
How Does E-mail-Delivered Cognitive Behavioral Therapy Work for Young Adults (18–28 Years) with Insomnia? Mediators of Changes in Insomnia, Depression, Anxiety, and Stress



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Insomnia Severity
Japanese Version of the Insomnia Severity Index
2.2.2. Insomnia-Related Measures
Japanese Version of the Sleep Hygiene Practices Scale
Japanese Version of the Ford Insomnia Response to Stress Test
Japanese Version of the Dysfunctional Beliefs and Attitudes about Sleep-16
Japanese Version of the Pre-Sleep Arousal Scale
2.2.3. Mental Health-Related Measures
Japanese Version of the Depression Anxiety Stress Scale-21
2.3. Procedure
2.4. Statistical Analysis
2.4.1. Descriptive Statistics and t-Test
2.4.2. Hierarchical Multiple Regression Analysis
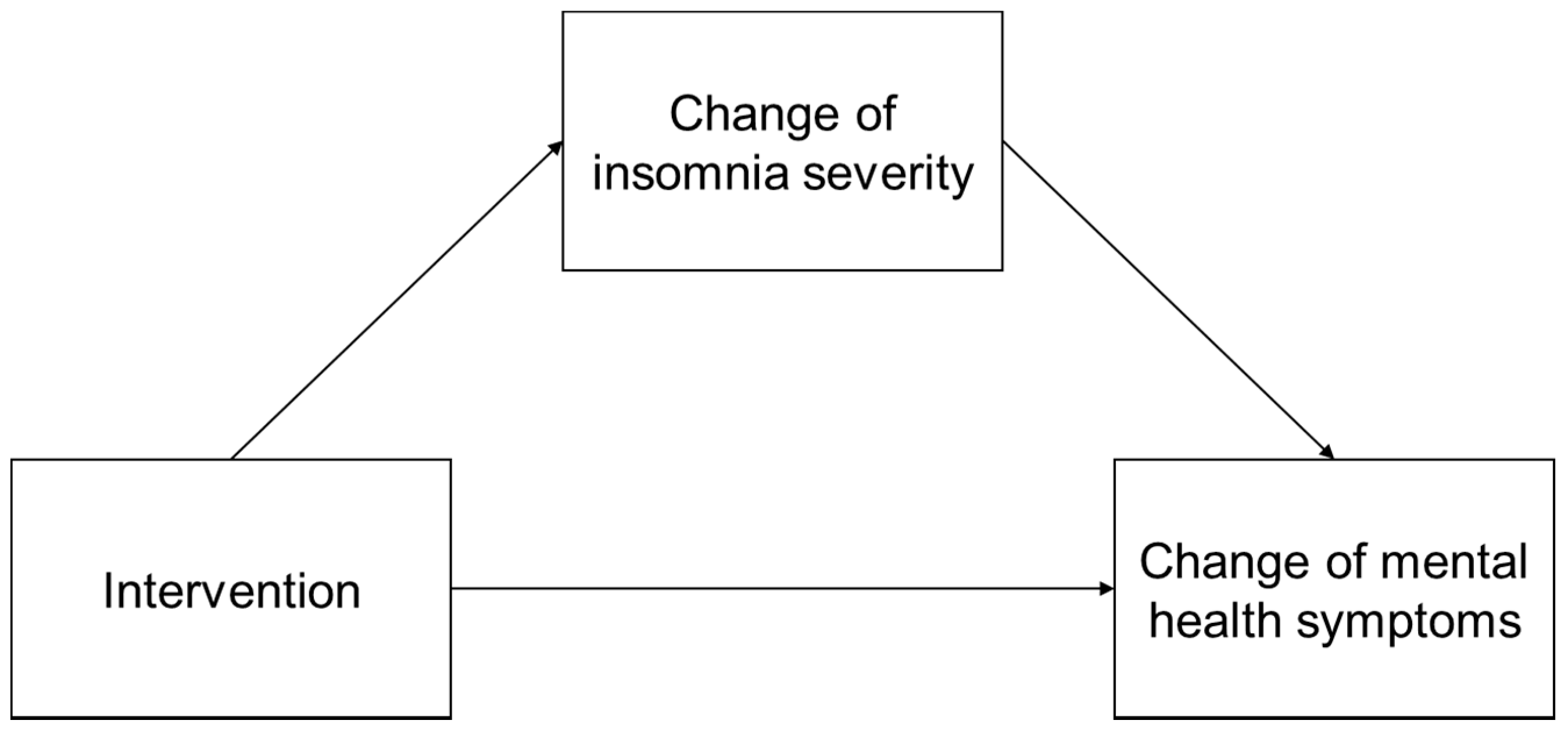
2.4.3. Mediation Analysis
2.5. Ethical Considerations
3. Results
3.1. Comparing Descriptive Statistics between Groups
3.2. Mediators of Improvement in Insomnia Severity
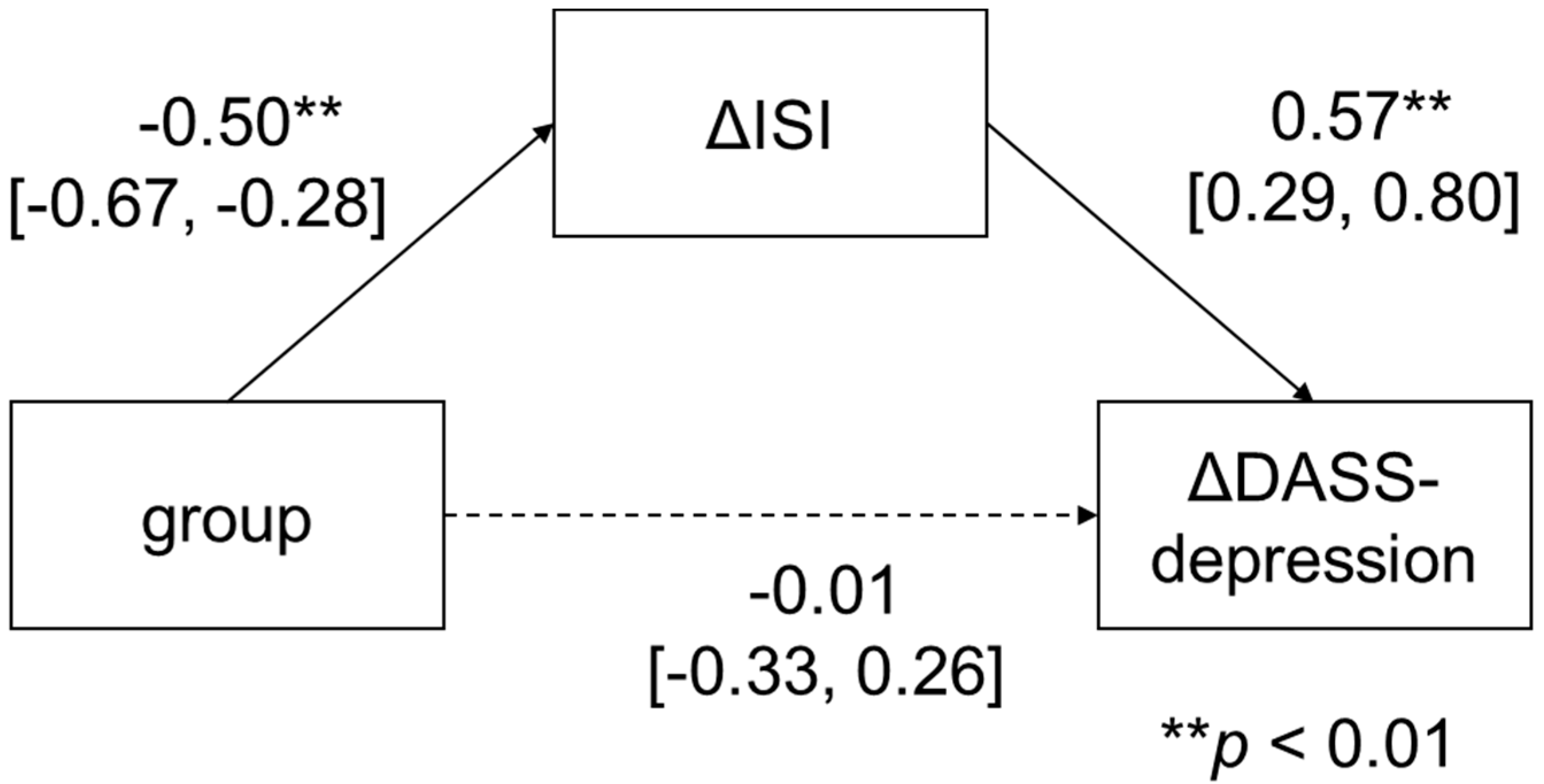
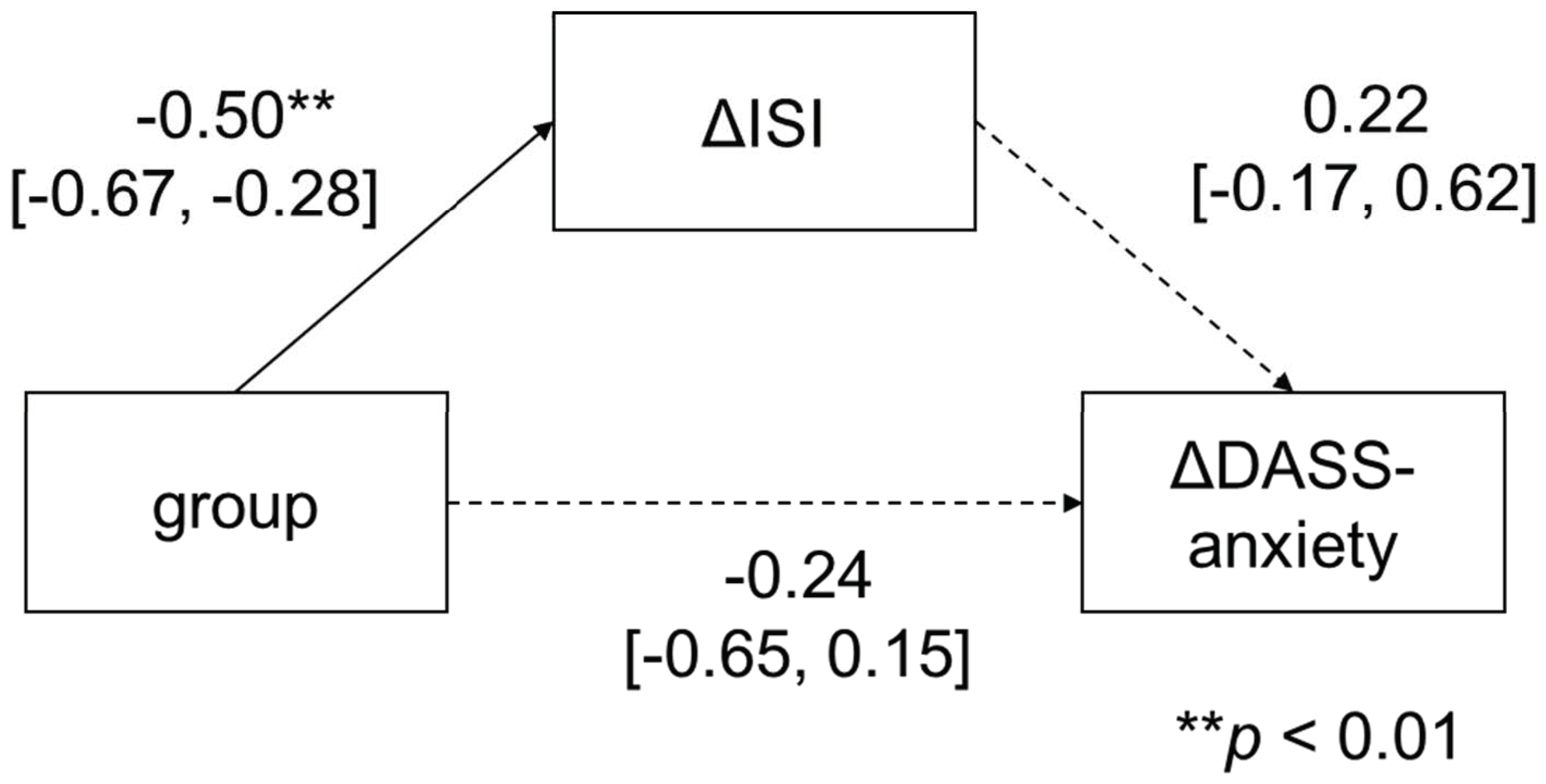
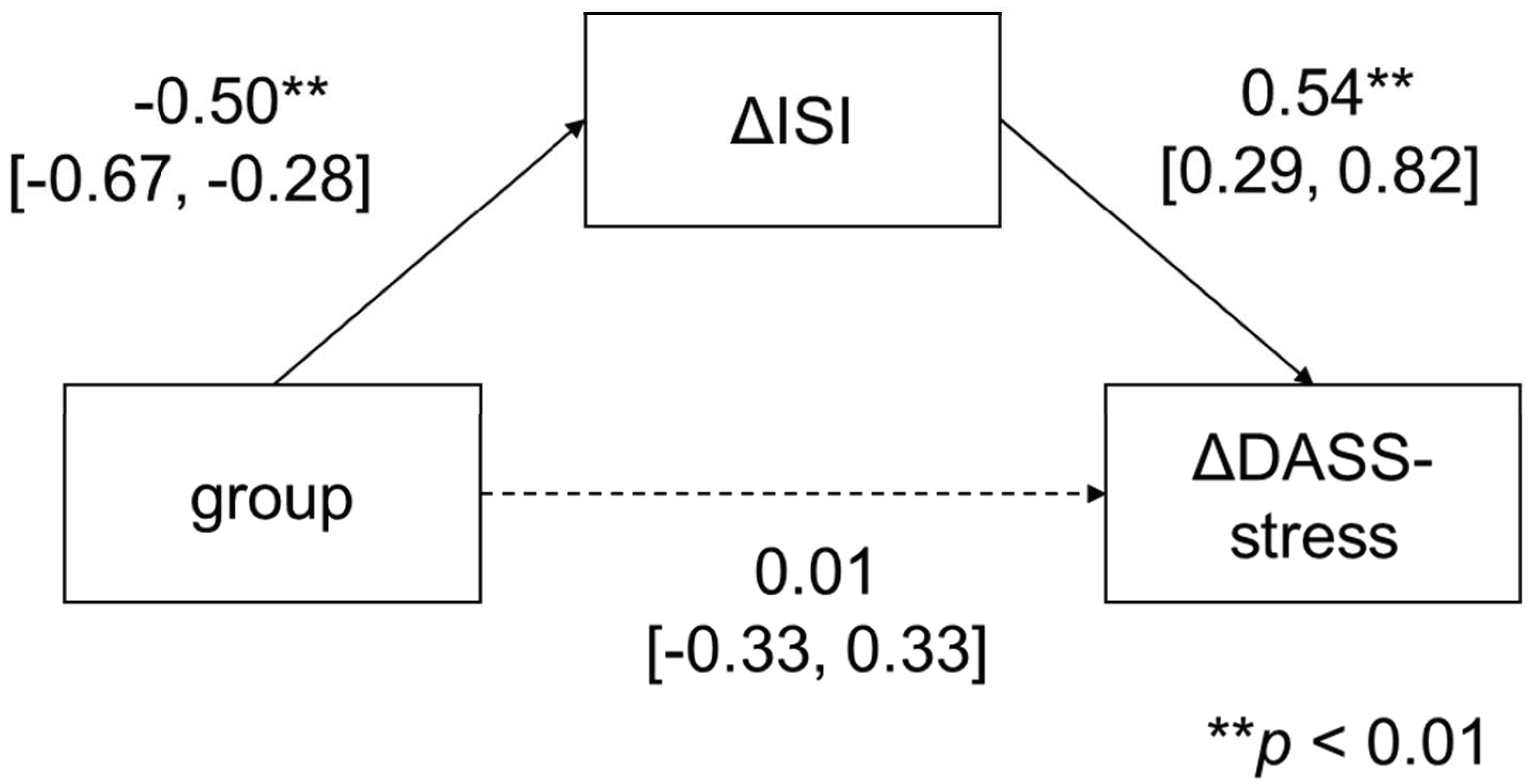
3.3. Improvement in Insomnia Mediated by Reductions in Depression, Anxiety, and Stress
4. Discussion
4.1. Mediators of Improvement in Insomnia Severity
4.2. Improvement in Insomnia Mediated by Reductions in Depression, Anxiety, and Stress
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Becker, S.P.; Dvorsky, M.R.; Holdaway, A.S.; Luebbe, A.M. Sleep problems and suicidal behaviors in college students. J. Psychiatr. Res. 2018, 99, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Japanese National University Council of Health Administration Facilities. University Student Health. 2015. Available online: http://www.htc.nagoya-u.ac.jp/wp-content/uploads/2019/09/hakusho2015.pdf (accessed on 30 January 2020).
