
The Psychological Experience of COVID-19 Vaccination and Its Impact on the Willingness to Receive Booster Vaccines among the Chinese Population: Evidence from a National Cross-Sectional Study


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedures, Participants and Study Design
2.2. Assessments
2.3. Statistical Analysis
3. Results
3.1. COVID-19 Vaccination Psychological Experience Score Status
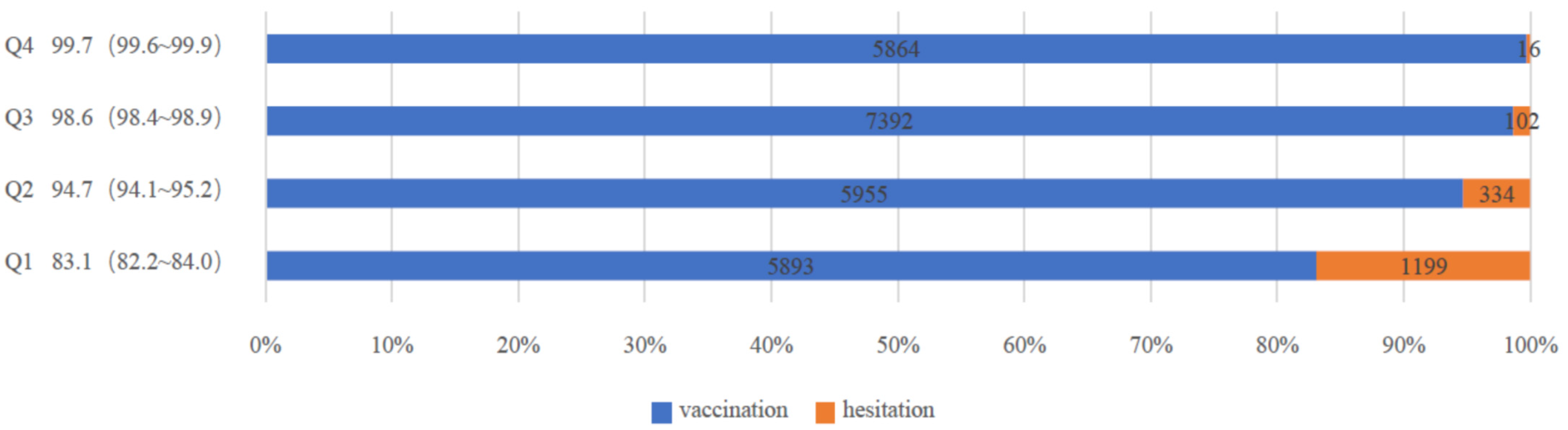
3.2. Prevalence of Willingness to Receive Booster Vaccines
3.3. Associations between Psychological Experience and Willingness to Receive Booster Vaccines
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Annemans, L.; Beutels, P.; Bloom, D.E.; De Backer, W.; Ethgen, O.; Luyten, J.; Van Wilder, P.; Willem, L.; Simoens, S. Economic Evaluation of Vaccines: Belgian Reflections on the Need for a Broader Perspective. Value Health 2021, 24, 105–111. [Google Scholar] [CrossRef] [PubMed]
- DeRoo, S.S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 Vaccination Program. JAMA J. Am. Med. Assoc. 2020, 323, 2458–2459. [Google Scholar] [CrossRef] [PubMed]
- Wan, X.; Huang, H.; Shang, J.; Xie, Z.; Jia, R.; Lu, G.; Chen, C. Willingness and influential factors of parents of 3-6-year-old children to vaccinate their children with the COVID-19 vaccine in China. Hum. Vaccines Immunother. 2021, 17, 3969–3974. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’; views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P.; Seror, V.; Cortaredona, S.; Launay, O.; Raude, J.; Verger, P.; Fressard, L.; Beck, F.; Legleye, S.; L’Haridon, O.; et al. A future vaccination campaign against COVID-19 at risk of vaccine hesitancy and politicisation. Lancet Infect. Dis. 2020, 20, 769–770. [Google Scholar] [CrossRef]
- Hurley, L.P.; Bridges, C.B.; Harpaz, R.; Allison, M.A.; O’Leary, S.T.; Crane, L.A.; Brtnikova, M.; Stokley, S.; Beaty, B.L.; Jimenez-Zambrano, A.; et al. U.S. physicians’ perspective of adult vaccine delivery. Ann. Intern. Med. 2014, 160, 161. [Google Scholar] [CrossRef] [Green Version]
- Tung, T.-H.; Lin, X.-Q.; Chen, Y.; Zhang, M.-X.; Zhu, J.-S. Willingness to receive a booster dose of inactivated coronavirus disease 2019 vaccine in Taizhou, China. Expert Rev. Vaccines 2021, 21, 261–267. [Google Scholar] [CrossRef]
- Rzymski, P.; Poniedziałek, B.; Fal, A. Willingness to Receive the Booster COVID-19 Vaccine Dose in Poland. Vaccines 2021, 9, 1286. [Google Scholar] [CrossRef]
- Landicho-Guevarra, J.; Reñosa, M.D.C.; Wachinger, J.; Endoma, V.; Aligato, M.F.; Bravo, T.A.; Landicho, J.; Bärnighausen, K.; McMahon, S. Scared, powerless, insulted and embarrassed: Hesitancy towards vaccines among caregivers in Cavite Province, the Philippines. BMJ Glob. Health 2021, 6, e006529. [Google Scholar] [CrossRef]
