


Exposure to Disinfectants and Cleaning Products and Respiratory Health of Workers and Children in Daycares: The CRESPI Cohort Protocol
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
Ethical Approval and Consent to Participate
2.2. Recruitment of Daycares
2.3. Exposure Assessment
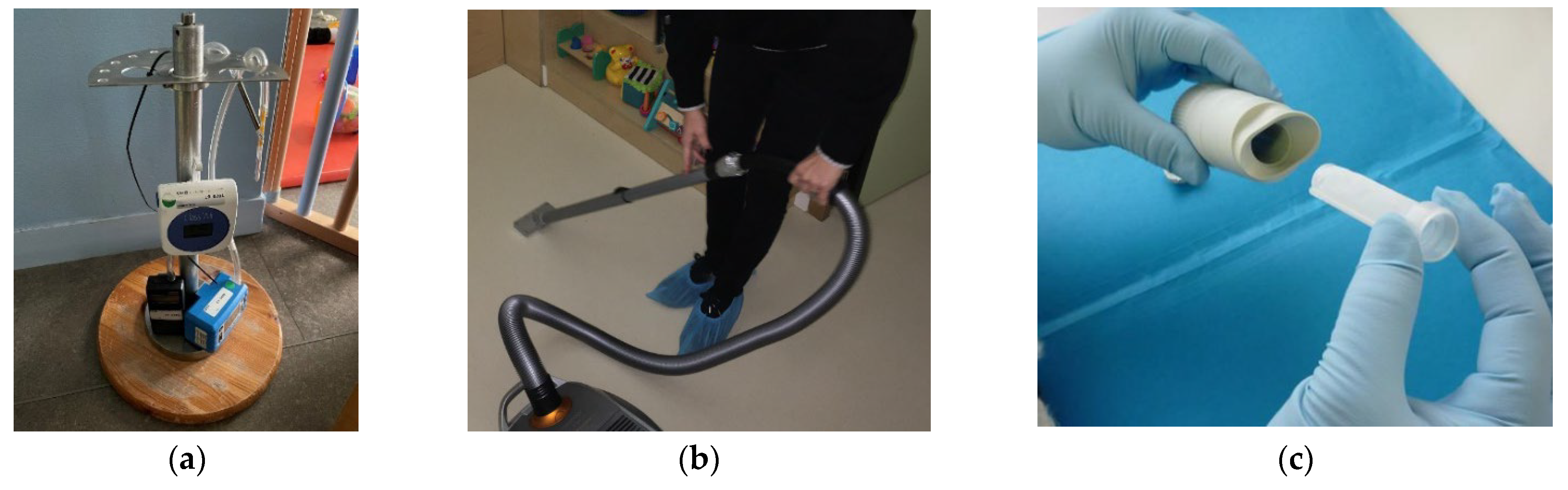
2.3.1. Environmental Measurements
2.3.2. Emissions of VOCs and SVOCs
2.3.3. Smartphone Applications
2.3.4. Database of Cleaning Products
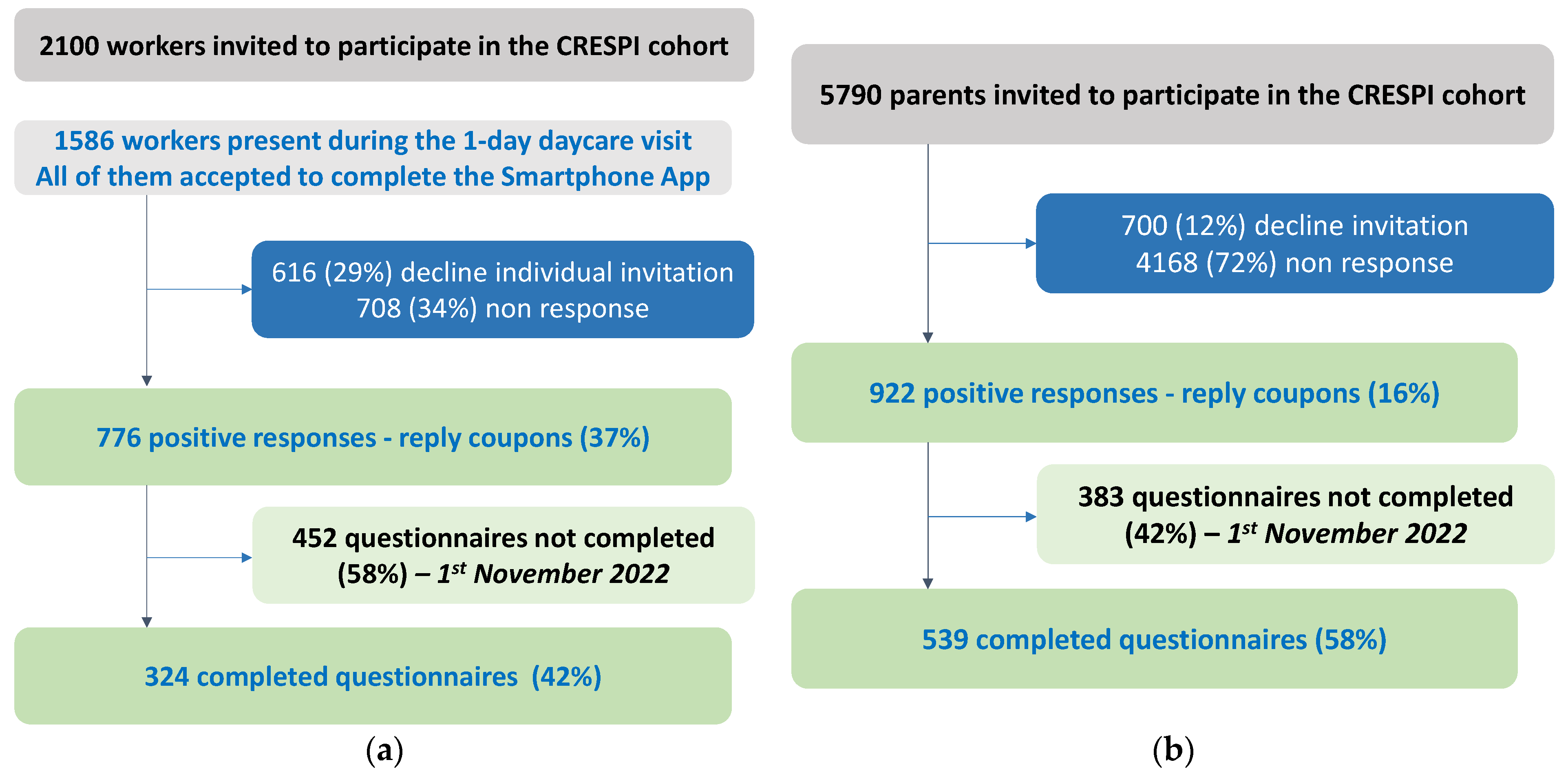
2.4. Recruitment and Inclusion of Participants—Sample Size
2.5. Respiratory Health Assessment
2.5.1. Adults—Daycare Workers
2.5.2. Children
2.6. Data Collection—Preliminary Results
2.6.1. Characteristics of Cleaning Tasks in the Daycares
2.6.2. Characteristics of Daycare Workers
2.6.3. Characteristics of Children
2.7. Biological Assessment
2.7.1. Nasal Swabs for Characterization of Nasal Microbiota
2.7.2. Buccal Cells for Characterization of the DNA Methylation
2.8. Statistical Analyses
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CRESPI | environmental exposures in dayCares and RESPIratory health of children and workers |
| CSTB | Scientific and Technical Center for Building |
| DCP | Disinfectants and Cleaning Products |
| DOHaD | Developmental Origins of Health and Disease |
| ECRHS | European Community Respiratory Health Survey |
| EGEA | Epidemiological study of Genetic and Environmental factors of Asthma, hyperactivity bronchial and atopy |
| OR | Odds Ratio |
| SVOC | Semi-Volatile Organic Compounds |
| VOC | Volatile Organic Compounds |
References
- Gur, M.; Hakim, F.; Bentur, L. Better understanding of childhood asthma, towards primary prevention—Are we there yet? Consideration of pertinent literature. F1000Research 2017, 6, 2152. [Google Scholar] [CrossRef] [PubMed]
- Diseases, G.B.D.; Injuries, C. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. Available online: https://www.thelancet.com/pb-assets/Lancet/gbd/summaries/diseases/asthma.pdf (accessed on 16 May 2023).
