1.1. Reseach Background
The Coronavirus disease (COVID-19) pandemic has spread rapidly around the world with 291,241,130 confirmed cases and 5,458,356 deaths as of the date 4 January 2022 [
1]. The pandemic had significantly altered every aspect of human life around the world. In Taiwan, the number of confirmed cases and deaths may be relatively small, 17,095 confirmed cases and 850 deaths, but the epidemic has noticeable influences on Taiwanese’s work and life behaviors.
Compared to the general coronavirus, COVID-19 attacks the human respiratory tract system more severely, and some cases will cause severe pneumonia and respiratory failure, and eventually lead to death. Prevailing treatments in response to the confirmed victim remain to support the human’s immune system to avoid the patient’s condition becoming severe after infection. Most severe cases of COVID-19 were found in the elderly or people with impaired or poor immune systems.
On the other hand, air pollution is one of the factors that are detrimental to human health, being accountable for 6.4 million deaths worldwide in 2015 [
2,
3], especially due to those particulate matters (PM) in the air with aerodynamic diameters ≤10 µm and ≤2.5 µm [
4]. Both air pollution and COVID-19 are detrimental to humans’ respiratory health. Although have some argued that the lockdowns during the pandemic of COVID-19 have sharply mitigated the burden of air pollution around the world [
5], residents in an area that had been exposed to high levels of PM have been proven to have a strong correlation with the deaths related to COVID-19 [
4]. Compared to the general population, people who had suffered polluted air are apparently situated in a more detrimental condition with higher risks to their health, especially the respiratory system. Literature has evidenced that people who work or live in the neighborhood of risk source, e.g., epicenters, will perceive a higher risk of threats and will cause corresponding symptoms [
6]. It will be interesting to know whether the threats of COVID-19 will be aggravated to the population who have long exposure to the risk of air pollution and accordingly affect their decisions in choosing preventive measures against COVID-19. Polluted air is one source of threats, and COVID-19 is another.
Although vaccination remains one of the primary measures to prevent infection of COVID-19, others measures such as physical distancing and personal hygiene, as well as nutrition supplementation for human immunity are also recommended [
4].
Maintaining a sufficient level of required nutrition is essential to support the human immune system, however, decisions on the kinds and doses of each nutrition for each individual are complicated. It is wise to consult with the healthcare professionals such as pharmacists, nutritionists, physicians to gain optimal effects. To minimize the infection, people were advised to avoid crowded gatherings in a closed space, including medical institutes during the pandemic. Gaining advice from the pharmacists in a community pharmacy is a better alternative than visiting the physicians in a hospital in this special period.
Just as we are concerned about the service provided by a medical institute, pharmacy as an integrated part of the national healthcare system can provide a wide range of services to help people’s health needs, including how to prevent being infected by COVID-19.
The Central Epidemic Command Center (CEEC) of Taiwan hosts press conferences and provides news and informative data on COVID-19 daily as part of the nation’s anti-epidemic countermeasures. CEEC is the legal source of national level for collecting and disseminating the epidemic-associated information, including the number of confirmed cases, death toll, as well as the knowledge, anti-epidemic practices, and regulations regarding COVID-19. In the meantime, news and information of this kind are transmitted with multiple languages (including dialects and major foreign languages) to the public through various media 24 h a day. Under such continuous news bombardments, we can infer that the elderly, especially those aged at least 55, have been duly informed as to those most susceptible to severe illness when infected by COVID-19 in Taiwan.
The question was over how the people who are under such an environment of multiple threats will decide over the pharmacy service utilization (PSU) as a protective measure to prevent COVID-19. The purpose of this study is to explore how people who have already been exposed to the risk of air pollution in their daily life will react to the threats of being infected by COVID-19, and how this perception will affect their willingness to use pharmacy services as a measure to support their actions in lowering the risk of being infected and/or the possibility of becoming severe when being infected.