- Fisher, K.A.; Bloomstone, S.J.; Walder, J.; Crawford, S.; Fouayzi, H.; Mazor, K.M. Attitudes toward a potential SARS-CoV-2 vaccine: A survey of U.S. adults. Ann. Intern. Med. 2020, 173, 964–973. [Google Scholar] [CrossRef] [PubMed]
- McAteer, J.; Yildirim, I.; Chahroudi, A. The VACCINES Act: Deciphering Vaccine Hesitancy in the Time of COVID-19. Clin. Infect. Dis. 2020, 71, 703–705. [Google Scholar] [CrossRef] [PubMed]
- Guljaš, S.; Bosnić, Z.; Salha, T.; Berecki, M.; Dupan, Z.K.; Rudan, S.; Trtica, L.M. Lack of Informations about COVID-19 Vaccine: From Implications to Intervention for Supporting Public Health Communications in COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 6141. [Google Scholar] [CrossRef] [PubMed]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Palamenghi, L.; Barello, S.; Boccia, S.; Graffigna, G. Mistrust in biomedical research and vaccine hesitancy: The forefront challenge in the battle against COVID-19 in Italy. Eur. J. Epidemiol. 2020, 35, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, N.D.; Kwitel, A.; McCaul, K.D.; Magnan, R.E.; Gerrard, M.; Gibbons, F.X. Risk perceptions: Assessment and relationship to influenza vaccination. Health Psychol. 2007, 26, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 50, 1–15. [Google Scholar] [CrossRef]
- Temsah, M.-H.; Alhuzaimi, A.N.; Aljamaan, F.; Bahkali, F.; Al-Eyadhy, A.; Alrabiaah, A.; Alhaboob, A.; Bashiri, F.A.; Alshaer, A.; Temsah, O.; et al. Parental Attitudes and Hesitancy About COVID-19 vs. Routine Childhood Vaccinations: A National Survey. Front. Public Health 2021, 9, 752323. [Google Scholar] [CrossRef]
- Allington, D.; McAndrew, S.; Moxham-Hall, V.; Duffy, B. Coronavirus conspiracy suspicions, general vaccine attitudes, trust and coronavirus information source as predictors of vaccine hesitancy among UK residents during the COVID-19 pandemic. Psychol. Med. 2021, 51, 1–12. [Google Scholar] [CrossRef]
- Arane, K.; Behboudi, A.; Goldman, R.D. Virtual reality for pain and anxiety management in children. Can. Fam. Physician 2017, 63, 932–934. [Google Scholar]
- Sato, R.; Fintan, B. Fear, knowledge, and vaccination behaviors among women in Northern Nigeria. Hum. Vaccines Immunother. 2020, 16, 2438–2448. [Google Scholar] [CrossRef] [PubMed]
- Moccia, G.; Carpinelli, L.; Savarese, G.; Borrelli, A.; Boccia, G.; Motta, O.; Capunzo, M.; De Caro, F. Perception of Health, Mistrust, Anxiety, and Indecision in a Group of Italians Vaccinated against COVID-19. Vaccines 2021, 9, 612. [Google Scholar] [CrossRef] [PubMed]
- Disease Prevention and Control Bureau. 2022. Available online: http://www.nhc.gov.cn/xcs/yqfkdt/202201/8d493478365041eeb4d66c51bb7941ea.shtml (accessed on 19 January 2022).
