
Depressive Symptoms and Their Associated Factors in Vocational–Technical School Students during the COVID-19 Pandemic

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Type
2.2. Context
2.3. Participants
2.4. Data Collection Procedure
2.5. Instruments
2.5.1. Sociodemographic- and COVID-19-Pandemic-Related Variables
2.5.2. Behavioral Habits
- (A).
- Eating habits: Feeling hungry due to lack of food in the last seven days; consumption of fruits, vegetables and soda in the last seven days.
- (B).
- Psychoactive substance use: Tobacco smoking (smoked at least once; frequency of smoking in the last 30 days); alcohol drinking (drank at least once; frequency of drinking in the last 30 days, experienced getting drunk at least once); illicit drug use, including marijuana, cocaine, and crack (used at least once; frequency of use in the last 30 days).
- (C).
- Risky sexual behavior: Prior sexual intercourse; age at first instance of sexual intercourse; number of sexual partners in lifetime.
- (D).
- Physical activity level: Self-reported physical activity was assessed using the short version of the International Physical Activity Questionnaire (IPAQ—short version), validated for Brazilian adolescents [48]. The IPAQ—short version assesses the frequency (days/week) and duration (minutes/day) of walking, and moderately and vigorously exercising, in the last seven days. The physical activity level in the participants was classified as “low” (not meeting the criteria for the “moderate” or “high” categories); “moderate” (at least 20 min of vigorous physical activity three or more days/week; at least 30 min of moderate physical activity or walking five or more days/week; any combination of walking, moderate, or vigorous physical activity reaching at least 600 metabolic equivalent of task (MET) minutes/week at least five days/week); and “high” (vigorous physical activity reaching at least 1500 MET minutes/week at least three days/week; any combination of walking, moderate, or vigorous physical activity reaching at least 3000 MET minutes/week at least seven days/week) [49].
2.5.3. Quality of Life
2.5.4. Depressive Symptoms
2.6. Data Analysis
3. Results
3.1. Sample Description
3.2. Depressive Symptoms, Behavioral Habits and QoL in Students
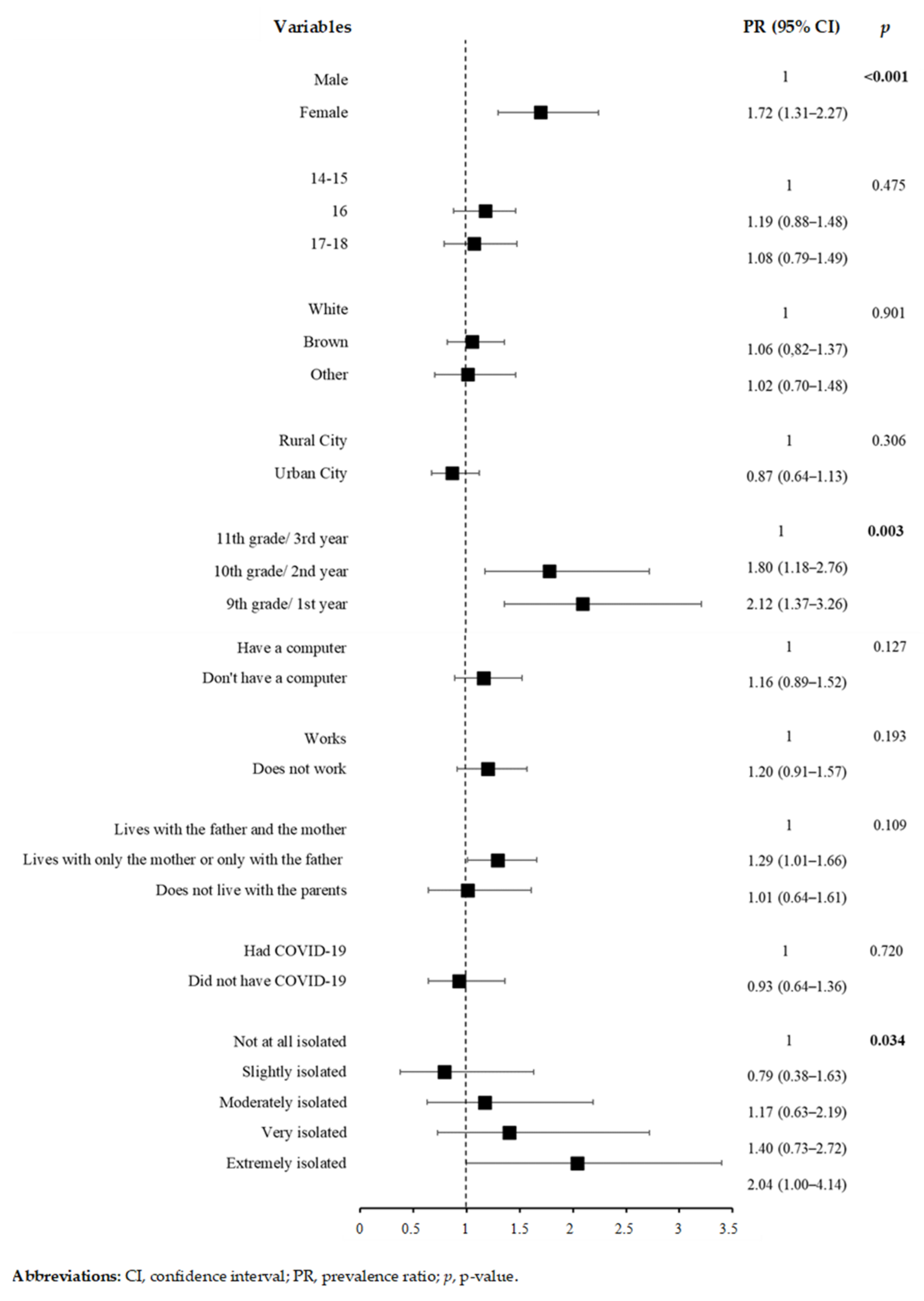
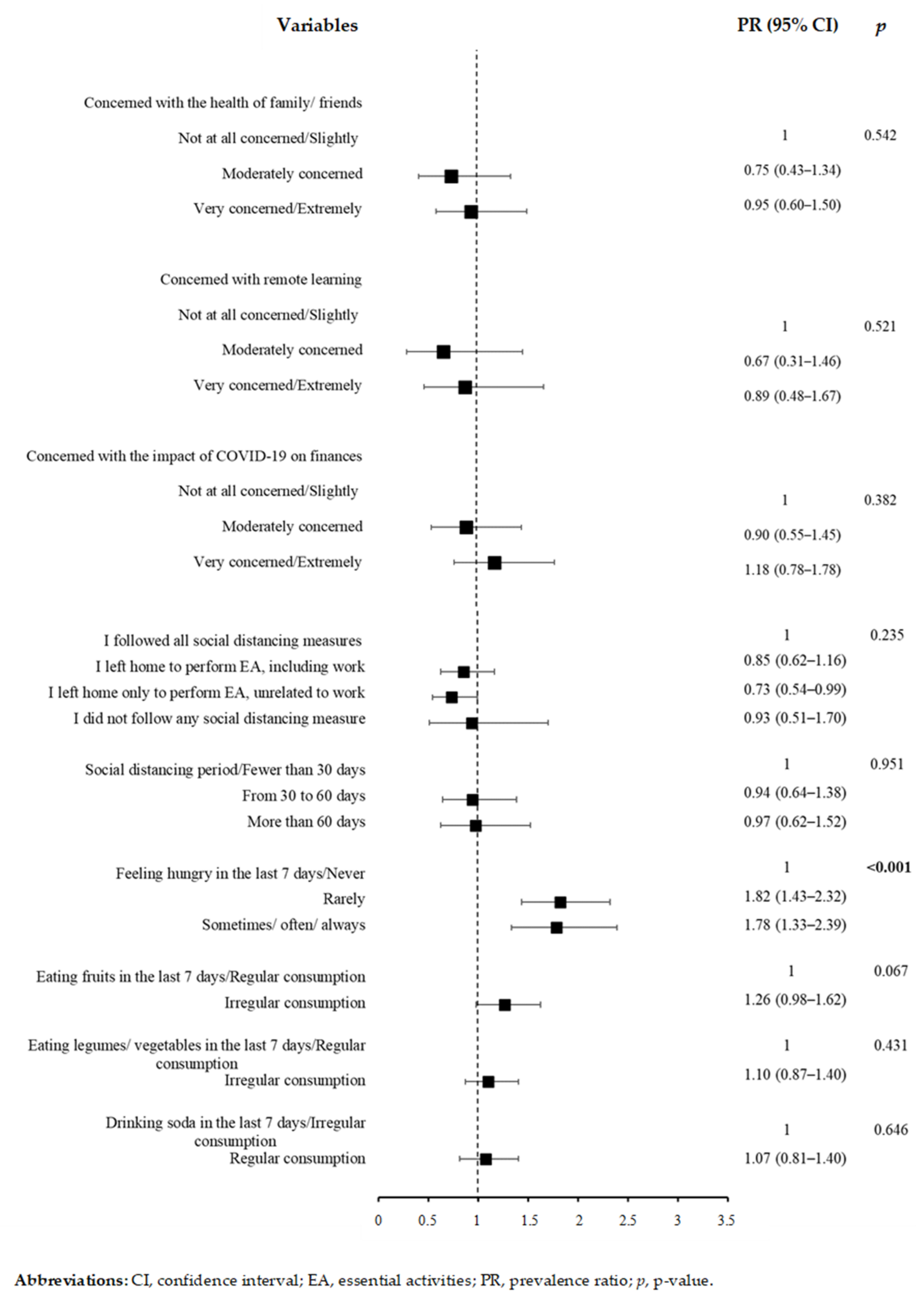
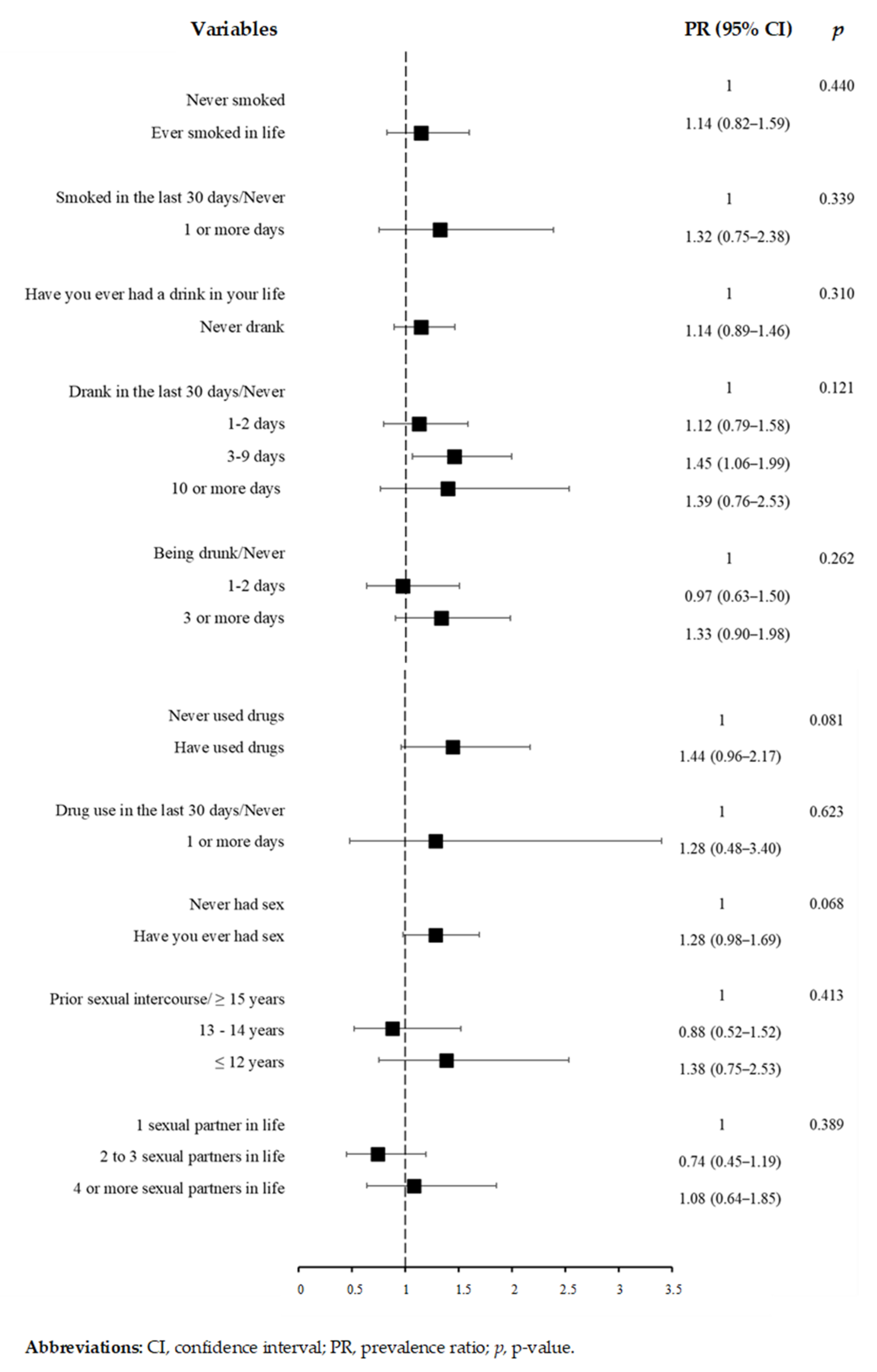
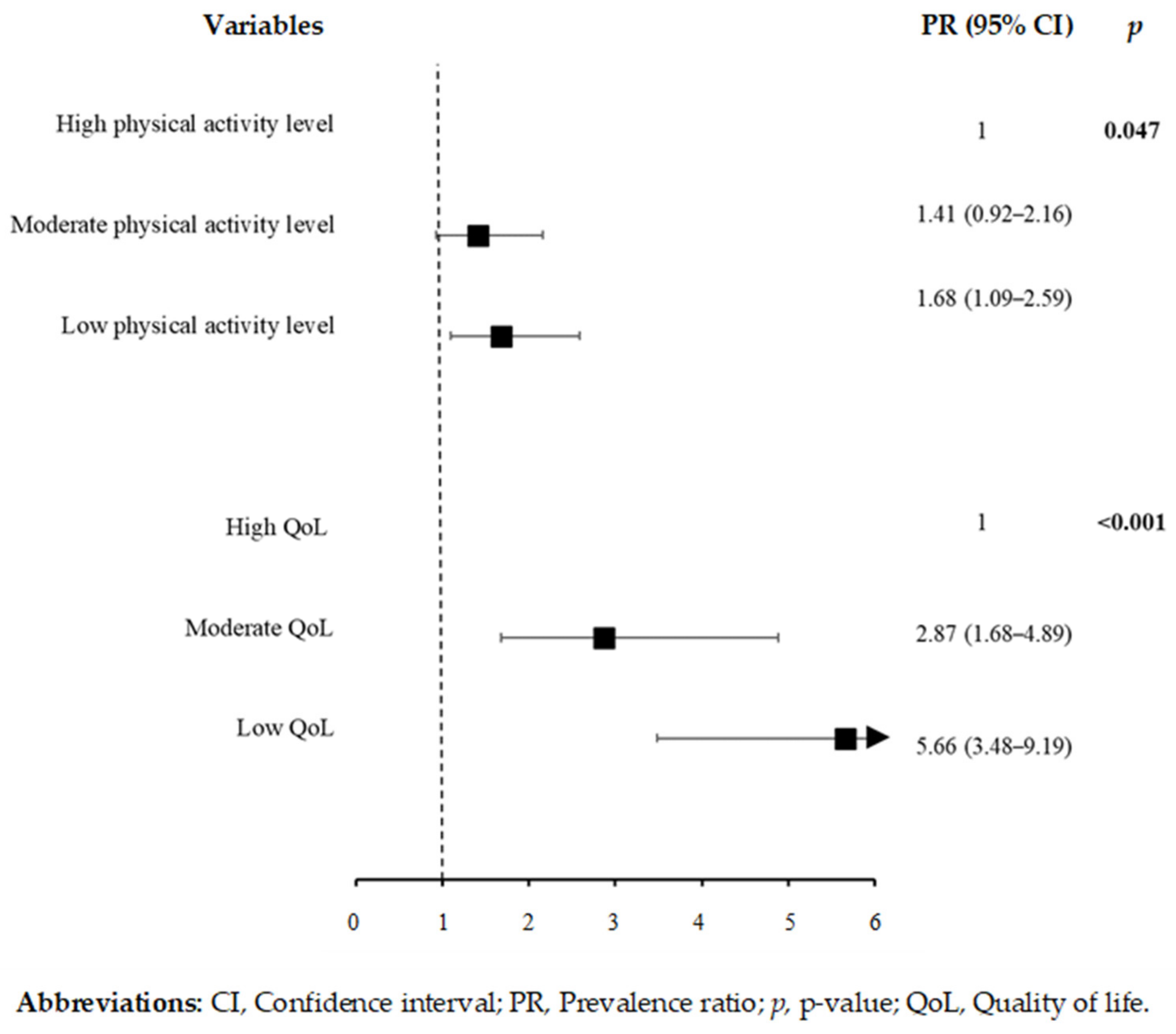
3.3. Depressive Symptoms and Associated Factors during the COVID-19 Pandemic
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, T.; Jia, X.; Shi, H.; Niu, J.; Yin, X.; Xie, J.; Wang, X. Prevalence of mental health problems during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 281, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Ravens-Sieberer, U.; Kaman, A.; Erhart, M.; Devine, J.; Schlack, R.; Otto, C. Impact of the COVID-19 pandemic on quality of life and mental health in children and adolescents in Germany. Eur. Child Adolesc. Psychiatry 2021, 11, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Hawes, M.T.; Szenczy, A.K.; Klein, D.N.; Hajcak, G.; Nelson, B.D. Increases in depression and anxiety symptoms in adolescents and young adults during the COVID-19 pandemic. Psychol. Med. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Qi, H.; Liu, R.; Feng, Y.; Li, W.; Xiang, M.; Cheung, T.; Jackson, T.; Wang, G.; Xiang, Y.T. Depression, anxiety and associated factors among Chinese adolescents during the COVID-19 outbreak: A comparison of two cross-sectional studies. Transl. Psychiatry 2021, 11, 148. [Google Scholar] [CrossRef] [PubMed]