- Porsbjerg, C.; Melen, E.; Lehtimaki, L.; Shaw, D. Asthma. Lancet 2023, 401, 858–873. [Google Scholar] [CrossRef] [PubMed]
- Delmas, M.C.; Guignon, N.; Leynaert, B.; Moisy, M.; Marguet, C.; Fuhrman, C. Increase in asthma prevalence among young children in France. Rev. Mal. Respir. 2017, 34, 525–534. [Google Scholar] [CrossRef]
- Delmas, M.C.; Benezet, L.; Ribet, C.; Iwatsubo, Y.; Provost, D.; Varraso, R.; Zins, M.; Leynaert, B.; Nadif, R.; Roche, N. Prevalence of asthma among adults in France, data from the Constances cohort study. Rev. Mal. Respir. 2021, 38, 797–806. [Google Scholar] [CrossRef]
- Asher, I.; Pearce, N. Global burden of asthma among children. Int. J. Tuberc. Lung Dis. 2014, 18, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, J.; Anto, J.M.; Berkouk, K.; Gergen, P.; Pinto Antunes, J.; Augé, P.; Camuzat, P.; Bringer, J.; Mercier, J.; Best, N.; et al. Developmental determinants in non-communicable chronic diseases and ageing. Thorax 2015, 70, 595–597. [Google Scholar] [CrossRef]
- Beasley, R.; Semprini, A.; Mitchell, E.A. Risk factors for asthma: Is prevention possible? Lancet 2015, 386, 1075–1085. [Google Scholar] [CrossRef] [PubMed]
- Barnish, M.S.; Tagiyeva, N.; Devereux, G.; Aucott, L.; Turner, S. Changes in the relationship between asthma and associated risk factors over fifty years. Pediatr. Allergy Immunol. 2017, 28, 162–169. [Google Scholar] [CrossRef]
- Herr, M.; Just, J.; Nikasinovic, L.; Foucault, C.; Le Marec, A.M.; Giordanella, J.P.; Momas, I. Risk factors and characteristics of respiratory and allergic phenotypes in early childhood. J. Allergy Clin. Immunol. 2012, 130, 389–396.e384. [Google Scholar] [CrossRef]
- Vernet, C.; Pin, I.; Giorgis-Allemand, L.; Philippat, C.; Benmerad, M.; Quentin, J.; Calafat, A.M.; Ye, X.; Annesi-Maesano, I.; Siroux, V.; et al. and the EDEN mother-child cohort study group. In Utero Exposure to Select Phenols and Phthalates and Respiratory Health in Five Year-old Boys: A Prospective Study. Environ. Health Perspect. 2017, 125, 097006. [Google Scholar] [CrossRef] [PubMed]
- Casas, L.; Dumas, O.; Le Moual, N. Indoor Air and Respiratory Health: Volatile Organic Compounds and Cleaning Products. Asthma in the 21st Century: New Research Advances, 1st ed.; Nadif, R., Ed.; Academic Press: Cambridge, MA, USA, 2022; pp. 135–146. [Google Scholar]
- Dumas, O.; Le Moual, N. Damaging effects of household cleaning products on the lungs. Expert Rev. Respir. Med. 2020, 14, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Franklin, P. Household chemicals: Good housekeeping or occupational hazard? Eur. Respir. J. 2008, 31, 489–491. [Google Scholar] [CrossRef]
- Quiros-Alcala, L.; Wilson, S.; Witherspoon, N.; Murray, R.; Perodin, J.; Trousdale, K.; Raspanti, G.; Sapkota, A. Volatile organic compounds and particulate matter in child care facilities in the District of Columbia: Results from a pilot study. Environ. Res. 2016, 146, 116–124. [Google Scholar] [CrossRef]
- Folletti, I.; Siracusa, A.; Paolocci, G. Update on asthma and cleaning agents. Curr. Opin. Allergy Clin. Immunol. 2017, 17, 90–95. [Google Scholar] [CrossRef]
- Rook, G.A.W.; Bloomfield, S.F. Microbial exposures that establish immunoregulation are compatible with targeted hygiene. J. Allergy Clin. Immunol. 2021, 148, 33–39. [Google Scholar] [CrossRef]
- Dumas, O. Cleaners and airway diseases. Curr. Opin. Allergy Clin. Immunol. 2021, 21, 101–109. [Google Scholar] [CrossRef] [PubMed]
- Zock, J.P.; Plana, E.; Jarvis, D.; Antó, J.M.; Kromhout, H.; Kennedy, S.M.; Künzli, N.; Villani, S.; Olivieri, M.; Torén, K.; et al. The use of household cleaning sprays and adult asthma: An international longitudinal study. Am. J. Respir. Crit. Care Med. 2007, 176, 735–741. [Google Scholar] [CrossRef]
