
Sleep Quality, Insomnia, Anxiety, Fatigue, Stress, Memory and Active Coping during the COVID-19 Pandemic

 ,
,  ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
2.2. Power Calculation
3. Results
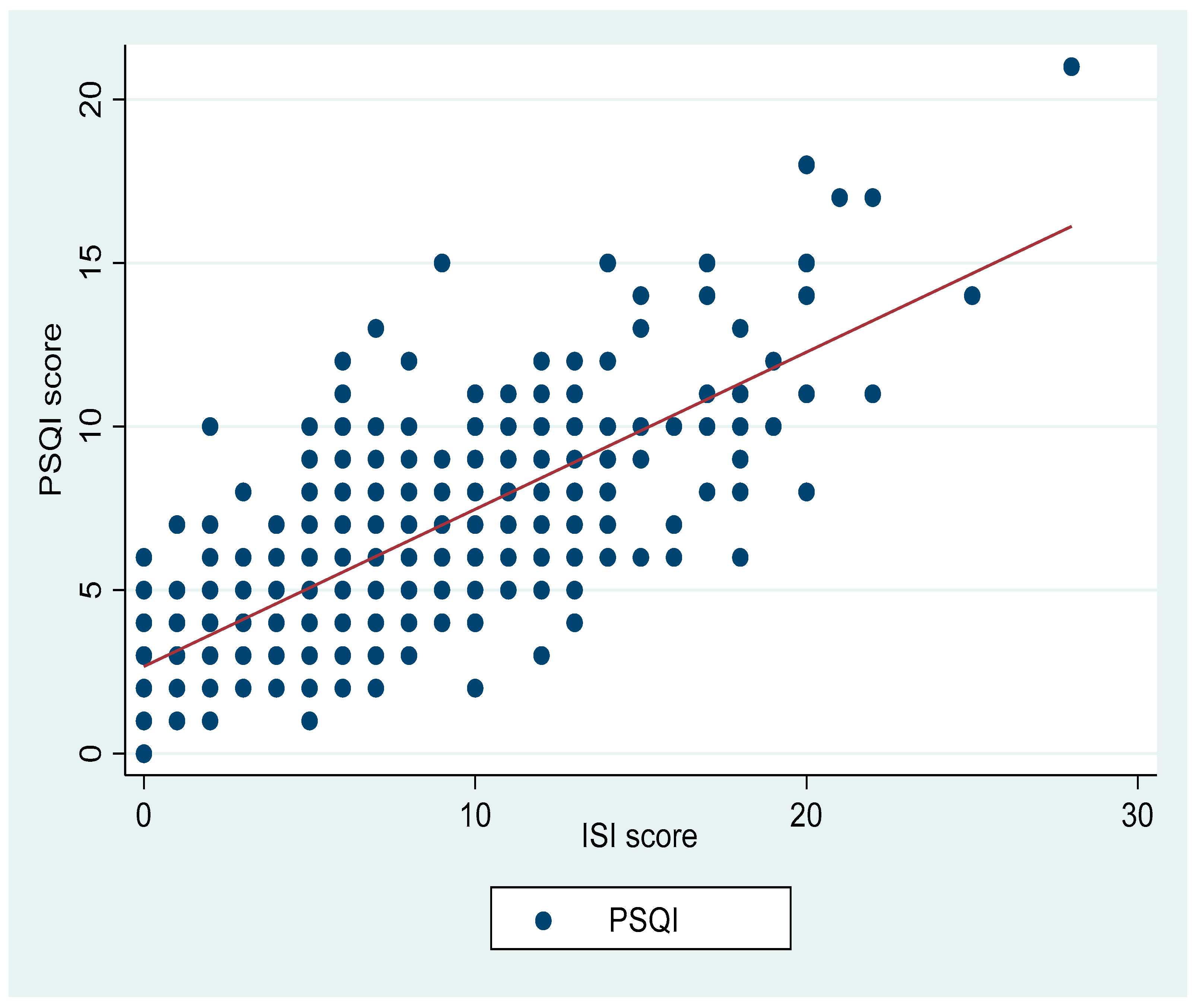
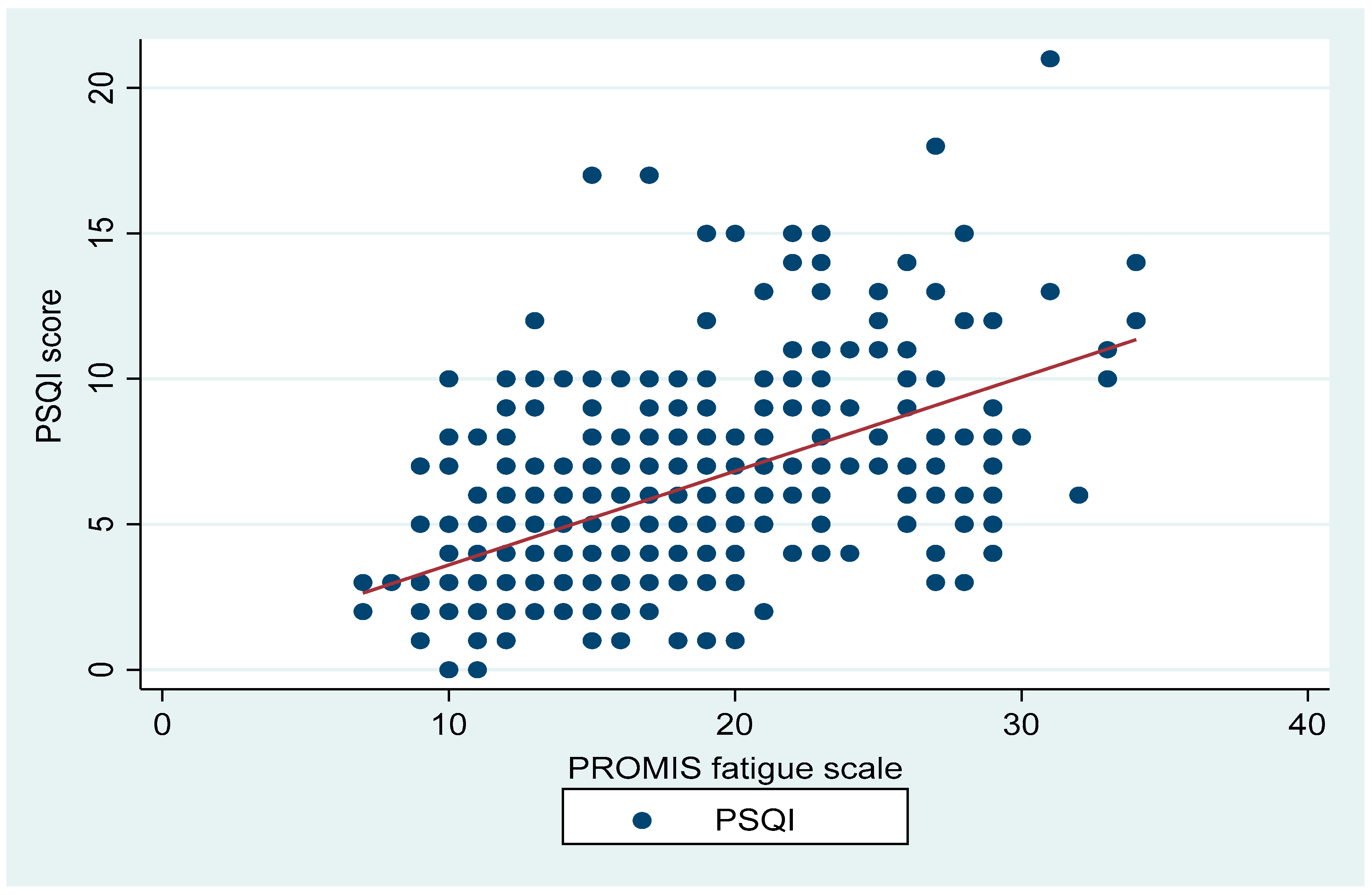
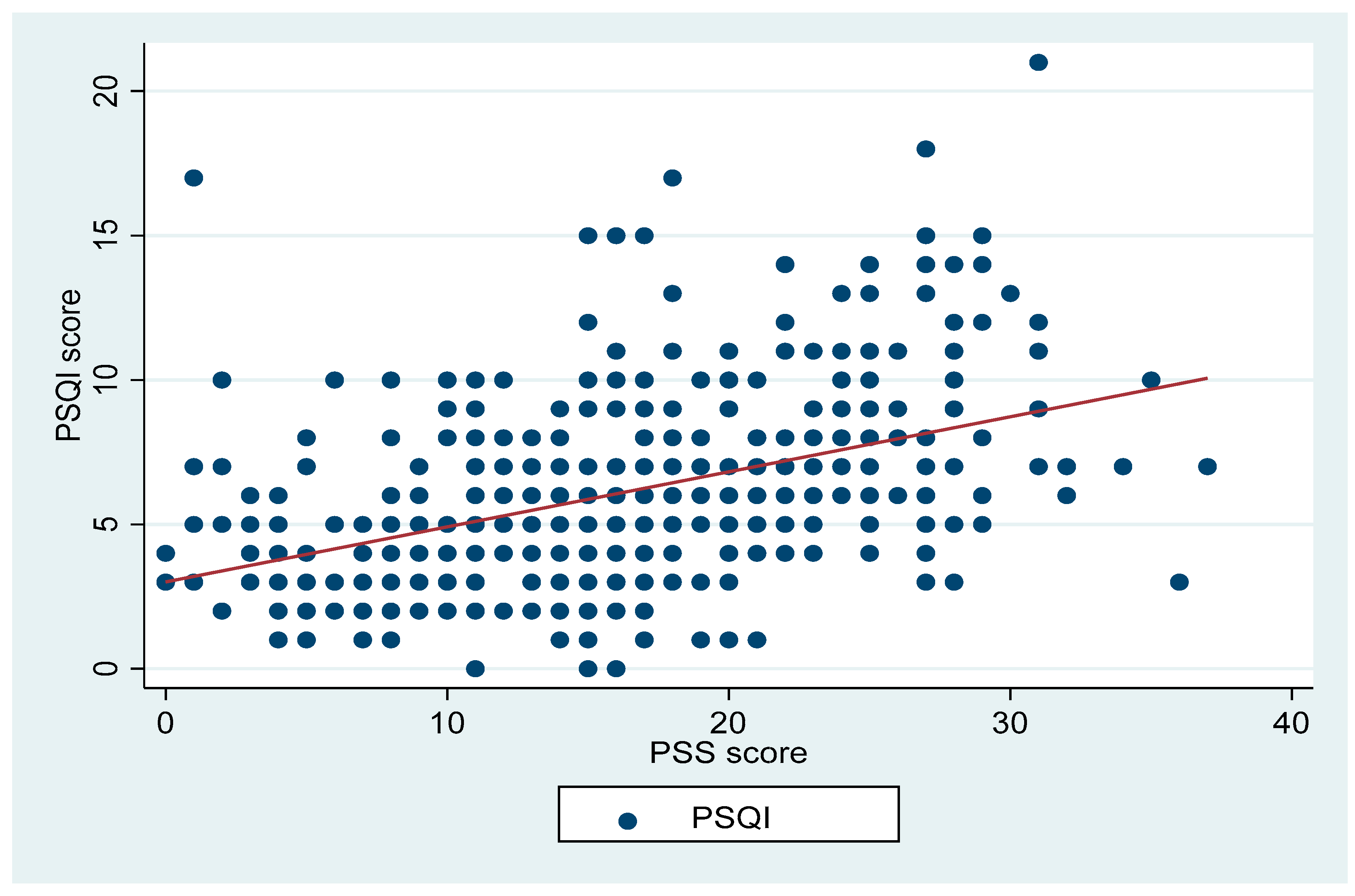
3.1. Correlations between PSQI and Other Parameters
3.2. Associations of PSQI with Other Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ciotti, M.; Ciccozzi, M.; Terrinoni, A.; Jiang, W.C.; Wang, C.B.; Bernardini, S. The COVID-19 pandemic. Crit. Rev. Clin. Lab. Sci. 2020, 57, 365–388. [Google Scholar] [CrossRef] [PubMed]
- Lythgoe, M.P.; Middleton, P. Ongoing Clinical Trials for the Management of the COVID-19 Pandemic. Trends Pharmacol. Sci. 2020, 41, 363–382. [Google Scholar] [CrossRef]
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427. [Google Scholar] [CrossRef] [PubMed]
- Cullen, W.; Gulati, G.; Kelly, B.D. Mental health in the COVID-19 pandemic. QJM 2020, 113, 311–312. [Google Scholar] [CrossRef]
- Kola, L. Global mental health and COVID-19. Lancet Psychiatry 2020, 7, 655–657. [Google Scholar] [CrossRef]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Abuhamdah, S.M.A.; Naser, A.Y.; Abdelwahab, G.M.; AlQatawneh, A. The Prevalence of Mental Distress and Social Support among University Students in Jordan: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 11622. [Google Scholar] [CrossRef]
- Alyami, H.S.; Naser, A.Y.; Dahmash, E.Z.; Alyami, M.H.; Alyami, M.S. Depression and anxiety during the COVID-19 pandemic in Saudi Arabia: A cross-sectional study. Int. J. Clin. Pract. 2021, 75, e14244. [Google Scholar] [CrossRef]
