

Self-Management of Diabetes and Associated Factors among Patients Seeking Chronic Care in Tshwane, South Africa: A Facility-Based Study
 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
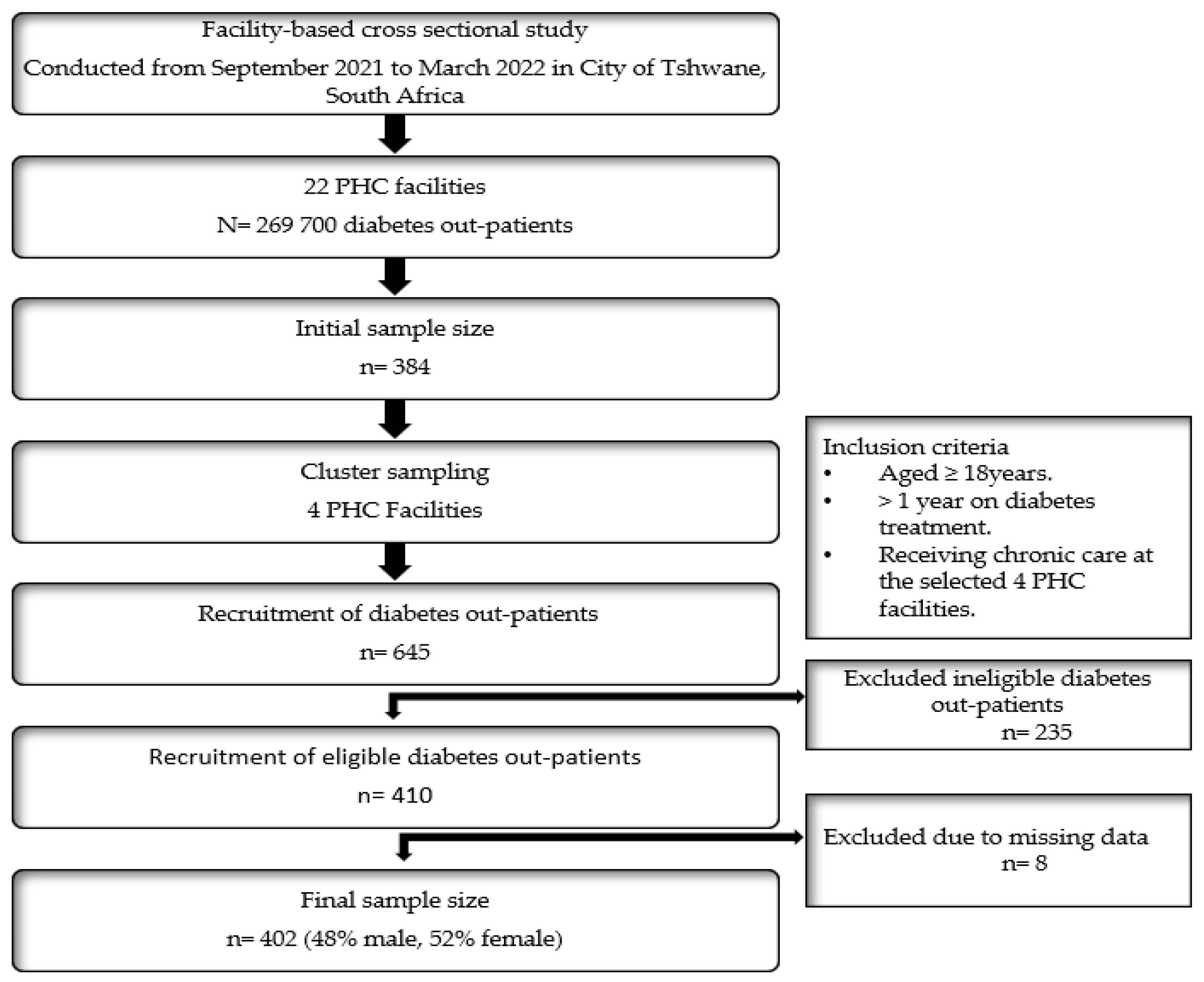
2.1. Study Design and Framework
2.2. Study Setting and Population
2.3. Sample Size and Sampling Techniques
2.4. Data Collection and Tool
2.4.1. Sociodemographic Data and Diabetes Measures, Activities, and Knowledge
2.4.2. Anthropometric and Physiological Measurements
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Characteristics of Out-Patients and Comparison by Sex
3.2. Glucose, Blood Pressure and Anthropometric Measurements of Patients
3.3. Self-Care Management Activities of the Patients
3.4. Factors Associated with Self-Management
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mbanya, J.C.N.; Motala, A.A.; Sobngwi, E.; Assah, F.; Enoru, S.T.; Assah, F.; Mbanya, J.C. Diabetes in Sub-Saharan Africa. Lancet 2010, 375, 2254–2266. [Google Scholar] [CrossRef] [PubMed]
- Chan, M. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016; Volume 58, pp. 1–88.
- Moucheraud, C.; Lenz, C.; Latkovic, M.; Wirtz, V.J. The costs of diabetes treatment in low-and middle-income countries: A systematic review. BMJ Glob. Health 2019, 4, e001258. [Google Scholar] [CrossRef] [PubMed]
- Green, A. Diabetes Risk Because of Status. 2017. Available online: https://www.news24.com/SouthAfrica/Local/City-Vision/diabetes-risk-because-of-status-20170503 (accessed on 20 March 2021).
- Giugliano, D.; Maiorino, M.I.; Bellastella, G.; Esposito, K. Glycemic control in type 2 diabetes: From medication nonadherence to residual vascular risk. Endocrine 2018, 61, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Kirkman, M.S.; Mahmud, H.; Korytkowski, M.T. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes mellitus. Endocrinol. Metab. Clin. 2018, 47, 81–96. [Google Scholar] [CrossRef] [PubMed]
- Avogaro, A.; Fadini, G.P. Microvascular complications in diabetes: A growing concern for cardiologists. Int. J. Cardiol. 2019, 291, 29–35. [Google Scholar] [CrossRef]
- Fowler, M.J. Microvascular and Macrovascular Complications of Diabetes. Clin. Diabetes 2008, 26, 77–82. [Google Scholar] [CrossRef]
- International Diabetes Federation. South Africa Diabetes Report 2010–2045. 2020. Available online: https://diabetesatlas.org/data/en/country/185/za.html (accessed on 7 March 2021).
