
Passive Smoking and Risk of Gestational Diabetes Mellitus among Nonsmoking Women: A Prospective Cohort Study in China

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
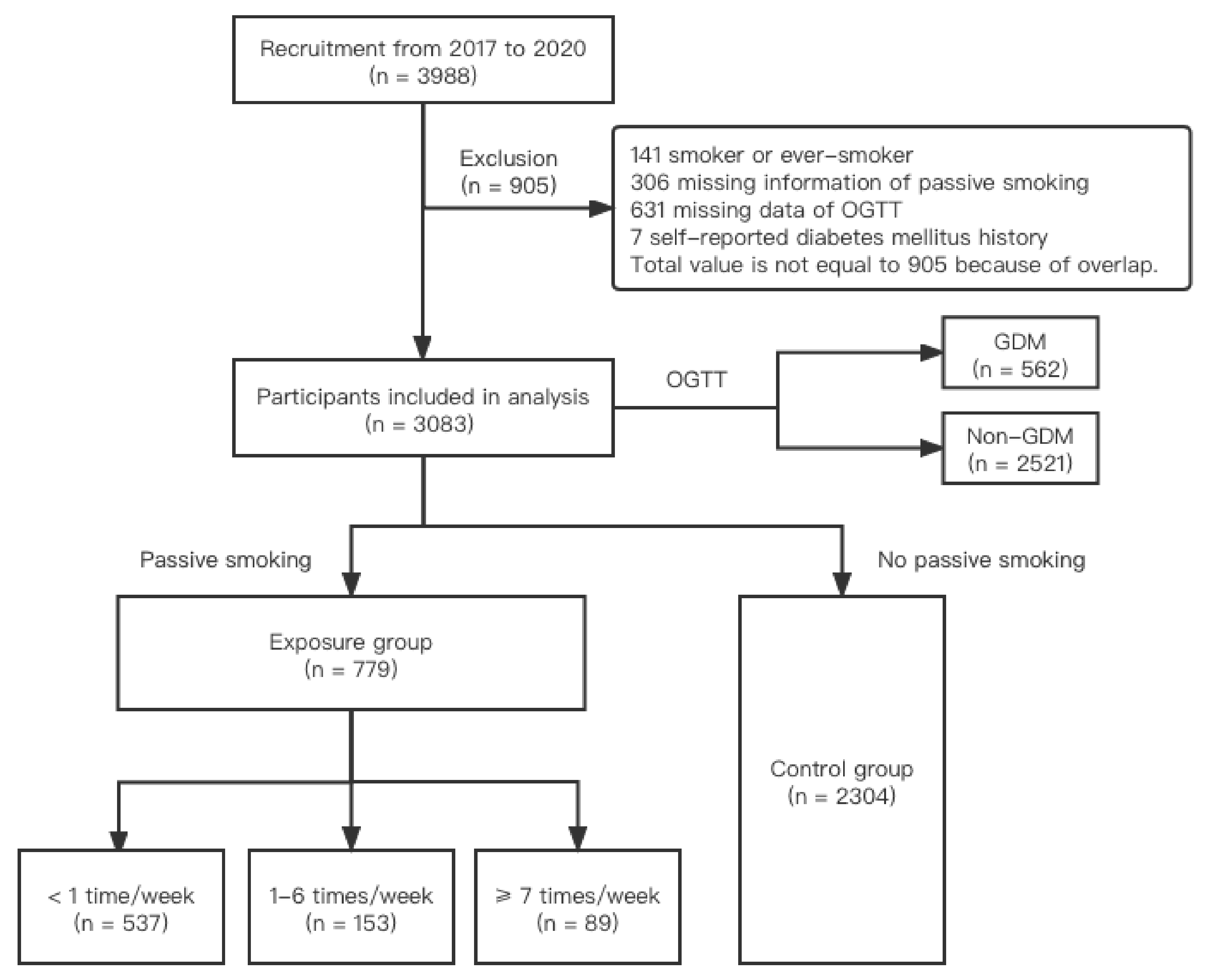
2.1. Study Design and Participants
2.2. Definition of Major Variable
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mack, L.R.; Tomich, P.G. Gesta tional diabetes: Diagnosis, classification, and clinical care. Obs. Gynecol. Clin. N. Am. 2017, 44, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhang, C. Prevalence of gestational diabetes and risk of progression to type 2 diabetes: A global perspective. Curr. Diab. Rep. 2016, 16, 7. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Kanguru, L.; Hussein, J.; Fitzmaurice, A.; Ritchie, K. Incidence of adverse outcomes associated with gestational diabetes mellitus in low- and middle-income countries. Int. J. Gynaecol. Obstet. 2013, 121, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, M.; Cao, Y.; Fadl, H.; Gustafson, H.; Simmons, D. Increasing prevalence of gestational diabetes mellitus when implementing the IADPSG criteria: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2021, 172, 108642. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Han, L.; Zhan, Y.; Cui, L.; Chen, W.a.; Ma, L.; Lv, J.; Pan, R.; Zhao, D.; Xiao, Z. Prevalence of gestational diabetes mellitus and associated risk factors in pregnant Chinese women: A cross-sectional study in Huangdao, Qingdao, China. Asia Pac. J. Clin. Nutr. 2018, 27, 383–388. [Google Scholar] [CrossRef]
- Baz, B.; Riveline, J.P.; Gautier, J.F. Endocrinology of pregnancy: Gestational diabetes mellitus: Definition, aetiological and clinical aspects. Eur. J. Endocrinol. 2016, 174, R43–R51. [Google Scholar] [CrossRef] [Green Version]
- Caulfield, L.E.; Harris, S.B.; Whalen, E.A.; Sugamori, M.E. Maternal nutritional status, diabetes and risk of macrosomia among Native Canadian women. Early Hum. Dev. 1998, 50, 293–303. [Google Scholar] [CrossRef]
- Kim, C.; Newton, K.M.; Knopp, R.H. Gestational diabetes and the incidence of type 2 diabetes: A systematic review. Diabetes Care 2002, 25, 1862–1868. [Google Scholar] [CrossRef] [Green Version]
- Ferrara, A. Increasing prevalence of gestational diabetes mellitus: A public health perspective. Diabetes Care 2007, 30 (Suppl. S2), S141–S146. [Google Scholar] [CrossRef] [Green Version]
