
Effects of Nursing Diabetes Self-Management Education on Glycemic Control and Self-Care in Type 1 Diabetes: Study Protocol

 , , and
, , and 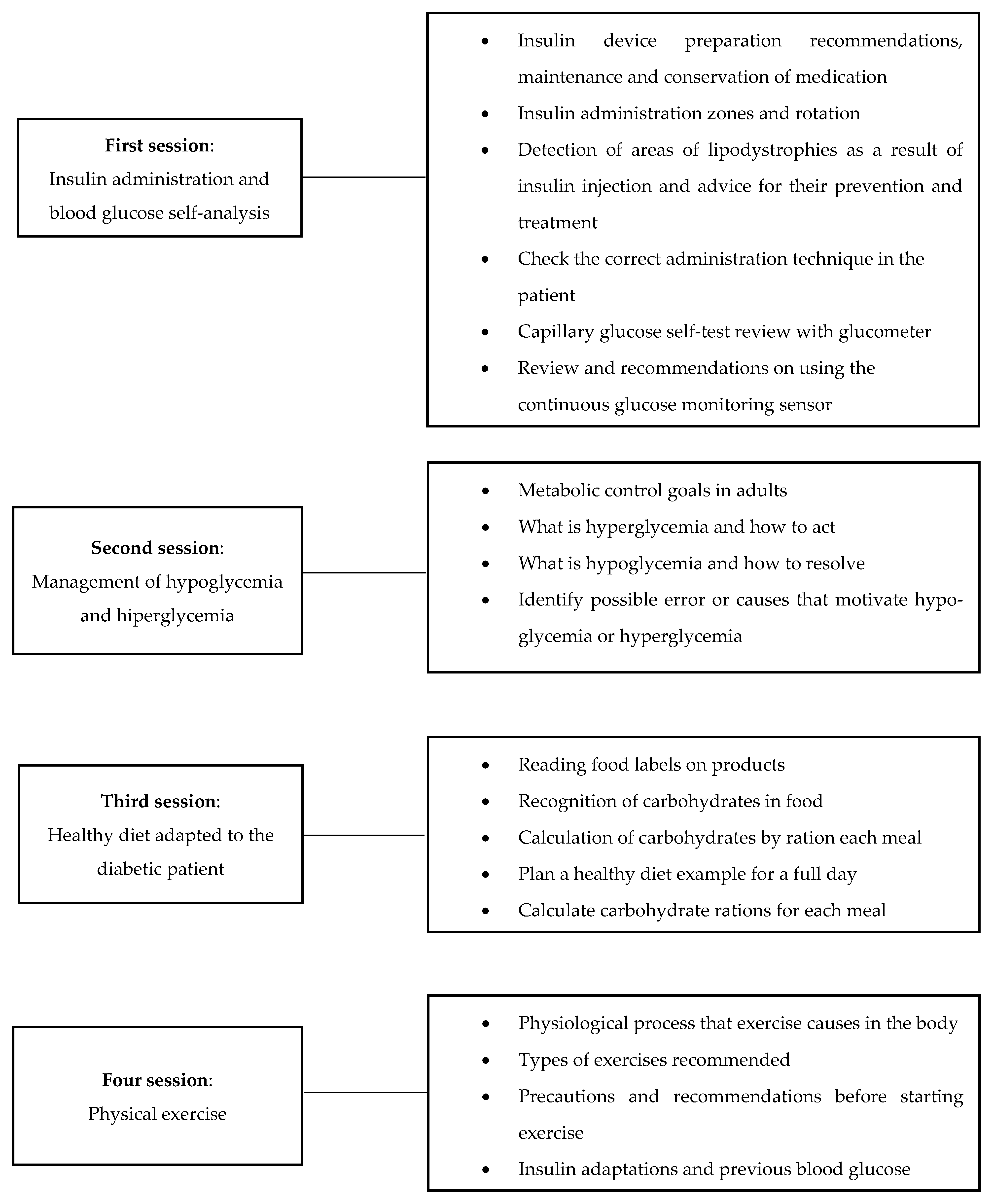{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Population and Sample
2.3. Eligibility Criteria
2.3.1. Inclusion Criteria
- Adults over the age of 18 years.