- Naser, A.Y.; Dahmash, E.Z.; Al-Rousan, R.; Alwafi, H.; Alrawashdeh, H.M.; Ghoul, I.; Abidine, A.; Bokhary, M.A.; Al-Hadithi, H.T.; Ali, D.; et al. Mental health status of the general population, healthcare professionals, and university students during 2019 coronavirus disease outbreak in Jordan: A cross-sectional study. Brain Behav. 2020, 10, e01730. [Google Scholar] [CrossRef] [PubMed]
- Varghese, A.; George, G.; Kondaguli, S.V.; Naser, A.Y.; Khakha, D.C.; Chatterji, R. Decline in the mental health of nurses across the globe during COVID-19: A systematic review and meta-analysis. J. Glob. Health 2021, 11, 05009. [Google Scholar] [CrossRef]
- Joffe, A.R. COVID-19: Rethinking the Lockdown Groupthink. Front. Public Health 2021, 9, 625778. [Google Scholar] [CrossRef] [PubMed]
- Stranges, S.; Tigbe, W.; Gómez-Olivé, F.X.; Thorogood, M.; Kandala, N.-B. Sleep problems: An emerging global epidemic? Findings from the INDEPTH WHO-SAGE study among more than 40,000 older adults from 8 countries across Africa and Asia. Sleep 2012, 35, 1173–1181. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (US) Committee on Sleep Medicine and Research. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem; Colten, H.R., Altevogt, B.M., Eds.; National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Simpson, N.; Manber, R. Treating Insomnia during the COVID-19 Pandemic: Observations and Perspectives from a Behavioral Sleep Medicine Clinic. Behav. Sleep Med. 2020, 18, 573–575. [Google Scholar] [CrossRef]
- Kokou-Kpolou, C.K.; Megalakaki, O.; Laimou, D.; Kousouri, M. Insomnia during COVID-19 pandemic and lockdown: Prevalence, severity, and associated risk factors in French population. Psychiatry Res. 2020, 290, 113128. [Google Scholar] [CrossRef]