- Wu, J.; Li, Q.; Tarimo, C.S.; Wang, M.; Gu, J.; Wei, W.; Ma, M.; Zhao, L.; Mu, Z.; Miao, Y. COVID-19 Vaccine Hesitancy Among Chinese Population: A Large-Scale National Study. Front. Immunol. 2021, 12, 4833. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Lambe, S.; Yu, L.-M.; Freeman, J.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Petit, A.; Vanderslott, S.; et al. Injection fears and COVID-19 vaccine hesitancy. Psychol. Med. 2021, 51, 1–11. [Google Scholar] [CrossRef] [PubMed]
- China, The National People’s Congress of the People’s Republic. The Law of the People’s Republic of China on Vaccine Management. 2019. Available online: http://www.npc.gov.cn/npc/c30834/201907/11447c85e05840b9b12c62b5b645fe9d.shtml (accessed on 13 October 2021).
- WHO. 2021. Available online: https://extranet.who.int/pqweb/sites/default/files/documents/Status_COVID_VAX_20Jan2021_v2.pdf (accessed on 15 October 2021).
- Guo, B.; Page, A.; Wang, H.; Taylor, R.; McIntyre, P. Systematic review of reporting rates of adverse events following immunization: An international comparison of post-marketing surveillance programs with reference to China. Vaccine 2013, 31, 603–617. [Google Scholar] [CrossRef]
- Wiley, K.E.; Massey, P.D.; Cooper, S.C.; Wood, N.J.; Ho, J.; Quinn, H.E.; Leask, J. Uptake of influenza vaccine by pregnant women: A cross-sectional survey. Med. J. Aust. 2013, 198, 373–375. [Google Scholar] [CrossRef] [Green Version]
- Kwok, K.O.; Li, K.K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Brewer, N.T.; Chapman, G.B.; Rothman, A.J.; Leask, J.; Kempe, A. Increasing Vaccination: Putting Psychological Science into Action. Psychol. Sci. Public Interest 2017, 18, 149–207. [Google Scholar] [CrossRef] [Green Version]
- French, J.; Deshpande, S.; Evans, W.; Obregon, R. Key Guidelines in Developing a Pre-Emptive COVID-19 Vaccination Uptake Promotion Strategy. Int. J. Environ. Res. Public Health 2020, 17, 5893. [Google Scholar] [CrossRef]
- Bernard, D.M.; Robbins, S.C.; McCaffery, K.J.; Scott, C.M.; Skinner, S.R. The domino effect: Adolescent girls’ response to human papillomavirus vaccination. Med. J. Aust. 2011, 194, 297–300. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Covariates | Total (%) | p-Value a | COVID-19 Vaccination Psychological Experience Score (Mean, 95% CI) | p-Value a | The Willingness to Uptake Booster Vaccines (95% CI) | p-Value a |
|---|---|---|---|---|---|---|
| Total participants | 26,755 (100) | 25.83 (25.78~25.89) | 93.83 (93.54~94.12) b | |||
| Demographic characteristics | ||||||
| Age (years) | <0.001 | <0.001 | <0.001 | |||
| 18–29 | 11,694 (43.7) | 25.22 (25.14~25.29) | 91.59 (91.08~92.09) b | |||
| 30–39 | 10,735 (40.1) | 26.29 (26.21~26.37) | 95.61 (95.22~96.00) b | |||
| 40–49 | 3044 (11.4) | 26.49 (26.34~26.63) | 96.16 (95.47~96.84) b | |||
