
Effects of Classical Breathing Exercises on Posture, Spinal and Chest Mobility among Female University Students Compared to Currently Popular Training Programs



Abstract
:1. Introduction
2. Materials and Methods
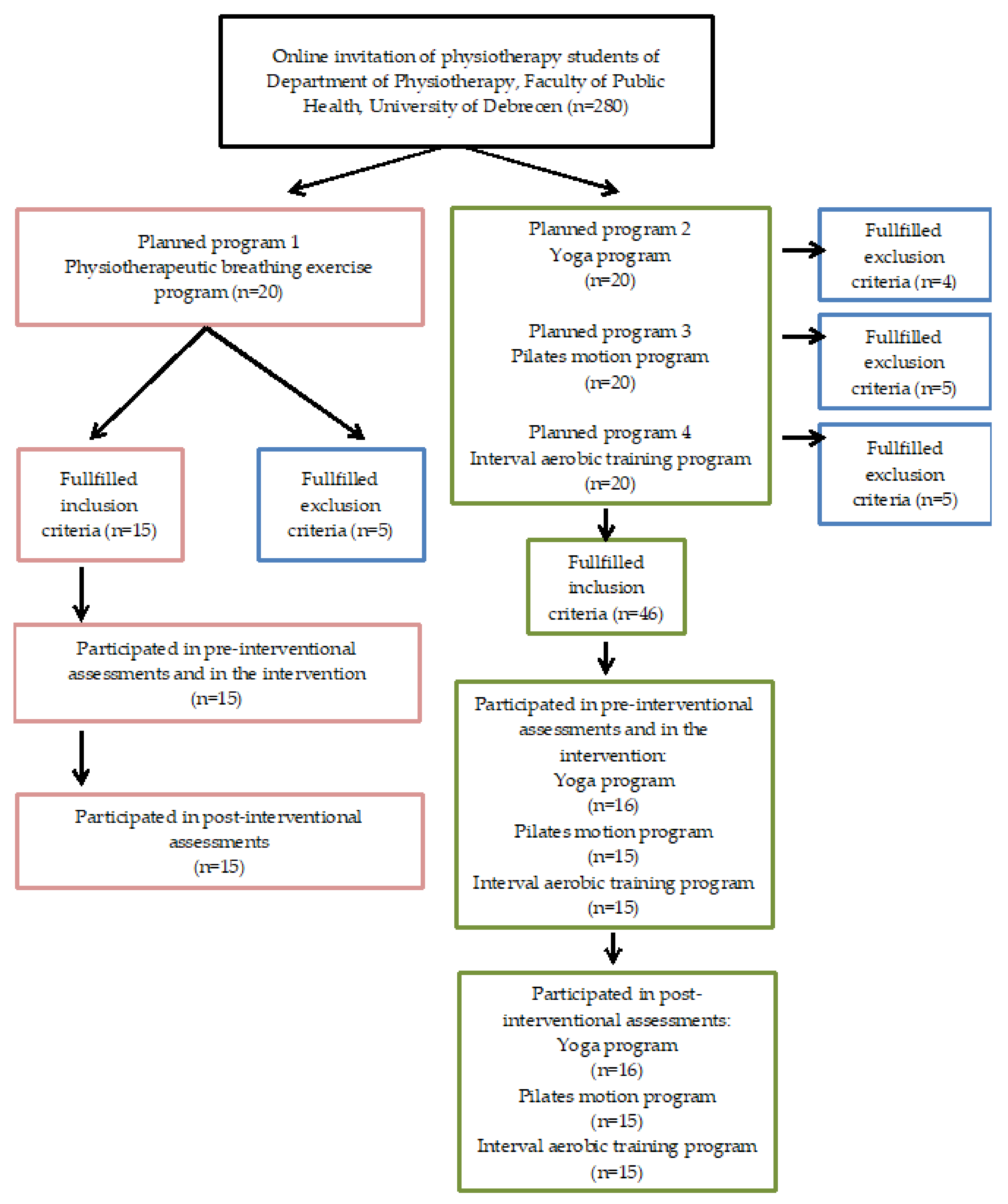
2.1. Participants
2.2. Outcome Measures by Standardized Clinical Tests
2.2.1. Assessment of Chest Expansion
2.2.2. Schober’s Test
2.2.3. Occiput-to-Wall Distance Test (OWD)
2.2.4. Fingertip-to-Floor Test
2.2.5. Trunk Side Bending (Lateral-Flexion) Test
2.2.6. Heart Rate Monitoring—Pulse Control
2.3. Applied Training Programmes
2.3.1. Breathing Exercise (BE) Programme
2.3.2. Yoga (Y) Programme
2.3.3. Pilates (P) Programme
2.3.4. Interval Training (IT) Program—Dynamic Aerobic Endurance Training
2.4. Statistical Analysis
2.5. Sample Size Calculation
2.6. Ethics
3. Results
3.1. Description of the Participants
3.2. Chest Expansion Results
3.3. Schober’s Test Results
3.4. Occiput-to-Wall Distance Test Results
3.5. Fingertip-to-Floor Test Results
3.6. Trunk Side Bending (Lateral Flexion) Test Results
3.7. Results of Kruskal–Wallis ANOVA and Dunn’s Post Hoc Tests
3.8. Results of Differences between the before and after Values Related to the Four Motion Programs
3.9. The Spearman’s Correlation Analysis Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Castro, O.; Bennie, J.; Vergeer, I.; Bosselut, G.; Biddle, S.J.H. How Sedentary Are University Students? A Systematic Review and Meta-Analysis. Prev. Sci. 2020, 21, 332–343. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Kim, Y. Effect of university students’ sedentary behavior on stress, anxiety, and depression. Perspect. Psychiatr. Care 2018, 55, 164–169. [Google Scholar] [CrossRef] [Green Version]
- Nikitara, K.; Odani, S.; Demenagas, N.; Rachiotis, G.; Symvoulakis, E.; Vardavas, C. Prevalence and correlates of physical inactivity in adults across 28 European countries. Eur. J. Public Health 2021, 31, 840–845. [Google Scholar] [CrossRef] [PubMed]
- López-Fernández, J.; López-Valenciano, A.; Mayo, X.; Liguori, G.; Lamb, M.A.; Copeland, R.J.; Jiménez, A. No changes in adolescent’s sedentary behaviour across Europe between 2002 and 2017. BMC Public Health 2021, 21, 784. [Google Scholar] [CrossRef] [PubMed]
- Czakwari, A.; Czernicki, K.; Durmala, J. Faulty posture and style of life in young adults. Stud. Health Technol. Inf. 2008, 140, 107–110. [Google Scholar] [CrossRef]