1.2. Literature Review
Poor air quality contains several pollutants in the air, such as PM
2.5, PM
10, O
3, SO
2 among others [
7,
8], in particular the particulate matters (PM). Adverse health effects of PM are mainly to induce pulmonary inflammation and consequently cause a higher risk of mortality and serious morbidity, especially for the population of the elderly, infants, and persons with chronic cardiopulmonary diseases or lung-related problems [
7,
8]. In Taiwan, the government adopted an Air Quality Index (AQI) to monitor the air quality, especially for those days with AQI > 100. AQI is composed of information of pollutants such as PM
2.5, PM
10, O
3, SO
2 among others that are harmful to human health. The air quality index (AQI) is composed of several sub-indicators of ozone (O
3), fine suspended particulate matter (PM
2.5, current standard at 15.0 μg/m
3/year average, 35.0 μg/m
3/24 H in Taiwan), suspended particulate matter (PM
10, 50.0 μg/m
3/year average, 100.0 μg/m
3/24 H), carbon monoxide (CO, 35 ppm/1 H, 9 ppm/8 H), sulfur dioxide (SO
2, 0.075 ppm/year average, 0.02 μg/m
3/8 H) and nitrogen dioxide (NO
2, 0.03 ppm/year average, 0.1 ppm/1 H), all of which are calculated according to their degree of impact on human health [
9].
In southern Taiwan, the most noted area of greatest concern for high air pollution risk is the neighborhood surrounding industrial parks, which covers Siaogang (Xiaogang), Linyuan, Cianjhen, Fongshan, and Daliao of Kaohsiung, as shown in
Figure 1.
Table 1 shows the number of days with AQI greater than 100 in each region [
9]. The major source of air pollution that affects the air quality of the target districts are Kaohsiung Linhai Industrial Park (KLIP), Dafa Industrial Park (DIP), and Linyuan Industrial Park (LIP). KLIP accommodates 502 companies and more than 40,000 workers including giant steel, shipbuilding, cement, petroleum, and chemical companies in its 1582 hectares of land; and LIP covered 403.2 hectares of land to accompany 33 giant companies of plastic, chemical, and petroleum, whereas DIP accommodates metal processing companies in its area of 378.8 hectares. Siaogang is the home of KLIP, Daliao is for Dafa Industrial Park, and Linyuan is for LIP. Cianjhen district is not only a neighbor of these two industrial parks, it is also an ocean port for fishing and shipbuilding industries and the home of the previous Kaohsiung Export Processing Zone. Daliao and Fongshan are districts adjacent to both industrial parks in the same Kaohsiung Metropolitan area [
10].
An AQI value of 100 or above indicates that the air quality is harmful to human health.
Table 1 shows the number of days with AQI exceeding 100 in each region of this study. Despite that the days exceeding the standard are decreasing, all regions far exceed the national average, among which Siaogang is almost the highest on both of the days of AQI > 100 and the PM
2.5 between years of 2018 and 2021, as shown in
Table 1.
The community pharmacy plays important role in the anti-epidemic battle by providing easy-accessible and timely epidemic prevention supplies and medical equipment, such as small-package masks, over-the-counter (OTC) drugs, thermometers, alcohol, and other items to prevent infection.
In this special risky period of time, community pharmacy can be helpful in many ways [
11], such as teaching and consulting appropriate hygiene techniques and methods, providing suggestions of nutrition intake, transmitting correct epidemic prevention knowledge, providing psychological (and emotional) support, assisting in preliminary tests for those suspicious customers such as body temperature, consulting travel history, etc., and help to monitor and report to the epidemic prevention agency for any suspicious cases [
1].
Pharmacists and their community pharmacies are one of the best alternatives or substitutes other than physicians in the medical institutes for health promotion requirements, since pharmacists are the healthcare professionals who were trained to provide services of medication expertise and health promotion advice to the patients. Compared to other healthcare professionals, the pharmacists in the community pharmacy are particularly easy to reach by people. In Taiwan, 6603 community pharmacies around the country were included with a contract with the National Health Insurance Agency (NHIA) in the national healthcare system (there are an additional 1510 pharmacies which were not contracted with NHIA) [
12].
Utilizing the pharmacy service is one of the best sources for health promotion decisions during the pandemic for at least several reasons as follows. Firstly, they are healthcare professionals with abundant healthcare knowledge; second, as a part of the national healthcare system, they can receive and disseminate timely information regarding national anti-epidemic measures; third, they store and provide anti-epidemic supplies (most of them are not allowed to be distributed in general channels) in a timely way; fourth, they are more familiar with the people and the environment of the area around the pharmacy than the other healthcare institutes; fifth, they have much easier access in terms of physical distance and business hours. In addition, community pharmacy that is contracted with the NHIB is particularly important for patients with chronic diseases to refill their choric prescriptions, especially in the epidemic season in Taiwan.