- Diagnosed with type 1 diabetes.
- Able to speak, read and understand Spanish.
2.3.2. Exclusion Criteria
- Have a terminal illness.
- Have at least one of the following clinical conditions or pathologies: brain injury of traumatic or hemorrhagic origin, dementia or serious mental illness such as schizophrenia.
- Have reading and hearing difficulties.
2.4. Intervention
2.4.1. Diabetes Education Program
2.4.2. Usual Care
2.5. Data Collection
2.5.1. Blood Glucose Levels According to Continuous Glucose Monitoring Sensor
2.5.2. General Knowledge about Diabetes Management
2.5.3. Clarke Test
2.5.4. Diabetes Self-Care Activities Scale
2.5.5. Goldberg Anxiety and Depression Scale
2.6. Data Analysis
2.7. Ethical Considerations
3. Discussion
Limitations
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Freeborn, D.; Dyches, T.; Roper, S.O. Lessons learned from a life with type 1 diabetes: Adult perspectives. Diabetes Spectr. 2017, 30, 188–194. [Google Scholar] [CrossRef] [Green Version]
- Alenazi, F.; Peddle, M.; Bressington, D.; Mahzari, M.; Gray, R. A study protocol for a feasibility trial of telephone-delivered Adherence Therapy for adults with type 2 diabetes. Nurs. Open 2021, 8, 1510–1519. [Google Scholar] [CrossRef] [PubMed]
- Nathan, D.M.; Cleary, P.A.; Backlund, J.Y.; Genuth, S.M.; Lachin, J.M.; Orchard, T.J.; Raskin, P.; Zinman, B. Diabetes control and complications trial/epidemiology of diabetes interventions and complications (DCCT/EDIC) Study research group. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N. Engl. J. Med. 2005, 353, 2643–2653. [Google Scholar] [CrossRef]
- Rising, K.L.; Kemp, M.; Davidson, P.; Hollander, J.E.; Jabbour, S.; Jutkowitz, E.; Leiby, B.E.; Marco, C.; McElwee, I.; Mills, G.; et al. Assessing the impact of medically tailored meals and medical nutrition therapy on type 2 diabetes: Protocol for Project MiNT. Contemp. Clin. Trials 2021, 108, 106511. [Google Scholar] [CrossRef] [PubMed]
- Amazi, G.; Lam Soh, K.; Sazlina, S.G.; Salmiah, S.; Aazami, S.; Mozafari, M.; Taghinejad, H. Effect of a nurse-led diabetes self-management education program on glycosylated hemoglobin among adults with type 2 diabetes. J. Diabetes Res. 2018, 2018, 4930157. [Google Scholar] [CrossRef]
- American Diabetes Association. Foundations of care: Education, nutrition, physical activity, smoking cessation, psychosocial care, and immunization. Diabetes Care 2015, 38 (Suppl. S1), S20–S30. [Google Scholar] [CrossRef] [Green Version]
- Garber, A.J.; Abrahamson, M.J.; Barzilay, J.I.; Blonde, L.; Bloomgarden, Z.; Bush, M.A.; Dagogo-Jack, S.; Davidson, M.B.; Einhorn, D.; Garvey, W.; et al. AACE comprehensive diabetes management algorithm 2013. Endocr. Pract. 2013, 19, 327–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hass, L.; Maryniuk, M.; Beck, J.; Cox, C.E.; Duker, P.; Edwards, L.; Fisher, E.; Hanson, L.; Kent, D.; Kolb, L.; et al. National standards for diabetes self-management education and support. Diabetes Educ. 2012, 38, 619–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urbanski, P.; Wolf, A.; Herman, W.H. Cost-effectiveness of diabetes education. J. Am. Diet. Assoc. 2008, 108 (Suppl. S1), S6–S11. [Google Scholar] [CrossRef] [PubMed]
