
Parental Views on the Acceptability and Feasibility of Measurement Tools Used to Assess Movement Behaviour of Pre-School Children: A Qualitative Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Data Analysis
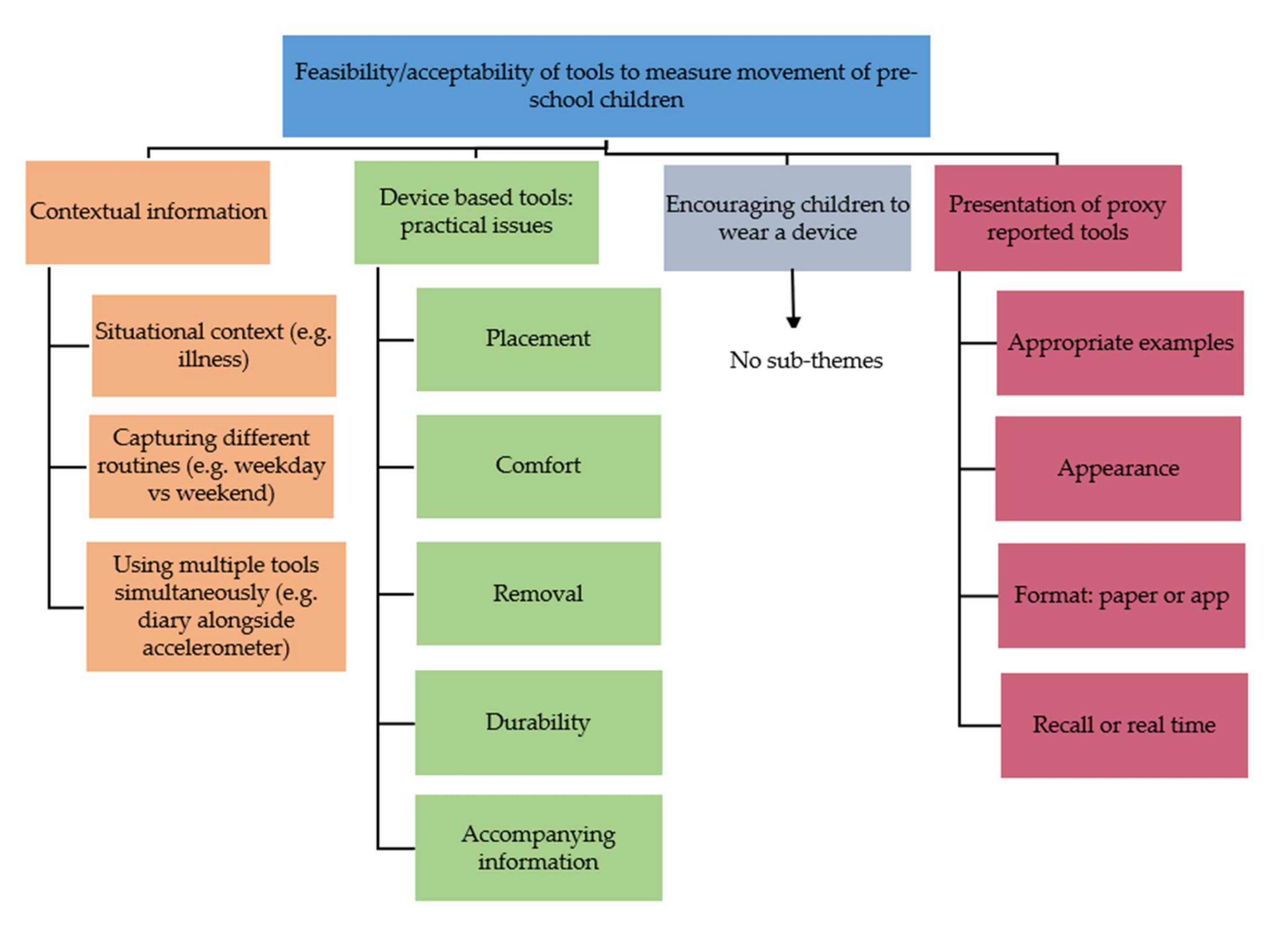
3. Results
3.1. Theme 1: Capturing Contextual Information Is Important to Parents and Carers
3.1.1. Situational Context
‘I think it all depends on whether they’re poorly or not…[name] sleeps like a trooper when she’s poorly during the day…But then they have their off-days, so it’s like if they’re poorly they’re going to have a nap.’(P5)
3.1.2. Capturing Different Routines
‘I definitely think that a box or a question in relation to how often is this usually the case, like being allowed to give a reason as to why on this particular day your child didn’t sleep very long or didn’t actually go to bed because they might have been ill or it might be a weekend, so they might be allowed to have a later night because it’s Friday night.’(P11)
3.1.3. Using Multiple Measurement Tools Simultaneously
3.2. Theme 2: Device Based Tools: Practical Issues
3.2.1. Placement of Devices
‘Yeah, they wouldn’t want something stuck to their body like that. I just don’t think they’d like it at all. Plasters don’t stay on very well, let alone…’(P2)
‘I think they’re great. The only issue I have with the actual monitors themselves is how children would react if they have sensory issues. So some children with sensory issues are fine with things touching their skin, but something that’s actually attached to the skin might be kind of irritating for some children.’(P9)
3.2.2. Comfort/Ease of Wearing
3.2.3. Removal of Devices
‘…just for practicality of, just so they’re not stressed as well, if they do want to take it off they can quite easily take it off themselves.’(P2)
‘I think the strap one would probably be the easiest for like grandparents and that, because then they don’t have to strip them to stick it back on their thigh.’(P10)
3.2.4. Durability of Devices
3.2.5. Acceptability of Accompanying Information—Instructions and Accelerometer Logs
‘Ideally probably a demonstration.’(P6)