- Bertram, M.Y.; Jaswal, A.V.; Van Wyk, V.P.; Levitt, N.S.; Hofman, K.J. The non-fatal disease burden caused by type 2 diabetes in South Africa, 2009. Glob. Health Action 2013, 6, 19244. [Google Scholar] [CrossRef]
- Ngassa Piotie, P.; Webb, E.M.; Rheeder, P. Suboptimal control for patients with type 2 diabetes in the Central Chronic Medicine Dispensing programme in South Africa. Afr. J. Prim. Health Care Fam. Med. 2021, 13, a2648. [Google Scholar] [CrossRef]
- South African National Treasury. Taxation of Sugar Sweetened Beverages in South Africa; Policy Paper; South African National Treasury: Pretoria, South Africa, 2016.
- Chatterjee, S.; Khunti, K.; Davies, M.J. Type 2 diabetes. Lancet 2017, 389, 2239–2251. [Google Scholar] [CrossRef]
- Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Colditz, G.; Liu, S.; Solomon, C.G.; Willett, W.C. Diet, lifestyle, and the risk of type 2 diabetes mellitus in women. N. Engl. J. Med. 2001, 345, 790–797. [Google Scholar] [CrossRef]
- Tuomilehto, J.; Lindström, J.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Corbin, J.M.; Strauss, A. Unending Work and Care: Managing Chronic Illness at Home; Jossey-Bass: Hoboken, NJ, USA, 1988. [Google Scholar]
- Koch, T.; Jenkin, P.; Kralik, D. Chronic illness self-management: Locating the ‘self’. J. Adv. Nurs. 2004, 48, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Elissen, A.; Nolte, E.; Knai, C.; Brunn, M.; Chevreul, K.; Conklin, A.; Durand-Zaleski, I.; Erler, A.; Flamm, M.; Frølich, A. Is Europe putting theory into practice? A qualitative study of the level of self-management support in chronic care management approaches. BMC Health Serv. Res. 2013, 13, 117. [Google Scholar] [CrossRef] [PubMed]
- Bodenheimer, T.; Wagner, E.H.; Grumbach, K. Improving primary care for patients with chronic illness. JAMA 2002, 288, 1775–1779. [Google Scholar] [CrossRef] [PubMed]
- Fina Lubaki, J.-P.; Omole, O.B.; Francis, J.M. Glycaemic control among type 2 diabetes patients in sub-Saharan Africa from 2012 to 2022: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2022, 14, 134. [Google Scholar] [CrossRef] [PubMed]
- Coetzee, A.; Beukes, A.; Dreyer, R.; Solomon, S.; van Wyk, L.; Mistry, R.; Conradie, M.; Van De Vyver, M. The prevalence and risk factors for diabetes mellitus in healthcare workers at Tygerberg hospital, Cape Town, South Africa: A retrospective study. J. Endocrinol. Metab. Diabetes S. Afr. 2019, 24, 77–82. [Google Scholar] [CrossRef]
- Erasmus, R.; Blanco, E.B.; Okesina, A.; Arana, J.M.; Gqweta, Z.; Matsha, T. Importance of family history in type 2 black South African diabetic patients. Postgrad. Med. J. 2001, 77, 323–325. [Google Scholar] [CrossRef]
- Werfalli, M.; Kassanjee, R.; Kalula, S.; Kowal, P.; Phaswana-Mafuya, N.; Levitt, N.S. Diabetes in south African older adults: Prevalence and impact on quality of life and functional disability–as assessed using SAGE wave 1 data. Glob. Health Action 2018, 11, 1449924. [Google Scholar] [CrossRef]
- Masilela, C.; Pearce, B.; Ongole, J.J.; Adeniyi, O.V.; Benjeddou, M. Factors associated with glycemic control among South African adult residents of Mkhondo municipality living with diabetes mellitus. Medicine 2020, 99, e23467. [Google Scholar] [CrossRef]
- Mercer, T.; Chang, A.C.; Fischer, L.; Gardner, A.; Kerubo, I.; Tran, D.N.; Laktabai, J.; Pastakia, S. Mitigating The Burden Of Diabetes In Sub-Saharan Africa Through An Integrated Diagonal Health Systems Approach. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2261–2272. [Google Scholar] [CrossRef]
- Adeniyi, O.V.; Yogeswaran, P.; Longo-Mbenza, B.; Ter Goon, D.; Ajayi, A.I. Cross-sectional study of patients with type 2 diabetes in OR Tambo district, South Africa. BMJ Open 2016, 6, e010875. [Google Scholar] [CrossRef] [PubMed]
- Polonsky, W.H.; Henry, R.R. Poor medication adherence in type 2 diabetes: Recognizing the scope of the problem and its key contributors. Patient Prefer. Adherence 2016, 10, 1299–1307. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Fernández, M.; Mancera-Romero, J.; Mediavilla-Bravo, J.J.; Comas-Samper, J.M.; López-Simarro, F.; Pérez-Unanua, M.P.; Iturralde-Iriso, J. Glycemic control and use of A1c in primary care patients with type 2 diabetes mellitus. Prim. Care Diabetes 2015, 9, 385–391. [Google Scholar] [CrossRef]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.L.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of hyperglycaemia in type 2 diabetes, 2015: A patient-centred approach. Update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 2015, 58, 429–442. [Google Scholar] [CrossRef] [PubMed]
- National Department Of Health. Strategic Plan for the Prevention and Control of Non-Communicable Diseases 2013–2017. 2013. Available online: extranet.who.int/ncdccs/Data/ZAF_B3_NCDs_STRAT_PLAN_1_29_1_3%5B2%5Dpdf (accessed on 14 March 2021).