- Maniaci, A.; Ferlito, S.; Bubbico, L.; Ledda, C.; Rapisarda, V.; Iannella, G.; La Mantia, I.; Grillo, C.; Vicini, C.; Privitera, E.; et al. Comfort rules for face masks among healthcare workers during COVID-19 spread. Ann. Ig. 2021, 33, 615–627. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, T.J.; Fields, E.C.; Kensinger, E.A. Boston College daily sleep and well-being survey data during early phase of the COVID-19 pandemic. Sci. Data 2021, 8, 110. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalised anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Rosch, P.J. Book Review: Measuring Stress: A Guide for Health and Social Scientists; Cohen, S., Kessler, R.C., Gordon, L.U., Eds.; Oxford University Press: New York, NY, USA, 1997; Volume 236, p. 67. [Google Scholar] [CrossRef]
- James, S.A. John Henryism and the health of African-Americans. Cult. Med. Psychiatry 1994, 18, 163–182. [Google Scholar] [CrossRef] [Green Version]
- Cella, D.; Lai, J.S.; Jensen, S.E.; Christodoulou, C.; Junghaenel, D.U.; Reeve, B.B.; Stone, A.A. PROMIS Fatigue Item Bank had Clinical Validity across Diverse Chronic Conditions. J. Clin. Epidemiol. 2016, 73, 128–134. [Google Scholar] [CrossRef] [Green Version]
- Alvaro, P.K.; Roberts, R.M.; Harris, J.K. A Systematic Review Assessing Bidirectionality between Sleep Disturbances, Anxiety, and Depression. Sleep 2013, 36, 1059–1068. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Quantity and quality of sleep and incidence of type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2010, 33, 414–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grandner, M.; Mullington, J.M.; Hashmi, S.D.; Redeker, N.S.; Watson, N.F.; Morgenthaler, T.I. Sleep Duration and Hypertension: Analysis of >700,000 Adults by Age and Sex. J. Clin. Sleep Med. 2018, 14, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Lowe, C.J.; Safati, A.; Hall, P.A. The neurocognitive consequences of sleep restriction: A meta-analytic review. Neurosci. Biobehav. Rev. 2017, 80, 586–604. [Google Scholar] [CrossRef] [PubMed]