- Nagy-Pénzes, G.; Vincze, F.; Bíró, É. Contributing factors in adolescents’ mental well-being—the role of socioeconomic status, social support, and health behavior. Sustainability 2020, 12, 9597. [Google Scholar] [CrossRef]
- Rice, F.; Riglin, L.; Lomax, T.; Souter, E.; Potter, R.; Smith, D.J.; Thapar, A.K.; Thapar, A. Adolescent and adult differences in major depression symptom profiles. J. Affect. Disord. 2019, 243, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Mojtabai, R.; Olfson, M.; Han, B. National trends in the prevalence and treatment of depression in adolescents and young adults. Pediatrics 2016, 138, e20161878. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, V.R.; Jardim, T.V.; Sousa, A.L.L.; Rosa, B.M.C.; Jardim, P.C.V. Smoking, alcohol consumption and mental health: Data from the Brazilian study of Cardiovascular Risks in Adolescents (ERICA). Addict. Behav. Rep. 2019, 9, 100147. [Google Scholar] [CrossRef]
- Rodzlan Hasani, W.S.; Saminathan, T.A.; Ab Majid, N.L.; Miaw Yn, J.L.; Mat Rifin, H.; Abd Hamid, H.A.; Robert Lourdes, T.G.; Ahmad, A.; Lsmail, H.; Rashid, R.A.; et al. Polysubstance use among adolescents in Malaysia: Findings from the national health and morbidity survey 2017. PLoS ONE 2021, 16, e0245593. [Google Scholar] [CrossRef]
- Dorn, L.D.; Hostinar, C.E.; Susman, E.J.; Pervanidou, P. Conceptualizing puberty as a window of opportunity for impacting health and well-being across the life Span. J. Res. Adolesc. 2019, 29, 155–176. [Google Scholar] [CrossRef] [Green Version]
- De Sousa Junior, I.; Nunes, R.S.M.; de Luca Corrêa, H.; Vieira, E. Functional training program: The impact on depression, anxiety and sleep quality in adolescents. Sport Sci. Health 2021, 17, 233–242. [Google Scholar] [CrossRef]
- De Faria, F.R.; Neves Miranda, V.P.; Howe, C.A.; Sasaki, J.E.; dos Santos Amorim, P.R. Behavioral classes related to physical activity and sedentary behavior on the evaluation of health and mental outcomes among Brazilian adolescents. PLoS ONE 2020, 15, e0234374. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Ayllon, M.; Cadenas-Sánchez, C.; Estévez-López, F.; Muñoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-García, P.; Henriksson, H.; Mena-Molina, A.; Martínez-Vizcaíno, V.; et al. Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: A systematic review and meta-analysis. Sport. Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef] [PubMed]
- Dale, L.P.; Vanderloo, L.; Moore, S.; Faulkner, G. Physical activity and depression, anxiety, and self-esteem in children and youth: An umbrella systematic review. Ment. Health Phys. Act. 2019, 16, 66–79. [Google Scholar] [CrossRef]
- Bolanis, D.; Orri, M.; Castellanos-Ryan, N.; Renaud, J.; Montreuil, T.; Boivin, M.; Vitaro, F.; Tremblay, R.E.; Turecki, G.; Côté, S.M.; et al. Cannabis use, depression and suicidal ideation in adolescence: Direction of associations in a population based cohort. J. Affect. Disord. 2020, 274, 1076–1083. [Google Scholar] [CrossRef] [PubMed]
- Bui, C.; Lin, L.Y.; Wu, C.Y.; Chiu, Y.W.; Chiou, H.Y. Association between emotional eating and frequency of unhealthy food consumption among Taiwanese adolescents. Nutrients 2021, 13, 2739. [Google Scholar] [CrossRef]