- Morin, C.M.; Jarrin, D.C.; Ivers, H.; Mérette, C.; LeBlanc, M.; Savard, J. Incidence, persistence, and remission rates of insomnia over 5 years. JAMA Netw. Open 2020, 3, e2018782. [Google Scholar] [CrossRef]
- Hertenstein, E.; Feige, B.; Gmeiner, T.; Kienzler, C.; Spiegelhalder, K.; Johann, A.; Jansson-Fröjmark, M.; Palagini, L.; Rücker, G.; Riemann, D.; et al. Insomnia as a predictor of mental disorders: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 43, 96–105. [Google Scholar] [CrossRef] [PubMed]
- Lund, H.G.; Reider, B.D.; Whiting, A.B.; Prichard, J.R. Sleep patterns and predictors of disturbed sleep in a large population of college students. J. Adolesc. Health 2010, 46, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.E.; Ramsay Roberts, C.; Chan, W. Persistence and change in symptoms of insomnia among adolescents. Sleep 2008, 31, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Li, S.X.; Chan, N.Y.; Yu, M.W.M.; Lam, S.P.; Zhang, J.; Chan, J.W.Y.; Li, A.M.; Wing, Y.K. Eveningness chronotype, insomnia symptoms, and emotional and behavioural problems in adolescents. Sleep Med. 2018, 47, 93–99. [Google Scholar] [CrossRef]
- Morioka, H.; Itani, O.; Kaneita, Y.; Ikeda, M.; Kondo, S.; Yamamoto, R.; Osaki, Y.; Kanda, H.; Higuchi, S.; Ohida, T. Associations between sleep disturbance and alcohol drinking: A large-scale epidemiological study of adolescents in Japan. Alcohol 2013, 47, 619–628. [Google Scholar] [CrossRef] [PubMed]