| 50–59 | 1036 (3.9) | 26.20 (25.97~26.44) | 94.40 (93.00~95.80) b | |||
| 60– | 246 (0.9) | 25.71 (25.18~26.24) | 91.46 (87.95~94.98) b | |||
| Sex | <0.001 | <0.001 | <0.001 | |||
| Men | 12,685 (47.4) | 25.59 (25.51~25.66) | 92.52 (92.06~92.98) b | |||
| Women | 14,070 (52.6) | 26.06 (25.99~26.13) | 95.01 (94.65~95.37) b | |||
| Educational status | <0.001 | <0.001 | <0.001 | |||
| Below high school | 2948 (11.0) | 24.61 (24.45~24.78) | 87.65 (86.46~88.84) b | |||
| High school graduate | 7032 (26.3) | 26.11 (26.00~26.21) | 95.39 (94.90~95.88) b | |||
| University graduate | 16,775 (62.7) | 25.93 (25.87~26.00) | 94.26 (93.91~94.61) b | |||
| Ethnic groups | <0.001 | <0.001 | <0.001 | |||
| Han | 25,741 (96.2) | 25.88 (25.82~25.93) | 94.12 (93.83~94.41) b | |||
| Minority | 1014 (3.8) | 24.78 (24.50~25.07) | 86.39 (84.28~88.50) b | |||
| Religion | <0.001 | <0.001 | <0.001 | |||
| Atheist | 23,228 (86.8) | 25.97 (25.92~26.03) | 94.45 (94.15~94.74) b | |||
| Others | 3527 (13.2) | 24.90 (24.75~25.06) | 89.76 (88.76~90.77) b | |||
| Marital status | <0.001 | <0.001 | <0.001 | |||
| Married | 16,666 (62.3) | 26.37 (26.30~26.43) | 95.49 (95.18~95.81) b | |||
| Others | 10,089 (37.7) | 24.95 (24.87~25.04) | 91.08 (90.52~91.64) b | |||
| Subjective social status | ||||||
| Society level | 7.64 ± 2.092 | <0.001 | 7.66 ± 2.09 c | <0.001 | ||
| Community level | 7.98 ± 2.13 | <0.001 | 8.00 ± 2.12 c | <0.001 | ||
| EQ-5D | 85.26 ± 13.64 | <0.001 | 85.71 ± 13.26 c | <0.001 | ||
| Chronic condition | <0.001 | <0.001 | <0.001 | |||
| Yes | 3251 (12.2) | 24.39 (24.23~24.54) | 87.63 (86.50~88.77) b | |||
| No | 23,504 (87.8) | 26.03 (25.98~26.09) | 94.69 (94.40~94.97) b | |||
| Smoking status | <0.001 | <0.001 | <0.001 | |||
| Current smoker | 7763 (29.0) | 24.28 (24.18~24.38) | 89.63 (88.95~90.31) b | |||
| Former smoker | 1482 (5.5) | 26.70 (26.47~26.92) | 94.33 (93.15~95.51) b | |||
| Never smoker | 17,510 (65.4) | 26.70 (26.47~26.92) | 95.65 (95.35~95.95) b | |||
| Drinking status | <0.001 | <0.001 | <0.001 | |||
| Current drinker | 16,122 (60.3) | 25.25 (25.19~25.32) | 92.28 (91.87~92.70) b | |||
| Former drinker | 930 (3.5) | 26.38 (26.09~26.67) | 94.19 (92.69~95.70) b | |||
| Never drinker | 9703 (36.3) | 26.74 (26.66~26.83) | 96.36 (95.99~96.73) b | |||
| Health behaviors | ||||||
| Washing hands | <0.001 | <0.001 | <0.001 | |||
| Increased | 23,491 (87.8) | 26.14 (26.09~26.20) | 95.26 (94.99~95.53) b | |||
| Unchanged | 2919 (10.9) | 23.70 (23.56~23.83) | 84.14 (82.81~85.46) b | |||
| Decreased | 345 (1.3) | 22.84 (22.43~23.26) | 78.55 (74.20~82.90) b | |||
| Wearing mask | <0.001 | <0.001 | <0.001 | |||
| Increased | 25,051 (93.6) | 26.05 (25.99~26.10) | 94.99 (94.72~95.26) b | |||
| Unchanged | 1323 (4.9) | 22.71 (22.50~22.92) | 77.40 (75.14~79.66) b | |||