‘Yeah, that’d be good, like a video or something to go on, wouldn’t it? That would be handy…Like just say oh if you go onto this YouTube website or whatever, it shows you how to do it, because all right it’s reading something, but sometimes I need showing…something to show me what to do. Because then otherwise you might not put it on properly and then it might not get the right reading for what you need.’(P7) (Extract from Focus Group 2)
3.3. Theme 3: Encouraging Children to Wear a Device
‘I’ve got a son that’s got these special boots. Like my kids know that he’s got to wear them. So I reckon if I told them they had to wear that they’d just wear it.’(P2)
3.4. Theme 4: Presentation of Diaries and Questionnaires
3.4.1. Examples of Movement Behaviours
‘Yeah. So we could just have examples so people don’t think hmm, what have they done?… Yeah, but then have the choice to also write your own if you can do that.’(P4)
3.4.2. Appearance of Diaries and Questionnaires
3.4.3. Format of Tools: Paper or App?
3.4.4. Recall or Real Time
’I think it’s a bit too hard for me this, because like she does so much each day, like all the different things she does through the day, and then you’re having to record them and remember, oh, it’s so confusing, I just don’t understand it.’(P3)
‘It might mean it’s more paperwork, but it makes it more- easier to look at. So it kind of looks like it’s more but it’s…’ (P4) ‘In the long run it’ll be easier.’ (P2) ‘I think it’s going to be easier, especially if you’ve got more kids, because then you’re not getting the kids mixed up either, because I know that’s what I do. I’m like, [child’s] done this today, no, he hasn’t, it was [other child], no, it was [other child]’.(P5), (Focus Group 1 Extract)
4. Discussion
4.1. Main Findings
- Importance of providing contextual information when using any measurement tool to report on children’s movement behaviours (e.g., child illness, capturing different routines such as home and school activity, and potentially using multiple measurement tools to obtain context alongside device based tools).
- Practical issues associated with devices (e.g., placement of devices and aversion to devices being attached directly to the skin of their child; concern of larger devices during sleep time; likelihood of removal of devices (and subsequently needing space to report this on an accompanying log); worry about durability of devices during child play; and preference for written and visual instructions for device administration).