- Soehner, A.M.; Harvey, A.G. Prevalence and functional consequences of severe insomnia symptoms in mood and anxiety disorders: Results from a nationally representative sample. Sleep 2012, 35, 1367–1375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, A.B.; Dzierzewski, J.M.; Griffin, S.C.; Lind, M.J.; Dick, D.; Rybarczyk, B.D. Insomnia disorder and behaviorally induced insufficient sleep syndrome: Prevalence and relationship to depression in college students. Behav. Sleep Med. 2020, 18, 275–286. [Google Scholar] [CrossRef]
- Hershner, S.; O’brien, L.M. The impact of a randomized sleep education intervention for college students. J. Clin. Sleep Med. 2018, 14, 337–347. [Google Scholar] [CrossRef] [Green Version]
- Trockel, M.; Manber, R.; Chang, V.; Thurston, A.; Tailor, C.B. An e-mail delivered CBT for sleep-health program for college students: Effects on sleep quality and depression symptoms. J. Clin. Sleep Med. 2011, 7, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Okajima, I.; Tanizawa, N.; Harata, M.; Suh, S.; Yang, C.M.; Li, S.X.; Trockel, M.T. Can an e-mail-delivered CBT for insomnia validated in the West be effective in the East? A randomized controlled trial. Int. J. Environ. Res. Public Health 2022, 19, 186. [Google Scholar] [CrossRef] [PubMed]
- Okajima, I.; Inoue, Y. Efficacy of cognitive behavioral therapy for comorbid insomnia: A meta-analysis. Sleep Biol. Rhythm. 2018, 16, 21–35. [Google Scholar] [CrossRef]