- Epifano, L.; Di Vincenzo, A.; Fanelli, C.; Porcellati, F.; Perriello, G.; De Feo, P.; Motolese, M.; Brunetti, P.; Bolli, G.B. Effect of cigarette smoking and of a transdermal nicotine delivery system on glucoregulation in type 2 diabetes mellitus. Eur. J. Clin. Pharmacol. 1992, 43, 257–263. [Google Scholar] [CrossRef]
- Maddatu, J.; Anderson-Baucum, E.; Evans-Molina, C. Smoking and the risk of type 2 diabetes. Transl. Res. 2017, 184, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Kataria, Y.; Gaewsky, L.; Ellervik, C. Prenatal smoking exposure and cardio-metabolic risk factors in adulthood: A general population study and a meta-analysis. Int. J. Obes. 2019, 43, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Masalin, S.; Kautiainen, H.; Gissler, M.; Pennanen, P.; Eriksson, J.G.; Laine, M.K. Impact of smoking on gestational diabetes mellitus and offspring birthweight in primiparous women. Acta Obstet. Gynecol. Scand. 2020, 99, 1632–1639. [Google Scholar] [CrossRef] [PubMed]
- Bar-Zeev, Y.; Haile, Z.T.; Chertok, I.A. Association between prenatal smoking and gestational diabetes mellitus. Obstet. Gynecol. 2020, 135, 91–99. [Google Scholar] [CrossRef]
- Leng, J.; Wang, P.; Shao, P.; Zhang, C.; Li, W.; Li, N.; Wang, L.; Nan, H.; Yu, Z.; Hu, G.; et al. Passive smoking increased risk of gestational diabetes mellitus independently and synergistically with prepregnancy obesity in Tianjin, China. Diabetes Metab. Res. Rev. 2017, 33, e2861. [Google Scholar] [CrossRef]
- Xu, X.; Liu, Y.; Liu, D.; Li, X.; Rao, Y.; Sharma, M.; Zhao, Y. Prevalence and determinants of gestational diabetes mellitus: A cross-sectional study in China. Int. J. Environ. Res. Public Health 2017, 14, 1532. [Google Scholar] [CrossRef] [Green Version]
- Carroll, X.; Liang, X.; Zhang, W.; Zhang, W.; Liu, G.; Turner, N.; Leeper-Woodford, S. Socioeconomic, environmental and lifestyle factors associated with gestational diabetes mellitus: A matched case-control study in Beijing, China. Sci. Rep. 2018, 8, 8103. [Google Scholar] [CrossRef]
- Hosler, A.S.; Nayak, S.G.; Radigan, A.M. Stressful events, smoking exposure and other maternal risk factors associated with gestational diabetes mellitus. Paediatr. Perinat. Epidemiol. 2011, 25, 566–574. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Cai, M.; Gao, J.; Tang, S.; Xu, L.; Critchley, J.A. Trends in smoking and quitting in China from 1993 to 2003: National health service survey data. Bull. World Health Organ. 2010, 88, 769–776. [Google Scholar] [CrossRef]