- Madrid-Valero, J.J.; Martínez-Selva, J.M.; Ordoñana, J.R. Sleep quality and body mass index: A co-twin study. J. Sleep Res. 2017, 26, 461–467. [Google Scholar] [CrossRef] [Green Version]
- Franceschini, C.; Musetti, A.; Zenesini, C.; Palagini, L.; Scarpelli, S.; Quattropani, M.C.; Lenzo, V.; Freda, M.F.; Lemmo, D.; Vegni, E.; et al. Poor Sleep Quality and Its Consequences on Mental Health During the COVID-19 Lockdown in Italy [Original Research]. Front. Psychol. 2020, 11, 3072. [Google Scholar] [CrossRef]
- Freeman, D.; Sheaves, B.; Goodwin, G.M.; Yu, L.M.; Nickless, A.; Harrison, P.J.; Emsley, R.; Luik, A.I.; Foster, R.G.; Wadekar, V.; et al. The effects of improving sleep on mental health (OASIS): A randomised controlled trial with mediation analysis. Lancet Psychiatry 2017, 4, 749–758. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Berglund, P.A.; Coulouvrat, C.; Hajak, G.; Roth, T.; Shahly, V.; Shillington, A.; Stephenson, J.J.; Walsh, J.K. Insomnia and the performance of US workers: Results from the America insomnia survey. Sleep 2011, 34, 1161–1171. [Google Scholar] [CrossRef]
- Voitsidis, P.; Gliatas, I.; Bairachtari, V.; Papadopoulou, K.; Papageorgiou, G.; Parlapani, E.; Syngelakis, M.; Holeva, V.; Diakogiannis, I. Insomnia during the COVID-19 pandemic in a Greek population. Psychiatry Res. 2020, 289, 113076. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.-N.; Zong, Q.-Q.; Yang, Y.; Zhang, L.; Xiang, Y.-F.; Ng, C.H.; Chen, L.-G.; Xiang, Y.-T. Gender Difference in the Prevalence of Insomnia: A Meta-Analysis of Observational Studies. Front. Psychiatry 2020, 11, 577429. [Google Scholar] [CrossRef] [PubMed]