Theories that can be applied to explain health behavior are many; this study uses the health belief model (HBM) as a foundation to build the research framework of this study [
13]. Compared to other theories on health behavior research, the logic behind the HBM is clear and straightforward; it is easier to communicate with participants and researchers than in the others [
14].
The HBM was formulated with several constructs to predict a health behavior [
15]. Perceived susceptibility and perceived severity in the HBM are sometimes combined and termed perceived threat; the former refers to a person’s perception about the possibility of getting a disease, and the latter refers to the feeling about the seriousness of the medical and social consequences of contracting such a disease. Perceived threat provides energy, whereas net perceived benefit (benefit minus barrier) provides a preferred path [
16]. Perceived benefit refers to the benefits an action may bring to reduce the disease threat, whereas the perceived barrier refers to one’s belief of any negative outcomes accompanying the action. Self-efficacy was later included in 1988 as an additional predictor in HBM [
17], which was defined as one’s conviction of successfully performed actions required for the expected outcomes [
18]. HBM was then widely used in studies on disease precaution behaviors, such as disease prevention behaviors in varied contexts [
19,
20], including COVID-19 precautionary measures and associated behaviors [
21]. In short, as a study on disease prevention behavior, HBM is the optimal theory for the current research context. Study results from the current research can be used to dialogue with previous studies as far as the precautionary behavior is concerned [
22,
23].
Psychological tension, as noted in many psychological studies [
24,
25,
26], emerges when problems are aroused as a disruption to obstruct the expected routine of life. Tensions of this kind are problems that need to ease or be managed [
27,
28], and certain thinking and behaviors will be activated by the persons who perceived such tensions and problems [
29]. Health is one of humans’ major concerns in almost every culture as it is the core for life survival, and the epidemic can be easily perceived as a threat and tension to human health when it breaks out. As a result, as the HBM studies asserted, corresponding behaviors in response to solving the threats will then be motivated and activated [
6]. In the current research context, plenty of measures and instruments had been developed and suggested to prevent people from being infected by the pandemic of COVID-19. Vaccination, physical distancing, intensive hygiene, and strengthening human immunity are major streams of alternatives. The current research proposed that they are motivated to seek and evaluate the net benefits of each alternative including PSU in response to the threats of the epidemic.
The net benefit is the perceived benefits minus the perceived barriers of taking the recommended health action, which was termed as the “likelihood of action” as in previous studies [
11,
30]. Other than perceived threats and the likelihood of action of alternatives as predictors to the health behavior, the social learning theorist argued that vicarious learning is also an important role for individuals to activate a self-regulatory mechanism to learn a novel behavior or to change the current behavior without the trial and error process [
31,
32,
33], as the links between cognition and behavior can be straight and direct [
28,
34,
35].
The HBM-based studies added self-efficacy [
17,
36] as an additional variable and proved to have better explanatory capability [
30]. Self-efficacy refers to an individual’s judgments of the capabilities s/he has that are required to gain the expected performances [
32]. Self-efficacy is thus added to the HBM to cover the individual differences in the learning process, and as many HBM-based studies acclaimed, HBM with self-efficacy can better explain health promotion or disease prevention behaviors. We thus have a hypothesis based on the HBM as follows.
H1: The stronger the perceived threats, perceived likelihood of action, and self-efficacy, the stronger the intention of using the pharmacy service.
The current research was conducted to explain how the residents in the highly air-polluted area perceived the threats of COVID-19. Since residents of such areas may have been alerted to the impaired function of the respiratory system due to poor air quality, it is logical for these people to seek alternatives for health protection, such as revitalizing the immune system through PSU. As a result, the levels of perceived threats of COVID-19, perceived likelihood of actions, and PSU intention can be higher than in those people who were not exposed to air pollution. Since Siaogang exposed the most to air pollution among the five districts of the research, we therefore proposed a hypothesis as follows.
H2: Perceived threats, perceived likelihood of action, and pharmacy service utilization intention will be higher for people in Siaogang than those of other districts.
