
The Current Practice of Gradual Return to Work in Germany: A Qualitative Study Protocol


{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Workplace Health Management and Return to Work
1.2. Gradual Return to Work in Germany
1.2.1. Legal Aspects
1.2.2. Purpose
1.2.3. Outreach
1.2.4. Implementation
1.2.5. Effects
2. Methods and Design
2.1. Aim
2.2. Research Questions
- What experience and action-guiding knowledge do the affected employees, organisational stakeholders as well as external experts contribute to the planning and implementation of GRTW? How does this influence RTW in general?
- What do affected employees, organisational stakeholders as well as external experts experience as beneficial or as hindering within the GRTW process, and why?
- How do affected employees, organisational stakeholders as well as external experts describe and experience the decision-making within the GRTW process (e.g., GRTW design; step-by-step plan; underlying illness)?
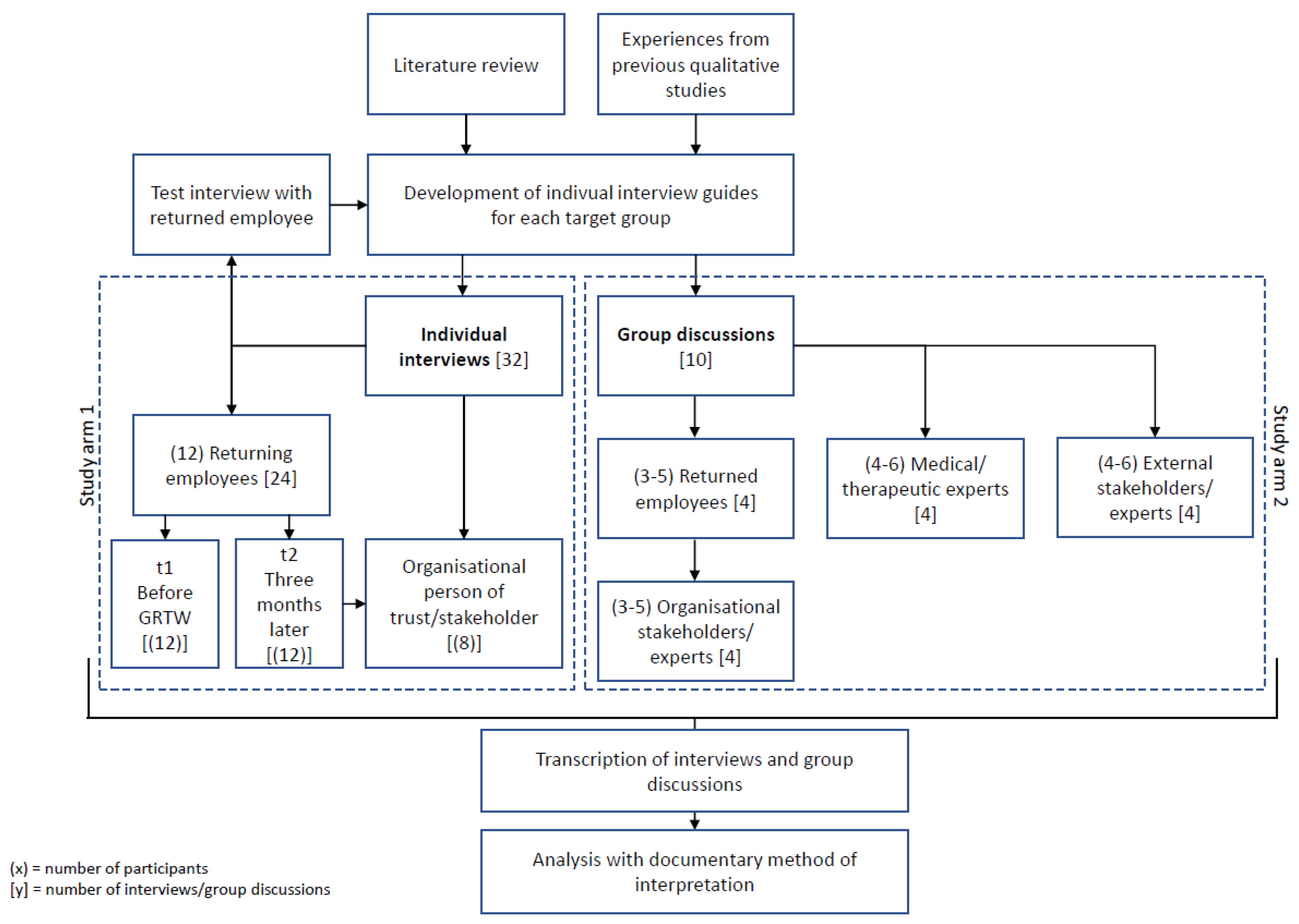
2.3. Study Design
2.4. Sample Profile
2.4.1. Interviews
- (a)
- 12 returning employees who are planning to return to work using GRTW after a period of sickness absence and between 18 and 60 years old.