- Lallukka, T.; Sares-Jäske, L.; Kronholm, E.; Sääksjärvi, K.; Lundqvist, A.; Partonen, T.; Rahkonen, O.; Knekt, P. Sociodemographic and socioeconomic differences in sleep duration and insomnia-related symptoms in Finnish adults. BMC Public Health 2012, 12, 565. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.W.; Juyal, R.; Shikha, D.; Gupta, R. Generalized Anxiety disorder but not depression is associated with insomnia: A population based study. Sleep Sci. 2018, 11, 166–173. [Google Scholar] [CrossRef]
- Kelly, M.M.; Tyrka, A.R.; Price, L.H.; Carpenter, L.L. Sex differences in the use of coping strategies: Predictors of anxiety and depressive symptoms. Depress. Anxiety 2008, 25, 839–846. [Google Scholar] [CrossRef] [Green Version]
- Nordin, Å.; Taft, C.; Lundgren-Nilsson, Å.; Dencker, A. Minimal important differences for fatigue patient reported outcome measures-a systematic review. BMC Med. Res. Methodol. 2016, 16, 62. [Google Scholar] [CrossRef] [Green Version]
- Dietch Jessica, R.; Taylor Daniel, J.; Sethi, K.; Kelly, K.; Bramoweth, A.D.; Roane, B.M. Psychometric Evaluation of the PSQI in U.S. College Students. J. Clin. Sleep Med. 2016, 12, 1121–1129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J.; Hall, M.L.; Strollo, P.J.; Kamarck, T.W.; Owens, J.; Lee, L.; Reis, S.E.; Matthews, K.A. Relationships between the Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), and clinical/polysomnographic measures in a community sample. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2008, 4, 563–571. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Peters, A.; Chen, G. Perceived Stress Mediates the Associations between Sleep Quality and Symptoms of Anxiety and Depression among College Nursing Students. Int. J. Nurs. Educ. Scholarsh. 2018, 20170020. [Google Scholar] [CrossRef]