- Rosal, M.C.; Ockene, I.S.; Restrepo, A.; White, M.J.; Borg, A.; Olendzki, B.; Scavron, J.; Candib, L.; Welch, G.; Reed, G. Randomized trial of a literacy-sensitive, culturally tailored diabetes self-management intervention for low-income latinos. Diabetes Care 2011, 34, 838–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, J.G.; Jennings, T.; Vittoria, I.; Fedders, M. Short and long-term outcomes from a multisession diabetes education program targeting low-income minority patients: A six-month follow up. Clin. Ther. 2013, 35, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Tang, P.C.; Overhage, J.M.; Chan, A.S.; Brown, N.L.; Aghighi, B.; Entwistle, M.P.; Hui, S.L.; Hyde, S.M.; Klieman, L.H.; Mitchell, C.J.; et al. Online disease management of diabetes: Engaging and motivating patients online with enhanced resources-diabetes (EMPOWER-D), a randomized controlled trial. J. Am. Med. Inform. Assoc. 2013, 20, 526–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, J.; Whittemore, R.; He, G. The relationship between diabetes self-management and metabolic control in youth with type 1 diabetes: An integrative review. J. Adv. Nurs. 2011, 67, 2294–2310. [Google Scholar] [CrossRef]
- Ong, W.M.; Chua, S.S.; Jenn, C. Barriers and facilitators to self-monitoring of blood glucose in people with type 2 diabetes using insulin: A qualitative study. Patient Prefer. Adherence 2014, 8, 237–246. [Google Scholar] [CrossRef] [Green Version]
- Paris, I.; Henry, C.; Pirard, F.; Gérard, A.; Colin, I.M. The new FreeStyle libre flash glucose monitoring system improves the glycaemic control in a cohort of people with type 1 diabetes followed in real-life conditions over a period of one year. Endocrinol. Diabetes Metab. 2018, 1, e00023. [Google Scholar] [CrossRef] [PubMed]
- Landau, Z.; Abiri, S.; Gruber, N.; Levy-Shraga, Y.; Brener, A.; Lebenthal, Y.; Barash, G.; Pinhas-Hamiel, O.; Rachmiel, M. Use of flash glucose-sensing technology (FreeStyle Libre) in youth with type 1 diabetes: AWeSoMe study group real-life observational experience. Acta Diabetol. 2018, 55, 1303–1310. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Seah, B.; Jiang, Y.; Lopez, V.; Tan, C.; Lim, S.T.; Ren, H.; Khoo, Y.H. A randomized controlled trial on a nurse-led smartphone-based self-management programme for people with poorly controlled type 2 diabetes: A study protocol. J. Adv. Nurs. 2018, 74, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Clarke, W.L.; Cox, D.J.; Gonder-Frederick, L.A.; Julian, D.; Schlundt, D.; Polonsky, W. Reduced awareness of hypoglycemia in adults with IDDM. A prospective study of hypoglycemic frequency and associated symptoms. Diabetes Care 1995, 18, 517–522. [Google Scholar] [CrossRef]
- Jansà, M.; Quirós, C.; Giménez, M.; Vidal, M.; Galindo, M.; Conget, I. Análisis psicométrico de las versions en lengua castellana y catalana de un cuestionario de percepción de la hipoglucemia. Med. Clín. 2015, 144, 440–444. [Google Scholar] [CrossRef]
- Caro-Bautista, J.; Morilla-Herrera, J.C.; Villa-Estrada, F.; Cuevas-Fernández-Gallego, M.; Lupiáñez-Pérez, I.; Morales-Asencio, J.M. Adaptación cultural al español y validación psicométrica del Summary of Diabetes Self-Care Activities measure (SDSCA) en personas con diabetes mellitus tipo 2. Atención Primaria 2016, 48, 458–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reivan-Ortiz, G.; Pineda-García, G.; León-Parias, B.D. Psychometric Properties of the Goldberg Anxiety and Depression Scale (GADS) in ecuatorian population. Int. J. Psychol. Res. 2019, 12, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Lamers, F.; Jonkers, C.; Bosma, H.; Knottnerus, J.A.; van Eijk, J. Treating depression in diabetes patients: Does a nurse-administered minimal psychological intervention affect diabetes-specific quality of life and glycaemic control? A randomized controlled trial. J. Adv. Nurs. 2011, 67, 788–799. [Google Scholar] [CrossRef] [PubMed]