- Encouraging children to wear a device (e.g., making devices attractive to children-‘superpowers’, colourful belts and personalised stickers).
- Presentation of diaries and questionnaires (e.g., parents would prefer examples of age appropriate movement activities, much prefer real-time recording than recall).
4.2. Recommendations
4.3. Strengths and Limitations
4.4. Implications and Areas for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chaput, P.J.; Carson, V.; Gray, E.C.; Tremblay, S.M. Importance of all movement behaviors in a 24 hour period for overall health. Int. J. Environ. Res. Public Health 2014, 11, 12575–12581. [Google Scholar] [CrossRef]
- Chaput, J.P.; Saunders, T.J.; Carson, V. Interactions between sleep, movement and other non-movement behaviours in the pathogenesis of childhood obesity. Obes. Rev. 2017, 18, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.; Palarea-Albaladejo, J.; Dontje, M.L.; Skelton, D.A. Combined Effects of Time Spent in Physical Activity, Sedentary Behaviors and Sleep on Obesity and Cardio-Metabolic Health Markers: A Novel Compositional Data Analysis Approach. PLoS ONE 2015, 10, e0139984. [Google Scholar] [CrossRef] [Green Version]
- Tremblay, M.S. Introducing 24-Hour Movement Guidelines for the Early Years: A New Paradigm Gaining Momentum. J. Phys. Act. Health 2020, 17, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Rosenberger, M.E.; Fulton, J.E.; Buman, M.P.; Troiano, R.P.; Grandner, M.A.; Buchner, D.M.; Haskell, W.L. The 24-Hour Activity Cycle: A New Paradigm for Physical Activity. Med. Sci. Sports Exerc. 2019, 51, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Rao, D.P.; Orpana, H.; Krewski, D. Physical activity and non-movement behaviours: Their independent and combined associations with metabolic syndrome. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 26. [Google Scholar] [CrossRef] [Green Version]
- Buman, M.P.; Winkler, E.A.; Kurka, J.M.; Hekler, E.B.; Baldwin, C.M.; Owen, N.; Ainsworth, B.E.; Healy, G.N.; Gardiner, P.A. Reallocating time to sleep, sedentary behaviors, or active behaviors: Associations with cardiovascular disease risk biomarkers, NHANES 2005-2006. Am. J. Epidemiol. 2014, 179, 323–334. [Google Scholar] [CrossRef]
- World Health Organization. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age. 2019. Available online: https://apps.who.int/iris/handle/10665/311664 (accessed on 31 August 2021).
- Tremblay, M.S.; Chaput, J.-P.; Adamo, K.B.; Aubert, S.; Barnes, J.D.; Choquette, L.; Duggan, M.; Faulkner, G.; Goldfield, G.S.; Grayet, C.E.; et al. Canadian 24-Hour Movement Guidelines for the Early Years (0–4 years): An Integration of Physical Activity, Sedentary Behaviour, and Sleep. BMC Public Health 2017, 17 (Suppl. S5), 874. [Google Scholar] [CrossRef]
- Okely, A.D.; Ghersi, D.; Hesketh, K.D.; Santos, R.; Loughran, S.P.; Cliff, D.P.; Shilton, T.; Grant, D.; Jones, R.A.; Stanleyet, R.M.; et al. A collaborative approach to adopting/adapting guidelines—The Australian 24-Hour Movement Guidelines for the early years (Birth to 5 years): An integration of physical activity, sedentary behavior, and sleep. BMC Public Health 2017, 17, 869. [Google Scholar] [CrossRef]
- Ministry of Health. Sit Less, Move More, Sleep Well: Active Play Quidelines for Under Fives; Ministry of Health, New Zealand: Wellington, New Zealand, 2017. [Google Scholar]
- Draper, C.E.; Silubonde, T.M.; Mukoma, G.M.; van Sluijs, E.M.F. The South African 24-Hour Movement Guidelines for Birth to 5 Years: An Integration of Physical Activity, Sitting Behavior, Screen Time, and Sleep. J. Phys. Act. Health 2020, 17, 109–119. [Google Scholar] [CrossRef] [Green Version]
- Reilly, J.J.; Hughes, A.R.; Janssen, X.; Hesketh, K.R.; Livingstone, S.; Hill, C.; Kipping, R.; Draper, C.E.; Okely, A.D.; Martin, A. GRADE-ADOLOPMENT Process to Develop 24-Hour Movement Behavior Recommendations and Physical Activity Guidelines for the Under 5s in the United Kingdom, 2019. J. Phys. Act. Health 2020, 17, 101–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forouhi, N.; Activity, P. Diet, Anthropometry and Physical Activity (DAPA) Measurement Toolkit. 2017. Available online: https://dapa-toolkit.mrc.ac.uk/ (accessed on 31 August 2021).