- Wu, J.Q.; Appleman, E.R.; Salazar, R.D.; Ong, J.C. Cognitive behavioral therapy for insomnia comorbid with psychiatric and medical conditions: A meta-analysis. JAMA Intern. Med. 2015, 175, 1461–1472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, P.I.; Ingersoll, K.S.; Thorndike, F.P.; Lord, H.R.; Gonder-Frederick, L.; Morin, C.M.; Ritterband, L.M. Cognitive mechanisms of sleep outcomes in a randomized clinical trial of internet-based cognitive behavioral therapy for insomnia. Sleep Med. 2018, 47, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Lancee, J.; Effting, M.; Van der Zweerde, T.; van Daal, L.; van Straten, A.; Kamphuis, J.H. Cognitive processes mediate the effects of insomnia treatment: Evidence from a randomized wait-list controlled trial. Sleep Med. 2019, 54, 86–93. [Google Scholar] [CrossRef]
- Okajima, I.; Nakajima, S.; Ochi, M.; Inoue, Y. Association among changes in sleep-related beliefs, sleep reactivity, and improvement of insomnia following cognitive behavioral therapy. Sleep Med. 2017, 29, 96. [Google Scholar] [CrossRef]
- Parsons, C.E.; Zachariae, R.; Landberger, C.; Young, K.S. How does cognitive behavioural therapy for insomnia work? A systematic review and meta-analysis of mediators of change. Clin. Psychol. Rev. 2021, 86, 102027. [Google Scholar] [CrossRef]
- Okajima, I.; Chen, J. The effect of insomnia on changes in anxiety, depression, and social function after a transdiagnostic treatment targeting excessive worry. Sleep Biol. Rhythm. 2017, 15, 243–249. [Google Scholar] [CrossRef]