- Dumas, O.; Bedard, A.; Marbac, M.; Sedki, M.; Temam, S.; Chanoine, S.; Severi, G.; Boutron-Ruault, M.-C.; Garcia-Aymerich, J.; Siroux, V.; et al. Household cleaning and poor asthma control among elderly women. J. Allergy Clin. Immunol. 2021, 9, 2358–2365.e4. [Google Scholar] [CrossRef]
- Lemire, P.; Dumas, O.; Chanoine, S.; Temam, S.; Severi, G.; Boutron-Ruault, M.-C.; Zock, J.-P.; Siroux, V.; Varraso, R.; Le Moual, N. Domestic exposure to irritant cleaning agents and asthma in women. Environ Int. 2020, 144, 106017. [Google Scholar] [CrossRef]
- Le Moual, N.; Rava, M.; Siroux, V.; Matran, R.; Nadif, R. Use of household cleaning products, exhaled nitric oxide and lung function in women. Eur. Respir. J. 2014, 44, 816–818. [Google Scholar] [CrossRef]
- Matulonga, B.; Rava, M.; Siroux, V.; Bernard, A.; Dumas, O.; Pin, I.; Zock, J.-P.; Nadif, R.; Leynaert, B.; Le Moual, N. Women using bleach for home cleaning are at increased risk of non-allergic asthma. Respir. Med. 2016, 117, 264–271. [Google Scholar] [CrossRef]
- Le Moual, N.; Carsin, A.E.; Siroux, V.; Radon, K.; Norback, D.; Toren, K.; Olivieri, M.; Urrutia, I.; Cazzoletti, L.; Jacquemin, B.; et al. Occupational exposures and uncontrolled adult-onset asthma in the ECRHS II. Eur. Respir. J. 2014, 43, 374–386. [Google Scholar] [CrossRef] [PubMed]
- Dumas, O.; Wiley, A.S.; Quinot, C.; Varraso, R.; Zock, J.P.; Henneberger, P.K.; Speizer, F.E.; Le Moual, N.; Camargo, C.A., Jr. Occupational exposure to disinfectants and asthma control in US nurses. Eur. Respir. J. 2017, 50, 1700237. [Google Scholar] [CrossRef] [PubMed]
- Dumas, O.; Varraso, R.; Boggs, K.M.; Descatha, A.; Henneberger, P.K.; Quinot, C.; Speizer, F.E.; Zock, J.P.; Le Moual, N.; Camargo, C.A., Jr. Association of hand and arm disinfection with asthma control in US nurses. Occup. Environ. Med. 2018, 75, 378–381. [Google Scholar] [CrossRef]
- Archangelidi, O.; Sathiyajit, S.; Consonni, D.; Jarvis, D.; De Matteis, S. Cleaning products and respiratory health outcomes in occupational cleaners: A systematic review and meta-analysis. Occup. Environ. Med. 2021, 78, 604–617. [Google Scholar] [CrossRef]
- Svanes, O.; Bertelsen, R.J.; Lygre, S.H.; Carsin, A.E.; Anto, J.M.; Forsberg, B.; Garcıa-Garcıa, J.M.; Gullon, J.A.; Heinrich, J.; Holm, M.; et al. Cleaning at Home and at Work in Relation to Lung Function Decline and Airway Obstruction. Am. J. Respir. Crit. Care Med. 2018, 197, 1157–1163. [Google Scholar] [CrossRef]
- Herr, M.; Just, J.; Nikasinovic, L.; Foucault, C.; Le Marec, A.M.; Giordanella, J.P.; Momas, I. Influence of host and environmental factors on wheezing severity in infants: Findings from the PARIS birth cohort. Clin. Exp. Allergy. 2012, 42, 275–283. [Google Scholar] [CrossRef]
- Casas, L.; Espinosa, A.; Borras-Santos, A.; Jacobs, J.; Krop, E.; Heederik, D.; Nemery, B.; Pekkanen, J.; Hyvärinen, A.; Täubel, M.; et al. Domestic use of bleach and infections in children: A multicentre cross-sectional study. Occup. Environ. Med. 2015, 72, 602–604. [Google Scholar] [CrossRef] [PubMed]
- Casas, L.; Zock, J.P.; Carsin, A.E.; Fernandez-Somoano, A.; Esplugues, A.; Santa-Marina, L.; Tardón, A.; Ballester, F.; Basterrechea, M.; Sunyer, J. The use of household cleaning products during pregnancy and lower respiratory tract infections and wheezing during early life. Int. J. Public Health 2013, 58, 757–764. [Google Scholar] [CrossRef]
- Casas, L.; Zock, J.P.; Torrent, M.; García-Esteban, R.; Gracia-Lavedan, E.; Hyvärinen, A.; Sunyer, J. Use of household cleaning products, exhaled nitric oxide and lung function in children. Eur. Respir. J. 2013, 42, 1415–1418. [Google Scholar] [CrossRef] [PubMed]
- Kojima, R.; Shinohara, R.; Kushima, M.; Horiuchi, S.; Otawa, S.; Yokomichi, H.; Akiyama, Y.; Ooka, T.; Miyake, K.; Yamagata, Z.; et al. Prenatal occupational disinfectant exposure and childhood allergies: The Japan Environment and Children’s study. Occup. Environ. Med. 2022, 79, 521–526. [Google Scholar] [CrossRef]