- Alsaggaf, M.A.; Wali, S.O.; Merdad, R.A.; Merdad, L. Sleep quantity, quality, and insomnia symptoms of medical students during clinical years. Relationship with stress and academic performance. Saudi Med. J. 2016, 37, 173–182. [Google Scholar] [CrossRef]
- Boluarte-Carbajal, A.; Navarro-Flores, A.; Villarreal-Zegarra, D. Explanatory Model of Perceived Stress in the General Population: A Cross-Sectional Study in Peru During the COVID-19 Context [Original Research]. Front. Psychol. 2021, 12, 673945. [Google Scholar] [CrossRef]
- Tsang, S.; Avery, A.R.; Seto, E.Y.W.; Duncan, G.E. Is COVID-19 Keeping us Up at Night? Stress, Anxiety, and Sleep Among Adult Twins [Original Research]. Front. Neurosci. 2021, 15, 479. [Google Scholar] [CrossRef] [PubMed]
- Jansson-Fröjmark, M.; Lindblom, K. A bidirectional relationship between anxiety and depression, and insomnia? A prospective study in the general population. J. Psychosom. Res. 2008, 64, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Rolle, T.; Vue, Z.; Murray, S.A.; Shareef, S.A.; Shuler, H.D.; Beasley, H.K.; Marshall, A.G.; Hinton, A. Toxic stress and burnout: John Henryism and social dominance in the laboratory and STEM workforce. Pathog. Dis. 2021, 79, ftab041. [Google Scholar] [CrossRef] [PubMed]
- Gais, S.; Mölle, M.; Helms, K.; Born, J. Learning-Dependent Increases in Sleep Spindle Density. J. Neurosci. 2002, 22, 6830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortier-Brochu, E.; Morin, C.M. Cognitive impairment in individuals with insomnia: Clinical significance and correlates. Sleep 2014, 37, 1787–1798. [Google Scholar] [CrossRef] [PubMed]
- Mellor, A.; Bucks, R.S.; McGowan, H.; Waters, F. Self-Reported Sleep and Cognition: An Examination of Competing Functional Models. Arch. Psychol. 2018, 2. Available online: https://archivesofpsychology.org/index.php/aop/article/view/37 (accessed on 10 September 2021).