- Huynh, Q.L.; Blizzard, C.L.; Sharman, J.; Magnussen, C.; Dwyer, T.; Venn, A.J. The cross-sectional association of sitting time with carotid artery stiffness in young adults. BMJ Open 2014, 4, e004384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.; Cho, M.; Park, Y.; Yang, Y. Effect of an exercise program for posture correction on musculoskeletal pain. J. Phys. Ther. Sci. 2015, 27, 1791–1794. [Google Scholar] [CrossRef] [Green Version]
- Neumann, D.A. Kinesiology of the Musculoskeletal System. Chapter 9,10,11 Kinesiology of Mastication and Ventilation, Part 2: Ventilation, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2009; pp. 312–318, 350–365, 379–412, 439–450. [Google Scholar]
- Magee, D. Thoracic (Dorsal) Spine, Lumbar Spine. In Orthopedic Physical Assessment, 6th ed.; Elsevier: Amsterdam, The Netherlands, 2013; pp. 508–648, 1017–1053. [Google Scholar]
- Bakar, Y.; Tuğral, A.; Özel, A.; Altuntaş, Y.D. Comparison of a 12-Week Whole-Body Exergaming Program on Young Adults: Differentiation in Flexibility, Muscle Strength, Reaction Time, and Walking Speed Between Sexes. Clin. Nurs. Res. 2018, 29, 424–432. [Google Scholar] [CrossRef]
- Powers, S.K.; Howley, E.T. Exercise Physiology: Theory and Application to Fitness and Performance, 8th ed.; McGraw-Hill: Boston, MA, USA, 2012; pp. 218–245, 351–367, 479–498. [Google Scholar]
- Tomaszewska, A.; Pawlicka-Lisowska, A. Evaluation of an influence of systematic motor activity on the body posture of young people. Pol. Merkur. Lek. 2014, 36, 336–340. [Google Scholar]
- Dunleavy, K.; Kava, K.; Goldberg, A.; Malek, M.; Talley, S.; Tutag-Lehr, V.; Hildreth, J. Comparative effectiveness of Pilates and yoga group exercise interventions for chronic mechanical neck pain: Quasi-randomised parallel controlled study. Physiotherapy 2016, 102, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Eliks, M.; Zgorzalewicz-Stachowiak, M.; Zeńczak-Praga, K. Application of Pilates-based exercises in the treatment of chronic non-specific low back pain: State of the art. Postgrad. Med. J. 2019, 95, 41–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valenza, M.; Rodríguez-Torres, J.; Cabrera-Martos, I.; Díaz-Pelegrina, A.; Aguilar-Ferrándiz, M.; Castellote-Caballero, Y. Results of a Pilates exercise program in patients with chronic non-specific low back pain: A randomized controlled trial. Clin. Rehabil. 2016, 31, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Kuppusamy, M.; Kamaldeen, D.; Pitani, R.; Amaldas, J.; Shanmugam, P. Effects of Bhramari Pranayama on health—A systematic review. J. Tradit. Complement. Med. 2017, 8, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Noggle, J.J.; Steiner, N.J.; Minami, T.; Khalsa, S.B. Benefits of Yoga for Psychosocial Well-Being in a US High School Curriculum. J. Dev. Behav. Pediatr. 2012, 33, 193–201. [Google Scholar] [CrossRef] [Green Version]