- Dowd, K.P.; Szeklicki, R.; Alessandro Minetto, M.; Murphy, M.H.; Polito, A.; Ghigo, E.; van der Ploeg, H.; Ekelund, U.; Maciaszek, J.; Stemplewski, R.; et al. A systematic literature review of reviews on techniques for physical activity measurement in adults: A DEDIPAC study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 15. [Google Scholar] [CrossRef] [PubMed]
- De Vet, H.C.; Terwee, C.B.; Mokkink, L.B.; Knol, D.L. Measurement in Medicine: A Practical Guide; Cambridge University Press: Cambridge, UK, 2017. [Google Scholar]
- Barber, S.E.; Jackson, C.; Hewitt, C.; Ainsworth, H.R.; Buckley, H.; Akhtar, S.; Bingham, D.D.; Routen, A.C.; Summerbell, C.; Richardson, G.; et al. Assessing the feasibility of evaluating and delivering a physical activity intervention for pre-school children: A pilot randomised controlled trial. Pilot Feasibility Stud. 2016, 2, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, J.C.; Temple, M.L.; Duck, A.; Klamm, M. Feasibility and effectiveness of two built environmental interventions on physical activity among 3–5-year-old preschoolers. J. Spec. Pediatric. Nurs. 2019, 24, e12262. [Google Scholar] [CrossRef]
- Delisle Nyström, C.; Alexandrou, C.; Henström, M.; Nilsson, E.; Okely, A.D.; Wehbe El Masri, S.; Löf, M. International Study of Movement Behaviors in the Early Years (SUNRISE): Results from SUNRISE Sweden’s Pilot and COVID-19 Study. Int J. Environ. Res. Public Health 2020, 17, 8491. [Google Scholar] [CrossRef]
- Hossain, M.S.; Deeba, I.M.; Hasan, M.; Kariippanon, K.E.; Chong, K.H.; Cross, P.L.; Ferdous, S.; Okely, A.D. International study of 24-h movement behaviors of early years (SUNRISE): A pilot study from Bangladesh. Pilot Feasibility Stud. 2021, 7, 176. [Google Scholar] [CrossRef]
- Okely, T.; Reilly, J.J.; Tremblay, M.S.; Kariippanon, K.E.; Draper, C.E.; El Hamdouchi, A.; Florindo, A.A.; Green, J.P.; Guan, H.; Katzmarzyk, P.T.; et al. Cross-sectional examination of 24-hour movement behaviours among 3- and 4-year-old children in urban and rural settings in low-income, middle-income and high-income countries: The SUNRISE study protocol. BMJ Open 2021, 11, e049267. [Google Scholar] [CrossRef]
- Phillips, S.M.; Summerbell, C.; Hobbs, M.; Hesketh, K.R.; Saxena, S.; Muir, C.; Hillier-Brown, F.C. A systematic review of the validity, reliability, and feasibility of measurement tools used to assess the physical activity and sedentary behaviour of pre-school aged children. Int J. Behav. Nutr. Phys. Act. 2021, 18, 141. [Google Scholar] [CrossRef]
- Phillips, S.M.; Summerbell, C.; Ball, H.L.; Hesketh, K.R.; Saxena, S.; Hillier-Brown, F.C. The Validity, Reliability, and Feasibility of Measurement Tools Used to Assess Sleep of Pre-school Aged Children: A Systematic Rapid Review. Front. Pediatrics 2021, 9, 770262. [Google Scholar] [CrossRef]
- Davies, G.; Reilly, J.J.; McGowan, A.J.; Dall, P.M.; Granat, M.H.; Paton, J.Y. Validity, practical utility, and reliability of the activPAL™ in preschool children. Med. Sci. Sports Exerc. 2012, 44, 761–768. [Google Scholar] [CrossRef] [Green Version]
- Cardon, G.; De Bourdeaudhuij, I. Comparison of pedometer and accelerometer measures of physical activity in preschool children. Pediatric Exerc. Sci. 2007, 19, 205–214. [Google Scholar] [CrossRef]
