
Accuracy of Fetal Biacromial Diameter and Derived Ultrasonographic Parameters to Predict Shoulder Dystocia: A Prospective Observational Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gherman, R.B.; Ouzounian, J.G.; Goodwin, T.M. Obstetric maneuvers for shoulder dystocia and associated fetal morbidity. Am. J. Obstet. Gynecol. 1998, 178, 1126–1130. [Google Scholar] [CrossRef]
- Gauthaman, N.; Walters, S.; Tribe, I.-A.; Goldsmith, L.; Doumouchtsis, S.K. Shoulder dystocia and associated manoeuvres as risk factors for perineal trauma. Int. Urol. J. 2016, 27, 571–577. [Google Scholar] [CrossRef]
- Gherman, R.B.; Goodwin, T.M.; Souter, I.; Neumann, K.; Ouzounian, J.G.; Paul, R.H. The McRoberts’ maneuver for the alleviation of shoulder dystocia: How successful is it? Am. J. Obstet. Gynecol. 1997, 176, 656–661. [Google Scholar] [CrossRef]
- Beta, J.; Khan, N.; Khalil, A.; Fiolna, M.; Ramadan, G.; Akolekar, R. Maternal and neonatal complications of fetal macrosomia: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2019, 54, 308–318. [Google Scholar] [CrossRef] [Green Version]
- American College of Obstetricians and Gynecologists. Shoulder dystocia. Practice bulletin No. 178. Obstet. Gynecol. 2017, 129, e123–e133. [Google Scholar] [CrossRef]
- Ouzounian, J.G.; Korst, L.M.; Miller, D.A.; Lee, R.H. Brachial plexus palsy and shoulder dystocia: Obstetric risk factors remain elusive. Am. J. Perinatol. 2013, 30, 303–308. [Google Scholar]
- Cheng, Y.W.; Norwitz, E.R.; Caughey, A.B. The relationship of fetal position and ethnicity with shoulder dystocia and birth injury. Am. J. Obstet. Gynecol. 2006, 195, 856–862. [Google Scholar] [CrossRef]
- Øverland, E.; Vatten, L.; Eskild, A. Pregnancy week at delivery and the risk of shoulder dystocia: A population study of 2 014 956 deliveries. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Schummers, L.; Hutcheon, J.A.; Bodnar, L.M.; Lieberman, E.; Himes, K.P. Risk of adverse pregnancy outcomes by prepregnancy body mass index: A population-based study to inform prepregnancy weight loss counseling. Obstet. Gynecol. 2015, 125, 133. [Google Scholar] [CrossRef] [Green Version]
- Abell, S.K.; Boyle, J.A.; de Courten, B.; Knight, M.; Ranasinha, S.; Regan, J.; Soldatos, G.; Wallace, E.M.; Zoungas, S.; Teede, H.J. Contemporary type 1 diabetes pregnancy outcomes: Impact of obesity and glycaemic control. Med. J. Aust. 2016, 205, 162–167. [Google Scholar] [CrossRef]