- Moitra, P.; Madan, J.; Shaikh, N.I. Eating habits and sleep patterns of adolescents with depression symptoms in Mumbai, India. Matern. Child Nutr. 2020, 16, e12998. [Google Scholar] [CrossRef]
- Xu, H.; Guo, J.; Wan, Y.; Zhang, S.; Yang, R.; Xu, H.; Ding, P.; Tao, F. Association Between Screen Time, Fast Foods, Sugar-Sweetened Beverages and Depressive Symptoms in Chinese Adolescents. Front. Psychiatry 2020, 11, 458. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Jeong, W.; Jang, S.; Kim, Y.; Park, E. Association between sexual behavior and depression in south korean adolescents: A cross-sectional study. Int. J. Environ. Res. Public Health 2021, 18, 4228. [Google Scholar] [CrossRef]
- Luseno, W.K.; Field, S.H.; Iritani, B.J.; Odongo, F.S.; Kwaro, D.; Amek, N.O.; Rennie, S. Pathways to depression and poor quality of life among adolescents in Western Kenya: Role of anticipated HIV stigma, HIV risk perception, and sexual behaviors. AIDS Behav. 2021, 25, 1423–1437. [Google Scholar] [CrossRef]
- Escobar, D.F.S.S.; Noll, P.R.e.S.; de Jesus, T.F.; Noll, M. Assessing the mental health of brazilian students involved in risky behaviors. Int. J. Environ. Res. Public Health 2020, 17, 3647. [Google Scholar] [CrossRef]
- Sinclair, R.; Millar, L.; Allender, S.; Snowdon, W.; Waqa, G.; Jacka, F.; Moodie, M.; Petersen, S.; Swinburn, B. The cross-sectional association between diet quality and depressive symptomology amongst fijian adolescents. PLoS ONE 2016, 11, e0161709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genta, F.D.; Rodrigues Neto, G.B.; Velletri Sunfeld, J.P.; Porto, J.F.; Xavier, A.D.; Moreno, C.R.C.; Lorenzi-Filho, G.; Genta, P.R. COVID-19 pandemic impact on sleep habits, chronotype and health-related quality of life among high school students: A longitudinal study. J. Clin. Sleep Med. 2021, 17, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated psychological problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef] [PubMed]
- Elbay, R.Y.; Kurtulmuş, A.; Arpacıoğlu, S.; Karadere, E. Depression, anxiety, stress levels of physicians and associated factors in Covid-19 pandemics. Psychiatry Res. 2020, 290, 113130. [Google Scholar] [CrossRef] [PubMed]
- Chawla, N.; Tom, A.; Sen, M.S.; Sagar, R. Psychological impact of COVID-19 on children and adolescents: A systematic review. Indian J. Psychol. Med. 2021, 43, 294–299. [Google Scholar] [CrossRef]
- Ahsan Khodami, M.; Hassan Seif, M.; Sadat Koochakzadeh, R.; Fathi, R.; Kaur, H. Perceived stress, emotion regulation and quality of life during the Covid-19 outbreak: A multi-cultural online survey. Ann. Med. Psychol. 2021, 43, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Nobari, H.; Fashi, M.; Eskandari, A.; Villafaina, S.; Murillo-Garcia, Á.; Pérez-Gómez, J. Effect of COVID-19 on health-related quality of life in adolescents and children: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 4563. [Google Scholar] [CrossRef]
- Mastorci, F.; Piaggi, P.; Doveri, C.; Trivellini, G.; Casu, A.; Pozzi, M.; Vassalle, C.; Pingitore, A. Health-related quality of life in italian adolescents during COVID-19 outbreak. Front. Pediatr. 2021, 9, 611136. [Google Scholar] [CrossRef]
- Rodrigues, P.H.E.; Carius, A.C. The implementation of emergency remote education in brazilian educational systems. Am. Sci. Res. J. Eng. 2020, 74, 181–194. [Google Scholar]