| Decreased | 381 (1.4) | 22.64 (22.24~23.04) | 74.28 (69.87~78.69) b | |||
| Gathering activities | <0.001 | <0.001 | <0.001 | |||
| Increased | 7116 (26.6) | 25.01 (24.90~25.12) | 92.45 (91.84~93.07) b | |||
| Unchanged | 2428 (9.1) | 23.44 (23.29~23.59) | 83.28 (81.79~84.76) b | |||
| Decreased | 17,211 (64.3) | 26.51 (26.45~26.57) | 95.89 (95.59~96.18) b | |||
| COVID-19 conspiracy beliefs | <0.001 | <0.001 | <0.001 | |||
| Level 1 | 2393 (8.9) | 25.61 (25.45~25.77) | 93.44 (92.45~94.43) b | |||
| Level 2 | 10,479 (39.2) | 27.34 (27.26~27.42) | 97.21 (96.90~97.53) b | |||
| Level 3 | 6812 (25.5) | 25.28 (25.19~25.38) | 93.35 (92.76~93.94) b | |||
| Level 4 | 7071 (26.4) | 24.21 (24.10~24.31) | 89.41 (88.69~90.12) b | |||
| Risk of COVID-19 infection | <0.001 | <0.001 | <0.001 | |||
| Very high | 1886 (7.0) | 24.10 (23.87~24.32) | 93.48 (92.36~94.59) b | |||
| High | 1895 (7.1) | 23.57 (23.37~23.77) | 86.12 (84.56~87.68) b | |||
| Medium | 3889 (14.5) | 24.83 (24.70~24.96) | 90.69 (89.78~91.61) b | |||
| Low | 14,080 (52.6) | 26.32 (26.26~26.39) | 95.62 (95.28~95.96) b | |||
| No | 4195 (15.7) | 27.23 (27.09~27.36) | 96.09 (95.50~96.68) b | |||
| Not sure | 810 (3.0) | 24.25 (23.99~24.51) | 84.94 (82.47~87.41) b | |||
| Curability of COVID-19 | <0.001 | <0.001 | <0.001 | |||
| Very high | 11,892 (44.4) | 27.03 (26.95~27.11) | 96.84 (96.52~97.15) b | |||
| High | 9811 (36.7) | 25.17 (25.09~25.24) | 93.48 (92.99~93.97) b | |||
| Medium | 2803 (10.5) | 23.74 (23.59~23.88) | 86.73 (85.47~87.99) b | |||
| Low | 1205 (4.5) | 25.08 (24.84~25.32) | 89.46 (87.72~91.20) b | |||
| No | 427 (1.6) | 26.62 (26.14~27.10) | 93.68 (91.36~95.99) b | |||
| Not sure | 617 (2.3) | 23.93 (23.64~24.22) | 82.33 (79.32~85.35) b | |||
| Vaccine adverse reactions | <0.001 | <0.001 | <0.001 | |||
| Yes | 5079 (19.0) | 23.61 (23.49~23.73) | 91.06 (90.28~91.85) b | |||
| No/Unclear | 21,676 (81.0) | 26.35 (26.30~26.41) | 94.48 (94.17~94.78) b | |||
| Channel of vaccine information | <0.001 | <0.001 | ||||
| Community worker | 7872 (29.4) | 26.55 (26.45~26.66) | <0.001 | 96.00 (95.57~96.43) b | ||
| Internet | 13,921 (52.0) | 25.67 (25.60~25.74) | 93.98 (93.59~94.38) b | |||
| Others | 4962 (18.5) | 25.15 (25.03~25.27) | 89.96 (89.13~90.80) b | |||
| Vaccine conspiracy beliefs | <0.001 | <0.001 | <0.001 | |||
| Level 1 | 1874 (7.0) | 25.00 (24.82~25.18) | 91.78 (90.54~93.03) b | |||
| Level 2 | 11,357 (42.4) | 27.97 (27.90~28.05) | 98.00 (97.74~98.26) b | |||
| Level 3 | 6265 (23.4) | 25.43 (25.35~25.51) | 96.15 (95.68~96.63) b | |||
| Level 4 | 7259 (27.1) | 23.05 (22.97~23.14) | 85.82 (85.02~86.63) b | |||
| Convenience of vaccination | <0.001 | <0.001 | <0.001 | |||
| High | 25,5559 (95.5) | 25.97 (25.92~26.02) | 94.50 (94.22~94.78) b | |||