- Munezawa, T.; Morin, C.M.; Inoue, Y.; Nedate, K. Development of the Japanese version of Insomnia Severity Index (ISI-J). Jpn. J. Psychiatr. Treat. 2009, 24, 219–225. [Google Scholar]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Yang, C.M.; Lin, S.C.; Hsu, S.C.; Cheng, C.P. Maladaptive sleep hygiene practices in good sleepers and patients with insomnia. J. Health Psychol. 2010, 15, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Hara, S.; Nonaka, S.; Ishii, M.; Ogawa, Y.; Yang, C.M.; Okajima, I. Validation of the Japanese version of the Sleep Hygiene Practice Scale. Sleep Med. 2021, 80, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Drake, C.L.; Pillai, V.; Roth, T. Stress and sleep reactivity: A prospective investigation of the stress-diathesis model of insomnia. Sleep 2014, 37, 1295–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakajima, S.; Okajima, I.; Sasai, T.; Kobayashi, M.; Furudate, N.; Drake, C.L.; Roth, T.; Inoue, Y. Validation of the Japanese version of the Ford Insomnia Response to Stress Test and the association of sleep reactivity with trait anxiety and insomnia. Sleep Med. 2014, 15, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Morin, C.M.; Vallières, A.; Ivers, H. Dysfunctional beliefs and attitudes about sleep (DBAS): Validation of a brief version (DBAS-16). Sleep 2007, 30, 1547–1554. [Google Scholar] [CrossRef] [Green Version]
- Munezawa, T.; Morin, C.M.; Inoue, Y.; Nedate, K. Development of the Japanese version of Dysfunctional Beliefs and Attitudes about Sleep Scale (DBAS-J). Jpn. J. Sleep Med. 2009, 3, 396–403. [Google Scholar]
- Nicassio, P.M.; Mendlowitz, D.R.; Fussell, J.J.; Petras, L. The phenomenology of the pre-sleep state: The development of the pre-sleep arousal scale. Behav. Res. Ther. 1985, 23, 263–271. [Google Scholar] [CrossRef]