- Chaturvedi, K.; Vishwakarma, D.K.; Singh, N. COVID-19 and its impact on education, social life and mental health of students: A survey. Child. Youth Serv. Rev. 2021, 121, 105866. [Google Scholar] [CrossRef]
- Pacheco, F.D.A.; Nonenmacher, S.E.B.; Cambraia, A.C. Mental illness in vocational and technological education: What do graduates of integrated technical courses think (Adoecimento Mental na Educação Profissional e Tecnológica: O Que Pensam os Estudantes Concluintes de Cursos Técnico Integrados). Rev. Bras. Educ. Prof. Tecnol. 2020, 1, e9173. [Google Scholar] [CrossRef] [Green Version]
- Soares, D.P.; Almeida, R.R. Intervention and anxiety management in integrated high school students (Intervenção e manejo de ansiedade em estudantes do ensino médio integrado). Res. Soc. Dev. 2020, 9, e3789106457. [Google Scholar] [CrossRef]
- Barreiro, C.B.; Mogarro, M.J. Teaching and professional education in Brazil and Portugal (Docência e ensino profissional no Brasil e em Portugal). Educ. Rev. 2021, 37, 1–21. [Google Scholar] [CrossRef]
- Brazil School Census of Basic Education 2016. 2017. Available online: http://download.inep.gov.br/educacao_basica/censo_escolar/notas_estatisticas/2017/notas_estatisticas_censo_escolar_da_educacao_basica_2016.pdf (accessed on 5 November 2021).
- Tsunematsu, J.D.P.J.; Pantoni, R.P.; Versuti, F.M. Student mental health in professional and technological education: Experiences of students and teachers of integrated technical courses (Saúde mental discente na educação profissional e tecnológica: Experiências de estudantes e docentes dos cursos técnicos integrado). Educ. Prof. Tecnol. Rev. 2021, 5, 70–90. [Google Scholar] [CrossRef]
- Bleicher, T.; Oliveira, R.C.N. Policies in health assistance for students in federal institutes and universities (Políticas de assistência estudantil em saúde nos institutos e universidades federais). Psicol. Esc. Educ. 2016, 20, 543–549. [Google Scholar] [CrossRef] [Green Version]
- Ahadi, Z.; Qorbani, M.; Kelishadi, R.; Ardalan, G. Regional disparities in psychiatric distress, violent behavior, and life satisfaction in Iranian adolescents: The CASPIAN-III study. J. Dev. Behav. Pediatr. 2014, 35, 582–590. [Google Scholar] [CrossRef] [Green Version]
- Vitorino, L.M.; Yoshinari Júnior, G.H.; Gonzaga, G.; Dias, I.F.; Pereira, J.P.L.; Ribeiro, I.M.G.; França, A.B.; Al-Zaben, F.; Koenig, H.G.; Trzesniak, C. Factors associated with mental health and quality of life during the COVID-19 pandemic in Brazil. BJPsych Open 2021, 7, e103. [Google Scholar] [CrossRef] [PubMed]
- Moilanen, S.; Autio, L.; Tolvanen, A.; Sevón, E.; Rönkä, A. From intense to leisurely study days: A diary study of daily wellbeing among students in higher education. Open Educ. Stud. 2021, 2, 295–311. [Google Scholar] [CrossRef]
- Aldridge, J.M.; McChesney, K. The relationships between school climate and adolescent mental health and wellbeing: A systematic literature review. Int. J. Educ. Res. 2018, 88, 121–145. [Google Scholar] [CrossRef]
- Brazilian Institute of Geography and Statistics. Cities@. 2022. Available online: https://cidades.ibge.gov.br/ (accessed on 5 November 2021).
- Establishes the Federal Network of Professional, Scientific and Technological Education, Creates the Federal Institutes of Education, Science and Technology, and Takes Other Measures. Available online: http://www.planalto.gov.br/ccivil_03/_ato2007-2010/2008/lei/l11892.htm (accessed on 10 November 2021).