- (b)
- Eight trusted persons from the same company of the interviewed employees who were proposed by the returning employee and who have accompanied GRTW of the employee referred to above.
2.4.2. Group Discussions
- (a)
- Four group discussions with three to five returned employees between 18 and 60 years old, who have returned to work via GRTW after a longer period of sickness absence at least once in the company they are currently employed at within the last three years of employment.
- (b)
- Four group discussions with three to five organisational experts and stakeholders who have long or intensive professional experience in the field of GRTW or RTW.
- (c)
- One group discussion with four to six external experts and stakeholders from GPI, GHI, integration services, and other services that support RTW and who have professional experience in the field of GRTW and/or RTW in their current position.
- (d)
- One group discussion with four to six external experts and stakeholders from medical and/or therapeutic healthcare, social work, occupational medicine, rehabilitation, and acute clinics.
2.5. Sample Selection and Recruitment Process
2.5.1. Interviews
2.5.2. Group Discussions
2.6. Data Collection
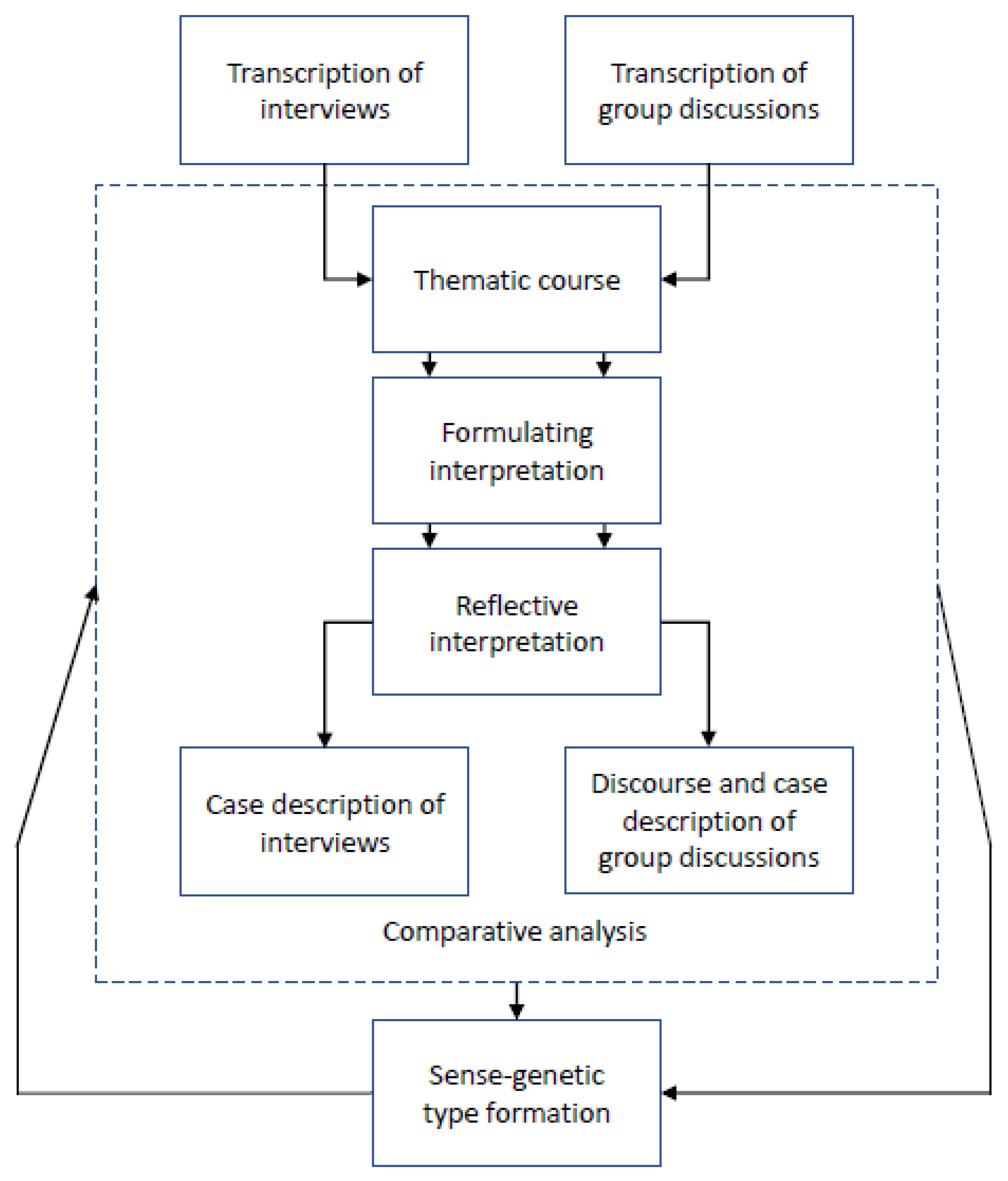
2.7. Analysis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Belin, A.; Dupont, C.; Oulès, L.; Kuipers, Y.; Fries-Tersch, E. Rehabilitation and Return to Work: Analysis Report on EU and Member States Policies, Strategies and Programmes; Report No.: 978-92-9240-925-8.4; European Agency for Safety and Health at Work: Luxembourg, 2016. [Google Scholar]
- OECD. OECD Employment Outlook 2019; OECD: Paris, France, 2019. [Google Scholar]
- OECD. Sickness, Disability and Work: Breaking the Barriers a Synthesis of Findings across OECD Countries; OECD: Paris, France, 2010. [Google Scholar]
- van Rijn, R.M.; Robroek, S.J.; Brouwer, S.; Burdorf, A. Influence of poor health on exit from paid employment: A systematic review. Occup. Env. Med. 2014, 71, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Kochskaemper, S. Gesetzliche Rentenversicherung wie lange arbeiten für ein stabiles Rentenniveau? In Statutory Pension Insurance How Long Work for a Stable Pension Level? IW-Kurzbericht, No. 27.2016; Institut der deutschen Wirtschaft Köln: Köln, Germany, 2016. [Google Scholar]
- Kochskaemper, S.; Pimpertz, J. Live Long and Prosper? Demographic Change and the Implications of Europe’s Pensions Crisis; Wilfried Martens Centre for European Studies: Brussels, Belgium, 2015. [Google Scholar]
- Malin, L.; Jansen, A.; Seyda, S.; Flake, R. Fachkräfteengpässe in Unternehmen. Fachkräftesicherung in Deutschland—Diese Potenziale gibt es noch. In Skilled Workforce Shortages in Companies. Securing Skilled Workers in Germany—This Potential Still Exists; Kompetenzzentrum Fachkräftesicherung: Köln, Germany, 2019. [Google Scholar]
- de Vroome, E.M.; Uegaki, K.; van der Ploeg, C.P.; Treutlein, D.B.; Steenbeek, R.; de Weerd, M.; van den Bossche, S.N. Burden of sickness absence due to chronic disease in the Dutch workforce from 2007 to 2011. J. Occup. Rehabil. 2015, 25, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Hoß, K.; Pomorin, N.; Reifferscheid, A.; Wasem, J. Arbeits- und Beschäftigungsfähigkeit vor dem Hintergrund des Demografischen Wandels. Workability and Employability against the Background of Demographic Change Version 1.0, IBES Diskussionsbeitrag, No. 200; Universität Duisburg-Essen, Institut für Betriebswirtschaft und Volkswirtschaft (IBES): Essen, Germany, 2013. [Google Scholar]