- Schmitt, A.; Gahr, A.; Hermanns, N.; Kulzer, B.; Huber, J.; Haak, T. The Diabetes Self-Management Questionnaire (DSMQ): Development and evaluation of an instrument to assess diabetes self-care activities associated with glycaemic control. Health Qual. Life Outcomes 2013, 11, 138. [Google Scholar] [CrossRef] [PubMed]
- Nsimbo, K.B.A.; Erumeda, N.; Pretorius, D. Food insecurity and its impact on glycaemic control in diabetic patients attending Jabulani Dumani community health centre, Gauteng province, South Africa. Afr. J. Prim. Health Care Fam. Med. 2021, 13, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Pillay, S.; Pillay, D.; Pillay, R. Glycated haemoglobin (HbA1c) use and glycaemic control in patients living with diabetes mellitus attending public healthcare facilities in KwaZulu-Natal Province, South Africa. S. Afr. Med. J. 2021, 111, 1060–1064. [Google Scholar] [CrossRef]
- Bains, S.S.; Egede, L.E. Associations between health literacy, diabetes knowledge, self-care behaviors, and glycemic control in a low income population with type 2 diabetes. Diabetes Technol. Ther. 2011, 13, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Pheiffer, C.; Pillay-van Wyk, V.; Joubert, J.D.; Levitt, N.; Nglazi, M.D.; Bradshaw, D. The prevalence of type 2 diabetes in South Africa: A systematic review protocol. BMJ Open 2018, 8, e021029. [Google Scholar] [CrossRef]
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. Role of self-care in management of diabetes mellitus. J. Diabetes Metab. Disord. 2013, 12, 14. [Google Scholar] [CrossRef]
- National Department Of Health. Management of Type 2 Diabetes in Adults at Primary Care Level. 2014. Available online: https://www.health.gov.za/wp-content/uploads/2021/09/Management-of-type-2-Diabetes-Electronic-copy-2014_compresseda.pdf (accessed on 30 January 2023).
- Duan, D.; Kengne, A.P.; Echouffo-Tcheugui, J.B. Screening for Diabetes and Prediabetes. Endocrinol. Metab. Clin. N. Am. 2021, 50, 369–385. [Google Scholar] [CrossRef] [PubMed]
- Mutyambizi, C.; Pavlova, M.; Hongoro, C.; Groot, W. Inequalities and factors associated with adherence to diabetes self-care practices amongst patients at two public hospitals in Gauteng, South Africa. BMC Endocr. Disord. 2020, 20, 15. [Google Scholar] [CrossRef] [PubMed]
- Dedefo, M.G.; Ejeta, B.M.; Wakjira, G.B.; Mekonen, G.F.; Labata, B.G. Self-care practices regarding diabetes among diabetic patients in West Ethiopia. BMC Res. Notes 2019, 12, 212. [Google Scholar] [CrossRef] [PubMed]
- Dube, L.; Van den Broucke, S.; Dhoore, W.; Kalweit, K.; Housiaux, M. An Audit of Diabetes Self-Management Education Programs in South Africa. J. Public Health Res. 2015, 4, 581. [Google Scholar] [CrossRef]
- Owolabi, E.O.; Goon, D.T.; Ajayi, A.I.; Adeniyi, O.V. Knowledge of diabetes and associated factors in rural Eastern Cape, South Africa: A cross sectional study. PLoS ONE 2022, 17, e0269811. [Google Scholar] [CrossRef]
- Schmidt-Busby, J.; Wiles, J.; Exeter, D.; Kenealy, T. Understanding ‘context’ in the self-management of type 2 diabetes with comorbidities: A systematic review and realist evaluation. Diabetes Res. Clin. Pract. 2018, 142, 321–334. [Google Scholar] [CrossRef]
- Blonde, L. Current challenges in diabetes management. Clin. Cornerstone 2005, 7 (Suppl. S3), S6–S17. [Google Scholar] [CrossRef]
- Manickum, P.; Ramklass, S.; Madiba, T. Diabetes and lower extremity amputation—Rehabilitation pathways and outcomes at a regional hospital. S. Afr. J. Surg. 2021, 59, 128a–128g. [Google Scholar] [CrossRef]
- Statista Research Department. Share of Individuals Who Are Members of Medical Aid Schemes in South Africa in 2021, by Population Group. 2021. Available online: https://www.statista.com/aboutus/our-research-commitment (accessed on 15 April 2023).
- Brown, A.F.; Ettner, S.L.; Piette, J.; Weinberger, M.; Gregg, E.; Shapiro, M.F.; Karter, A.J.; Safford, M.; Waitzfelder, B.; Prata, P.A.; et al. Socioeconomic position and health among persons with diabetes mellitus: A conceptual framework and review of the literature. Epidemiol. Rev. 2004, 26, 63–77. [Google Scholar] [CrossRef]
- Sousa, V.D.; Zauszniewski, J.A.; Bergquist-Beringer, S.; Musil, C.M.; Neese, J.B.; Jaber, A.F. Reliability, validity and factor structure of the Appraisal of Self-Care Agency Scale-Revised (ASAS-R). J. Eval. Clin. Pract. 2010, 16, 1031–1040. [Google Scholar] [CrossRef]
- Wikipedia. City of Tshwane Metropolitan Municipality. 2023. Available online: https://en.wikipedia.org/wiki/City_of_Tshwane_Metropolitan_Municipality#cite_note-adrianfrith-8 (accessed on 12 January 2023).
- City of Tshwane. Primary Healthcare Clinic Services. 2023. Available online: https://www.tshwane.gov.za/?page_id=649 (accessed on 12 January 2023).
- Statistic South Africa. Data Reworked by Adrian Frith Tshwane—Census. 2011. Available online: https://census2011.adrianfrith.com/place/799 (accessed on 11 March 2020).
- Department of Health. South Africa Demographic and Health Survey 2003; Department of Health: Pretoria, South Africa, 2007.
- Peltzer, K. Patient experiences and health system responsiveness in South Africa. BMC Health Serv. Res. 2009, 9, 117. [Google Scholar] [CrossRef] [PubMed]
- Elfil, M.; Negida, A. Sampling Methods in Clinical Research; an Educational Review. Emergency 2016, 4, e52. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- Perneger, T.V.; Courvoisier, D.S.; Hudelson, P.M.; Gayet-Ageron, A. Sample size for pre-tests of questionnaires. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2015, 24, 147–151. [Google Scholar] [CrossRef]
- Toobert, D.J.; Hampson, S.E.; Glasgow, R.E. The summary of diabetes self-care activities measure: Results from 7 studies and a revised scale. Diabetes Care 2000, 23, 943–950. [Google Scholar] [CrossRef]
- WHO. Physical Status: The Use and Interpretation of Anthropometry; WHO Technical Report Series No. 854; WHO: Geneva, Switzerland, 1995.