| Medium | 969 (3.6) | 22.96 (22.75~23.18) | 79.67 (77.13~82.21) b | |||
| Low | 227 (0.8) | 22.85 (22.33~23.37) | 78.85 (73.50~84.21) b | |||
| Trust in doctors | <0.001 | <0.001 | <0.001 | |||
| Level 1 | 7033 (26.3) | 23.16 (23.07~23.25) | 85.58 (84.76~86.40) b | |||
| Level 2 | 7979 (29.8) | 25.04 (24.96~25.12) | 94.30 (93.79~94.81) b | |||
| Level 3 | 5159 (19.3) | 27.15 (27.05~27.26) | 97.81 (97.41~98.21) b | |||
| Level 4 | 6584 (24.6) | 28.61 (28.52~28.71) | 98.95 (98.71~99.20) b | |||
| Trust in developers | <0.001 | <0.001 | <0.001 | |||
| Level 1 | 7580 (28.3) | 23.23 (23.14~23.32) | 85.34 (84.55~86.14) b | |||
| Level 2 | 7930 (29.6) | 25.21 (25.13~25.29) | 95.44 (94.98~95.89) b | |||
| Level 3 | 11,245 (42.0) | 28.03 (27.95~28.10) | 98.42 (98.19~98.65) b | |||
| Model | Number of Surveys | Tendency to Hesitate Rate (%, 95%CI) | Unadjusted Variable | Adjusted Variable | |||
|---|---|---|---|---|---|---|---|
| OR | 95%CI | OR | 95%CI | ||||
| Negative psychological experience model | Q1 | 7169 | 16.1 (15.3~17.0) | 1.000 | 1.000 | ||
| Q2 | 9060 | 4.1 (3.7~4.5) | 4.495 | 3.981~5.075 | 2.474 | 2.154~2.843 | |
| Q3 | 4560 | 1.9 (1.5~2.3) | 10.012 | 8.015~12.506 | 3.935 | 3.093~5.006 | |
| Q4 | 5966 | 0.6 (0.4~0.8) | 31.701 | 22.708~44.255 | 8.871 | 6.240~12.612 | |
| Positive psychological experience model | Q1 | 1,0750 | 9.6 (9.0~10.1) | 1.000 | 1.000 | ||
| Q2 | 3822 | 5.3 (4.6~6.1) | 1.885 | 1.615~2.201 | 1.931 | 1.630~2.288 | |
| Q3 | 6919 | 4.2 (3.7~4.6) | 2.439 | 2.133~2.789 | 2.460 | 2.111~2.867 | |
| Q4 | 5264 | 2.4 (2.0~2.8) | 4.371 | 3.619~5.278 | 3.933 | 3.176~4.871 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miao, Y.; Li, Y.; Zhang, W.; Wu, J.; Gu, J.; Wang, M.; Wei, W.; Ye, B.; Miao, C.; Tarimo, C.S.; et al. The Psychological Experience of COVID-19 Vaccination and Its Impact on the Willingness to Receive Booster Vaccines among the Chinese Population: Evidence from a National Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 5464. https://doi.org/10.3390/ijerph19095464
Miao Y, Li Y, Zhang W, Wu J, Gu J, Wang M, Wei W, Ye B, Miao C, Tarimo CS, et al. The Psychological Experience of COVID-19 Vaccination and Its Impact on the Willingness to Receive Booster Vaccines among the Chinese Population: Evidence from a National Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(9):5464. https://doi.org/10.3390/ijerph19095464
Chicago/Turabian StyleMiao, Yudong, Yi Li, Wanliang Zhang, Jian Wu, Jianqin Gu, Meiyun Wang, Wei Wei, Beizhu Ye, Chengyuan Miao, Clifford Silver Tarimo, and et al. 2022. "The Psychological Experience of COVID-19 Vaccination and Its Impact on the Willingness to Receive Booster Vaccines among the Chinese Population: Evidence from a National Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 9: 5464. https://doi.org/10.3390/ijerph19095464