- Lamers, F.; Jonkers, C.; Bosma, H.; Kempen, G.I.J.M.; Meijer, J.A.M.J.; Penninx, B.; Knottnerus, J.A.; van Eijk, J. A minimal psychological intervention in chronically ill elderly patients with depression: A randomized trial. Psychother. Psychosom. 2010, 79, 217–226. [Google Scholar] [CrossRef]
- Pandit, A.U.; Bailey, S.C.; Curtis, L.M.; Seligman, H.K.; Davis, T.C.; Parker, R.M.; Schillinger, D.; DeWalt, D.; Fleming, D.; Mohr, D.C.; et al. Disease-related distress, self-care and clinical outcomes among low-income patients with diabetes. J. Epidemiol. Commun. Health 2014, 68, 557–564. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.H.; Hsu, H.C.; Kao, C.C.; Yang, Y.M.; Lee, Y.J.; Shin, S.J. Associations of changes in psychosocial factors and their interactions with diabetes distress in patients with type 2 diabetes: A longitudinal study. J. Adv. Nurs. 2016, 73, 1137–1146. [Google Scholar] [CrossRef]
- Martyn-Nemeth, P.; Phillips, S.A.; Mihailescu, D.; Farabi, S.S.; Park, C.; Lipton, R.; Idemudia, E.; Quinn, E. Poor sleep quality is associated with nocturnal glycaemic variability and fear of hypoglycaemia in adults with type 1 diabetes. J. Adv. Nurs. 2017, 74, 2373–2380. [Google Scholar] [CrossRef]
- Reutrakul, S.; Thakkinstian, A.; Anothaisintawee, T.; Chontong, S.; Borel, A.L.; Perfect, M.M.; Knutson, K.L. Sleep characteristics in type 1 diabetes and associations with glycemic control. Systematic review and meta-anlysis. Sleep Med. 2016, 23, 26–45. [Google Scholar] [CrossRef] [Green Version]
- Yoon, J.E.; Sunwoo, J.S.; Kim, J.S.; Roh, H.; Ahn, M.Y.; Woo, H.Y.; Lee, K.B. Poststroke glycemic variability increased recurrent cardiovascular events in diabetic patients. J. Diabetes Its Complicat. 2016, 31, 390–394. [Google Scholar] [CrossRef]
- American Diabetes Association. Standards of medical care in diabetes-2018. Diabetes Care 2018, 41 (Suppl. S1), S73–S74. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romero-Castillo, R.; Pabón-Carrasco, M.; Jiménez-Picón, N.; Ponce-Blandón, J.A. Effects of Nursing Diabetes Self-Management Education on Glycemic Control and Self-Care in Type 1 Diabetes: Study Protocol. Int. J. Environ. Res. Public Health 2022, 19, 5079. https://doi.org/10.3390/ijerph19095079
Romero-Castillo R, Pabón-Carrasco M, Jiménez-Picón N, Ponce-Blandón JA. Effects of Nursing Diabetes Self-Management Education on Glycemic Control and Self-Care in Type 1 Diabetes: Study Protocol. International Journal of Environmental Research and Public Health. 2022; 19(9):5079. https://doi.org/10.3390/ijerph19095079
Chicago/Turabian StyleRomero-Castillo, Rocío, Manuel Pabón-Carrasco, Nerea Jiménez-Picón, and José Antonio Ponce-Blandón. 2022. "Effects of Nursing Diabetes Self-Management Education on Glycemic Control and Self-Care in Type 1 Diabetes: Study Protocol" International Journal of Environmental Research and Public Health 19, no. 9: 5079. https://doi.org/10.3390/ijerph19095079