- Ashwell, M. Obesity risk: Importance of the waist-to-height ratio. Nurs. Stand. 2009, 23, 49–54. [Google Scholar] [CrossRef]
- WHO. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycaemia; WHO: Geneva, Switzerland, 2006.
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Yamazaki, D.; Hitomi, H.; Nishiyama, A. Hypertension with diabetes mellitus complications. Hypertens. Res. 2018, 41, 147–156. [Google Scholar] [CrossRef]
- World Medical Association. Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects; World Medical Association: Ferney-Voltaire, France, 2001; p. 373. [Google Scholar]
- Atlas, D. International diabetes federation. In IDF Diabetes Atlas, 7th ed.; International Diabetes Federation: Brussels, Belgium, 2015; p. 2. [Google Scholar]
- Erasmus, R.; Blanco, E.B.; Okesina, A.; Gqweta, Z.; Matsha, T. Assessment of glycaemic control in stable type 2 black South African diabetics attending a peri-urban clinic. Postgrad. Med. J. 1999, 75, 603–606. [Google Scholar] [CrossRef]
- Kok, A.; Hariram, A.; Webb, D.; Amod, A. Patterns of diabetes management in South Africa: Baseline and 24-month data from the South African cohort of the DISCOVER study. J. Endocrinol. Metab. Diabetes S. Afr. 2021, 26, 60–65. [Google Scholar] [CrossRef]
- Steyn, K.; Levitt, D.; Patel, M.; Fourie, J.; Gwebushe, N.; Lombard, C.; Everett, K. Hypertension and diabetes: Poor care for patients at community health centres. S. Afr. Med. J. 2008, 98, 618–622. [Google Scholar] [CrossRef] [PubMed]
- Mokgalaboni, K.; Dludla, P.V.; Nyambuya, T.M.; Yakobi, S.H.; Mxinwa, V.; Nkambule, B.B. Monocyte-mediated inflammation and cardiovascular risk factors in type 2 diabetes mellitus: A systematic review and meta-analysis of pre-clinical and clinical studies. JRSM Cardiovasc. Dis. 2020, 9, 2048004019900748. [Google Scholar] [CrossRef] [PubMed]
- Modjadji, P. Communicable and non-communicable diseases coexisting in South Africa. Lancet Glob. Health 2021, 9, e889–e890. [Google Scholar] [CrossRef]
- Chauke, P.; Huma, M.; Madiba, S. Lost to follow up rate in the first year of ART in adults initiated in a universal test and treat programme: A retrospective cohort study in Ekurhuleni District, South Africa. Pan Afr. Med. J. 2020, 37, 198. [Google Scholar] [CrossRef]
- Mahlangu, K.; Modjadji, P.; Madiba, S. The Nutritional Status of Adult Antiretroviral Therapy Recipients with a Recent HIV Diagnosis; A Cross-Sectional Study in Primary Health Facilities in Gauteng, South Africa. Healthcare 2020, 8, 290. [Google Scholar] [CrossRef] [PubMed]
- Mabetwa, E.M.; Mokwena, K.E.; Mphekgwana, P.M.; Modjadji, P. Metabolic Syndrome and Its Components among Taxi Drivers in the City of Tshwane, South Africa. Appl. Sci. 2022, 12, 1767. [Google Scholar] [CrossRef]
- Sekgala, M.; Opperman, M.; Mpahleni, B.; McHiza, Z. Sociodemographic and lifestyle factors and the risk of metabolic syndrome in taxi drivers: A focus on street food. Front. Nutr. 2023, 10, 1112975. [Google Scholar] [CrossRef] [PubMed]
- Modjadji, P.; Bokaba, M.; Mokwena, K.E.; Mudau, T.S.; Monyeki, K.D.; Mphekgwana, P.M. Obesity as a Risk Factor for Hypertension and Diabetes among Truck Drivers in a Logistics Company, South Africa. Appl. Sci. 2022, 12, 1685. [Google Scholar] [CrossRef]
- Modjadji, P. Socio-Demographic determinants of overweight and obesity among mothers of primary school children living in a rural health and demographic surveillance system site, South Africa. Open Public Health J. 2020, 13, 518–528. [Google Scholar] [CrossRef]
- Mashinya, F.; Alberts, M.; Cook, I.; Ntuli, S. Determinants of body mass index by gender in the Dikgale Health and Demographic Surveillance System site, South Africa. Glob. Health Action 2018, 11, 1537613. [Google Scholar] [CrossRef]
- Ataklte, F.; Erqou, S.; Kaptoge, S.; Taye, B.; Echouffo-Tcheugui, J.B.; Kengne, A.P. Burden of undiagnosed hypertension in sub-saharan Africa: A systematic review and meta-analysis. Hypertension 2015, 65, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Mphekgwana, P.M.; Malema, N.; Monyeki, K.D.; Mothiba, T.M.; Makgahlela, M.; Kgatla, N.; Makgato, I.; Sodi, T. Hypertension Prevalence and Determinants among Black South African Adults in Semi-Urban and Rural Areas. Int. J. Environ. Res. Public Health 2020, 17, 7463. [Google Scholar] [CrossRef]
- Maimela, E.; Alberts, M.; Modjadji, S.E.P.; Choma, S.S.R.; Dikotope, S.A.; Ntuli, T.S.; Van Geertruyden, J.-P. The Prevalence and Determinants of Chronic Non-Communicable Disease Risk Factors amongst Adults in the Dikgale Health Demographic and Surveillance System (HDSS) Site, Limpopo Province of South Africa. PLoS ONE 2016, 11, e0147926. [Google Scholar] [CrossRef] [PubMed]