- Brussig, M. Demografischer Wandel, Alterung und Arbeitsmarkt in Deutschland. Demographic Change, Aging and the Labor Market in Germany. Kölner Z. Für Soziologie Und Soz. 2015, 67, 295–324. [Google Scholar] [CrossRef]
- Windscheid, E.C. Reintegrationskonflikte bei der Rückkehr an den Arbeitsplatz nach psychischer Erkrankung. Problemfelder und Lösungsstrategien im BEM aus Sicht von Betroffenen, Kollegen und Führungskräften. Reintegration conflicts when returning to work after mental illness. Problem areas and solution strategies in BEM from the perspective of those affected, colleagues and managers. Z. Arb. Wiss. 2019, 73, 261–273. [Google Scholar] [CrossRef]
- Wrage, W.; May-Schmidt, J. Betriebliches Gesundheitsmanagement und Betriebliches Arbeitsschutzmanagement. In Workplace Health Management and Workplace Health and Safety Management; Vom Stein, J., Rothe, I., Schlegel, R., Eds.; Gesundheitsmanagement und Krankheit im Arbeitsverhältnis; Verlag C.H.Beck: München, Germany, 2021; pp. 385–422. [Google Scholar]
- Hoge, A.; Ehmann, A.T.; Rieger, M.A.; Siegel, A. Caring for Workers’ Health: Do German Employers Follow a Comprehensive Approach Similar to the Total Worker Health Concept? Results of a Survey in an Economically Powerful Region in Germany. Int. J. Environ. Res. Public Health 2019, 16, 726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bamberg, E.; Ducki, A.; Metz, A.-M. Handlungsbedingungen von Gesundheitsförderung und Gesundheitsmanagement. Action Conditions of Health Promotion and Health Management; Bamberg, E., Ducki, A., Metz, A.-M., Eds.; Gesundheitsförderung und Gesundheitsmanagement in der Arbeitswelt; Ein Handbuch; Hogrefe Verlag: Göttingen, Germany, 2011; pp. 109–122. [Google Scholar]
- Kausto, J.; Miranda, H.; Martimo, K.P.; Viikari-Juntura, E. Partial sick leave--review of its use, effects and feasibility in the Nordic countries. Scand. J. Work. Env. Health. 2008, 34, 239–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stergiou-Kita, M.; Pritlove, C.; van Eerd, D.; Holness, L.D.; Kirsh, B.; Duncan, A.; Jones, J. The provision of workplace accommodations following cancer: Survivor, provider, and employer perspectives. J. Cancer Surviv. 2016, 10, 489–504. [Google Scholar] [CrossRef]
- Sikora, A.; Schneider, G.; Stegmann, R.; Wegewitz, U. Returning to work after sickness absence due to common mental disorders: Study design and baseline findings from an 18 months mixed methods follow-up study in Germany. BMC Public Health 2019, 19, 1653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loerbroks, A.; Scharf, J.; Angerer, P.; Spanier, K.; Bethge, M. the prevalence and determinants of being offered and accepting operational management services—A cohort study. Int. J. Environ. Res. Public Health 2021, 18, 2158. [Google Scholar] [CrossRef] [PubMed]
- Nebe, K. Die stufenweise Wiedereingliederung. Sicherung der Erwerbsteilhabe durch komplementäres Arbeits- und Sozialrecht. Gradual return to work. Securing employment through complementary labor and social law. Die Soz. 2015, 62, 125–134. [Google Scholar]
- Webendörfer, S.; Frey, G. Die stufenweise Wiedereingliederung als wirksames Instrument der Tertiärprävention. Gradual retun to work as an effective tool of tertiary prevention. ASU Arb. Soz. Umw. 2017, 52, 366–370. [Google Scholar]
- Federal Ministry of Labour and Social Affairs. Social Security at a Glance 2020; Report No.: A 998; Federal Ministry of Labour and Social Affairs: Bonn, Germany, 2020.
- Schian, M.; Thimmel, R. Betriebliches Eingliederungsmanagement. Operational Integration Management. ASU Arb. Soz. Umw. 2017, 12, 877–886. [Google Scholar]