- Le Moual, N.; Dumas, O. Asthme et produits ménagers. La Lett. Du Pneumol. 2016, XIX, 280–286. [Google Scholar]
- Zhou, C.; Baiz, N.; Zhang, T.; Banerjee, S.; Annesi-Maesano, I.; Group EM-CCS. Modifiable exposures to air pollutants related to asthma phenotypes in the first year of life in children of the EDEN mother-child cohort study. BMC Public Health 2013, 13, 506. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Boumier, J.; Wyart, G.; Ramalho, O.; Mandin, C. Cleaning practices and cleaning products in nurseries and schools: To what extent can they impact indoor air quality? Indoor Air 2016, 26, 517–525. [Google Scholar] [CrossRef]
- Strachan, D.P. Hay fever, hygiene, and household size. BMJ 1989, 299, 1259–1260. [Google Scholar] [CrossRef] [PubMed]
- de Hoog, M.L.; Venekamp, R.P.; van der Ent, C.K.; Schilder, A.; Sanders, E.A.; Damoiseaux, R.A.; Bogaert, D.; Uiterwaal, C.S.; Smit, H.A.; Bruijning-Verhagen, P. Impact of early daycare on healthcare resource use related to upper respiratory tract infections during childhood: Prospective WHISTLER cohort study. BMC Med. 2014, 12, 107. [Google Scholar] [CrossRef] [PubMed]
- Dumas, O.; Le Moual, N. Do chronic workplace irritant exposures cause asthma? Curr. Opin. Allergy Clin. Immunol. 2016, 16, 75–85. [Google Scholar] [CrossRef]
- Roda, C.; Guihenneuc-Jouyaux, C.; Momas, I. Environmental triggers of nocturnal dry cough in infancy: New insights about chronic domestic exposure to formaldehyde in the PARIS birth cohort. Environ. Res. 2013, 123, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Tagiyeva, N.; Sheikh, A. Domestic exposure to volatile organic compounds in relation to asthma and allergy in children and adults. Expert Rev. Clin. Immunol. 2014, 10, 1611–1639. [Google Scholar] [CrossRef]
- Rumchev, K.; Spickett, J.; Bulsara, M.; Phillips, M.; Stick, S. Association of domestic exposure to volatile organic compounds with asthma in young children. Thorax 2004, 59, 746–751. [Google Scholar] [CrossRef]
- Delclos, G.L.; Gimeno, D.; Arif, A.A.; Benavides, F.G.; Zock, J.P. Occupational exposures and asthma in health-care workers: Comparison of self-reports with a workplace-specific job exposure matrix. Am. J. Epidemiol. 2009, 169, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.H.; Wu, X.M.; Teague, C.H.; Lee, K.; Cassady, D.L.; Ritz, B.; Hertz-Picciotto, I. Passive sampling methods to determine household and personal care product use. J. Expo. Sci. Environ. Epidemiol. 2012, 22, 148–160. [Google Scholar] [CrossRef]
- Temam, S.; Lyon-Caen, S.; Félicité, J.; Quinot, C.; Slama, R.; Siroux, V.; Dumas, O.; Le Moual, N. Development of a barcode-based Smartphone application to assess household exposure to cleaning products. e-Health Res. Int. Congr. 2016; e-poster:1,12. [Google Scholar]
- Quinot, C.; Amsellem-Dubourget, S.; Temam, S.; Sevin, E.; Barreto, C.; Tackin, A.; Félicité, J.; Lyon-Caen, S.; Siroux, V.; Girard, R.; et al. Development of a bar code-based exposure assessment method to evaluate occupational exposure to disinfectants and cleaning products: A pilot study. Occup. Environ. Med. 2018, 75, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Lemire, P.; Temam, S.; Lyon-Caen, S.; Quinot, C.; Sévin, E.; Remacle, S.; Supernant, K.; Slama, R.; Dumas, O.; Siroux, V.; et al. Comparison of a Barcode-Based Smartphone Application to a Questionnaire to Assess the Use of Cleaning Products at Home and Their Association with Asthma Symptoms. Int. J. Environ. Res. Public. Health 2021, 18, 3366. [Google Scholar] [CrossRef]
- Lemire, P.; Chevallier, E.; Lyon-Caen, S.; Sévin, E.; Boudier, A.; Pacheco Da Silva, E.; De Thuin, C.; Slama, R.; Dumas, O.; Siroux, V.; et al. Association between household cleaning product profiles evaluated by the Ménag’Score® index and asthma symptoms among women from the SEPAGES Cohort. Int. Arch. Occup. Environ. Health 2022, 95, 1719–1729. [Google Scholar] [CrossRef]