- Nascimento, M.M.; Cavalcanti, C.; Ostermann, F. Ten years of institution of the federal network of professional, scientific and technological education: The social role of Federal Institutes (Dez anos de instituição da rede federal de educação profissional, científica e tecnológica: O papel social dos Institutos Federais). Rev. Bras. Estud. Pedagógicos 2020, 101, 120–145. [Google Scholar] [CrossRef] [Green Version]
- Federal Institutes: Revolution in Vocational and Technological Education (Institutos Federais: Uma Revolução na Educação Profissional e Tecnológica. Available online: https://www.fundacaosantillana.org.br/wp-content/uploads/2019/12/67_Institutosfederais.pdf (accessed on 15 November 2021).
- Raosoft Inc. RaoSoft® Sample Size Calculator. 2004. Available online: http://www.raosoft.com/samplesize.html (accessed on 10 November 2021).
- Okruszek, Ł.; Aniszewska-Stańczuk, A.; Piejka, A.; Wiśniewska, M.; Żurek, K. Safe but lonely? Loneliness, anxiety, and depression symptoms and COVID-19. Front. Psychol. 2020, 11, 579181. [Google Scholar] [CrossRef]
- Guedes, D.P.; Lopes, C.C.; Guedes, J.E.R.P. Reproducibility and validity of the international physical activity questionnaire in adolescents. Rev. Bras. Med. Esporte 2005, 11, 151–158. [Google Scholar] [CrossRef]
- Craig, C.L.C.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A. Guidelines for data processing and analysis of the IPAQ-short and long forms. Med. Sci. Sport. Exerc. 2004, 35, 1–7. [Google Scholar]
- Fleck, M.P.A.; Louzada, S.; Xavier, M.; Chachamovich, E.; Vieira, G.; Santos, L.; Pinzon, V. Application of the Portuguese version of the abbreviated quality of life assessment instrument “WHOQOL-bref.” (Aplicação da versão em português do instrumento abreviado de avaliação da qualidade de vida “WHOQOL-bref.”). Rev. Saude Publica 2000, 34, 178–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHOQOL. WHO Quality of Life Scale (WHOQOL). Psuchol. Med. 1998, 28, 551–558. [Google Scholar]
- Gouveia, V.; Barbosa, G.; Almeida, H.; Gaião, A. Childhood Depression Inventory—CDI: Adaptation study with students from João Pessoa (Inventário de depressão infantil—CDI: Estudo de adaptação com escolares de João Pessoa). J. Bras. Psiquiatr. 1995, 44, 345–349. [Google Scholar]
- Wathier, J.L.; Dell’Aglio, D.D.; Bandeira, D.R. Factor analysis of the childhood depression inventory (CDI) in a sample of young Brazilians (Análise fatorial do inventário de depressão infantil (CDI) em amostra de jovens brasileiros). Av. Psicol. 2008, 1, 75–84. [Google Scholar]
- Coutinho, M.d.P.d.L.; Carolino, Z.C.G.; Medeiros, E.D. Inevntário de Childhood Depression Inventory (CDI): Evidence of construct validity and internal consistency (Inventário de Depressão Infantil (CDI): Evidências de validade de constructo e consistência interna). J. Psychol. Assess. 2008, 7, 291–300. [Google Scholar]
- Greenland, S.; Daniel, R.; Pearce, N. Outcome modelling strategies in epidemiology: Traditional methods and basic alternatives. Int. J. Epidemiol. 2016, 45, 565–575. [Google Scholar] [CrossRef] [Green Version]
- Barros, A.J.; Hirakata, V.N. Alternatives for logistic regression in cross-sectional studies: An empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 2003, 2003, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santomauro, D.F.; Mantilla Herrera, A.M.; Shadid, J.; Zheng, P.; Ashbaugh, C.; Pigott, D.M.; Abbafati, C.; Adolph, C.; Amlag, J.O.; Aravkin, A.Y.; et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Escobar, D.F.S.S.; De Jesus, T.F.; Noll, P.R.e.S.; Matias, N. Family and school context: Effects on the mental health of Brazilian students. Int. J. Environ. Res. Public Health 2020, 17, 6042. [Google Scholar] [CrossRef]
- Zhang, C.; Ye, M.; Fu, Y.; Yang, M.; Luo, F.; Yuan, J.; Tao, Q. The psychological impact of the COVID-19 pandemic on teenagers in China. J. Adolesc. Health 2020, 67, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Noll, M.; Noll, P.R.e.S.; Tiggemann, C.L.; Custodio, D.C.; Silveira, E.A. Health-risk behavior differences between boarding and non-resident students: Brazilian adolescent National School Health Survey. Arch. Public Health 2020, 78, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephanou, A.T.; Dias, A.C.G. Psychological factors associated with adolescent sexual behavior. Psico 2021, 52, e36084. [Google Scholar] [CrossRef]
- Gazendam, N.; Cleverley, K.; King, N.; Pickett, W.; Phillips, S.P. Individual and social determinants of early sexual activity: A study of gender-based differences using the 2018 Canadian Health Behaviour in School-aged Children Study (HBSC). PLoS ONE 2020, 15, e0238515. [Google Scholar] [CrossRef] [PubMed]
- Pozuelo, J.R.; Desborough, L.; Stein, A.; Cipriani, A. Systematic review and meta-analysis: Depressive symptoms and risky behaviors among adolescents in low- and middle-income countries. J. Am. Acad. Child Adolesc. Psychiatry 2021, 61, 255–276. [Google Scholar] [CrossRef] [PubMed]
- Hallfors, D.D.; Waller, M.W.; Bauer, D.; Ford, C.A.; Halpern, C.T. Which comes first in adolescence—Sex and drugs or depression? Am. J. Prev. Med. 2005, 29, 163–170. [Google Scholar] [CrossRef]
- Armoon, B.; Mokhayeri, Y.; Haroni, J.; Karimy, M.; Noroozi, M. How is the quality of life of students?: The role of depression, anxiety and stress. Pol. Psychol. Bull. 2019, 50, 43–48. [Google Scholar] [CrossRef]
- Ma, L.; Mazidi, M.; Li, K.; Li, Y.; Chen, S.; Kirwan, R.; Zhou, H.; Yan, N.; Rahman, A.; Wang, W.; et al. Prevalence of mental health problems among children and adolescents during the COVID-19 pandemic: A systematic review and meta-analysis. J. Affect. Disord. 2021, 293, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global prevalence of depressive and anxiety symptoms in children and adolescents during COVID-19: A meta-analysis. JAMA Pediatr. 2021, 175, 1142–1150. [Google Scholar] [CrossRef]
- Orben, A.; Tomova, L.; Blakemore, S.J. The effects of social deprivation on adolescent development and mental health. Lancet Child Adolesc. Health 2020, 4, 634–640. [Google Scholar] [CrossRef]