- Stegmann, R.; Schröder, U.B.; Schulz, I.L. Return to Work after Sickness Absence Due to Common Mental Disorders from the Employees’ Perspective. Findings of the Qualitative Study Part F 2386 of a Mixed-Methods Follow-Up Study Regarding Paths Into Crisis and Return to Work; BAuA Bericht; Bundesanstalt für Arbeitsschutz und Arbeitsmedizin: Dortmund, Berlin, Dresden, Germany, 2021. [Google Scholar]
- Bundesarbeitsgemeinschaft für Rehabilitation e.V. Stufenweise Wiedereingliederung in den Arbeitsprozess—Arbeitshilfe. In Gradual Return Into the Work Process—Work Aid; Frankfurt am Main: Bundesarbeitsgemeinschaft für Rehabilita-tion (BAR) e.V: Frankfurt, Germany, 2019. [Google Scholar]
- Faßmann, H.; Oertel, M.; Wasilewski, R. Konzepte, Erfahrungen und Probleme im Bereich der stufenweisen Wiedereingliederung in den Arbeitsprozeß. Concepts, experiences and problems in the field of gradual return into the work process. Das Offentl. Gesundh. 1991, 53, 115–120. [Google Scholar]
- Stegmann, R.; Schroeder, U.B. Anders Gesund—Psychische Krisen in der Arbeitswelt. Prävention, Return-to-Work und Eingliederungsmanagement. Differently Healthy—Mental Crises in the World of Work. Prevention, Return-to-Work and Integration Management; Springer Fachmedien Wiesbaden GmbH: Wiesbaden, Germany, 2018. [Google Scholar]
- Blonk, R.W.B.; Brenninkmeijer, V.; Lagerveld, S.E.; Houtman, I.L.; Houtman, D. Return to work: A comparison of two cognitive behavioural interventions in cases of workrelated psychological complaints among the selfemployed. Work. Stress 2006, 20, 129–144. [Google Scholar] [CrossRef]
- Hillert, A.; Weber, A.; Köllner, V. Stufenweise Wiedereingliederung in den Arbeitsprozess. Gradual return into the work process. Psychother. Im Dialog 2016, 17, 69–73. [Google Scholar]
- Weber, A.; Peschkes, L.; Boer, W.D. Return to Work—Arbeit für Alle. Grundlagen der Beruflichen Reintegration. Return to Work—Work for Everyone. Basics of Professional Reintegration; Gentner Verlag: Stuttgart, Germany, 2014. [Google Scholar]
- Ducki, A.; Bamberg, E.; Metz, A.-M. Prozessmerkmale von Gesundheitsförderung und Gesundheitsmanagement. Process Characteristics of Health Promotion and Health Management; Bamberg, E., Ducki, A., Metz, A.-M., Eds.; Gesundheitsförderung und Gesundheitsmanagement in der Arbeitswelt; Ein Handbuch; Hogrefe Verlag: Göttingen, Germany, 2011; pp. 135–156. [Google Scholar]
- Niehaus, M.; Marfels, B.; Vater, G.; Magin, J.; Werkstetter, E. Betriebliches Eingliederungsmanagement: Studie zur Umsetzung des Betrieblichen Eingliederungsmanagements Nach § 84 Abs. 2 SGB IX. Operational Integration Management: Study on the Implementation of Operational Integration Management According to § 84 Paragraph 2 SGB IX; Report No.: FB374.71; Bundesministerium für Arbeit und Soziales: Köln, Germany, 2008. [Google Scholar]
- Schmid, L.; Jankowiak, S.; Kaluscha, R.; Krischak, G. Nachsorgeempfehlungen zur stufenweisen Wiedereingliederung: Inwieweit erklären Rehabilitandenmerkmale die bestehenden Unterschiede zwischen den Einrichtungen? Follow-up recommendations for gradual return to work: To what extent do rehabilitee characteristics explain the existing differences between the institutions? Rehabil. Stuttg. 2016, 55, 167–174. [Google Scholar] [CrossRef]
- Bürger, W.; Streibelt, M. Wonach richtet sich die Inanspruchnahme von stufenweiser Wiedereingliederung zu Lasten der gesetzlichen Rentenversicherung? Erste Ergebnisse der STW-Kohortenstudie. What Determines the Participation in Stepwise Occupational Reintegration on Behalf of the German Pension Insurance? Results of the “SOR Cohort Study”. Rehabilitation 2015, 54, 10–15. [Google Scholar] [CrossRef]