- Radhakrishnan, D.K.; Dell, S.D.; Guttmann, A.; Shariff, S.Z.; Liu, K.; To, T. Trends in the age of diagnosis of childhood asthma. J. Allergy Clin. Immunol. 2014, 134, 1057–1062.e1055. [Google Scholar] [CrossRef]
- Pinart, M.; Albang, R.; Maier, D.; Duran-Tauleria, E.; Mena, G.; Gimeno-Santos, E.; Solà, I.; Garcia-Aymerich, J.; Guerra, S.; Stein, R.T.; et al. Systematic Review on the Definition of Allergic Diseases in Children: The MeDALL Study. Int. Arch. Allergy Immunol. 2015, 168, 110–121. [Google Scholar] [CrossRef]
- Pinart, M.; Benet, M.; Annesi-Maesano, I.; von Berg, A.; Berdel, D.; Carlsen, K.C.L.; Carlsen, K.H.; Bindslev-Jensen, C.; Eller, E.; Fantini, M.P.; et al. Comorbidity of eczema, rhinitis, and asthma in IgE-sensitised and non-IgE-sensitised children in MeDALL: A population-based cohort study. Lancet Respir. Med. 2014, 2, 131–140. [Google Scholar] [CrossRef]
- Reddy, M.B.; Covar, R.A. Asthma phenotypes in childhood. Curr. Opin. Allergy Clin. Immunol. 2016, 16, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Martinez, F.D.; Wright, A.L.; Taussig, L.M.; Holberg, C.J.; Halonen, M.; Morgan, W.J. Asthma and wheezing in the first six years of life. The Group Health Medical Associates. N. Engl. J. Med. 1995, 332, 133–138. [Google Scholar] [CrossRef]
- Savenije, O.E.; Granell, R.; Caudri, D.; Koppelman, G.H.; Smit, H.A.; Wijga, A.; de Jongste, J.C.; Brunekreef, B.; Sterne, J.A.; Postma, D.S.; et al. Comparison of childhood wheezing phenotypes in 2 birth cohorts: ALSPAC and PIAMA. J. Allergy Clin. Immunol. 2011, 127, 1505–1512.e1514. [Google Scholar] [CrossRef]
- Herr, M.; Nikasinovic, L.; Clarisse, B.; Momas, I.; Just, J. Epidemiology of allergic respiratory disorders in infants. Rev. Mal. Respir. 2007, 24, 1314–1328. [Google Scholar] [CrossRef]
- Bousquet, J.; Caimmi, D.P.; Bedbrook, A.; Bewick, M.; Hellings, P.W.; Devillier, P.; Arnavielhe, S.; Bachert, C.; Bergmann, K.C.; Canonica, G.W.; et al. Pilot study of mobile phone technology in allergic rhinitis in European countries. The MASK-rhinitis study. Allergy 2017, 72, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Teo, S.M.; Mok, D.; Pham, K.; Kusel, M.; Serralha, M.; Troy, N.; Holt, B.J.; Hales, B.J.; Walker, M.L.; Hollams, E.; et al. The infant nasopharyngeal microbiome impacts severity of lower respiratory infection and risk of asthma development. Cell Host Microb. 2015, 17, 704–715. [Google Scholar] [CrossRef]
- Depner, M.; Ege, M.J.; Cox, M.J.; Dwyer, S.; Walker, A.W.; Birzele, L.T.; Genuneit, J.; Horak, E.; Braun-Fahrlander, C.; Danielewicz, H.; et al. Bacterial microbiota of the upper respiratory tract and childhood asthma. J. Allergy Clin. Immunol. 2017, 139, 826–834.e813. [Google Scholar] [CrossRef]
- Hasegawa, K.; Mansbach, J.M.; Ajami, N.J.; Espinola, J.A.; Henke, D.M.; Petrosino, J.F.; Piedra, P.A.; Shaw, C.A.; Sullivan, A.F.; Camargo, C.A., Jr.; et al. Association of nasopharyngeal microbiota profiles with bronchiolitis severity in infants hospitalised for bronchiolitis. Eur. Respir. J. 2016, 48, 1329–1339. [Google Scholar] [CrossRef]
- Biesbroek, G.; Tsivtsivadze, E.; Sanders, E.A.; Montijn, R.; Veenhoven, R.H.; Keijser, B.J.F.; Bogaert, D. Early respiratory microbiota composition determines bacterial succession patterns and respiratory health in children. Am. J. Respir. Crit. Care Med. 2014, 190, 1283–1292. [Google Scholar] [CrossRef]
- Hasegawa, K.; Linnemann, R.W.; Mansbach, J.M.; Ajami, N.J.; Espinola, J.A.; Fiechtner, L.G.; Petrosino, J.F.; Camargo, C.A., Jr. Household siblings and nasal and fecal microbiota in infants. Pediatr. Int. 2017, 59, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Bosch, A.A.T.M.; de Steenhuijsen Piters, W.A.A.; van Houten, M.A.; Chu, M.L.J.L.; Biesbroek, G.; Kool, J.; Pernet, P.; de Groot, P.-K.C.M.; Eijkemans, M.J.C.; Keijser, B.J.F.; et al. Maturation of the Infant Respiratory Microbiota, Environmental Drivers, and Health Consequences. A Prospective Cohort Study. Am. J. Respir. Crit. Care Med. 2017, 196, 1582–1590. [Google Scholar] [CrossRef] [PubMed]