- Birkel, D.A.; Edgren, L. Hatha yoga: Improved vital capacity of college students. Altern. Ther. Health Med. 2000, 6, 55–63. [Google Scholar] [PubMed]
- Tousignant, M.; Poulin, L.; Marchand, S.; Viau, A.; Place, C. The Modified—Modified Schober Test for range of motion assessment of lumbar flexion in patients with low back pain: A study of criterion validity, intra- and inter-rater reliability and minimum metrically detectable change. Disabil. Rehabil. 2005, 27, 553–559. [Google Scholar] [CrossRef]
- Castro, M.P.; Stebbings, S.M.; Milosavljevic, S.; Bussey, M.D. Construct validity of clinical spinal mobility tests in ankylosing spondylitis: A systematic review and meta-analysis. Clin. Rheumatol. 2015, 35, 1777–1787. [Google Scholar] [CrossRef]
- Wiyanad, A.; Chokphukiao, P.; Suwannarat, P.; Thaweewannakij, T.; Wattanapan, P.; Gaogasigam, C.; Amatachaya, P.; Amatachaya, S. Is the occiput-wall distance valid and reliable to determine the presence of thoracic hyperkyphosis? Musculoskelet. Sci. Pract. 2018, 38, 63–68. [Google Scholar] [CrossRef]
- Ekedahl, H.; Jönsson, B.; Frobell, R.B. Fingertip-to-Floor Test and Straight Leg Raising Test: Validity, Responsiveness, and Predictive Value in Patients With Acute/Subacute Low Back Pain. Arch. Phys. Med. Rehabil. 2012, 93, 2210–2215. [Google Scholar] [CrossRef] [Green Version]
- Perret, C.; Poiraudeau, S.; Fermanian, J.; Colau, M.M.L.; Benhamou, M.A.M.; Revel, M. Validity, reliability, and responsiveness of the fingertip-to-floor test. Arch. Phys. Med. Rehabil. 2001, 82, 1566–1570. [Google Scholar] [CrossRef] [PubMed]
- Zuberbier, O.A.; Kozlowski, A.J.; Hunt, D.G.; Berkowitz, J.; Schultz, I.Z.; Crook, J.M.; Milner, R.A. Analysis of the Convergent and Discriminant Validity of Published Lumbar Flexion, Extension, and Lateral Flexion Scores. Spine 2001, 26, E472–E478. [Google Scholar] [CrossRef] [PubMed]
- Saur, P.M.M.; Ensink, F.-B.M.; Frese, K.; Seeger, D.; Hildebrandt, J. Lumbar Range of Motion: Reliability and Validity of the Inclinometer Technique in the Clinical Measurement of Trunk Flexibility. Spine 1996, 21, 1332–1338. [Google Scholar] [CrossRef] [PubMed]