- Ntuli, S.; Maimela, E.; Alberts, M.; Choma, S.; Dikotope, S.A. Prevalence and associated risk factors of hypertension amongst adults in a rural community of Limpopo Province, South Africa. Afr. Prim. Health Care Fam. Med. 2015, 7, 847. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, N.; Sb, Y.; Am, J.; Bdp, P.; Shrestha, J.T.M.; Dl, B. Diabetes Knowledge and Associated Factors among Diabetes Patients in Central Nepal. Int. J. Collab. Res. Intern. Med. Public Health 2015, 7, 82–91. [Google Scholar]
- Lambrinou, E.; Hansen, T.B.; Beulens, J.W. Lifestyle factors, self-management and patient empowerment in diabetes care. Eur. J. Prev. Cardiol. 2019, 26, 55–63. [Google Scholar] [CrossRef]
- Sidahmed, S.; Geyer, S.; Beller, J. Socioeconomic inequalities in diabetes prevalence: The case of South Africa between 2003 and 2016. BMC Public Health 2023, 23, 324. [Google Scholar] [CrossRef]
- Ataguba, J.E.; Akazili, J.; McIntyre, D. Socioeconomic-related health inequality in South Africa: Evidence from General Household Surveys. Int. J. Equity Health 2011, 10, 48. [Google Scholar] [CrossRef]
- Agardh, E.; Allebeck, P.; Hallqvist, J.; Moradi, T.; Sidorchuk, A. Type 2 diabetes incidence and socio-economic position: A systematic review and meta-analysis. Int. J. Epidemiol. 2011, 40, 804–818. [Google Scholar] [CrossRef]
- Rivera, L.A.; Lebenbaum, M.; Rosella, L.C. The influence of socioeconomic status on future risk for developing Type 2 diabetes in the Canadian population between 2011 and 2022: Differential associations by sex. Int. J. Equity Health 2015, 14, 101. [Google Scholar] [CrossRef]
- Manickum, P.; Madiba, T.; Ramklass, S. The effectiveness of diabetic foot-care education in a South African regional hospital: A randomised controlled trial. J. Endocrinol. Metab. Diabetes S. Afr. 2022, 27, 20–31. [Google Scholar] [CrossRef]
- Mutyambizi, C.; Booysen, F.; Stokes, A.; Pavlova, M.; Groot, W. Lifestyle and socio-economic inequalities in diabetes prevalence in South Africa: A decomposition analysis. PLoS ONE 2019, 14, e0211208. [Google Scholar] [CrossRef] [PubMed]
- Xhakaza, L.; Abrahams-October, Z.; Mohammednur, M.M.; Pearce, B.; Adeniyi, O.V.; Johnson, R.; Benjeddou, M. Socio-demographic and modifiable risk factors of diabetes and hypertension among resource constrained patients from rural areas in Mdantsane Township in South Africa. Afr. Health Sci. 2020, 20, 1344–1354. [Google Scholar] [CrossRef] [PubMed]
- Willi, C.; Bodenmann, P.; Ghali, W.A.; Faris, P.D.; Cornuz, J. Active smoking and the risk of type 2 diabetes: A systematic review and meta-analysis. JAMA 2007, 298, 2654–2664. [Google Scholar] [CrossRef]
- Salama, M.S.; Isunju, J.B.; David, S.K.; Muneza, F.; Ssemanda, S.; Tumwesigye, N.M. Prevalence and factors associated with alcohol consumption among persons with diabetes in Kampala, Uganda: A cross sectional study. BMC Public Health 2021, 21, 719. [Google Scholar] [CrossRef]
- Reddy, P.; Zuma, K.; Shisana, O.; Kim, J.; Sewpaul, R. Prevalence of tobacco use among adults in South Africa: Results from the first South African National Health and Nutrition Examination Survey. S. Afr. Med. J. 2015, 105, 648–655. [Google Scholar] [CrossRef]
- Association, A.D. Standards of medical care in diabetes—2015 abridged for primary care providers. Clin. Diabetes A Publ. Am. Diabetes Assoc. 2015, 33, 97. [Google Scholar] [CrossRef]
- Adegbola, S.A.; Marincowitz, G.J.; Govender, I.; Ogunbanjo, G.A. Assessment of self-reported adherence among patients with type 2 diabetes in Matlala District Hospital, Limpopo Province. Afr. J. Prim. Health Care Fam. Med. 2016, 8, e1–e5. [Google Scholar] [CrossRef]
- Xu, Y.; Pan, W.; Liu, H. Self-management practices of Chinese Americans with type 2 diabetes. Nurs. Health Sci. 2010, 12, 228–234. [Google Scholar] [CrossRef]
- Krass, I.; Schieback, P.; Dhippayom, T. Adherence to diabetes medication: A systematic review. Diabet. Med. 2015, 32, 725–737. [Google Scholar] [CrossRef]
- Ra, D.; Omole, O. Awareness and practices of foot self-care in patients with diabetes at Dr Yusuf Dadoo district hospital, Johannesburg. JEMDSA 2013, 18, 112–118. [Google Scholar] [CrossRef]
- Okoye, O.C.; Ohenhen, O.A. Assessment of diabetes self-management amongst Nigerians using the diabetes self-management questionnaire: A cross-sectional study. Pan Afr. Med. J. 2021, 40, 178. [Google Scholar] [CrossRef] [PubMed]