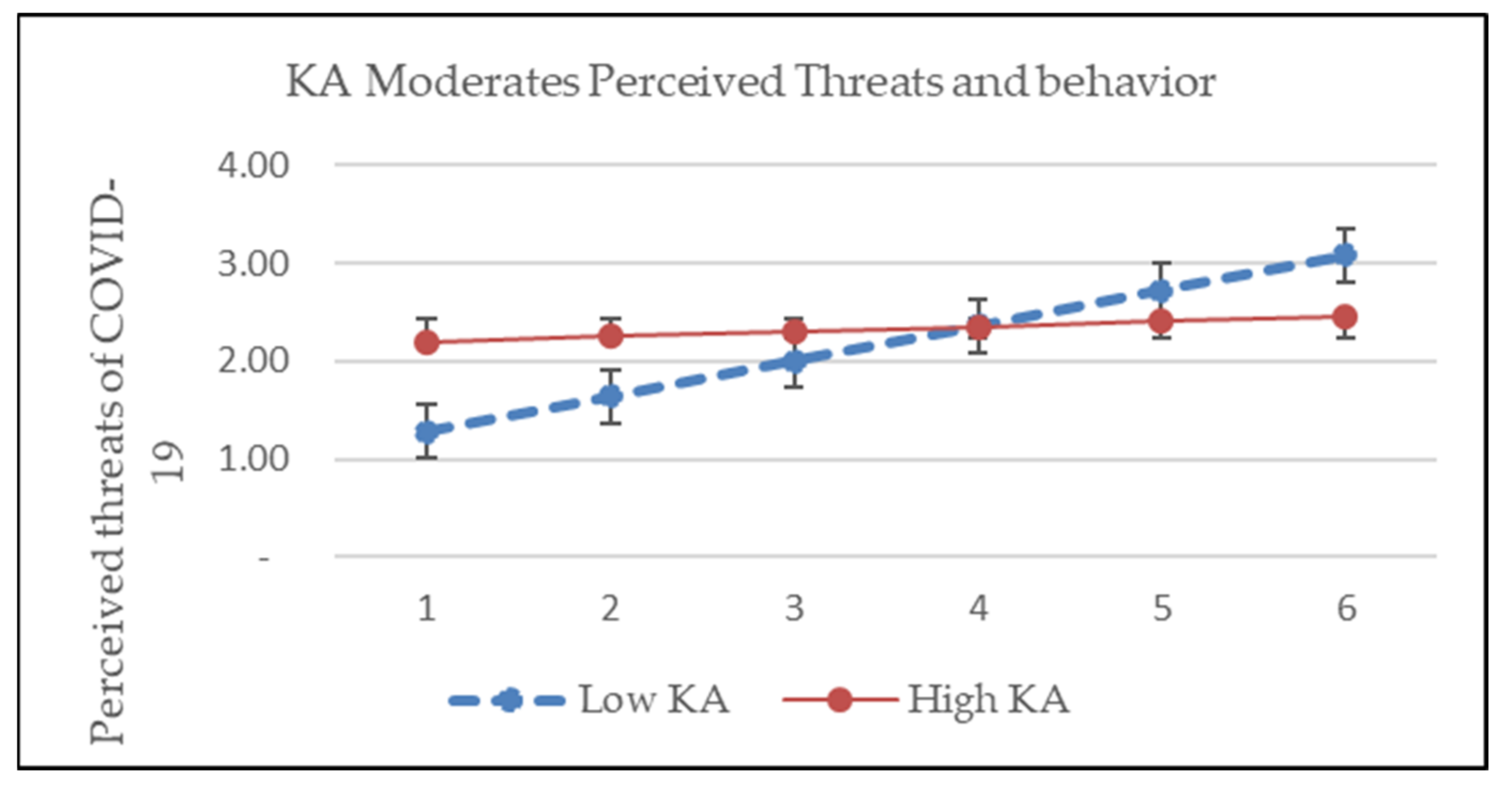
According to HBM, the threat of COVID-19 infection, and the benefits and barriers of specific measures in response to the threats are the main predictors of such behavior. This study believes that HBM predictors are originated or affected by personal subjective opinions. As bounded rationality theory suggested, personal rationality is limited by one’s own levels of knowledge. In other words, the individual’s knowledge and attitude (KA) regarding COVID-19 will affect the individual’s cognition of disease threats, the perceived benefits of the focus measure against the COVID-19, and the actions to be taken. Therefore, unlike some literature that suggested examining possible mediation and moderation between the core components of the HBM than exploring direct effects [
37], the current research attempts to include KA toward the threats as an additional factor in the model to expand our understanding in a different perspective. Since knowledge and attitude basically act as the foundation to motivate and shape human behavior, we thus proposed a hypothesis as follows.