- Debouche, S.; Pitance, L.; Robert, A.; Liistro, G.; Reychler, G. Reliability and Reproducibility of Chest Wall Expansion Measurement in Young Healthy Adults. J. Manip. Physiol. Ther. 2016, 39, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Samo, D.G.; Chen, S.-P.C.; Crampton, A.R.; Chen, E.H.; Conrad, K.M.; Egan, L.; Mitton, J. Validity of Three Lumbar Sagittal Motion Measurement Methods. J. Occup. Environ. Med. 1997, 39, 209–216. [Google Scholar] [CrossRef]
- Nattrass, C.L.; Nitschke, J.E.; Disler, P.B.; Chou, M.J.; Ooi, K.T. Lumbar spine range of motion as a measure of physical and functional impairment: An investigation of validity. Clin. Rehabil. 1999, 13, 211–218. [Google Scholar] [CrossRef]
- Limongi, V.; dos Santos, D.; da Silva, A.; Ataide, E.; Mei, M.; Udo, E.; Boin, I.; Stucchi, R. Effects of a Respiratory Physiotherapeutic Program in Liver Transplantation Candidates. Transplant. Proc. 2014, 46, 1775–1777. [Google Scholar] [CrossRef]
- Westerdahl, E. Optimal technique for deep breathing exercises after cardiac surgery. Minerva. Anestesiol. 2015, 81, 678–683. [Google Scholar]
- Clarkson, H.M. Head, neck and trunk. In Musculoskeletal Assessment—Joint Range of Motion and Manual Muscle Strength, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2000; pp. 68–77. [Google Scholar]
- Norkin, C.C.; White, D.J. The thoracic and lumbar spine. In Measurement of Joint Motion, 4th ed.; F.A. Davis Company: Philadelphia, PA, USA, 2009; pp. 365–407. [Google Scholar]
- Heuft-Dorenbosch, L.; Vosse, D.; Landewé, R.; Spoorenberg, A.; Dougados, M.; Mielants, H.; Van Der Tempel, H.; Van Der Linden, S.; Van Der Heijde, D. Measurement of spinal mobility in ankylosing spondylitis: Comparison of occiput-to-wall and tragus-to-wall distance. J. Rheumatol. 2004, 31, 1779–1784. [Google Scholar]
- Grieco, C.R.; Colberg, S.R.; Somma, C.T.; Thompson, A.G.; Vinik, A.I. Acute Effect of Breathing Exercises on Heart Rate Variability in Type 2 Diabetes: A Pilot Study. J. Altern. Complement. Med. 2014, 20, 642–648. [Google Scholar] [CrossRef]
- Chiang, L.-C.; Ma, W.-F.; Huang, J.-L.; Tseng, L.-F.; Hsueh, K.-C. Effect of relaxation-breathing training on anxiety and asthma signs/symptoms of children with moderate-to-severe asthma: A randomized controlled trial. Int. J. Nurs. Stud. 2009, 46, 1061–1070. [Google Scholar] [CrossRef] [PubMed]
- Meier, M.; Wirz, L.; Dickinson, P.; Pruessner, J.C. Laughter yoga reduces the cortisol response to acute stress in healthy individuals. Stress 2020, 24, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Geremia, J.M.; Iskiewicz, M.M.; Marschner, R.A.; Lehnen, T.E.; Lehnen, A.M. Effect of a physical training program using the Pilates method on flexibility in elderly subjects. Age 2015, 37, 119. [Google Scholar] [CrossRef] [Green Version]