- Okajima, I.; Ishii, M.; Ochi, M.; Nicassio, P.M. Psychometric properties of the Japanese version of the Pre-Sleep Arousal Scale. Tohoku J. Exp. Med. 2020, 252, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Adachi, K.; Yoshino, M.; Ueno, T. The standardization of DASS Japanese version (II). In Proceedings of the 26th Convention of the Japanese Association of Health Psychology, Tokyo, Japan, 21 July 2013. [Google Scholar]
- Cohen, M.A. Some new evidence on the seriousness of crime. Criminology 1988, 26, 343–353. [Google Scholar] [CrossRef]
- Bei, B.; Ong, J.C.; Rajaratnam, S.M.; Manber, R. Chronotype and improved sleep efficiency independently predict depressive symptom reduction after group cognitive behavioral therapy for insomnia. J. Clin. Sleep Med. 2015, 11, 1021–1027. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K. Somnology; Jihou: Tokyo, Japan, 2003. [Google Scholar]
- McGowan, S.K.; Espejo, E.P.; Balliett, N.; Werdowatz, E.A. The effects of transdiagnostic group CBT for anxiety on insomnia symptoms. Cogn. Behav. Ther. 2016, 45, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Short, N.A.; Allan, N.P.; Raines, A.M.; Schmidt, N.B. The effects of an anxiety sensitivity intervention on insomnia symptoms. Sleep Med. 2015, 16, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, T.; Inugami, M.; Ishihara, K.; Fukuda, K. Construction of sleep-hygiene scales and classification of sleep patterns in undergraduates. Jpn. J. Educ. Psychol. 2000, 48, 294–304. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Intervention Group (n = 21) | Control Group (n = 20) | Hedges’ g | ||||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | t Value | [95% CI] | ||