- Adjei Boakye, E.; Varble, A.; Rojek, R.; Peavler, O.; Trainer, A.K.; Osazuwa-Peters, N.; Hinyard, L. Sociodemographic Factors Associated With Engagement in Diabetes Self-management Education Among People With Diabetes in the United States. Public Health Rep. 2018, 133, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Cherrington, A.; Ayala, G.X.; Scarinci, I.; Corbie-Smith, G. Developing a family-based diabetes program for Latino immigrants: Do men and women face the same barriers? Fam. Community Health 2011, 34, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Whittemore, R.; Melkus, G.D.E.; Grey, M. Metabolic control, self-management and psychosocial adjustment in women with type 2 diabetes. J. Clin. Nurs. 2005, 14, 195–203. [Google Scholar] [CrossRef]
- Arnetz, L.; Ekberg, N.R.; Alvarsson, M. Sex differences in type 2 diabetes: Focus on disease course and outcomes. Diabetes Metab. Syndr. Obes. Targets Ther. 2014, 7, 409–420. [Google Scholar] [CrossRef] [PubMed]
- Mathew, R.; Gucciardi, E.; De Melo, M.; Barata, P. Self-management experiences among men and women with type 2 diabetes mellitus: A qualitative analysis. BMC Fam. Pract. 2012, 13, 122. [Google Scholar] [CrossRef]
- Diriba, D.C.; Bekuma, T.T.; Bobo, F.T. Predictors of self-management practices among diabetic patients attending hospitals in western Oromia, Ethiopia. PLoS ONE 2020, 15, e0232524. [Google Scholar] [CrossRef]
- Flor, L.S.; Campos, M.R. The prevalence of diabetes mellitus and its associated factors in the Brazilian adult population: Evidence from a population-based survey. Rev. Bras. Epidemiol. 2017, 20, 16–29. [Google Scholar] [CrossRef]
- Cornelis, M.C.; Chiuve, S.E.; Glymour, M.M.; Chang, S.C.; Tchetgen Tchetgen, E.J.; Liang, L.; Koenen, K.C.; Rimm, E.B.; Kawachi, I.; Kubzansky, L.D. Bachelors, divorcees, and widowers: Does marriage protect men from type 2 diabetes? PLoS ONE 2014, 9, e106720. [Google Scholar] [CrossRef]
- Umberson, D. Gender, marital status and the social control of health behavior. Soc. Sci. Med. 1992, 34, 907–917. [Google Scholar] [CrossRef]
- Akindana, A.; Ogunedo, C. Managing type 2 diabetes in Black patients. Nurse Pract. 2015, 40, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Darawad, M.W.; Hammad, S.M.; Mosleh, S.M.; Samarkandi, O.A.; Hamdan-Mansour, A.M.; Khalil, A.A.; Arabiat, D.H. Psychosocial Correlates of Diabetes Self-management Practices. Iran. J. Public Health 2017, 46, 771–781. [Google Scholar] [PubMed]
- Fock, K.M.; Khoo, J. Diet and exercise in management of obesity and overweight. J. Gastroenterol. Hepatol. 2013, 28 (Suppl. S4), 59–63. [Google Scholar] [CrossRef] [PubMed]
- Peer, N.; Steyn, K.; Lombard, C.; Lambert, E.V.; Vythilingum, B.; Levitt, N.S. Rising diabetes prevalence among urban-dwelling black South Africans. PLoS ONE 2012, 7, e43336. [Google Scholar] [CrossRef] [PubMed]
- Smalls, B.L.; Gregory, C.M.; Zoller, J.S.; Egede, L.E. Direct and indirect effects of neighborhood factors and self-care on glycemic control in adults with type 2 diabetes. J. Diabetes Complicat. 2015, 29, 186–191. [Google Scholar] [CrossRef] [PubMed]
- Chesla, C.A.; Fisher, L.; Mullan, J.T.; Skaff, M.M.; Gardiner, P.; Chun, K.; Kanter, R. Family and disease management in African-American patients with type 2 diabetes. Diabetes Care 2004, 27, 2850–2855. [Google Scholar] [CrossRef]
- Rondhianto, R.; Nursalam, N.; Kusnanto, K.; Melaniani, S.; Ahsan, A. Analysis of the Sociodemographic and Psychological Factors of the Family Caregivers’ Self-Management Capabilities for Type 2 Diabetes Mellitus. J. Ners. 2020, 14, 215. [Google Scholar] [CrossRef]
- Lubkin, I.M.; Larsen, P.D. Family Caregiving. In Chronic Illnes: Impact and Intervention, 8th ed.; Jones & Bartlett Learning, LLC: Burlington, MA, USA, 2012; pp. 47–54. [Google Scholar]
- Kugbey, N.; Oppong Asante, K.; Adulai, K. Illness perception, diabetes knowledge and self-care practices among type-2 diabetes patients: A cross-sectional study. BMC Res Notes 2017, 10, 381. [Google Scholar] [CrossRef]
- American Diabetes Association. Tests of Glycemia in Diabetes. Diabetes Care 2003, 26 (Suppl. S1), s106–s108. [Google Scholar] [CrossRef]
- Kolossváry, E.; Farkas, K.; Karahan, O.; Golledge, J.; Schernthaner, G.-H.; Karplus, T.; Bernardo, J.J.; Marschang, S.; Abola, M.T.; Heinzmann, M.; et al. The importance of socio-economic determinants of health in the care of patients with peripheral artery disease: A narrative review from VAS. Vasc. Med. 2023. [Google Scholar] [CrossRef] [PubMed]
- Masupe, T.; Onagbiye, S.; Puoane, T.; Pilvikki, A.; Alvesson, H.M.; Delobelle, P. Diabetes self-management: A qualitative study on challenges and solutions from the perspective of South African patients and health care providers. Glob. Health Action 2022, 15, 2090098. [Google Scholar] [CrossRef] [PubMed]
- Yildirim Duman, J.G. Self-Management of Chronic Diseases: A Descriptive Phenomenological Study. Soc. Work Public Health 2021, 36, 300–310. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | All | Males | Females | p-Value |