- Burkhardt, T.; Schmidt, M.; Kurmanavicius, J.; Zimmermann, R.; Schäffer, L. Evaluation of fetal anthropometric measures to predict the risk for shoulder dystocia. Ultrasound Obstet. Gynecol. 2014, 43, 77–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berggren, E.K.; Boggess, K.A.; Funk, M.J.; Stuebe, A.M. Racial disparities in perinatal outcomes among women with gestational diabetes. J. Women Health 2012, 21, 521–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parantainen, J.; Palomäki, O.; Talola, N.; Uotila, J. Clinical and sonographic risk factors and complications of shoulder dystocia–a case-control study with parity and gestational age matched controls. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 177, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Mazouni, C.; Porcu, G.; Cohen-Solal, E.; Heckenroth, H.; Guidicelli, B.; Bonnier, P.; Gamerre, M. Maternal and anthropomorphic risk factors for shoulder dystocia. Acta Obstet. Et Gynecol. Scand. 2006, 85, 567–570. [Google Scholar] [CrossRef] [PubMed]
- Kleitman, V.; Feldman, R.; Walfisch, A.; Toledano, R.; Sheiner, E. Recurrent shoulder dystocia: Is it predictable? Arch. Gynecol. Obstet. 2016, 294, 1161–1166. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Hockley, C.; Quigley, M.A.; Yeh, P.; Impey, L. Antenatal and intrapartum prediction of shoulder dystocia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 151, 134–139. [Google Scholar] [CrossRef]
- Dodd, J.M.; Catcheside, B.; Scheil, W. Can shoulder dystocia be reliably predicted? Aust. N. Z. J. Obstet. Gynaecol. 2012, 52, 248–252. [Google Scholar] [CrossRef]
- Leduc, D.; Biringer, A.; Lee, L.; Dy, J.; Corbett, T.; Duperron, L.; Lange, I.; Muise, S.; Parish, B.; Regush, L. Induction of labour. J. Obstet. Gynaecol. Can. 2013, 35, 840–857. [Google Scholar] [CrossRef]
- Gülmezoglu, A.M.; Crowther, C.A.; Middleton, P.; Heatley, E. Induction of labour for improving birth outcomes for women at or beyond term. Cochrane Database Syst. Rev. 2012, 13, CD004945. [Google Scholar] [CrossRef]
- Riemma, G.; La Verde, M.; Schiattarella, A.; Cobellis, L.; De Franciscis, P.; Colacurci, N.; Morlando, M. Efficacy of hyoscine butyl-bromide in shortening the active phase of labor: Systematic review and meta-analysis of randomized trials. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 252, 218–224. [Google Scholar] [CrossRef]
- Cyna, A.M.; Dodd, J. Clinical update: Obstetric anaesthesia. Lancet 2007, 370, 640–642. [Google Scholar] [CrossRef]