- Bürger, W.; Glaser-Möller, N.; Kulick, B.; Pallenberg, C.; Stapel, M. Stufenweise Wiedereingliederung zulasten der gesetzlichen Rentenversicherung—Ergebnisse umfassender Routinedatenanalysen und teilnehmerbefragungen. Stepwise Occupational Reintegration under the German Pension Insurance Scheme—Results of Comprehensive Routine Data Analyses and Participants Surveys. Rehabilitation 2011, 50, 74–85. [Google Scholar] [CrossRef]
- Schneider, U.; Linder, R.; Verheyen, F. Long-term sick leave and the impact of a graded return-to-work program: Evidence from Germany. Eur. J. Health Econ. 2016, 17, 629–643. [Google Scholar] [CrossRef]
- Bürger, W. Entwicklung von Zugangskriterien zum Effektiven und Kostendeckenden Einsatz Ei-Ner STW zu Lasten der Deutschen Rentenversicherung. Ergebnisse von Routinedatenanalysen und Versichertenbefragungen zur Stufenweisen Wiedereingliederung. Development of Access Criteria for Effective and Cost-Covering Use of an STW at the Expense of the German Pension Insurance. Results of Routine Data Analysis and Surveys of Insured Persons for Gradual Return to Work; Report No.: Ab-schlussbericht zum Projekt der DRV BUND: AZ 8011—106—31/31.106; Fbg forschung und beratung im gesundheitswesen: Karlsruhe, Germany, 2016. [Google Scholar]
- Bethge, M. Effects of graded return-to-work: A propensity-score-matched analysis. Scand. J. Work. Env. Health 2016, 42, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Streibelt, M.; Burger, W.; Nieuwenhuijsen, K.; Bethge, M. Effectiveness of graded return to work after multimodal rehabilitation in patients with mental disorders: A propensity score analysis. J. Occup. Rehabil. 2018, 28, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Bürger, W.; Kluth, W.; Koch, U. Stufenweise Wiedereingliederung zu Lasten der Gesetzlichen Ren-Tenversicherung—Häufigkeit, Indikationsstellung, Einleitung, Durchführung, Bewertung und Ergebnisse. Ergebnisse von Routinedatenanalysen und Versichertenbefragungen zur stufenweisen Wiedereingliederung. Gradual Return to Work at the Expense of the Statutory Pension Insurance—Frequency, Indication, Initiation, Implementation, Evaluation and Results. Results of Routine Data Analyzes and Surveys of Insured Persons for Gradual Return to Work; Abschlussbericht. 77; Universitätsklinikum Hamburg-Eppendorf; fbg forschung und beratung im gesundheitswesen: Karlsruhe, Germany, 2008. [Google Scholar]
- Bürger, W.; Streibelt, M. Wer profitiert von stufenweisen Wiedereingliederungen zu Lasten der Deutschen Rentenversicherung? Ergebnisse einer Kohortenstudie. Stepwise Occupational Reintegration under the German Pension Insurance Scheme—Results of Comprehensive Routine Data Analyses and Participants Surveys. Rehabilitation 2019, 58, 163–171. [Google Scholar] [CrossRef]
- Stergiou-Kita, M.; Grigorovich, A.; Tseung, V.; Milosevic, E.; Hebert, D.; Phan, S.; Jones, J. Qualitative meta-synthesis of survivors’ work experiences and the development of strategies to facilitate return to work. J. Cancer Surviv. 2014, 8, 657–670. [Google Scholar] [CrossRef] [PubMed]
- Dewa, C.S.; Hoch, J.S.; Loong, D.; Trojanowski, L.; Bonato, S. Evidence for the cost-effectiveness of return-to-work interventions for mental illness related sickness absences: A systematic literature review. J. Occup. Rehabil. 2021, 1, 26–40. [Google Scholar] [CrossRef] [PubMed]