| Mental health | |||||||
| ΔDASS | −9.52 | 9.25 | −2.90 | 9.43 | 2.27 | * | −0.70 [−1.31, −0.08] |
| ΔDASS-depression | −3.19 | 3.86 | −0.75 | 4.31 | 1.91 | −0.59 [−1.20, 0.03] | |
| ΔDASS-anxiety | −2.38 | 2.54 | −0.50 | 2.69 | 2.31 | * | −0.71 [−1.32, −0.09] |
| ΔDASS-stress | −3.67 | 4.18 | −1.55 | 3.80 | 1.69 | −0.52 [−1.13, 0.09] | |
| Insomnia symptoms | |||||||
| ΔISI | −6.57 | 4.14 | −2.00 | 3.92 | 3.63 | ** | −1.11 [−1.76, −0.46] |
| Sleep-related cognitive behavioral factor | |||||||
| ΔSHPS total | −17.86 | 26.38 | −2.8 | 17.92 | 2.13 | * | −0.65 [−1.27, −0.03] |
| ΔSleep schedule and timing | −7.24 | 7.64 | −1.2 | 4.44 | 3.11 | ** | −0.94 [−1.58, −0.31] |
| ΔArousal-related behaviors | −6.48 | 10.06 | −1.1 | 6.87 | 2.00 | −0.67 [−1.29, −0.05] | |
| ΔEating/drinking habits prior to sleep | −3.10 | 4.64 | 0.2 | 4.89 | 2.21 | * | −0.68 [−1.30, −0.06] |
| ΔSleep environment | −1.05 | 8.22 | −0.7 | 6.03 | 0.15 | −0.05 [−0.65, 0.55] | |
| ΔDBAS | −17.76 | 18.96 | −7.2 | 16.47 | 1.90 | −0.58 [−1.20, 0.03] | |
| ΔPSAS total | −11.81 | 13.47 | −2.75 | 6.97 | 2.68 | * | −0.82 [−1.45, −0.20] |
| ΔPSASs | −4.10 | 4.74 | 0.05 | 4.44 | 2.89 | * | −0.89 [−1.52, −0.26] |
| ΔPSASc | −7.71 | 9.39 | −2.8 | 4.53 | 2.15 | * | −0.65 [−1.26, −0.03] |
| ΔFIRST | −2.71 | 5.26 | −2.75 | 3.88 | −0.03 | 0.01 [−0.59, 0.61] | |
| Variables | B | SE | β | R2 | ΔR2 | ||||
|---|---|---|---|---|---|---|---|---|---|
| ΔISI | |||||||||
| Step1: | group | −2.00 | 0.90 | −0.50 | ** | 0.25 | ** | 0.25 | ** |