- Maronge, L.; Bogod, D. Complications in obstetric anaesthesia. Anaesthesia 2018, 73, 61–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riemma, G.; Schiattarella, A.; Cianci, S.; La Verde, M.; Morlando, M.; Sisti, G.; Esposito, I.; Della Corte, L.; Sansone, P.; De Franciscis, P. Transversus abdominis plane block versus wound infiltration for post-cesarean section analgesia: A systematic review and meta-analysis of randomized controlled trials. Int. J. Gynecol. Obstet. 2021, 153, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Christoffersson, M.; Kannisto, P.; Rydhstroem, H.; Stale, H.; Walles, B. Shoulder dystocia and brachial plexus injury: A case-control study. Acta Obstet. Gynecol. Scand. 2003, 82, 147–151. [Google Scholar] [CrossRef]
- Cohen, B.K.; Penning, S.; Ansley, D.; Porto, M.; Garite, T. The incidence and severity of shoulder dystocia correlates with a sonographic measurement of asymmetry in patients with diabetes. Am. J. Perinatol. 1999, 16, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Modanlou, H.D.; Komatsu, G.; Dorchester, W.; Freeman, R.K.; Bosu, S.K. Large-for-gestational-age neonates: Anthropometric reasons for shoulder dystocia. Obstet. Gynecol. 1982, 60, 417–423. [Google Scholar]
- Youssef, A.E.A.; Amin, A.F.; Khalaf, M.; Khalaf, M.S.; Ali, M.K.; Abbas, A.M. Fetal biacromial diameter as a new ultrasound measure for prediction of macrosomia in term pregnancy: A prospective observational study. J. Matern. Fetal Neonatal Med. 2019, 32, 2674–2679. [Google Scholar] [CrossRef]
- Syngelaki, A.; Hammami, A.; Bower, S.; Zidere, V.; Akolekar, R.; Nicolaides, K. Diagnosis of fetal non-chromosomal abnormalities on routine ultrasound examination at 11–13 weeks’ gestation. Ultrasound Obstet. Gynecol. 2019, 54, 468–476. [Google Scholar] [CrossRef] [Green Version]
- Esinler, D.; Bircan, O.; Esin, S.; Sahin, E.G.; Kandemir, O.; Yalvac, S. Finding the best formula to predict the fetal weight: Comparison of 18 formulas. Gynecol. Obstet. Investig. 2015, 80, 78–84. [Google Scholar] [CrossRef]
- Devane, D.; Lalor, J.G.; Daly, S.; McGuire, W.; Cuthbert, A.; Smith, V. Cardiotocography versus intermittent auscultation of fetal heart on admission to labour ward for assessment of fetal wellbeing. Cochrane Database Syst. Rev. 2017, 26, CD005122. [Google Scholar] [CrossRef]
- La Verde, M.; Riemma, G.; Torella, M.; Torre, C.; Cianci, S.; Conte, A.; Capristo, C.; Morlando, M.; Colacurci, N.; De Franciscis, P. Impact of Braxton-Hicks contractions on fetal wellbeing; a prospective analysis through computerised cardiotocography. J. Obstet. Gynaecol. 2021, 1–5. [Google Scholar] [CrossRef] [PubMed]