- AlAzzam, M.; Abuhammad, S.; Abdalrahim, A.; Hamdan-Mansour, A.M. Predictors of depression and anxiety among senior high school students during COVID-19 pandemic: The context of home quarantine and online education. J. Sch. Nurs. 2021, 37, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; McManus, M.N.; Borwick, C.; Crawley, E. Rapid systematic review: The impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1218–1239.e3. [Google Scholar] [CrossRef] [PubMed]
- Askeland, K.G.; Bøe, T.; Breivik, K.; la Greca, A.M.; Sivertsen, B.; Hysing, M. Life events and adolescent depressive symptoms: Protective factors associated with resilience. PLoS ONE 2020, 15, e0234109. [Google Scholar] [CrossRef] [PubMed]
- Carpena, M.X.; Costa, F.D.S.; Martins-Silva, T.; Xavier, M.O.; de Mola, C.L. Why Brazilian women suffer more from depression and suicidal ideation: A mediation analysis of the role of violence. Braz. J. Psychiatry 2020, 42, 469–474. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhai, A.; Yang, M.; Zhang, J.; Zhou, H.; Yang, C.; Duan, S.; Zhou, C. Prevalence of depression and anxiety symptoms of high school students in shandong province during the COVID-19 epidemic. Front. Psychiatry 2020, 11, 570096. [Google Scholar] [CrossRef]
- Morssinkhof, M.W.L.; van Wylick, D.W.; Priester-Vink, S.; van der Werf, Y.D.; den Heijer, M.; van den Heuvel, O.A.; Broekman, B.F.P. Associations between sex hormones, sleep problems and depression: A systematic review. Neurosci. Biobehav. Rev. 2020, 118, 669–680. [Google Scholar] [CrossRef]
- Pfeifer, J.H.; Allen, N.B. Puberty initiates cascading relationships between neurodevelopmental, social, and internalizing processes across adolescence. Soc. Biol. Psychiatry 2021, 89, 99–108. [Google Scholar] [CrossRef]
- Chauhan, S.; Srivastava, S.; Kumar, P.; Patel, R.; Muhammad, T.; Dhillon, P. Interaction of substance use with physical activity and its effect on depressive symptoms among adolescents. J. Subst. Use 2021, 26, 524–530. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Global trends in insufficient physical activity among adolescents: A pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc. Health 2020, 4, 23–35. [Google Scholar] [CrossRef]
- Fruzzetti, F.; Fidecicchi, T. Hormonal contraception and depression: Updated evidence and implications in clinical practice. Clin. Drug Investig. 2020, 40, 1097–1106. [Google Scholar] [CrossRef] [PubMed]
- Connor, J.; Madhavan, S.; Mokashi, M.; Amanuel, H.; Johnson, N.R.; Pace, L.E.; Bartz, D. Health risks and outcomes that disproportionately affect women during the COVID-19 pandemic: A review. Soc. Sci. Med. 2020, 266, 113364. [Google Scholar] [CrossRef] [PubMed]
- Sumra, M.K.; Schillaci, M.A. Stress and the multiple-role woman: Taking a closer look at the “superwoman”. PLoS ONE 2015, 10, e0120952. [Google Scholar] [CrossRef] [Green Version]
- Brar, S.K.; Beattie, T.S.H.; Abas, M.; Vansia, D.; Phanga, T.; Maseko, B.; Bekker, L.G.; Pettifor, A.E.; Rosenberg, N.E. The relationship between intimate partner violence and probable depression among adolescent girls and young women in Lilongwe, Malawi. Glob. Public Health 2020, 15, 865–876. [Google Scholar] [CrossRef]
- Carvalhaes, R.d.S.; Cárdenas, C.M.M. “Dating is pure suffering”: Violence within affective-sexual relationships between adolescents in a school in the Costa Verde, Rio de Janeiro, Brazil. Cienc. Saude Coletiva 2021, 26, 2719–2728. [Google Scholar] [CrossRef]
- Chi, X.; Liu, X.; Huang, Q.; Huang, L.; Zhang, P.; Chen, X. Depressive symptoms among junior high school students in Southern China: Prevalence, Changes, and Psychosocial Correlates. J. Affect. Disord. 2020, 274, 1191–1200. [Google Scholar] [CrossRef]
- Gordia, A.P.; Silva, R.C.R.; Quadros, T.M.B.; De Campos, W. Behavioral and sociodemographic variables are associated with the psychological domain of adolescents’ quality of life. Rev. Paul. Pediatr. 2010, 28, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Finning, K.; Ukoumunne, O.C.; Ford, T.; Danielsson-Waters, E.; Shaw, L.; Romero De Jager, I.; Stentiford, L.; Moore, D.A. The association between child and adolescent depression and poor attendance at school: A systematic review and meta-analysis. J. Affect. Disord. 2019, 245, 928–938. [Google Scholar] [CrossRef]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Bathelt, J.; Vignoles, A.; Astle, D.E. Just a phase? Mapping the transition of behavioural problems from childhood to adolescence. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 821–836. [Google Scholar] [CrossRef]
- Dush, J.L. Adolescent food insecurity: A review of contextual and behavioral factors. Public Health Nurs. 2020, 37, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.; Oliveira, A.M. Poverty and food insecurity may increase as the threat of COVID-19 spreads. Public Health Nutr. 2020, 23, 3236–3240. [Google Scholar] [CrossRef] [PubMed]
- Rani, D.; Singh, J.; Acharya, D.; Paudel, R.; Lee, K.; Singh, S. Household food insecurity and mental health among teenage girls living in Urban Slums in Varanasi, India: A cross-sectional study. Int. J. Environ. Res. Public Health 2018, 15, 1585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyundo, A.; Manu, A.; Regan, M.; Ismail, A.; Chukwu, A.; Dessie, Y.; Njau, T.; Kaaya, S.F.; Smith Fawzi, M.C. Factors associated with depressive symptoms and suicidal ideation and behaviours amongst sub-Saharan African adolescents aged 10–19 years: Cross-sectional study. Trop. Med. Int. Health 2020, 25, 54–69. [Google Scholar] [CrossRef] [PubMed]
- Elgar, F.J.; Pickett, W.; Pförtner, T.K.; Gariépy, G.; Gordon, D.; Georgiades, K.; Davison, C.; Hammami, N.; MacNeil, A.H.; Da Silva, M.A.; et al. Relative food insecurity, mental health and wellbeing in 160 countries. Soc. Sci. Med. 2021, 268, 113556. [Google Scholar] [CrossRef]
- Hatem, C.; Lee, C.Y.; Zhao, X.; Reesor-Oyer, L.; Lopez, T.; Hernandez, D.C. Food insecurity and housing instability during early childhood as predictors of adolescent mental health. J. Fam. Psychol. 2020, 34, 721–730. [Google Scholar] [CrossRef]
- Frömel, K.; Jakubec, L.; Groffik, D.; ChmelÍk, F.; Svozil, Z.; Šafář, M. Physical activity of secondary school adolescents at risk of depressive symptoms. J. Sch. Health 2020, 90, 641–650. [Google Scholar] [CrossRef]