{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (SD Unless Stated Otherwise) |
|---|---|
| Age | 38.8 (17.8) |
| Gender, n (%) | |
| Male vs. female | 73 (15%) vs. 403 (85%) |
| Education, n (%) | |
| Some high school | 2 (0.4%) |
| High school diploma or GED | 15 (3.2%) |
| Some college | 62 (13%) |
| College degree | 125 (26.3%) |
| Some post-graduate education | 50 (10.5%) |
| Graduate, medical, or professional education | 222 (46.6%) |
| Income, n (%) | |
| $0–$25,000 | 4 (10.3%) |
| $25,001–$50,000 | 78 (16.4%) |
| $50,001–$75,000 | 85 (17.9%) |
| $75,001–$100,000 | 84 (17.7%) |
| $100,001–$150,000 | 54 (11.3%) |
| $150,001–$250,000 | 54 (11.3%) |
| $250,000+ | 39 (8.2%) |
| Clinical parameters | |
| PSQI | 6 (3.2) |
| JHACS | 43.6 (6.3) |
| ISI | 6.9 (5.2) |
| PROMIS Fatigue Scale | 17.4 (5.4) |
| PSS | 15.8 (7.6) |
| GAD-7 | 5.3 (4.8) |
| MMQ Satisfaction | 48.4 (14.6) |
| COVID-19 Positive Impact | 20 (5.7) |
| Poor sleep quality, n (%) | 311/476 (65%) |
| Clinical Insomnia, n (%) | 55/476 (11.5%) |
| Variable | ||
|---|---|---|
| Pittsburgh Sleep Quality Index | ||
| r | p Value | |
| JHACS | −0.1637 | <0.001 |
| ISI | 0.7691 | <0.001 |
| PROMIS Fatigue Scale | 0.5358 | <0.001 |
| PSS | 0.4456 | <0.001 |
| GAD-7 | 0.4660 | <0.001 |
| MMQ Satisfaction | −0.3152 | <0.001 |
| COVID Positive Impact | −0.1908 | <0.001 |
| Dependent Variable: PSQI | ||||||
|---|---|---|---|---|---|---|
| Model 1: β (95% CI) | p Value | Model 2: β (95% CI) | p Value | Model 3: β (95% CI) | p Value | |
| JHACS | −0.08 (−0.13 to −0.03) | 0.001 | −0.08 (−0.13 to −0.03) | 0.001 | −0.03 −0.07 to 0.004 | 0.005 |
| ISI | 0.48 (0.44 to 0.51) | <0.001 | 0.48 (0.44 to 0.52) | <0.001 | 0.4 0.35 to 0.44 | <0.001 |
| PROMIS fatigue scale | 0.32 (0.27 to 037) | <0.001 | 0.33 (0.28 to 0.38) | <0.001 | 0.05 0.005 to 0.1 | 0.03 |
| PSS | 0.19 (0.15 to 0.22) | <0.001 | 0.20 (0.17 to 0.24) | <0.001 | 0.004 −0.037 to 0.05 | 0.83 |
| GAD-7 | 0.32 (0.26 to 0.37) | <0.001 | 0.32 (0.27 to 0.38) | <0.001 | 0.09 0.02 to 0.01 | 0.013 |
| MMQ | −0.06 (−0.08 to −0.05) | <0.001 | −0.06 (−0.08 to 0.−05) | <0.001 | −0.002 −0.02 to 0.01 | 0.52 |
| COVID-19 impact | −0.12 (−0.16 to −0.05) | <0.001 | −0.10 (−0.16 to −0.05) | <0.001 | −0.01 −0.04 to 0.02 | 0.86 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alqahtani, J.S.; AlRabeeah, S.M.; Aldhahir, A.M.; Siraj, R.; Aldabayan, Y.S.; Alghamdi, S.M.; Alqahtani, A.S.; Alsaif, S.S.; Naser, A.Y.; Alwafi, H. Sleep Quality, Insomnia, Anxiety, Fatigue, Stress, Memory and Active Coping during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 4940. https://doi.org/10.3390/ijerph19094940
Alqahtani JS, AlRabeeah SM, Aldhahir AM, Siraj R, Aldabayan YS, Alghamdi SM, Alqahtani AS, Alsaif SS, Naser AY, Alwafi H. Sleep Quality, Insomnia, Anxiety, Fatigue, Stress, Memory and Active Coping during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(9):4940. https://doi.org/10.3390/ijerph19094940
Chicago/Turabian StyleAlqahtani, Jaber S., Saad M. AlRabeeah, Abdulelah M. Aldhahir, Rayan Siraj, Yousef S. Aldabayan, Saeed M. Alghamdi, Abdullah S. Alqahtani, Sulaiman S. Alsaif, Abdallah Y. Naser, and Hassan Alwafi. 2022. "Sleep Quality, Insomnia, Anxiety, Fatigue, Stress, Memory and Active Coping during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 9: 4940. https://doi.org/10.3390/ijerph19094940