealth: Building a Healthier Northern Powerhouse for UK Productivity; Northern Health Sciences Alliance: Newcastle, UK, 2018. [Google Scholar]
- Whitehead, M.; Bambra, C.; Barr, B.; Bowles, J.; Caulfield, R.; Doran, T.; Harrison, D.; Lynch, A.; Pleasant, S.; Weldon, J. Due North: Report of the Inquiry on Health Equity for the North; University of Liverpool and Centre for Local Economic Strategies: Liverpool, UK, 2014. [Google Scholar]
- Brown, J.; Kirk-Wade, E. Coronavirus: A History of English Lockdown Laws; House of Commons Library Briefing Paper: Westminster, UK, 2021. [Google Scholar]
- Walley, T.; Roberts, D. Average daily quantities: A tool for measuring prescribing volume in England. Pharmacoepidemiol. Drug Saf. 2000, 9, 55–58. [Google Scholar] [CrossRef]
- Office for Health Improvement and Disparities. Available online: https://fingertips.phe.org.uk (accessed on 1 May 2023).
- Lloyd, D.; Scrivener, G. Prescribing at the primary care group level: Census data and prescribing indicators. J. Clin. Pharm. Ther. 2001, 26, 93–101. [Google Scholar] [CrossRef]
- NHS England. Enhancing the Quality of Life for People Living with Long Term Conditions; NHS England: London, UK, 2014.
- Dayan, M. Are Parts of England ‘Left Behind’ by the NHS; Nuffield Trust Comment: London, UK, 2018. [Google Scholar]
- Iacobucci, G. GPs in deprived areas face severest pressures, analysis shows. BMJ 2019, 365, l2104. [Google Scholar] [CrossRef]
- Hu, P.; Wagle, N.; Goldman, N.; Weinstein, M.; Seeman, T.E. The associations between socioeconomic status, allostatic load and measures of health in older Taiwanese persons: Taiwan social environment and biomarkers of aging study. J. Biosoc. Sci. 2007, 39, 545–556. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Zhang, X.; Jin, C.; Wang, D. Inequality of access to health care among the urban elderly in northwestern China. Health Policy 2009, 93, 111–117. [Google Scholar] [CrossRef]
- Menec, V.H.; Shooshtari, S.; Nowicki, S.; Fournier, S. Does the relationship between neighborhood socioeconomic status and health outcomes persist into very old age? A population-based study. J. Aging Health 2010, 22, 27–47. [Google Scholar] [CrossRef]
- Shea, S.; Lima, J.; Diez-Roux, A.; Jorgensen, N.W.; McClelland, R.L. Socioeconomic status and poor health outcome at 10 years of follow-up in the multi-ethnic study of atherosclerosis. PLoS ONE 2016, 11, e0165651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stringhini, S.; Carmeli, C.; Jokela, M.; Avendaño, M.; McCrory, C.; d’Errico, A.; Bochud, M.; Barros, H.; Costa, G.; Chadeau-Hyam, M. Socioeconomic status, non-communicable disease risk factors, and walking speed in older adults: Multi-cohort population based study. BMJ 2018, 360, k1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.; Deng, S.; Xiong, X.; Tang, S. Equity in access to healthcare among the urban elderly in China: Does health insurance matter? Int. J. Health Plan. Manag. 2014, 29, e127–e144. [Google Scholar] [CrossRef] [PubMed]
- Duffy, B. Satisfaction and Expectations: Attitudes to Public Services in Deprived Areas; LSE STICERD Research Paper No. CASE045: London, UK, 2000. [Google Scholar]
- Roder-DeWan, S.; Gage, A.D.; Hirschhorn, L.R.; Twum-Danso, N.A.; Liljestrand, J.; Asante-Shongwe, K.; Rodríguez, V.; Yahya, T.; Kruk, M.E. Expectations of healthcare quality: A cross-sectional study of internet users in 12 low-and middle-income countries. PLoS Med. 2019, 16, e1002879. [Google Scholar] [CrossRef] [Green Version]
- Alegría, M.; Chatterji, P.; Wells, K.; Cao, Z.; Chen, C.-N.; Takeuchi, D.; Jackson, J.; Meng, X.-L. Disparity in depression treatment among racial and ethnic minority populations in the United States. Psychiatr. Serv. 2008, 59, 1264–1272. [Google Scholar] [CrossRef] [Green Version]
- Noorwali, R.; Almotairy, S.; Akhder, R.; Mahmoud, G.; Sharif, L.; Alasmee, N.; Mahsoon, A.; Hafez, D. Barriers and Facilitators to Mental Health Help-Seeking among Young Adults in Saudi Arabia: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 2848. [Google Scholar] [CrossRef]
- Fitzpatrick, K.M.; Harris, C.; Drawve, G. How bad is it? Suicidality in the middle of the COVID-19 pandemic. Suicide Life-Threat. Behav. 2020, 50, 1241–1249. [Google Scholar] [CrossRef]
- Untu, I.; Chiriţă, V. The Maudsley Prescribing Guidelines in Psychiatry. Bull. Integr. Psychiatry 2018, 3, 119–121. [Google Scholar]
- Mishra, V.; Seyedzenouzi, G.; Almohtadi, A.; Chowdhury, T.; Khashkhusha, A.; Axiaq, A.; Wong, W.Y.E.; Harky, A. Health inequalities during COVID-19 and their effects on morbidity and mortality. J. Healthc. Leadersh. 2021, 13, 19–26. [Google Scholar] [CrossRef]
- Burström, B.; Tao, W. Social Determinants of Health and Inequalities in COVID-19; Oxford University Press: Oxford, UK, 2020; Volume 30, pp. 617–618. [Google Scholar]
- McNeely, C.L.; Schintler, L.A.; Stabile, B. Social determinants and COVID-19 disparities: Differential pandemic effects and dynamics. World Med. Health Policy 2020, 12, 206–217. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).




{kind=link}