| Step2: | group | −4.79 | 1.61 | −0.53 | ** | 0.53 | * | 0.28 | * |
| ΔSleep schedule and timing | 0.17 | 0.13 | 0.26 | ||||||
| ΔArousal-related behaviors | −0.10 | 0.11 | −0.19 | ||||||
| ΔEating/drinking habits prior to sleep | 0.13 | 0.18 | 0.14 | ||||||
| ΔSleep environment | 0.16 | 0.13 | 0.25 | ||||||
| ΔDBAS | −0.06 | 0.04 | −0.23 | ||||||
| ΔPSASs | −0.13 | 0.16 | −0.14 | ||||||
| ΔPSASc | −0.01 | 0.12 | −0.01 | ||||||
| ΔFIRST | 0.39 | 0.18 | 0.39 | * | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ubara, A.; Tanizawa, N.; Harata, M.; Suh, S.; Yang, C.-M.; Li, X.; Okajima, I. How Does E-mail-Delivered Cognitive Behavioral Therapy Work for Young Adults (18–28 Years) with Insomnia? Mediators of Changes in Insomnia, Depression, Anxiety, and Stress. Int. J. Environ. Res. Public Health 2022, 19, 4423. https://doi.org/10.3390/ijerph19084423
Ubara A, Tanizawa N, Harata M, Suh S, Yang C-M, Li X, Okajima I. How Does E-mail-Delivered Cognitive Behavioral Therapy Work for Young Adults (18–28 Years) with Insomnia? Mediators of Changes in Insomnia, Depression, Anxiety, and Stress. International Journal of Environmental Research and Public Health. 2022; 19(8):4423. https://doi.org/10.3390/ijerph19084423
Chicago/Turabian StyleUbara, Ayaka, Noriko Tanizawa, Megumi Harata, Sooyeon Suh, Chien-Ming Yang, Xin Li, and Isa Okajima. 2022. "How Does E-mail-Delivered Cognitive Behavioral Therapy Work for Young Adults (18–28 Years) with Insomnia? Mediators of Changes in Insomnia, Depression, Anxiety, and Stress" International Journal of Environmental Research and Public Health 19, no. 8: 4423. https://doi.org/10.3390/ijerph19084423