- Daussin, F.N.; Zoll, J.; Dufour, S.P.; Ponsot, E.; Lonsdorfer-Wolf, E.; Doutreleau, S.; Mettauer, B.; Piquard, F.; Geny, B.; Richard, R. Effect of interval versus continuous training on cardiorespiratory and mitochondrial functions: Relationship to aerobic performance improvements in sedentary subjects. Am. J. Physiol. Integr. Comp. Physiol. 2008, 295, R264–R272. [Google Scholar] [CrossRef] [Green Version]
- StataCorp. Stata Statistical Software: Release 13; StataCorp LP: College Station, TX, USA, 2013. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viitanen, J.V.; Heikkilä, S.; Kokko, M.-L.; Kautiainen, H. Clinical Assessment of Spinal Mobility Measurements in Ankylosing Spondylitis: A Compact Set for Follow-up and Trials? Clin. Rheumatol. 2000, 19, 131–137. [Google Scholar] [CrossRef]
- Çelenay, T.; Kaya, D.; Özüdoğru, A. Spinal postural training: Comparison of the postural and mobility effects of electrotherapy, exercise, biofeedback trainer in addition to postural education in university students. J. Back Musculoskelet. Rehabil. 2015, 28, 135–144. [Google Scholar] [CrossRef]
- Kisner, C.; Colby, L.A.; Borstad, J. Management of pulmonary conditions, chapter 19. In Therapeutic Exercise: Foundation and Techniques, 4th ed.; F.A. Davis Company: Philadelphia, PA, USA, 2002; pp. 749–757. [Google Scholar]
- Frownfelter, D.; Dean, E.; Stout, M.; Kruger, R.; Anthony, J. Cardiovascular and pulmonary Physical Therapy: Interventions, chapter 26–27. In Cardiovascular and Pulmonary Physical Therapy, 5th ed.; Elsevier: Amsterdam, The Netherlands, 2012; pp. 419–426, 435–450. [Google Scholar]
- Csepregi, É.; Szekanecz, Z.; Szántó, S. The effects of breathing exercises in comparison with other exercise programs on cardiorespiratory fitness among healthy female college students. J. Sports Med. Phys. Fit. 2020, 60, 62–68. [Google Scholar] [CrossRef]


{kind=link}
| Groups | Breathing Exercises (BE) | Yoga (Y) | Pilates (P) | Interval Training (IT) |
|---|---|---|---|---|
| Age (year) | 20.1 ± 0.99 | 20.4 ± 1.40 | 20.3 ± 1.20 | 21.2± 1.21 |
| Number of participants (female:male) | 15:0 | 16:0 | 15:0 | 15:0 |
| Body Mass Index (kg/m2) | 20.97 ± 2.51 | 21.35 ± 3.42 | 20.89 ± 2.29 | 24.49 ± 2.64 |
| Body fat (%) | 30.15 ± 5.05 | 29.66 ± 7.50 | 28.29 ± 5.93 | 34.31 ± 4.82 |