- Michel, S.; Busato, F.; Genuneit, J.; Pekkanen, J.; Dalphin, J.-C.; Riedler, J.; Mazaleyrat, N.; Weber, J.; Karvonen, A.M.; Hirvonen, M.-R.; et al. Farm exposure and time trends in early childhood may influence DNA methylation in genes related to asthma and allergy. Allergy 2013, 68, 355–364. [Google Scholar] [CrossRef]
- Joubert, B.R.; Felix, J.F.; Yousefi, P.; Bakulski, K.M.; Just, A.C.; Breton, C.; Reese, S.E.; Markunas, C.A.; Richmond, R.C.; Xu, C.J.; et al. DNA Methylation in Newborns and Maternal Smoking in Pregnancy: Genome-wide Consortium Meta-analysis. Am. J. Hum. Genet. 2016, 98, 680–696. [Google Scholar] [CrossRef] [PubMed]
- Hew, K.M.; Walker, A.I.; Kohli, A.; Garcia, M.; Syed, A.; McDonald-Hyman, C.; Noth, E.M.; Mann, J.K.; Pratt, B.; Balmes, J.; et al. Childhood exposure to ambient polycyclic aromatic hydrocarbons is linked to epigenetic modifications and impaired systemic immunity in T cells. Clin. Exp. Allergy 2015, 45, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Kauffmann, F.; Dizier, M.H.; Annesi-Maesano, I.; Bousquet, J.; Charpin, D.; Demenais, F.; Ecochard, D.; Feingold, J.; Gormand, F.; Grimfeld, A.; et al. EGEA (Epidemiological study on the Genetics and Environment of Asthma, bronchial hyperresponsiveness and atopy)—Descriptive characteristics. Clin. Exp. Allergy 1999, 29 (Suppl. 4), 17–21. [Google Scholar]
- The European Community Respiratory Health Survey II. Eur. Respir. J. 2002, 20, 1071–1079. [CrossRef]
- Sunyer, J.; Pekkanen, J.; Garcia-Esteban, R.; Svanes, C.; Künzli, N.; Janson, C.; de Marco, R.; Antó, J.M.; Burney, P. Asthma score: Predictive ability and risk factors. Allergy 2007, 62, 142–148. [Google Scholar] [CrossRef]
- Herr, M.; Nikasinovic, L.; Foucault, C.; Le Marec, A.M.; Giordanella, J.P.; Just, J.; Momas, I. Management of wheezing disorders in infants participating in the PARIS birth cohort. Rev. Mal. Respir. 2012, 29, 52–59. [Google Scholar] [CrossRef]
- Luna, P.N.; Hasegawa, K.; Ajami, N.J.; Espinola, J.A.; Henke, D.M.; Petrosino, J.F.; Piedra, P.A.; Sullivan, A.F.; Camargo, C.A., Jr.; Shaw, C.A.; et al. The association between anterior nares and nasopharyngeal microbiota in infants hospitalized for bronchiolitis. Microbiome 2018, 6, 2. [Google Scholar] [CrossRef]
- Toivonen, L.; Karppinen, S.; Schuez-Havupalo, L.; Waris, M.; He, Q.; Hoffman, K.L.; Petrosino, J.F.; Dumas, O.; Camargo, C.A., Jr.; Hasegawa, K.; et al. Longitudinal Changes in Early Nasal Microbiota and the Risk of Childhood Asthma. Pediatrics 2020, 146, e20200421. [Google Scholar] [CrossRef] [PubMed]
- Vanderweele, T.J. A three-way decomposition of a total effect into direct, indirect, and interactive effects. Epidemiology 2013, 24, 224–232. [Google Scholar] [CrossRef]
- Li, Z.; Rava, M.; Bédard, A.; Dumas, O.; Garcia-Aymerich, J.; Leynaert, B.; Pison, C.; Le Moual, N.; Romieu, I.; Siroux, V.; et al. Cured meat intake is associated with worsening asthma symptoms. Thorax 2017, 72, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Pacheco Da Silva, E.; Sit, G.; Goldberg, M.; Leynaert, B.; Nadif, R.; Ribet, C.; Roche, N.; Zins, M.; Varraso, R.; Dumas, D.; et al. Household use of green and homemade cleaning products, wipe application mode, and asthma among French adults from the CONSTANCES cohort. Indoor Air 2022, 32, e13078. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Paris Metropolitan Area | Randomized Daycares (n = 102) | Non-Randomized Daycares (n = 6) | |||
|---|---|---|---|---|---|
| Expected | Complete Visit | Incomplete Visit * | Pilot Visits | Other Visits | |
| 75 | 34 | 33 | 1 | 2 | |
| 92 | 26 | 25 | |||