- Van Cauwenberghe, E.; Wooler, L.; Mackay, L.; Cardon, G.; Oliver, M. Comparison of Actical and activPAL measures of sedentary behaviour in preschool children. J. Sci. Med. Sport 2012, 15, 526–531. [Google Scholar] [CrossRef]
- Bar-Or, T.; Bar-Or, O.; Waters, H.; Hirji, A.; Russell, S. Validity and Social Acceptability of the Polar Vantage XL for Measuring Heart Rate in Preschoolers. Pediatric Exerc. Sci. 1996, 8, 115–121. [Google Scholar] [CrossRef]
- De Craemer, M.; Decraene, M.; Willems, I.; Buysse, F.; Van Driessche, E.; Verbestel, V. Objective Measurement of 24-Hour Movement Behaviors in Preschool Children Using Wrist-Worn and Thigh-Worn Accelerometers. Int J. Environ. Res. Public Health 2021, 18, 9482. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.C. Calibration of an Accelerometer to Measure Physical Activity in Preschool Children: A Feasibility Study. Master’s Thesis, University of Illinois, Champaign, IL, USA, 2015. [Google Scholar]
- Kowalski, K.; Rhodes, R.; Naylor, P.J.; Tuokko, H.; MacDonald, S. Direct and indirect measurement of physical activity in older adults: A systematic review of the literature. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Summerbell, C.D.; Moore, H.J.; Vögele, C.; Kreichauf, S.; Wildgruber, A.; Manios, Y.; Douthwaite, W.; Nixon, C.A.; Gibson, E.L.; ToyBox-study group; et al. Evidence-based recommendations for the development of obesity prevention programs targeted at preschool children. Obes. Rev. 2012, 13, 129–132. [Google Scholar] [CrossRef]
- Thabane, L.; Ma, J.; Chu, R.; Cheng, J.; Ismaila, A.; Rios, L.P.; Goldsmith, C.H. A tutorial on pilot studies: The what, why and how. BMC Med. Res. Methodol. 2010, 10, 1. [Google Scholar] [CrossRef] [Green Version]
- Lancaster, G.A.; Dodd, S.; Williamson, P.R. Design and analysis of pilot studies: Recommendations for good practice. J. Eval. Clin. Pract. 2004, 10, 307–312. [Google Scholar] [CrossRef]
- Hillier, F.; Pedley, C.; Summerbell, C. Evidence base for primary prevention of obesity in children and adolescents. Bundesgesundheitsblatt Gesundh. Gesundh. 2011, 54, 259–264. [Google Scholar] [CrossRef]
- Love, R.E.; Adams, J.; van Sluijs, E.M.F. Equity effects of children’s physical activity interventions: A systematic scoping review. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 134. [Google Scholar] [CrossRef] [Green Version]
- Cliff, D.P.; Reilly, J.J.; Okely, A.D. Methodological considerations in using accelerometers to assess habitual physical activity in children aged 0–5 years. J. Sci. Med. Sport 2009. [Google Scholar] [CrossRef] [PubMed]
- Sallis, J.F. Self-report measures of children’s physical activity. J. Sch. Health 1991, 61, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Atkin, A.J.; Gorely, T.; Clemes, S.A.; Yates, T.; Edwardson, C.; Brage, S.; Salmon, J.; Marshall, S.J.; Biddle, S.J.H. Methods of Measurement in epidemiology: Sedentary behaviour. Int. J. Epidemiol. 2012, 41, 1460–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aubert, S.; Sayavera, J.B.; González, S.A.; Janssen, I.; Manyanga, T.; Oyeyemi, A.L.; Picard, P.; Sherar, L.B.; Turner, E.; Tremblay, M.S.; et al. Global prevalence of physical activity for children and adolescents; inconsistencies, research gaps, and recommendations: A narrative review. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 81. [Google Scholar] [CrossRef]