| Chest Expansion—Axillar Level (cm) | |||||||
|---|---|---|---|---|---|---|---|
| before | after | ||||||
| Q1 | Median | Q3 | Q1 | Median | Q3 | p-Value | |
| Breathing exercises (BE) (n = 15) | 3.5 | 4.5 (min 3.0; max 7.0) | 5.0 | 6.0 | 7.0 (min 6.0; max 8.0) | 8.0 | ≤0.001 |
| Yoga (Y) (n = 16) | 4.0 | 5.0 (min 3.0; max 10.0) | 6.0 | 6.0 | 7.5 (min 4.0; max 9.0) | 8.0 | ≤0.01 |
| Pilates (P) (n = 15) | 4.0 | 5.0 (min 2.0; max 9.0) | 8.0 | 5.0 | 6.0 (min 4.0; max 10.0) | 9.0 | ≤0.01 |
| Interval training (IT) (n = 15) | 5.0 | 6.0 (min 4.0; max 8.0) | 7.0 | 5.0 | 7.0 (min 4.0; max 10.0) | 8.0 | <0.05 |
| Schober’s Test (cm) | |||||||
|---|---|---|---|---|---|---|---|
| before | after | ||||||
| Q1 | Median | Q3 | Q1 | Median | Q3 | p-Value | |
| Breathing exercises (BE) (n = 15) | 4.5 | 5.0 (min 4.0; max 6.5) | 6.0 | 5.0 | 5.5 (min 5.0; max 6.5) | 6.0 | <0.05 |
| Yoga (Y) (n = 16) | 3.0 | 4.0 (min 2.0; max 7.0) | 6.0 | 5.0 | 6.0 (min 3.0; max 7.0) | 7.0 | ≤0.01 |
| Pilates (P) (n = 15) | 4.0 | 5.0 (min 3.0; max 7.0) | 6.0 | 6.0 | 6.0 (min 3.0; max 7.0) | 7.0 | ≤0.01 |
| Interval training (IT) (n = 15) | 4.5 | 5.5 (min 3.0; max 7.0) | 6.0 | 5.0 | 5.5 (min 4.0; max 8.0) | 6.0 | 0.271 |
| Occiput-to-Wall Distance Test (cm) | |||||||
|---|---|---|---|---|---|---|---|
| before | after | ||||||
| Q1 | Median | Q3 | Q1 | Median | Q3 | p-Value | |
| Breathing exercises (BE) (n = 15) | 3.5 | 4.0 (min 3.0; max 5.0) | 4.5 | 1.0 | 2.0 (min 1.0; max 3.0) | 2.0 | ≤0.001 |
| Yoga (Y) (n = 16) | 1.0 | 3.0 (min 0.0; max 9.0) | 4.5 | 0.0 | 0.0 (min 0.0; max 8.0) | 0.0 | ≤0.01 |
| Pilates (P) (n = 15) | 0.0 | 2.0 (min 0.0; max 10.0) | 5.0 | 0.0 | 0.0 (min 0.0; max 4.0) | 0.0 | ≤0.01 |
| Interval training (IT) (n = 15) | 0.0 | 1.5 (min 0.0; max 4.5) | 3.0 | 0.0 | 1.5 (min 0.0; max 6.0) | 2.0 | 0.917 |
| Fingertip-to-Floor Test (cm) | |||||||
|---|---|---|---|---|---|---|---|
| before | after | ||||||
| Q1 | Median | Q3 | Q1 | Median | Q3 | p-Value | |
| Breathing exercises (BE) (n = 15) | 0.0 | 0.0 (min 0.0; max 22.5) | 5.0 | 0.0 | 0.0 (min 0.0; max 10.0) | 0.0 | 0.056 |
| Yoga (Y) (n = 16) | 0.0 | 0.0 (min 0.0; max 23.0) | 5.0 | 0.0 | 0.0 (min 0.0; max 16.0) | 0.0 | <0.05 |
| Pilates (P) (n = 15) | 0.0 | 1.0 (min 0.0; max 21.0) | 4.0 | 0.0 | 0.0 (min 0.0; max 9.0) | 0.0 | <0.01 |
| Interval training (IT) (n = 15) | 0.0 | 0.0 (min 0.0; max 3.0) | 0.0 | 0.0 | 0.0 (min 0.0; max 6.0) | 0.0 | - |
| Trunk Side Bending (Lateral Flexion) to RIGHT Side (cm) | |||||||
|---|---|---|---|---|---|---|---|