| 93 | 17 | 15 | 1 | 1 | |
| 94 | 12 | 13 | 2 | ||
| 77 | 7 | 7 | 1 | ||
| 91 | 4 | 7 | |||
| Total | 100 | 100 | 2 | 4 | 2 |
| Characteristics | n (%) |
|---|---|
| Time for floor wet cleaning (multiple answers) | |
| in the morning, before children arrive during the day, in presence of children during the day, without children (during the nap) in the evening, after children depart | 40 (37.7) 7 (6.6) 11 (10.4) 66 (62.3) |
| Window opening during floor cleaning | |
| during cleaning only after cleaning only during and after cleaning never missing information | 52 (49.1) 1 (0.9) 31 (29.2) 6 (5.7) 16 (15.1) |
| Time for furniture cleaning (multiple answers) | |
| in the morning, before children arrive during the day, in presence of children during the day, without children (during the nap) in the evening, after children depart | 29 (27.3) 29 (27.3) 29 (27.3) 72 (67.9) |
| Window opening during furniture cleaning | |
| during cleaning only after cleaning only during and after cleaning never missing information | 62 (58.5) 3 (2.8) 29 (27.4) 10 (9.4) 2 (1.9) |
| Number of DCP used in daycares | |
| 1–2 3 4 5 6–9 | 16 (15.1) 26 (24.5) 30 (28.3) 16 (15.1) 18 (17.0) |
| Characteristics | n (%) |
|---|---|
| Women | 299 (98.4) |
| Age, years | |
| Mean ± Standard Deviation [min; max] | 43.2 ± 10.2 [18.4; 64.8] |
| Job | |
| Children care Cleaner/Cook/Clothes washing Administrative support Others | 202 (66.4) 19 (6.3) 46 (15.1) 37 (12.2) |
| Educational level | |
| <high school diploma high school to 2-level university >3-level university | 98 (32.5) 91 (30.1) 113 (37.4) |
| Smoking status | |
| Never smoker Ex-smoker Smoker | 194 (64.0) 73 (24.1) 36 (11.9) |
| Respiratory symptoms | |
| Asthma symptom score, last 12 months 0 >1 Ever Asthma Asthma attacks, last 12 months Woken by an attack of coughing, last 12 months | 261 (85.9) 43 (14.1) 45 (14.8) 21 (7.0) 49 (16.2) |
| Eczema, ever | 105 (34.4) |
| Characteristics | n (%) |
|---|---|
| Girls | 235 (47.1) |
| Daycare group | |
| <1 year old | 180 (36.1) |
| 1–2 years old | 144 (28.9) |
| >2 years old | 131 (26.3) |
| Grouped sections | 43 (8.7) |
| Age, months | |
| Mean ± Standard Deviation | 22.7 ± 10.3 |
| Respiratory symptoms | |
| Wheezing | 157 (31.5) |
| Wheezing and breathlessness | 36 (7.2) |
| Woken by breathlessness | 20 (4.2) |
| Attack of coughing during the night | 135 (27.5) |
| Bronchiolitis | 205 (42.6) |
| Asthma attack | 59 (12.1) |
| Eczema | 77 (15.4) |
| Cleaning, Daycare * | Sprays, Daycare † | |
|---|---|---|
| Wheezing (31%) | 1.51 | 1.70 |
| Nocturnal cough (27%) | 1.56 | 1.77 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Le Moual, N.; Dumas, O.; Bonnet, P.; Eworo Nchama, A.; Le Bot, B.; Sévin, E.; Pin, I.; Siroux, V.; Mandin, C.; The CRESPI Study Group. Exposure to Disinfectants and Cleaning Products and Respiratory Health of Workers and Children in Daycares: The CRESPI Cohort Protocol. Int. J. Environ. Res. Public Health 2023, 20, 5903. https://doi.org/10.3390/ijerph20105903
Le Moual N, Dumas O, Bonnet P, Eworo Nchama A, Le Bot B, Sévin E, Pin I, Siroux V, Mandin C, The CRESPI Study Group. Exposure to Disinfectants and Cleaning Products and Respiratory Health of Workers and Children in Daycares: The CRESPI Cohort Protocol. International Journal of Environmental Research and Public Health. 2023; 20(10):5903. https://doi.org/10.3390/ijerph20105903
Chicago/Turabian StyleLe Moual, Nicole, Orianne Dumas, Pierre Bonnet, Anastasie Eworo Nchama, Barbara Le Bot, Etienne Sévin, Isabelle Pin, Valérie Siroux, Corinne Mandin, and The CRESPI Study Group. 2023. "Exposure to Disinfectants and Cleaning Products and Respiratory Health of Workers and Children in Daycares: The CRESPI Cohort Protocol" International Journal of Environmental Research and Public Health 20, no. 10: 5903. https://doi.org/10.3390/ijerph20105903