- Maas, E.T.; Koehoorn, M.; McLeod, C.B. Descriptive epidemiology of gradual return to work for workers with a work-acquired musculoskeletal disorder in British Columbia, Canada. J. Occup. Environ. Med. 2020, 62, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Gray, S.E.; Hassani-Mahmooei, B.; Kendall, E.; Cameron, I.D.; Kenardy, J.; Collie, A. Factors associated with graduated return to work following injury in a road traffic crash. J. Transp. Health 2018, 10, 167–177. [Google Scholar] [CrossRef]
- van Vilsteren, M.; van Oostrom, S.H.; de Vet, H.C.; Franche, R.L.; Boot, C.R.; Anema, J.R. Workplace interventions to prevent work disability in workers on sick leave. Cochrane Database Syst Rev. 2015, 10, CD006955. [Google Scholar] [CrossRef] [PubMed]
- Franche, R.L.; Cullen, K.; Clarke, J.; Irvin, E.; Sinclair, S.; Frank, J. Workplace-based return-to-work interventions: A systematic review of the quantitative literature. J. Occup. Rehabil. 2005, 15, 607–631. [Google Scholar] [CrossRef]
- Krause, N.; Dasinger, L.K.; Neuhauser, F. Modified work and return to work: A review of the literature. J. Occup. Rehabil. 1998, 8, 113–139. [Google Scholar] [CrossRef]
- Mikkelsen, M.B.; Rosholm, M. Systematic review and meta-analysis of interventions aimed at enhancing return to work for sick-listed workers with common mental disorders, stress-related disorders, somatoform disorders and personality disorders. Occup. Environ. Med. 2018, 75, 675–686. [Google Scholar] [CrossRef]
- Andrén, D. Does part-time sick leave help individuals with mental disorders recover lost work capacity? J. Occup. Rehabil. 2014, 24, 344–360. [Google Scholar] [CrossRef] [PubMed]
- Høgelund, J.; Holm, A.; McIntosh, J. Does graded return-to-work improve sick-listed workers’ chance of returning to regular working hours? J. Health Econ. 2010, 29, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Viikari-Juntura, E.; Leinonen, T.; Virta, L.J.; Hiljanen, I.; Husgafvel-Pursiainen, K.; Autti-Rämö, I.; Rissanen, P.; Burdorf, A.; Solovieva, S. Early part-time sick leave results in considerable savings in social security costs at national level: An analysis based on a quasi-experiment in Finland. Scand. J. Work Environ. Health 2019, 2, 203–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoefsmit, N.; Houkes, I.; Nijhuis, F.J. Intervention characteristics that facilitate return to work after sickness absence: A systematic literature review. J. Occup. Rehabil. 2012, 22, 462–477. [Google Scholar] [CrossRef] [Green Version]
- Haugli, L.; Maeland, S.; Magnussen, L.H. What facilitates return to work? Patients’ experiences 3 years after occupational rehabilitation. J. Occup. Rehabil. 2011, 21, 573–581. [Google Scholar] [CrossRef] [Green Version]
- Esteban, E.; Coenen, M.; Ito, E.; Gruber, S.; Scaratti, C.; Leonardi, M.; Roka, O.; Vasilou, E.; Muñoz-Murillo, A.; Ávila, C.C.; et al. Views and experiences of persons with chronic diseases about strategies that aim to integrate and re-integrate them into work: A systematic review of qualitative studies. Int. J. Env. Res. Public Health 2018, 15, 1022. [Google Scholar] [CrossRef] [Green Version]
- Kools, L.; Koning, P. Graded Return-to-Work as a Stepping Stone to Full Work Resumption; Report No.: IZA DP No. 11471; IZA Institute of Labor Economics: Bonn, Germany, 2018. [Google Scholar]
- Bouffard, J.; Durand, M.J.; Coutu, M.F. Adaptation of a Guide to Equip Employers to Manage the Gradual Return to Work of Individuals with a Musculoskeletal Disorder. J. Occup. Rehabil. 2019, 29, 625–635. [Google Scholar] [CrossRef]
- Helfferich, C. Die Qualität Qualitativer Daten. Manual für Die Durchführung Qualitativer Interviews. The Quality of Qualitative Data. Manual for Conducting Qualitative Interviews; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2011. [Google Scholar]