- La Verde, M.; Torella, M.; Lanza, G.; Rapisarda, A.M.C.; Morlando, M.; Cianci, S.; Colacurci, N.; Capristo, C.; Torre, C.; De Franciscis, P.; et al. Objective and quantitative evaluation of fetal hiccups by computerized cardiotocography: A prospective observational study. Ital. J. Gynaecol. Obstet. 2021, 33, 249–255. [Google Scholar] [CrossRef]
- Gourounti, K.; Sandall, J. Admission cardiotocography versus intermittent auscultation of fetal heart rate: Effects on neonatal Apgar score, on the rate of caesarean sections and on the rate of instrumental delivery—A systematic review. Int. J. Nurs. Stud. 2007, 44, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Nocon, J.J.; McKenzie, D.K.; Thomas, L.J.; Hansell, R.S. Shoulder dystocia: An analysis of risks and obstetric maneuvers. Am. J. Obstet. Gynecol. 1993, 168, 1732–1739. [Google Scholar] [CrossRef]
- Revicky, V.; Mukhopadhyay, S.; Morris, E.P.; Nieto, J.J. Can we predict shoulder dystocia? Arch. Gynecol. Obstet. 2012, 285, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Belfort, M.A.; Dildy, G.A.; Saade, G.R.; Suarez, V.; Clark, S.L. Prediction of shoulder dystocia using multivariate analysis. Am. J. Perinatol. 2007, 24, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Palatnik, A.; Grobman, W.A.; Hellendag, M.G.; Janetos, T.M.; Gossett, D.R.; Miller, E.S. Predictors of shoulder dystocia at the time of operative vaginal delivery. Am. J. Obstet. Gynecol. 2016, 215, 624.e1–624.e5. [Google Scholar] [CrossRef]
- Tsur, A.; Batsry, L.; Toussia-Cohen, S.; Rosenstein, M.G.; Barak, O.; Brezinov, Y.; Yoeli-Ullman, R.; Sivan, E.; Sirota, M.; Druzin, M.L. Development and validation of a machine-learning model for prediction of shoulder dystocia. Ultrasound Obstet. Gynecol. 2020, 56, 588–596. [Google Scholar] [CrossRef]
- Maruotti, G.M.; Saccone, G.; Martinelli, P. Third trimester ultrasound soft-tissue measurements accurately predicts macrosomia. J. Matern. Fetal Neonatal Med. 2017, 30, 972–976. [Google Scholar] [CrossRef] [Green Version]
- Dyachenko, A.; Ciampi, A.; Fahey, J.; Mighty, H.; Oppenheimer, L.; Hamilton, E.F. Prediction of risk for shoulder dystocia with neonatal injury. Am. J. Obstet. Gynecol. 2006, 195, 1544–1549. [Google Scholar] [CrossRef]
- Rouse, D.J.; Owen, J. Prophylactic cesarean delivery for fetal macrosomia diagnosed by means of ultrasonography—A Faustian bargain? Am. J. Obstet. Gynecol. 1999, 181, 332–338. [Google Scholar] [CrossRef]
- Miller, R.S.; Devine, P.C.; Johnson, E.B. Sonographic fetal asymmetry predicts shoulder dystocia. J. Ultrasound Med. 2007, 26, 1523–1528. [Google Scholar] [CrossRef]