- Sampasa-Kanyinga, H.; Sampasa-Kanyinga, H.; Colman, I.; Colman, I.; Goldfield, G.S.; Goldfield, G.S.; Janssen, I.; Wang, J.; Wang, J.; Podinic, I.; et al. Combinations of physical activity, sedentary time, and sleep duration and their associations with depressive symptoms and other mental health problems in children and adolescents: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 72. [Google Scholar] [CrossRef]
- Chi, X.; Liang, K.; Chen, S.-T.; Huang, Q.; Huang, L.; Yu, Q.; Jiao, C.; Guo, T.; Stubbs, B.; Hossain, M.M.; et al. Mental health problems among Chinese adolescents during the COVID-19: The importance of nutrition and physical activity. Int. J. Clin. Health Psychol. 2021, 21, 100218. [Google Scholar] [CrossRef]
- Lin, T.-W.; Kuo, Y.-M. Exercise benefits brain function: The monoamine connection. Brain Sci. 2013, 3, 39–53. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.; Richards, J.; Hillman, C.; Faulkner, G.; Beauchamp, M.; Nilsson, M.; Kelly, P.; Smith, J.; Raine, L.; Biddle, S. Physical activity for cognitive and mental health in youth: A systematic review of mechanisms. Pediatrics 2016, 138, e20161642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matta Mello Portugal, E.; Cevada, T.; Sobral Monteiro-Junior, R.; Teixeira Guimarães, T.; da Cruz Rubini, E.; Lattari, E.; Blois, C.; Camaz Deslandes, A. Neuroscience of Exercise: From Neurobiology Mechanisms to Mental Health. Neuropsychobiology 2013, 68, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiPietro, L.; Al-Ansari, S.S.; Biddle, S.J.H.; Borodulin, K.; Bull, F.C.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; Chastin, S.; et al. Advancing the global physical activity agenda: Recommendations for future research by the 2020 WHO physical activity and sedentary behavior guidelines development group. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 143. [Google Scholar] [CrossRef]
- Solomou, I.; Constantinidou, F. Prevalence and predictors of anxiety and depression symptoms during the COVID-19 pandemic and compliance with precautionary measures: Age and sex matter. Int. J. Environ. Res. Public Health 2020, 17, 4924. [Google Scholar] [CrossRef]
- Assana, S.; Laohasiriwong, W.; Rangseekajee, P. Quality of life, mental health and educational stress of high school students in the northeast of Thailand. J. Clin. Diagn. Res. 2017, 11, VC01–VC06. [Google Scholar] [CrossRef]
- Geng, Y.; Gu, J.; Zhu, X.; Yang, M.; Shi, D. Negative emotions and quality of life among adolescents: A moderated mediation model. Int. J. Clin. Health Psychol. 2020, 20, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Cleofas, J.V. Student involvement, mental health and quality of life of college students in a selected university in Manila, Philippines. Int. J. Adolesc. Youth 2020, 25, 435–447. [Google Scholar] [CrossRef] [Green Version]
- Moutinho, I.L.D.; Lucchetti, A.L.G.; Ezequiel, O.d.S.; Lucchetti, G. Mental health and quality of life of Brazilian medical students: Incidence, prevalence, and associated factors within two years of follow-up. Psychiatry Res. 2019, 274, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Eddolls, W.T.B.; McNarry, M.A.; Lester, L.; Winn, C.O.N.; Stratton, G.; Mackintosh, K.A. The association between physical activity, fitness and body mass index on mental well-being and quality of life in adolescents. Qual. Life Res. 2018, 27, 2313–2320. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables a | Urban Campus (N = 110) | Rural Campus (N = 233) | ||
|---|---|---|---|---|
| Sociodemographic Characteristics | N (%) | N (%) | N (%) | |
| Sex | <0.001 | |||
| Male | 152 (44.3) | 29 (26.4) | 123 (52.8) | |
| Female | 191 (55.7) | 81 (73.6) | 110 (47.2) | |
| Age (years) | 0.166 | |||
| 14 | 10 (2.9) | 5 (4.5) | 5 (2.1) | |
| 15 | 89 (25.9) | 21 (19.1) | 68 (29.2) | |
| 16 | 133 (38.8) | 45 (40.9) | 88 (37.8) | |
| 17–18 | 111 (32.4) | 39 (35.5) | 72 (30.9) | |
| Color/ethnicity | 0.072 | |||
| White | 133 (38.8) | 38 (34.5) | 95 (40.8) | |
| Brown | 165 (48.1) | 51 (46.4) | 114 (48.9) | |
| Other | 45 (13.1) | 21 (19.1%) | 24 (10.3) | |
| Grade/Year | ||||
| 9th grade/1st year | 150 (43.7) | 47 (42.7) | 103 (44.2) | 0.075 |
| 10th grade/2nd year | 114 (33.2) | 30 (27.3) | 84 (36.1) | |
| 11th grade/3rd year | 79 (23.0) | 33 (30.0) | 46 (19.7) | |
| Computer | 0.359 | |||
| Yes | 266 (77.6) | 82 (74.5) | 184 (79.0) | |
| No | 77 (22.4) | 28 (25.5) | 49 (21.0) | |
| Employment | 0.520 | |||
| Yes | 83 (24.2) | 29 (26.4) | 54 (23.2) | |
| No | 260 (75.8) | 81 (73.6) | 179 (76.8) | |
| Household | 0.121 | |||
| Lives with the parents | 189 (55.1) | 57 (51.8) | 132 (56.7) | |
| Lives only with the mother | 111 (32.4) | 33 (30.0) | 78 (33.5) | |
| Lives only with the father | 16 (4.7) | 9 (8.2) | 7 (3.0) | |
| Does not live with the parents | 27 (7.9) | 11 (10.0) | 16 (6.9) | |
| Pandemic-related situations | ||||
| COVID-19 diagnosis | 0.330 | |||
| Yes | 43 (12.5 | 11 (10.0) | 32 (13.7) | |
| No | 300 (87.5) | 99 (90.0) | 201 (86.3) | |
| Social isolation | 0.881 | |||
| Extremely isolated | 29 (8.5) | 9 (8.2) | 20 (8.6) | |
| Very isolated | 69 (20.1) | 23 (20.9) | 46 (19.7) | |
| Moderately isolated | 142 (41.4) | 49 (44.5) | 93 (39.9) | |
| Slightly isolated | 68 (19.8) | 19 (17.3) | 49 (21.0) | |
| Not at all isolated | 35 (10.2) | 10 (9.1) | 25 (10.7) | |
| Concern with the health of family/friends | 0.269 | |||
| Extremely concerned | 79 (23.0) | 32 (29.1) | 47 (20.2) | |
| Very concerned | 141 (41.1) | 39 (35.5) | 102 (43.8) | |
| Moderately concerned | 71 (20.7) | 22 (20.0) | 49 (21.0) | |
| Slightly concerned | 36 (10.5) | 10 (9.1) | 26 (11.2) | |
| Not at all concerned | 16 (4.7) | 7 (6.4) | 9 (3.9) | |
| Concern with remote learning | 0.275 | |||
| Extremely concerned | 165 (48.1) | 52 (47.3) | 113 (48.5) | |
| Very concerned | 106 (30.9) | 29 (26.4) | 77 (33.0) | |
| Moderately concerned | 48 (14.0) | 17 (15.5) | 31 (13.3) | |
| Slightly concerned | 17 (5.0) | 9 (8.2) | 8 (3.4) | |
| Not at all concerned | 7 (2.0) | 3 (2.7) | 4 (1.7) | |
| Concern with the impact of COVID-19 on finances | 0.137 | |||
| Extremely concerned | 80 (23.3) | 30 (27.3) | 50 (21.5) | |