|---|---|---|---|---|
| (n = 402) | (n = 192) | (n = 210) | ||
| n (%) | n (%) | n (%) | ||
| Age (years) | ||||
| ≤45 | 252 (63) | 126 (66) | 129 (61) | 0.383 |
| >45 | 147 (37) | 66 (34) | 81 (39 | |
| Place of residence | ||||
| Urban | 291 (72) | 291 (72) | 146 (76) | 0.117 |
| Peri-urban | 111 (28) | 111 (24) | 46 (24) | |
| Race | ||||
| Black Africans | 179 (45) | 79 (41) | 100 (48) | 0.013 * |
| Whites | 185 (40) | 101 (53) | 84 (40) | |
| Coloureds | 33 (8) | 12 (6) | 21 (10) | |
| Indian/Asian | 5 91)) | 0 (0) | 5 (2) | |
| Marital status | ||||
| Single | 161 (40) | 82 (42) | 79 (38) | 0.005 * |
| Married | 175 (44) | 88 (46) | 87 (41) | |
| Divorced | 36 (9) | 17 (9) | 25 (12) | |
| Widowed | 30 (7) | 5 (3) | 19 (9) | |
| Level of education | ||||
| No school/Primary | 48 (12) | 21 (11) | 27 (13) | 0.125 |
| Secondary | 136 (34) | 76 (40) | 60 (29) | |
| Completed grade 12. | 198 (48) | 85 (44) | 107 (51) | |
| Post grade 12 | 26 (6) | 10 (15) | 16 (8) | |
| Household income/month | ||||
| <$83,06 | 20 (5) | 8 (4) | 12 (6) | 0.228 |
| $83,11–$276,85 | 214 (53) | 104 (54) | 110 (52) | |
| $276,91–$553,70 | 51 (13) | 20 (10) | 31 (15) | |
| $553,76–$830,55 | 65 (16) | 38 (20) | 27 (13) | |
| >830,55 | 52 (13) | 22 (12) | 30 (14) | |
| Social support of family and friends | ||||
| Poor | 38 (9) | 19 (10) | 19 (9) | |
| Average | 85 (21) | 39 (20) | 45 (21) | 0.934 |
| Good | 280 (70) | 134 (70) | 146 (70) | |
| Duration of diabetes diagnosis | ||||
| <5 | 199 (49) | 96 (50) | 103 (49) | 0.849 |
| ≥5 | 203 (51) | 96 (50) | 107 (51) | |
| Have comorbid conditions | ||||
| No | 371 (92) | 182 (95) | 189 (90) | 0.072 |
| Yes | 31 (8) | 10 (5) | 21 (10) | |
| Comorbid conditions | ||||
| High blood pressure (yes) | 94 (24) | 41 (21) | 56 (27) | 0.214 |
| High cholesterol (yes) | 86 (21) | 44 (23) | 42 (20) | 476 |
| Heart disease (yes) | 16 (4) | 10 (5) | 6 (3) | 0.228 |
| Combination of the above (yes) | 24 (6) | 15 (81) | 9 (5) | 0.136 |
| Diabetes complications | ||||
| Amputation (yes) | 28 (7) | 16 (8) | 12 (6) | 0.303 |
| Kidney disease (yes) | 21 (5) | 12 (6) | 9 (4) | 0.377 |
| Neuropathy (yes) | 88 (22) | 33 (17) | 55 (26) | 0.029 * |
| Eyesight problem (yes) | 64 (16) | 31 (16) | 33 (16) | 0.906 |
| More than two of the above (yes) | 25 (6) | 12 (6) | 13 (6) | 0.89 |
| Ever been hospitalised | ||||
| No | 311 (77) | 157 (82) | 154 (73) | 0.043 * |
| Yes | 91 (23) | 35 (18) | 56 (27) | |
| Blood glucose self-testing | ||||
| No | 198 (49) | 93 (48) | 105 (50) | 0.754 |
| Yes | 204 (51) | 99 (52) | 105 (50) | |
| Diabetes medication | ||||
| Oral hypoglycaemics tablets (yes) | 197 (49) | 74 (39) | 123 (59) | ≤0.0001 * |
| Insulin (yes) | 112 (28) | 72 (38) | 39 (19) | ≤0.0001 * |
| Both above (yes) | 85 (21) | 40 (21) | 45 (21) | 0.884 |
| Neither (yes) | 8 (2) | 5 (3) | 3 (1) | 0.399 |
| Diabetes knowledge | ||||
| Good | 61 (15) | 28 (15) | 33 (16) | 0.165 |
| Average | 222 (55) | 11 (60) | 107 (51) | |
| Poor | 119 (30) | 49 (26) | 70 (33) | |
| Variables | All | Males | Females | p-Value |
|---|---|---|---|---|
| (n = 402) | (n = 192) | (n = 210) | ||
| n (%) | n (%) | n (%) | ||
| Glucose (mmol/L) | 0.012 * | |||
| controlled | 313 (78) | 160 (83) | 153 (73) | |
| uncontrolled | 89 (22) | 36 (17) | 57 (27) | |
| Hypertension (mmHg) | 0.725 | |||
| normal | 286 (71) | 135 (70) | 151 (72) | |
| hypertension | 116 (29) | 57 (30) | 59 (28) | |
| BMI (Kg/m2) | 0.007 * | |||
| normal | 29 (7) | 15 (8) | 14 (7) | |
| overweight | 122 (30) | 72 (38) | 50 (24) | |
| obese | 251 (63) | 105 (55) | 146 (70) | |
| WC (cm) | 0.450 | |||
| normal | 27 (7) | 11 (6) | 16 (8) | |
| abdominal obesity | 375 (93) | 181 (94) | 199 (92) | |
| WHR | 0.386 | |||
| normal | 23 (6) | 13 (8) | 10 (5) | |
| abdominal obesity | 379 (94) | 179 (93) | 200 (95) | |
| WHtR | 0.338 | |||
| normal | 1 (1) | 0 (0) | 1 (1) | |
| abdominal obesity | 401 (99) | 192 (100) | 209 (99) |
| Self-Management Activities | Mean ± SD | Categories | n (%) |
|---|---|---|---|
| Diet On how many of the past seven (7) days did you eat five or more servings of fruit and/or vegetables? High fat foods On how many of the past seven (7) days did you eat high fat foods such as red meat of full-fat dairy products? | 3.4 ± 2.0 3.4 ± 1.6 | Poor Fair Good Poor Fair Good | 190 (47) 166 (41) 46 (11) 197 (49) 174 (43) 31 (8) |
| Exercise On how many of the past seven (7) days did you participate in at least 30 min of continuous exercise? (Total minutes of continuous activity, including walking) | 1.6 ± 2.1 | Poor Fair Good | 282 (70) 66 (16) 54 (13) |
| Blood glucose self-testing On how many of the past seven (7) days did you test your blood sugar? | 1.1 ± 1.4 | Poor Fair Good | 373 (93) 21 (5) 8 (2) |