- Quante, M.; Kaplan, E.R.; Rueschman, M.; Cailler, M.; Buxton, O.M.; Redline, S. Practical considerations in using accelerometers to assess physical activity, sedentary behavior, and sleep. Sleep Health 2015, 1, 275–284. [Google Scholar] [CrossRef] [PubMed]
- Kuzik, N.; Poitras, V.J.; Tremblay, M.S.; Lee, E.-Y.; Hunter, S.; Valeria, C. Systematic review of the relationships between combinations of movement behaviours and health indicators in the early years (0–4 years). BMC Public Health 2017, 17, 849. [Google Scholar] [CrossRef] [Green Version]
- Costa, S.; Barber, S.E.; Griffiths, P.L.; Cameron, N.; Clemes, S.A. Qualitative feasibility of using three accelerometers with 2-3-year-old children and both parents. Res. Q. Exerc. Sport 2013, 84, 295–304. [Google Scholar] [CrossRef]
- Ministry of Housing, Communities and Local Government. Indices of Deprivation 2015 Explorer; Ministry of Housing, Communities and Local Government: London, UK, 2015. [Google Scholar]
- Carney, C.E.; Buysse, D.J.; Ancoli-Israel, S.; Edinger, J.D.; Krystal, A.D.; Lichstein, K.L.; Morin, C.M. The consensus sleep diary: Standardizing prospective sleep self-monitoring. Sleep 2012, 35, 287–302. [Google Scholar] [CrossRef] [Green Version]
- Bingham, D.D.; Costa, S.; Clemes, S.A.; Routen, A.C.; Moore, H.J.; Barber, S.E. Accelerometer data requirements for reliable estimation of habitual physical activity and sedentary time of children during the early years-a worked example following a stepped approach. J. Sports Sci. 2016. [Google Scholar] [CrossRef]
- Cliff, D.P.; McNeill, J.; Vella, S.A.; Howard, S.J.; Santos, R.; Batterham, M.; Batterham, M.; Melhuish, E.; Okely, A.D.; de Rosnay, M. Adherence to 24-Hour Movement Guidelines for the Early Years and associations with social-cognitive development among Australian preschool children. BMC Public Health 2017, 17, 207–215. [Google Scholar] [CrossRef] [Green Version]
- Migueles, J.; Cadenas-Sanchez, C.; Ekelund, U.; Nyström, C.D.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, O.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Clarke, V.; Braun, C. Thematic analysis. J. Posit. Psychol. 2017, 12, 297–298. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. What Can “Thematic Analysis” Offer Health and Wellbeing Researchers. Int. J. Qual. Stud. Health Well-being 2014, 9, 26152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clarke, V.; Braun, C. Successful Qualitative Research: A Practical Guide for Beginners; Sage: London, UK, 2013. [Google Scholar]
- Mahase, E. Covid-19: Schools set to close across UK except for children of health and social care workers. Br. Med. J. 2020, 368, m1140. [Google Scholar] [CrossRef] [Green Version]
- De Decker, E.; De Craemer, M.; Santos-Lozano, A.; Van Cauwenberghe, E.; De Bourdeaudhuij, I.; Cardon, G. Validity of the ActivPAL™ and the ActiGraph monitors in preschoolers. Med. Sci. Sports Exerc. 2013, 45, 200–2011. [Google Scholar] [CrossRef]