- Nohl, A.-M. Interview und Dokumentarische Methode. Anleitungen für Die Forschungspraxis. Interview and Documentary Method. Guidelines for Research Practice; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2017. [Google Scholar]
- Flick, U.; von Kardorff, E.; Uwe Flick Steinke, I. Wasist Qualitative Forschung? Einleitung und Überblick. What is Qualitative Research? Introduction and Overview; Flick, U., von Kardorff, E., Uwe, F., Steinke, I., Eds.; Qualitative Forschung. Ein Handbuch. Rowohlts Enzyklopädie; Rowohlt-Taschenbuch Verlag: Reinbek, Germany, 2010; pp. 13–29. [Google Scholar]
- Schütze, F. Kognitive Figuren des Autobiographischen Stegreiferzählens. Cognitive Figures of Autobiographical Impromptu Storytelling; Kohli, M., Robert, G., Eds.; Biographie und soziale Wirklichkeit: Neue Beiträge und Forschungsperspektiven; Metzler: Stuttgart, Germany, 1984; pp. 78–117. [Google Scholar]
- Küsters, I. Narratives Interview. Handbuch Methoden der Empirischen Sozialforschung. Handbook of Methods in Empirical Social Research; Baur, N., Blasius, J., Eds.; Springer: Wiesbaden, Germany, 2014; pp. 687–693. [Google Scholar]
- Kleemann, F.; Kraehnke, U.; Matuschek, I. Interpretative Sozialforschung. Eine Einführung in Die Praxis Des Interpretierens. Interpretive Social Research. An introduction to the Practice of Interpreting; Springer: Wiesbaden, Germany, 2013. [Google Scholar]
- Bohnsack, R. Rekonstruktive Sozialforschung: Einführung in Qualitative Methoden. Reconstructive Social Research: Introduction to Qualitative Methods; Verlag Barbara Budrich UTB: Stuttgart, Germany, 2007. [Google Scholar]
- Liebig, B.; Nentwig-Gesemann, I. Gruppendiskussion. Group discussions. In Handbuch Methoden der Organisationsforschung: Quantitative und Qualitative Methoden; Kuehl, S., Strodtholz, P., Taffertshofer, A., Eds.; Springer: Wiesbaden, Germany, 2009; pp. 102–123. [Google Scholar]
- Denzin, N.K. The Research Act: A Theoretical Introduction to Sociological Methods; McGraw-Hill Inc.: New York, NY, USA, 1978. [Google Scholar]
- Thurmond, V.A. The point of triangulation. J. Nurs. Scholarsh. 2001, 33, 253–258. [Google Scholar] [CrossRef]
- Breuer, F.; Muckel, P.; Dieris, B. Reflexive Grounded Theory. Eine Einführung für Die Forschungspraxis. Reflexive Grounded Theory. An Introduction to Research Practice; Springer: Wiesbaden, Germany, 2019. [Google Scholar]
- Strauss, A.; Corbin, J.M. Basics of Qualitative Research: Grounded Theory Procedures and Techniques; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1990. [Google Scholar]
- Kruse, J. Qualitative Interviewforschung. Ein integrativer Ansatz. Qualitative Interview Research. An Integrative Approach; Beltz Juventa: Weinheim, Germany; Basel, Switzerland, 2015. [Google Scholar]
- WAI-Netzwerk Deutschland. Wie Steht es um Ihre Arbeitsfähigkeit? WAI-Fragebogen & Auswertung (Kurzversion). How is Your Workability? WAI Questionnaire & Evaluation (Short Version); Institut für Arbeitsfähigkeit: Mainz, Germany, 2017. [Google Scholar]
- Bürger, W.; Deck, R.; Raspe, H.; Koch, U. SIBAR“ Screening-Instrument Beruf und Arbeit in der Rehabilitation. Entwicklung und Implementierungsmöglichkeiten Eines Generischen Screening-Instruments zur Identifikation von Beruflichen Problemlagen und des Bedarfes an Berufsorientierten und Beruflichen Rehabilitationleistungen. Abschlussbericht. “SIBAR” Screening Instrument for Occupation and Work in Rehabilitation. Development and Implementation Options of a Generic Screening Instrument to Identify Professional Problems and the Need for Job-Oriented and Professional Rehabilitation Services; Fbg Forschung und Beratung im Gesundheitswesen; Universitätsklinikum Schleswig-Holstein: Karlsruhe, Lübeck, Germany, 2007. [Google Scholar]