- Schwartz, N.; Nachum, Z.; Green, M.S. The prevalence of gestational diabetes mellitus recurrence--effect of ethnicity and parity: A metaanalysis. Am. J. Obstet. Gynecol. 2015, 213, 310–317. [Google Scholar] [CrossRef]
- Jia, X.; Zhang, L.; Zhao, J.; Ren, M.; Li, Z.; Wang, J.; Wang, S.; Liu, Y.; An, H.; Li, Y.; et al. Associations between endocrine-disrupting heavy metals in maternal hair and gestational diabetes mellitus: A nested case-control study in China. Environ. Int. 2021, 157, 106770. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Classification and diagnosis of diabetes: Standards of medical care in diabetes—2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Hsia, J.; Tu, X.; Xia, Y.; Zhang, L.; Bi, Z.; Liu, H.; Li, X.; Stanton, B. Exposure to secondhand tobacco smoke and interventions among pregnant women in China: A systematic review. Prev. Chronic Dis. 2015, 12, E35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muthumalage, T.; Pritsos, K.; Hunter, K.; Pritsos, C. Commonly used air filters fail to eliminate secondhand smoke induced oxidative stress and inflammatory responses. Toxicol. Mech. Methods 2017, 27, 458–466. [Google Scholar] [CrossRef]
- Kostikas, K.; Minas, M.; Nikolaou, E.; Papaioannou, A.I.; Liakos, P.; Gougoura, S.; Gourgoulianis, K.I.; Dinas, P.C.; Metsios, G.S.; Jamurtas, A.Z.; et al. Secondhand smoke exposure induces acutely airway acidification and oxidative stress. Respir. Med. 2013, 107, 172–179. [Google Scholar] [CrossRef] [Green Version]
- Messner, B.; Bernhard, D. Smoking and cardiovascular disease: Mechanisms of endothelial dysfunction and early atherogenesis. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Reinehr, T. Inflammatory markers in children and adolescents with type 2 diabetes mellitus. Clin. Chim. Acta 2019, 496, 100–107. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Total | GDM | Non-GDM | p |
|---|---|---|---|---|
| (n = 3083) | (n = 562) | (n = 2521) | ||
| No. | No. (%) | No. (%) | ||
| Age (years) a | 30.69 ± 3.73 | 31.68 ± 4.12 | 30.47 ± 3.60 | <0.001 |
| BMI (kg/m2) a | 21.68 ± 3.05 | 22.60 ± 3.23 | 21.47 ± 2.97 | <0.001 |
| Ethnicity | ||||
| Han | 2892 | 527 (20.33) | 2365 (81.67) | 1.000 |
| Others | 189 | 34 (17.99) | 155 (82.01) | |
| Education | ||||
| Master’s or above | 877 | 143 (16.31) | 734 (83.69) | 0.216 |