| Feet days On how many of the past seven (7) days did you check your feet for any wounds, skin changes or ingrown toenails? Shoe care On how many of the past seven (7) days did you inspect the inside of your shoes for any holes, thorns, small stones, or other abnormalities that may cause injury | 3.0 ± 2.2 2.4 ± 2.2 | Poor Fair Good Poor Fair Good | 243 (60) 99 (25) 60 (15) 280 (70) 73 (18) 49 (12) |
| Medication On how many of the last seven (7) days did you take your diabetes medication as recommended? | 5.8 ± 1.5 | Poor Fair Good | 38 (10) 93 (23) 271 (67) |
| Smoking If you are a smoker, on how many of the past seven (7) days did you smoke? How many cigarettes did you smoke on average every day? _______cigarettes I do not smoke | 2.2 ± 1.5 | Non Light Heavy | 264 (66) 39 (10) 99 (25) |
| Alcohol consumption If you drink alcohol, on how many of the past seven (7) days did you drink alcohol? How many alcoholic beverages did you drink on average per day? _______drinks I do not drink alcohol | 1.0 ± 1.6 | Non Light Heavy | 262 (65) 7 (2) 133 (33) |
| Combined Scores | Mean ± SD | Categories | n (%) | Range |
|---|---|---|---|---|
| Total diet score | 9.77 ± 2.3 | Poor | 29 (7) | 2–17 |
| (Mean fruit/veg and inversion high fat) | Fair | 333 (83) | ||
| + Sweets + Good diet =17 | Good | 40 (10) | ||
| Total exercise score | 6.99 ± 3.76 | Poor | 238 (59) | 2–17 |
| Fair | 126 (31) | |||
| Exercise days + Avoid exercise + Physical activity = 17 | Good | 38 (10) | ||
| Total medication score | 9.89 ± 2.26 | Poor | 11 (3) | 3–12 |
| Medication days + Forgetting medication = 12 | Fair | 90 (22) | ||
| Good | 301 (75) | |||
| Total self-testing score | 3.69 ± 2.20 | Poor | 289 (72) | 1–12 |
| Testing days + Measure = 12 | Fair | 99 (25) | ||
| Good | 14 (3) | |||
| Total self-management | 41.5 ± 8.2 | Poor | 125 (31) | 21–71 |
| (Total diet score, total exercise score, total medication score, total self-testing score, foot care (Mean feet days + shoes days), smoking (1 if smoker, 0 if non-smoker), alcohol (1 if drinker, 0 if non-smoker), doctor, and self-care = 77 |
| Self-Management | OR (95%CI) | p-Value | AOR (95%CI) | p-Value |
|---|---|---|---|---|
| Sex | ||||
| Females | 1 | 1 | ||
| Males | 0.56 (0.37–0.86) | 0.008 * | 0.55 (0.34–0.90) | 0.017 * |
| Race | ||||
| Black | 1 | |||
| Coloured | 1.58 (1.01–2.46) | 0.045 * | 2.84 (1.69–4. 77) | ≤0.0001 * |
| White | 1.82 (0.78–4.28) | 0.166 | 3.84 (1.46–10.1) | 0.006 * |
| Other | 2.34 (0.25–21.35) | 0.452 | 2.70 (0.25–29.5) | 0.417 |
| Marital status | ||||
| Single | 1 | |||
| Married | 1.19 (0.75–1.89) | 0.451 | 1.39 (0.83–2.34) | 0.216 |
| Divorced | 2.52 (0.92–6.96) | 0.074 | 3.41 (1.13–10.29) | 0.029 * |
| Widowed | 0.79 (0.38–1.67) | 0.542 | 0.86 (0.36–2.04) | 0.731 |
| Social Support | ||||
| Poor | 1 | |||
| Average | 2.86 (1.04–4.94) | 0.041 * | 2.51 (1.05–6.00) | 0.038 * |
| Good | 2.91 (1.46–5.80) | 0.002 * | 4.49 (1.61–7.57) | 0.002 * |
| BMI | ||||
| Normal | 1 | |||
| Overweight | 0.64 (0.25–1.82) | 0.402 | 0.74 (0.23–2.36) | 0.617 |
| Obesity | 0.37 (0.14–1.01) | 0.052 | 0.31 (0.10–0.95) | 0.040 * |
| Uncontrolled | ||||
| glucose | ||||
| <7.0 mmol/l | 1 | |||
| ≥7.0 mmol/l | 2.94 (1.59–5.45) | 0.001 * | 2.97 (1.47–5.98) | 0.002 * |
| Diabetes knowledge | ||||
| Poor | 1 | |||
| Average | 0.66 (0.41–1.06) | 0.087 | 0.58 (0.34–0.10) | 0.049 * |
| Good | 3.09 (1.28–7.45) | 0.012 * | 1.86 (0.71–4.91) | 0.209 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zwane, J.; Modjadji, P.; Madiba, S.; Moropeng, L.; Mokgalaboni, K.; Mphekgwana, P.M.; Kengne, A.P.; Mchiza, Z.J.-R. Self-Management of Diabetes and Associated Factors among Patients Seeking Chronic Care in Tshwane, South Africa: A Facility-Based Study. Int. J. Environ. Res. Public Health 2023, 20, 5887. https://doi.org/10.3390/ijerph20105887
Zwane J, Modjadji P, Madiba S, Moropeng L, Mokgalaboni K, Mphekgwana PM, Kengne AP, Mchiza ZJ-R. Self-Management of Diabetes and Associated Factors among Patients Seeking Chronic Care in Tshwane, South Africa: A Facility-Based Study. International Journal of Environmental Research and Public Health. 2023; 20(10):5887. https://doi.org/10.3390/ijerph20105887
Chicago/Turabian StyleZwane, Janke, Perpetua Modjadji, Sphiwe Madiba, Lucky Moropeng, Kabelo Mokgalaboni, Peter Modupi Mphekgwana, Andre Pascal Kengne, and Zandile June-Rose Mchiza. 2023. "Self-Management of Diabetes and Associated Factors among Patients Seeking Chronic Care in Tshwane, South Africa: A Facility-Based Study" International Journal of Environmental Research and Public Health 20, no. 10: 5887. https://doi.org/10.3390/ijerph20105887