- Gerber, S.; Goldsmith, S.; Sharkey, J.; Grobman, W. 236: Ultrasonographic prediction of shoulder dystocia risk. Am. J. Obstet. Gynecol. 2008, 199, S76. [Google Scholar] [CrossRef]
- Terzi, E. A new approach to predicting shoulder dystocia: Fetal clavicle measurement. Turk. J. Med. Sci. 2021, 51, 1932–1939. [Google Scholar] [CrossRef] [PubMed]
- Hill, M.G.; Cohen, W.R. Shoulder dystocia: Prediction and management. Women Health 2016, 12, 251–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hope, P.; Breslin, S.; Lamont, L.; Lucas, A.; Martin, D.; Moore, I.; Pearson, J.; Saunders, D.; Settatree, R. Fatal shoulder dystocia: A review of 56 cases reported to the Confidential Enquiry into Stillbirths and Deaths in Infancy. BJOG Int. J. Obstet. Gynaecol. 1998, 105, 1256–1261. [Google Scholar] [CrossRef] [PubMed]
- Inglis, S.R.; Feier, N.; Chetiyaar, J.B.; Naylor, M.H.; Sumersille, M.; Cervellione, K.L.; Predanic, M. Effects of shoulder dystocia training on the incidence of brachial plexus injury. Am. J. Obstet. Gynecol. 2011, 204, 322.e1–322.e6. [Google Scholar] [CrossRef]
- Schifrin, B.S.; Cohen, W.R. The maternal fetal medicine viewpoint: Causation and litigation. In Shoulder Dystocia and Birth Injury; Springer: Berlin/Heidelberg, Germany, 2009; pp. 227–247. [Google Scholar]
- Athukorala, C.; Crowther, C.A.; Willson, K.; Austrailian Carbohydrate Intolerance Study in Pregnant Women (ACHOIS) Trial Group. Women with gestational diabetes mellitus in the ACHOIS trial: Risk factors for shoulder dystocia. Aust. N. Z. J. Obstet. Gynaecol. 2007, 47, 37–41. [Google Scholar] [CrossRef]
- Keller, J.D.; Lopez-Zeno, J.A.; Dooley, S.L.; Socol, M.L. Shoulder dystocia and birth trauma in gestational diabetes: A five-year experience. Am. J. Obstet. Gynecol. 1991, 165, 928–930. [Google Scholar] [CrossRef]
- Young, B.C.; Ecker, J.L. Fetal macrosomia and shoulder dystocia in women with gestational diabetes: Risks amenable to treatment? Curr. Diabetes Rep. 2013, 13, 12–18. [Google Scholar] [CrossRef]
- Sherer, D.M.; Sokolovski, M.; Dalloul, M.; Khoury-Collado, F.; Osho, J.A.; Lamarque, M.D.; Abulafia, O. Fetal clavicle length throughout gestation: A nomogram. Ultrasound Obstet. Gynecol. 2006, 27, 306–310. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age, (years) | |
| mean ± SD | 31.67 ± 5.6 |
| Height, (cm) | |
| mean ± SD | 162.8 ± 5.7 |
| Pre-gestational weight, (Kg) | |
| mean ± SD | 78.4 ± 14.47 |
| BMI, (Kg/m2) | |
| mean ± SD | 29.65 ± 5.18 |
| Weight gain, (Kg) | |
| mean ± SD | 15.88 ± 17.05 |
| Week of gestation | |
| mean ± SD | 40.0 ± 1.1 |
| Parity, | |