- Lagerveld, S.E.; Blonk, R.W.B.; Brenninkmeijer, V.; Schaufeli, W.B. Return to work among employees with mental health problems: Development and validation of a self-efficacy questionnaire. Work Stress 2010, 24, 359–375. [Google Scholar] [CrossRef] [Green Version]
- Bohnsack, R. Qualitative Evaluationsforschung und Dokumentarische Methode. Qualitative evaluation research and Documentary Method. In Dokumentarische Evaluationsforschung. Theoretische Grundlagen und Beispiele aus der Praxis. Opladen; Bohnsack, R., Nentwig-Gesemann, I., Eds.; Verlag Barbara Budrich: Farmington Hills, MI, USA, 2010; pp. 23–62. [Google Scholar]
- Bohnsack, R. Documentary method and group discussions. In Qualitative Analysis and Documentary Method in International Educational Research; Bohnsack, R., Pfaff, N., Weller, W., Eds.; Barbara Budrich Publishers: Opladen, Germany; Farmington Hills, MI, USA, 2010; pp. 99–124. [Google Scholar]
- Bourdieu, P. Entwurf Einer Theorie der Praxis—Auf der Ethnologischen Grundlage der Kabylischen Gesellschaft. Outline of a Theory of Practice—On the Ethnological Basis of Kabyle Society; Droz S. A.: Genf, Switzerland, 1972. [Google Scholar]
- Mannheim, K. Strukturen des Denkens. Structures of Thinking, 2nd ed.; Suhrkamp Verlag: Berlin, Germany, 1980. [Google Scholar]
- Bohnsack, R.; Nohl, A.-M. Exemplarische Textinterpretation: Die Sequenzanalyse der Dokumentarischen Methode. Exemplary text interpretation: The sequence analysis of the documentary method. In Die Dokumentarische Methode und ihre Forschungspraxis; Bohnsack, R., Nentwig-Gesemann, I., Nohl, A.-M., Eds.; Verlag für Sozialwissenschaften; Spinger: Wiesbaden, Germany, 2013; pp. 325–329. [Google Scholar]
- Bohnsack, R.; Pfaff, N.; Weller, W. Qualitative Analysis and Documentary Method in International Educational Research; Barbara Budrich Publishers: Opladen, Germany; Farmington Hills, MI, USA, 2010; pp. 7–38. [Google Scholar]
- Nohl, A.-M. Komparative Analyse. Comparative analysis. In Die Dokumentarische Methode und Ihre Forschungspraxis; Bohnsack, R., Nentwig-Gesemann, I., Nohl, A.-M., Eds.; Verlag für Sozialwissenschaften; Spinger: Wiesbaden, Germany, 2013; pp. 271–293. [Google Scholar]
- Bohnsack, R.H.; Hoffmann, N.F.; Nentwig-Gesemann, I. Typenbildung und Dokumentarische Methode. Type formation and Documentary Method. In Jahrbuch Dokumentarische Methode. 1/2019; Amling, S., Geimer, A., Schondelmayer, A.-C., Stuetzel, K., Thomsen, S., Eds.; Centrum für Qualitative Evaluations und Sozialforschung e.V. (ces): Berlin, Germany, 2019; pp. 17–50. [Google Scholar]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulz, I.L.; Stegmann, R.; Wegewitz, U.; Bethge, M. The Current Practice of Gradual Return to Work in Germany: A Qualitative Study Protocol. Int. J. Environ. Res. Public Health 2022, 19, 3740. https://doi.org/10.3390/ijerph19063740
Schulz IL, Stegmann R, Wegewitz U, Bethge M. The Current Practice of Gradual Return to Work in Germany: A Qualitative Study Protocol. International Journal of Environmental Research and Public Health. 2022; 19(6):3740. https://doi.org/10.3390/ijerph19063740
Chicago/Turabian StyleSchulz, Inga L., Ralf Stegmann, Uta Wegewitz, and Matthias Bethge. 2022. "The Current Practice of Gradual Return to Work in Germany: A Qualitative Study Protocol" International Journal of Environmental Research and Public Health 19, no. 6: 3740. https://doi.org/10.3390/ijerph19063740