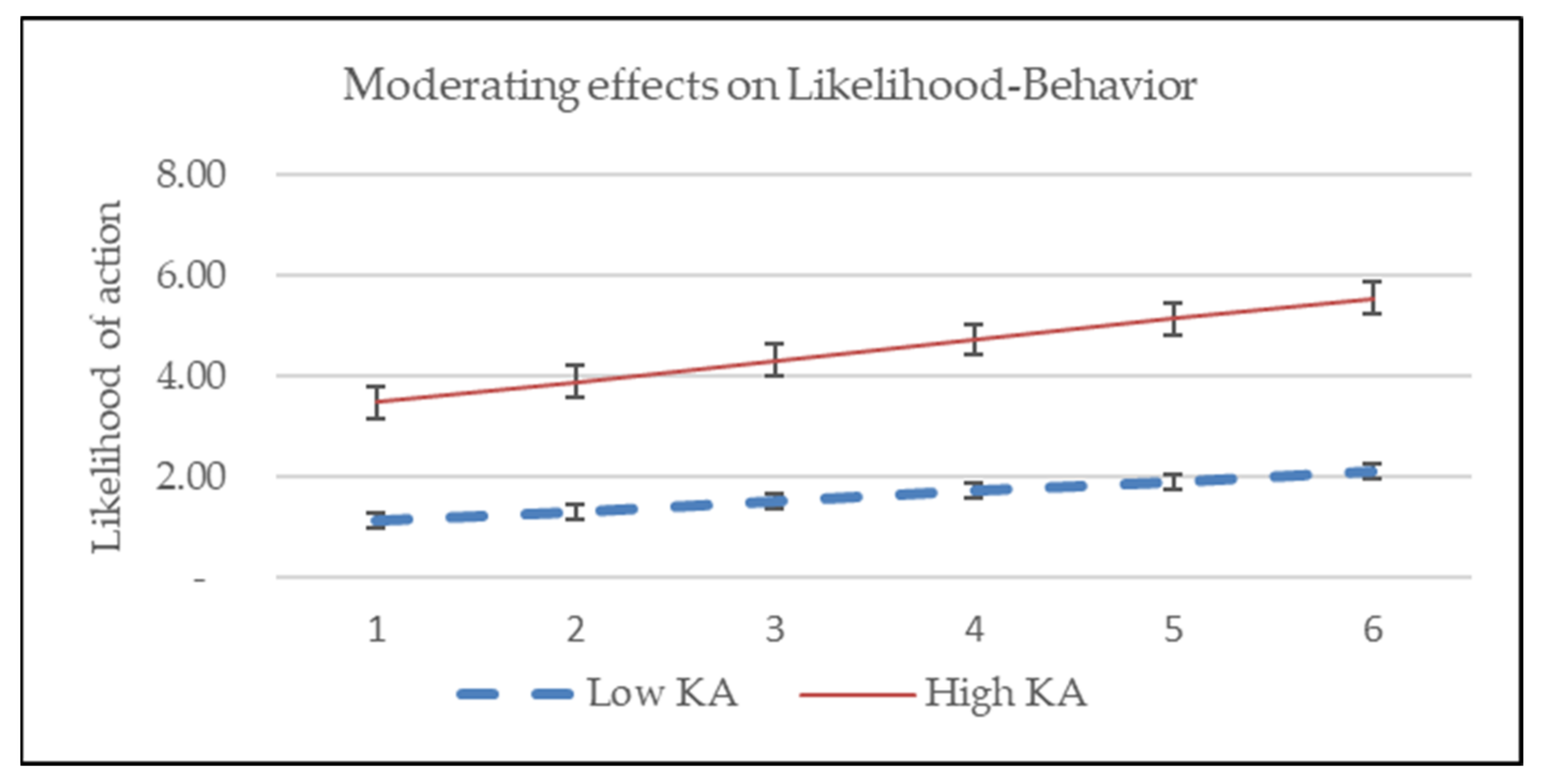
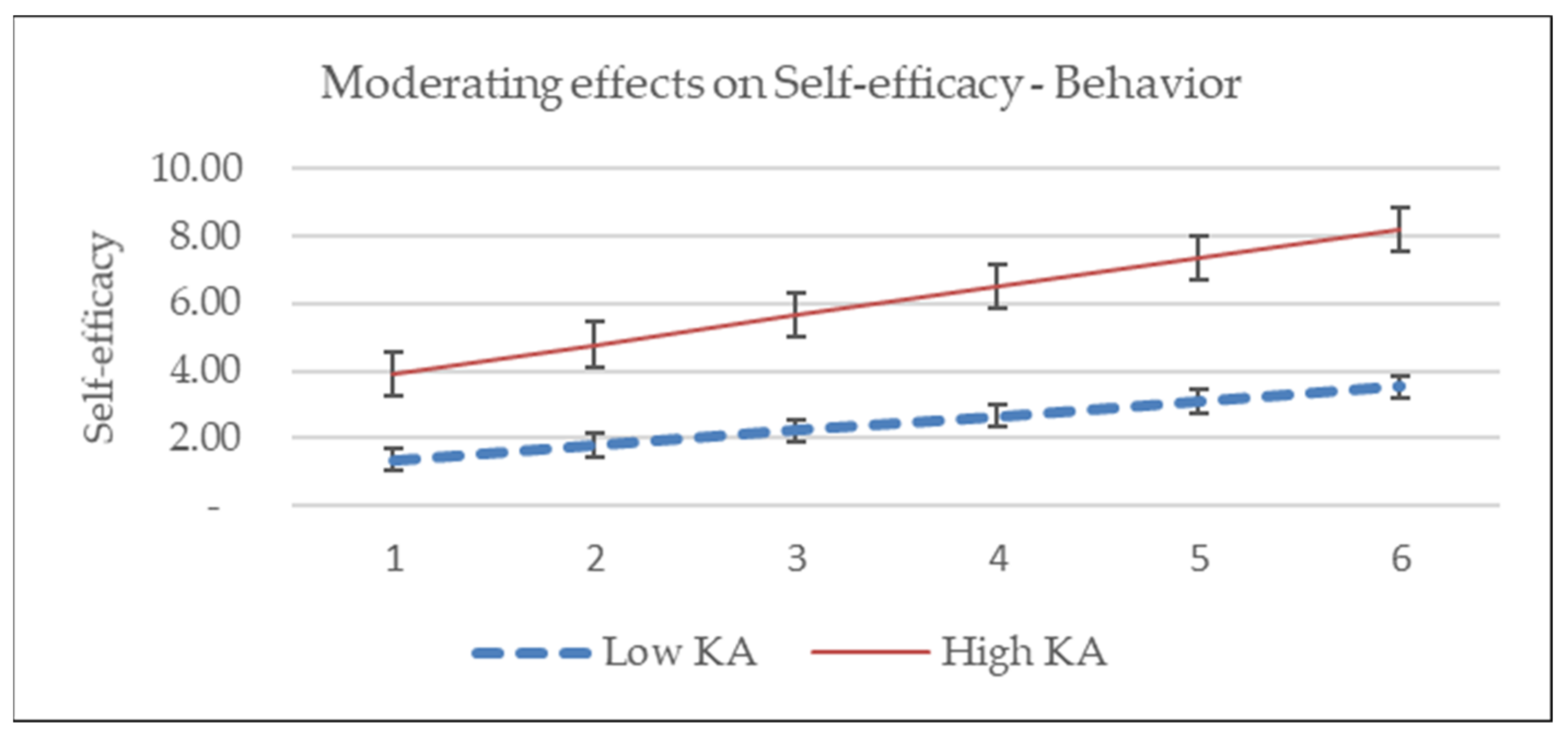
H3: Knowledge and attitude regarding COVID-19 moderate the relationship between perceived threat, net likelihood of action, self-efficacy, and pharmacy service utilization intention.
By accomplishing the purpose of the research, we wish to shed more light on how the knowledge and attitude regarding COVID-19 will affect the known relationship of HBM, in particular for the residents of highly air-polluted areas. In the meantime, it will also provide better insight into how people will react to protect their health when additional threats from the environment emerge.








{kind=link}
{kind=link}
{kind=link}
{kind=link}