- Van Cauwenberghe, E.; Gubbels, J.; De Bourdeaudhuij, I.; Cardon, G. Feasibility and validity of accelerometer measurements to assess physical activity in toddlers. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 67. [Google Scholar] [CrossRef] [Green Version]
- Barber, S.E.; Akhtar, S.; Jackson, C.; Bingham, D.D.; Hewitt, C.; Routen, A.; Richardson, G.; Ainsworth, H.; Moore, H.J.; Summerbell, C.D.; et al. Preschoolers in the Playground: A pilot cluster randomised controlled trial of a physical activity intervention for children aged 18 months to 4 years. Public Health Res. 2015. [Google Scholar] [CrossRef] [Green Version]
- Tracy, J.D.; Donnelly, T.; Sommer, E.C.; Heerman, W.J.; Barkin, S.L.; Buchowski, M.S. Identifying bedrest using waist-worn triaxial accelerometers in preschool children. PLoS ONE 2021, 16, e0246055. [Google Scholar] [CrossRef]
- Dobell, A.P.; Eyre, E.L.; Tallis, J.; Chinapaw, M.J.; Altenburg, T.M.; Duncan, M.J. Examining accelerometer validity for estimating physical activity in pre-schoolers during free-living activity. Scand. J. Med. Sci. Sports 2019, 29, 1618–1628. [Google Scholar] [CrossRef]
- Janssen, X.; Cliff, D.; Reilly, J.; Hinkley, T.; Jones, R.; Batterham, M.; Ekelund, U.; Brage, S.; Okely, T. Evaluation of Actical equations and thresholds to predict physical activity intensity in young children. J. Sports Sci. 2015, 33, 498–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terwee, C.B.; Prinsen, C.A.C.; Chiarotto, A.; Westerman, M.J.; Patrick, D.L.; Alonso, J.; Bouter, L.M.; de Vet, H.C.W.; Mokkink, L.B. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: A Delphi study. Qual. Life Res. 2018, 27, 1159–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolfe, D.E.; Ramsden, V.R.; Banner, D.; Graham, I.D. Using qualitative Health Research methods to improve patient and public involvement and engagement in research. Res. Involv. Engagem. 2018, 4, 49. [Google Scholar] [CrossRef] [PubMed]
- IPSOS MORI. Active Lives Survey 2019/2020, Full-Year 5 Technical Note. 2021. Available online: https://sportengland-production-files.s3.eu-west-2.amazonaws.com/s3fs-public/2021-04/Active%20Lives%20%2719-20%20Year%205%20%28full%29%20-%20Technical%20note.pdf?VersionId=v_pi0vf2bt2bfP6hlyl2kZstAxXOu8BD (accessed on 31 August 2021).
- Bennett, D.H.; Lee, K.; Cassady, D.L.; Ritz, B.; Hertz-Picciotto, I. Feasibility of using web surveys to collect time–activity data. J. Expo. Sci. Environ. Epidemiol. 2012, 22, 116–125. [Google Scholar]
- Brown, T.; Moore, T.H.; Hooper, L.; Gao, Y.; Zayegh, A.; Ijaz, S.; Elwenspoek, M.; Foxen, S.C.; Magee, L.; O’Malley, C.; et al. Interventions for preventing obesity in children. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef] [Green Version]
- Smith, B. Generalizability in qualitative research: Misunderstandings, opportunities and recommendations for the sport and exercise sciences. Qual. Res. Sport Exerc. Health 2018, 10, 137–149. [Google Scholar] [CrossRef]
- Office for National Statistics. Population Denominators by Broad Ethnic Group and for White British, Local Authorities in England and Wales: 2011 to 2019. 2011. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/adhocs/008781populationdenominatorsbybroadethnicgroupandforwhitebritishlocalauthoritiesinenglandandwales2011to2017 (accessed on 31 August 2021).