| mean ± SD | 0.4 ± 0.7 |
| Primigravida, | |
| number (%) | 40 (44.4) |
| Multigravida, | |
| number (%) | 60 (55.56) |
| Previous miscarriage, | |
| number (%) | 24 (26.67) |
| Gestational diabetes, | |
| number (%) | 11 (12.22) |
| Pregestational diabetes mellitus, | |
| number (%) | 1 (1.11) |
| Gestational hypertension and preeclampsia, | |
| number ± (%) | 8 (8.89) |
| ShD (4) | No ShD (86) | p-Value | |
|---|---|---|---|
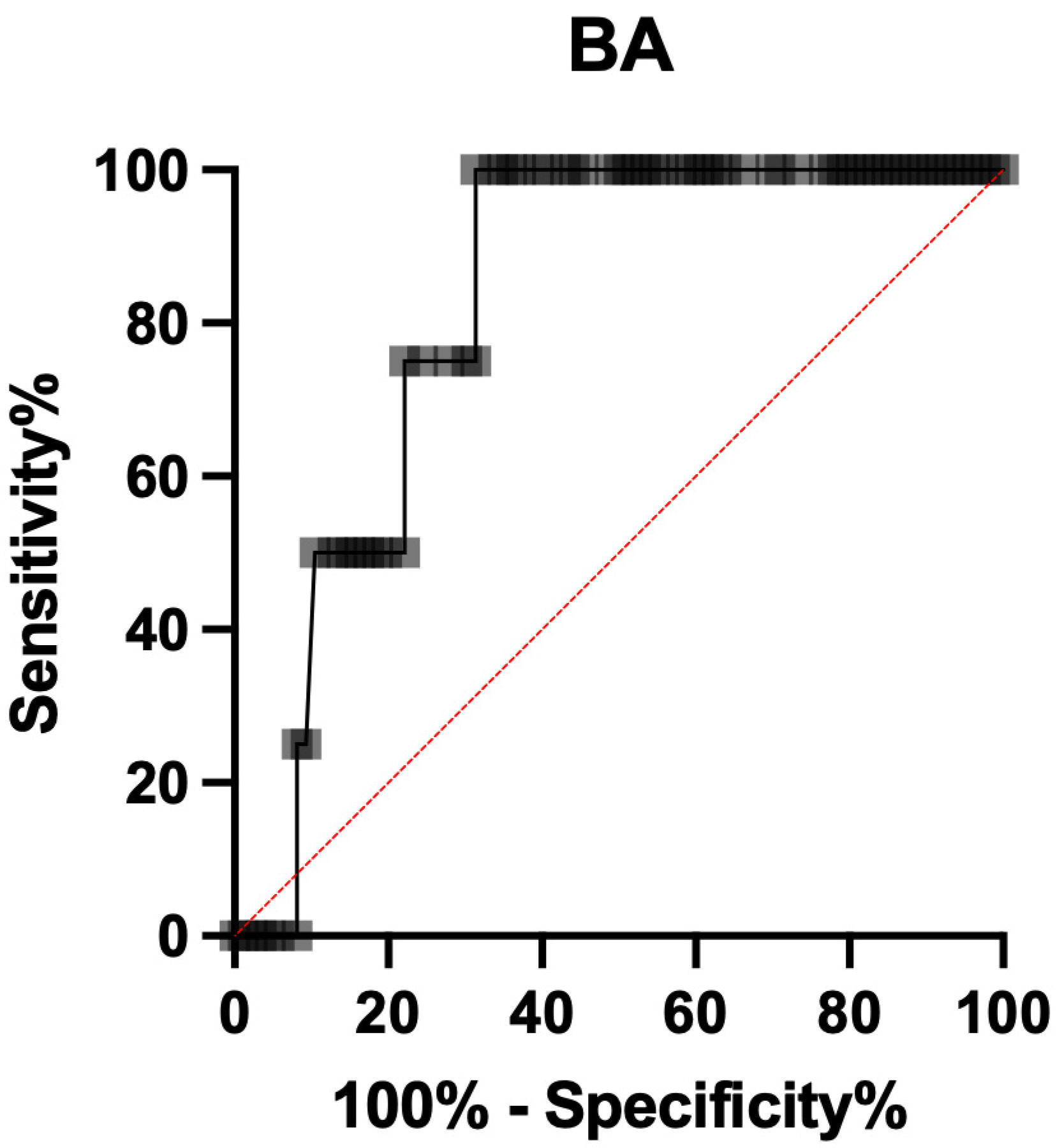
| Biacromial diameter, cm | 0.04 * | ||
| mean | 150.4 | 133.5 | |
| 95% CI | 133.2–167.6 | 130.1–137.0 | |
| BA/BPD, | 0.04 * | ||
| mean | 1.66 | 1.44 | |
| 95% CI | 1.46–1.86 | 1.41–1.48 | |
| BA/HC, | 0.01 * | ||
| mean | 0.45 | 0.39 | |
| 95% CI | 0.40–0.49 | 0.38–0.40 | |
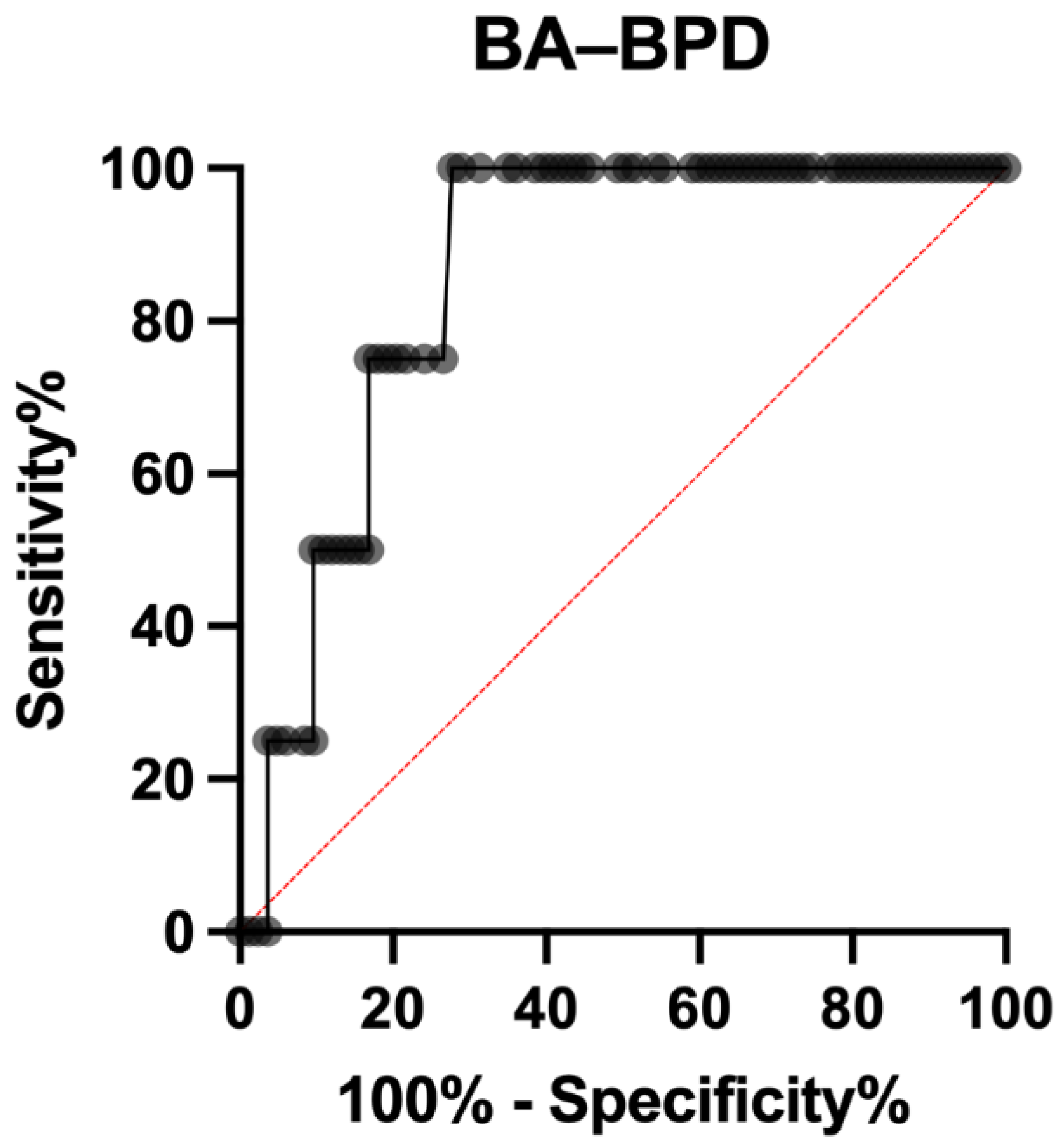
| BA–BPD, | 0.03 * | ||
| mean | 60.0 | 41.4 | |
| 95% CI | 42.4–77.6 | 38.2–44.6 | |
| Estimated fetal weight, g | 0.61 | ||
| Mean ± SD | 3273 ± 618 | 3448 ± 352 |
| Mode of Delivery Number (%) | Vaginal Cesarean Section Operative Delivery | 78 (86.67) 12 (13.33) 10 (11.11) |
|---|---|---|
| Apgar score, mean ± SD | 1′ 5′ | 8.2 ± 0.89 9.4 ± 0.54 |
| Birth weight, gr mean ± SD | 3426 ± 32 | |
| Birth length, cm mean ± SD | 51.32 ± 1.62 | |
| Cranial circumference, cm mean ± SD | 34.62 ± 1.12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
La Verde, M.; De Franciscis, P.; Torre, C.; Celardo, A.; Grassini, G.; Papa, R.; Cianci, S.; Capristo, C.; Morlando, M.; Riemma, G. Accuracy of Fetal Biacromial Diameter and Derived Ultrasonographic Parameters to Predict Shoulder Dystocia: A Prospective Observational Study. Int. J. Environ. Res. Public Health 2022, 19, 5747. https://doi.org/10.3390/ijerph19095747
La Verde M, De Franciscis P, Torre C, Celardo A, Grassini G, Papa R, Cianci S, Capristo C, Morlando M, Riemma G. Accuracy of Fetal Biacromial Diameter and Derived Ultrasonographic Parameters to Predict Shoulder Dystocia: A Prospective Observational Study. International Journal of Environmental Research and Public Health. 2022; 19(9):5747. https://doi.org/10.3390/ijerph19095747
Chicago/Turabian StyleLa Verde, Marco, Pasquale De Franciscis, Clelia Torre, Angela Celardo, Giulia Grassini, Rossella Papa, Stefano Cianci, Carlo Capristo, Maddalena Morlando, and Gaetano Riemma. 2022. "Accuracy of Fetal Biacromial Diameter and Derived Ultrasonographic Parameters to Predict Shoulder Dystocia: A Prospective Observational Study" International Journal of Environmental Research and Public Health 19, no. 9: 5747. https://doi.org/10.3390/ijerph19095747