| College | 1424 | 273 (19.17) | 1151 (80.83) | |
| High school or below | 778 | 144 (18.51) | 634 (81.49) | |
| Occupation | ||||
| Famer/industry/business/service | 742 | 137 (18.46) | 605 (81.54) | 0.935 |
| Civil servant | 1665 | 298 (17.90) | 1367 (82.10) | |
| Others | 640 | 114 (17.81) | 526 (82.19) | |
| Parity | ||||
| Nulliparous | 2501 | 422 (16.87) | 2079 (83.13) | <0.001 |
| Multiparous | 582 | 140 (24.05) | 442 (75.95) |
| Total No. | GDM | Non-GDM | Crude OR (95% CI) | Adjusted OR a (95% CI) | |
|---|---|---|---|---|---|
| No. (%) | No. (%) | ||||
| No passive smoking | 2304 | 391 (16.97) | 1913 (83.03) | 1 | 1 |
| Passive smoking b (times/week) | 779 | 171 (21.95) | 608 (78.05) | 1.38 (1.12, 1.68) | 1.37 (1.11, 1.70) |
| <1 | 537 | 106 (19.74) | 431 (80.26) | 1.20 (0.95, 1.53) | 1.21 (0.94, 1.55) |
| 1–6 | 153 | 43 (28.10) | 110 (71.90) | 1.91 (1.32, 2.77) | 1.81 (1.22, 2.69) |
| ≥7 c | 89 | 22 (24.72) | 67 (75.28) | 1.61 (0.98, 2.63) | 1.70 (1.02, 2.84) |
| Parity | GDM | Non-GDM | Crude OR (95% CI) | Adjusted OR a (95% CI) |
|---|---|---|---|---|
| No. (%) | No. (%) | |||
| Total | 562 (18.23) | 2521 (81.77) | 1.38 (1.12, 1.68) | 1.37 (1.11, 1.70) |
| Nulliparous | 422 (16.87) | 2079 (83.13) | 1.43 (1.14, 1.80) | 1.45 (1.14, 1.85) |
| Multiparous | 140(24.05) | 442 (75.85) | 1.16 (0.77, 1.77) | 1.14 (0.73, 1.78) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Na, J.; Chen, H.; An, H.; Ren, M.; Jia, X.; Wang, B.; Li, Z.; Liu, X.; Ye, R.; Li, N. Passive Smoking and Risk of Gestational Diabetes Mellitus among Nonsmoking Women: A Prospective Cohort Study in China. Int. J. Environ. Res. Public Health 2022, 19, 4712. https://doi.org/10.3390/ijerph19084712
Na J, Chen H, An H, Ren M, Jia X, Wang B, Li Z, Liu X, Ye R, Li N. Passive Smoking and Risk of Gestational Diabetes Mellitus among Nonsmoking Women: A Prospective Cohort Study in China. International Journal of Environmental Research and Public Health. 2022; 19(8):4712. https://doi.org/10.3390/ijerph19084712
Chicago/Turabian StyleNa, Jigen, Huiting Chen, Hang An, Mengyuan Ren, Xiaoqian Jia, Bin Wang, Zhiwen Li, Xiaohong Liu, Rongwei Ye, and Nan Li. 2022. "Passive Smoking and Risk of Gestational Diabetes Mellitus among Nonsmoking Women: A Prospective Cohort Study in China" International Journal of Environmental Research and Public Health 19, no. 8: 4712. https://doi.org/10.3390/ijerph19084712