{kind=link}
{kind=link}
| Demographic Characteristics | n = 11 | |
|---|---|---|
| Sex (%) | Female | 100 |
| Ethnicity (%) | White British | 100 |
| Age of parent/carer (years) | Median | 29 |
| Range | 21–61 | |
| Age of pre-school child participant cared for (years) | Median | 3.7 |
| Range | 3.3–4.9 | |
| Education level (%) | Masters/PhD or equivalent | 0 |
| Bachelor degree or equivalent | 9 | |
| A levels or equivalent | 9 | |
| Diploma in higher education/BTEC or equivalent | 18 | |
| GCSE’s or equivalent | 27 | |
| Vocational qualifications (NVQ Level 2) | 9 | |
| National nursery examination board | 9 | |
| No formal qualifications | 9 | |
| Did not specify | 9 | |
| Employment status (%) | Working full-time | 36 |
| Working part-time | 27 | |
| Looking after the home | 9 | |
| Not working | 27 | |
| Household income per year (%) | <£4999 | 0 |
| £5000–£9999 | 9 | |
| £10,000–£14,999 | 9 | |
| £15,000–£19,999 | 18 | |
| £20,000–£24,999 | 18 | |
| £25,000–£29,999 | 18 | |
| £30,000–£34,999 | 0 | |
| £35,000–£39,999 | 9 | |
| >£40,000–£44,999 | 0 | |
| Don’t know | 18 | |
| Index Multiple Deprivation quintile (%) | 1 | 81 |
| (1 = most deprived, 5 = least deprived) | 2 | 9 |
| 3 | 0 | |
| 4 | 0 | |
| 5 | 9 | |
| Recommendations and Practical Considerations | |
|---|---|
| 1 | Context is important to parents and carers—having space to explain their child’s health status (e.g., illness) helps make measurement meaningful. |
| 2 | Ensuring measurement captures different routines to be reflective of children’s movement e.g., home vs school, weekday vs weekend. |
| 3 | Devices worn as watches or placed out of sight were preferred. Devices stuck to the skin were less favourable. |
| 4 | Smaller devices preferred for 24 hour movement measurement, but different devices may be favoured if measuring only one proportion of the 24 hour day (e.g., larger devices for day time, smaller devices for night time). |
| 5 | Removal of devices by young children may be inevitable so include detailed device wear time logs with plenty of space to report when the device is worn/removed. |
| 6 | ‘Child-friendly’ devices—suitable for playing in mud, slime, sand and water—and no small parts! Demonstrate safety of devices prior to studies. |
| 7 | Written and visual (video demonstrations) study instructions are most helpful to act as a reminder during the measurement period. |
| 8 | Frame research to young children so that taking part is ‘cool’—devices can give ‘superpowers’ or ‘magic’. |
| 9 | Modify tools to make them ‘childlike’ e.g., so children can personalise their device with stickers or provide devices with colourful belts or with children’s favourite characters on. |
| 10 | Daily reporting easier for proxy reported tools—recall can be particularly challenging with young children. Ensure that age appropriate activities are included on the tool. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phillips, S.M.; Summerbell, C.; Hesketh, K.R.; Saxena, S.; Hillier-Brown, F.C. Parental Views on the Acceptability and Feasibility of Measurement Tools Used to Assess Movement Behaviour of Pre-School Children: A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 3733. https://doi.org/10.3390/ijerph19063733
Phillips SM, Summerbell C, Hesketh KR, Saxena S, Hillier-Brown FC. Parental Views on the Acceptability and Feasibility of Measurement Tools Used to Assess Movement Behaviour of Pre-School Children: A Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(6):3733. https://doi.org/10.3390/ijerph19063733
Chicago/Turabian StylePhillips, Sophie M., Carolyn Summerbell, Kathryn R. Hesketh, Sonia Saxena, and Frances C. Hillier-Brown. 2022. "Parental Views on the Acceptability and Feasibility of Measurement Tools Used to Assess Movement Behaviour of Pre-School Children: A Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 6: 3733. https://doi.org/10.3390/ijerph19063733