| Very concerned | 86 (25.1) | 26 (23.6) | 60 (25.8) | |
| Moderately concerned | 91 (26.5) | 35 (31.8) | 56 (24.0) | |
| Slightly concerned | 51 (14.9) | 12 (10.0) | 39 (16.7) | |
| Not at all concerned | 35 (10.2) | 7 (6.4) | 28 (12.0) | |
| Social distancing measures | 0.037 | |||
| I followed all social distancing measures, and I did not leave home to perform any activity | 62 (18.1) | 20 (18.2) | 42 (18.0) | |
| I only left home to perform essential activities, unrelated to work | 157 (45.8) | 39 (35.5) | 118 (50.6) | |
| I left home to perform essential activities, including work | 106 (30.9) | 44 (40.0) | 62 (26.6) | |
| I did not follow any social distancing measure | 18 (5.2) | 7 (6.4) | 11 (4.7) | |
| Social distancing period | 0.538 | |||
| Fewer than 30 days | 59 (17.2) | 19 (17.3) | 40 (17.2) | |
| From 30 to 60 days | 94 (27.4) | 26 (23.6) | 68 (29.2) | |
| More than 60 days | 190 (55.4) | 65 (65) | 125 (53.6) | |
| Variables a | TOTAL (N = 343) N (%) | Campuses N (%) | p | |
|---|---|---|---|---|
| Urban Campus (N = 110) | Rural Campus (N = 233) | |||
| Eating habits * | ||||
| Feeling hungry ** | 0.696 | |||
| Never | 285 (83.1) | 90 (81.8) | 195 (83.7) | |
| Rarely | 40 (11.7) | 15 (13.6) | 25 (10.7) | |
| Sometimes/often/always | 18 (5.3) | 5 (4.5) | 13 (5.6) | |
| Eating fruits ** | 0.714 | |||
| Regular consumption b | 151 (44.0) | 50 (45.5) | 101 (43.3) | |
| Irregular consumption | 192 (56.0) | 60 (54.5) | 132 (56.7) | |
| Eating legumes/vegetables ** | 0.339 | |||
| Regular consumption b | 212 (61.8) | 72 (65.5) | 140 (60.1) | |
| Irregular consumption | 131 (38.2) | 38 (34.5) | 93 (39.9) | |
| Drinking soda ** | 0.078 | |||
| Regular consumption b | 100 (29.2) | 39 (35.5) | 61 (26.2) | |
| Irregular consumption | 243 (70.8) | 71 (64.5) | 172 (73.8) | |
| Substance use * | ||||
| Tobacco smoking | 0.682 | |||
| Yes | 41 (12.0) | 12 (10.9) | 29 (12.4) | |
| No | 302 (88.0) | 98 (89.1) | 204 (87.6) | |
| Smoked *** | 0.617 | |||
| Never | 334 (97.4) | 106 (96.4) | 228 (97.9) | |
| 1–2 days | 4 (1.2) | 2 (1.8) | 2 (0.9) | |
| 3–9 days | 1 (0.3) | 0 (0.0) | 1 (0.4) | |
| 10 or more days | 4 (1.2) | 2 (1.8) | 2 (0.9) | |
| Alcohol drinking | 0.500 | |||
| Yes | 150 (43.7) | 51 (46.4) | 99 (42.5) | |
| No | 193 (56.3) | 59 (53.6) | 134 (57.5) | |
| Drank *** c | 0.404 | |||
| Never | 275 (80.2) | 85 (77.3) | 190 (81.5) | |
| 1–2 days | 37 (10.8) | 16 (14.5) | 21 (9.1) | |
| 3–9 days | 23 (6.7) | 6 (5.5) | 17 (7.4) | |
| 10 or more | 8 (2.3) | 3 (2.7) | 5 (2.2) | |
| Being drunk *** c | 0.617 | |||
| Never | 278 (81.0) | 84 (76.4) | 194 (83.3) | |
| 1–2 days | 37 (10.8) | 16 (14.5) | 21 (9.0) | |
| 3–9 days | 24 (7.0) | 9 (8.2) | 15 (6.4) | |
| 10 or more days | 4 (1.2) | 1 (0.9) | 3 (1.3) | |
| Prior drug use d | 0.924 | |||
| Yes | 12 (3.5) | 4 (3.6) | 8 (3.4) | |
| No | 331 (96.5) | 106 (96.4) | 225 (96.6) | |
| Drug use *** c | >0.005 | |||
| Never | 340 (99.1) | 110 (100.0) | 230 (98.7) | |
| 1–2 days | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| 3–9 days | 1 (0.3) | 0 (0.0) | 1 (0.4) | |
| 10 or more | 2 (0.6) | 0 (0.0) | 3 (0.9) | |
| Sexual behavior | ||||
| Prior sexual intercourse | 0.049 | |||
| Yes | 89 (25.9) | 36 (32.1) | 53 (22.7) | |
| No | 254 (74.1) | 74 (67.3) | 180 (77.3) | |
| Age of first sexual intercourse c | ||||
| ≤12 years | 7 (7.9) | 3 (8.3) | 4 (7.5) | |
| 13–14 years | 25 (28.1) | 8 (22.2) | 17 (32.1) | 0.549 |
| ≥15 years | 57 (64.0) | 25 (69.4) | 32 (60.4) | |
| Number of sexual partners in life c | ||||
| 1 | 40 (44.9) | 18 (50.0) | 22 (41.5) | |
| 2 or 3 | 31 (34.8) | 13 (36.1) | 18 (34.0) | 0.461 |
| 4 or more | 18 (20.2) | 5 (13.9) | 13 (24.5) | |
| Physical activity level | ||||
| Low | 110 (32.1) | 35 (31.8) | 75 (32.2) | 0.189 |
| Moderate | 173 (50.4) | 50 (45.5) | 123 (52.8) | |
| High | 60 (17.5) | 25 (22.7) | 35 (15.0) | |
| WHOQOL-Bref | ||||
| High QoL | 114 (33.2) | 52 (47.3) | 62 (26.6) | <0.001 |
| Moderate QoL | 115 (33.2) | 24 (21.8) | 91 (39.1) | |
| Low QoL | 114 (33.5) | 34 (30.9) | 80 (34.3) | |
| Depressive symptoms (CDI) | ||||
| Yes (≥17) | 149 (43.4) | 48 (43.6) | 101 (43.3) | 0.960 |
| No (<17) | 194 (56.6) | 62 (56.4) | 132 (56.7) | |
| Total (n = 343) | Campus Urban (n = 110) | Campus Rural (n = 233) | ||
|---|---|---|---|---|
| Variables | Mean (SD), 95% CI | Mean (SD), 95% CI | Mean (SD), 95% CI | p * |
| CDI total score | 15.8 (9.4), 14.8–16.8 | 16.4 (10.9), 14.3–18.4 | 15.5 (8.7), 14.4–16.6 | 0.922 |
| Female | 17.9 (9.3), 16.4–19.2 | 17.7 (10.4), 15.4–20.0 | 18.0 (8.4), 16.4–19.6 | |
| Male | 13.1 (9.0), 11.7–14.6 | 12.7 (11.6), 8.3–17.1 | 13.2 (8.3), 11.8–14.7 | |
| p * | <0.001 | 0.009 | <0.001 | |
| WHOQOL-bref | ||||
| Physical health | 52.6 (14.0), 51.1–54.1 | 52.8 (16.8), 49.6–55.9 | 52.5 (18.04), 50.9–54.2 | 0.913 |
| Psychological | 53.0 (19.7), 50.9–55.0 | 51.1 (22.8), 46.8–55.4 | 53.9 (18.24), 51.6–56.2 | 0.243 |
| Social relationships | 52.0 (19.5), 49.9–54.0 | 62.1 (18.2), 58.7–65.6 | 47.2 (11.8), 44.9–49.6 | <0.001 |
| Environment | 57.5 (14.6), 56.0–59.1 | 62.4 (18.3), 58.9–65.8 | 55.2 (10.8), 53.7–56.8 | <0.001 |
| Overall QoL | 53.8 (12.8), 52.4–55.1 | 57.1 (16.0), 54.1–60.1 | 52.2 (10.8), 50.8–53.6 | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernandes, M.d.S.V.; Silva, T.M.V.d.; Noll, P.R.e.S.; Almeida, A.A.d.; Noll, M. Depressive Symptoms and Their Associated Factors in Vocational–Technical School Students during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 3735. https://doi.org/10.3390/ijerph19063735
Fernandes MdSV, Silva TMVd, Noll PReS, Almeida AAd, Noll M. Depressive Symptoms and Their Associated Factors in Vocational–Technical School Students during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(6):3735. https://doi.org/10.3390/ijerph19063735
Chicago/Turabian StyleFernandes, Michele da Silva Valadão, Thays Martins Vital da Silva, Priscilla Rayanne e Silva Noll, Alexandre Aparecido de Almeida, and Matias Noll. 2022. "Depressive Symptoms and Their Associated Factors in Vocational–Technical School Students during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 6: 3735. https://doi.org/10.3390/ijerph19063735