| before | after | ||||||
| Q1 | Median | Q3 | Q1 | Median | Q3 | p-Value | |
| Breathing exercises (BE) (n = 15) | 40.0 | 42.0 (min 33.0; max 46.0) | 44.0 | 35.0 | 39.0 (min 28.0; max 42.0) | 40.0 | ≤0.001 |
| Yoga (Y) (n = 16) | 41.5 | 42.5 (min 39.0; max 52.0) | 46.5 | 39.5 | 42.0 (min 35.0; max 49.0) | 46.0 | 0.254 |
| Pilates (P) (n = 15) | 39.0 | 41.0 (min 35.0; max 48.0) | 46.0 | 36.0 | 39.0 (min 35.0; max 48.0) | 45.0 | 0.136 |
| Interval training (IT) (n = 15) | 41.0 | 45.5 (min 36.5; max 51.5) | 47.0 | 38.0 | 43.0 (min 34.0; max 48.0) | 45.0 | ≤0.01 |
| Trunk Side Bending (Lateral Flexion) to LEFT Side (cm) | |||||||
|---|---|---|---|---|---|---|---|
| before | after | ||||||
| Q1 | Median | Q3 | Q1 | Median | Q3 | p-Value | |
| Breathing exercises (BE) (n = 15) | 40.0 | 42.5 (min 30.5; max 48.0) | 45.0 | 37.0 | 40.0 (min 29.0; max 43.0) | 41.0 | ≤0.001 |
| Yoga (Y) (n = 16) | 40.5 | 44.0 (min 37.0; max 49.0) | 46.5 | 39.0 | 42.5 (min 28.0; max 48.0) | 45.0 | 0.156 |
| Pilates (P) (n = 15) | 40.0 | 42.0 (min 35.0; max 49.0) | 46.0 | 37.0 | 40.0 (min 34.0; max 49.0) | 45.0 | <0.05 |
| Interval training (IT) (n = 15) | 42.0 | 45.0 (min 37.0; max 53.0) | 49.0 | 38.5 | 42.5 (min 36.0; max 48.5) | 47.0 | <0.05 |
| Physical Examination Tests | Compared Programs | p Value |
|---|---|---|
| Occiput-to-wall distance test before the intervention | Breathing-Interval | 0.004 |
| Occiput-to-wall distance test after the intervention | Breathing-Pilates | 0.002 |
| Occiput-to-wall distance test after the intervention | Breathing-Yoga | 0.004 |
| Occiput-to-wall distance test after the intervention | Interval-Pilates | 0.038 |
| Occiput-to-wall distance test after the intervention | Interval-Yoga | 0.036 |
| Side bending to the right after the intervention | Breathing-Interval | 0.028 |
| Side bending to the right after the intervention | Breathing-Yoga | 0.030 |
| BEFORE (Median [IQR]) | AFTER (Median [IQR]) | p Value | |
|---|---|---|---|
| Schober test | 5 (4–6) | 6 (5–6) | <0.001 |
| Occiput-to-wall distance test | 3 (1–4) | 1 (0–2) | <0.001 |
| Fingertip-to-floor test | 0 (0–1) | 0 (0–0) | 0.001 |
| Side bending (lateral flexion) to the right | 42 (40–46) | 40 (38–44) | <0.001 |
| Side bending (lateral flexion) to the left | 44 (40–46.5) | 41 (38–44) | <0.001 |
| Chest expansion | 5 (4–6) | 7 (6–8) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Csepregi, É.; Gyurcsik, Z.; Veres-Balajti, I.; Nagy, A.C.; Szekanecz, Z.; Szántó, S. Effects of Classical Breathing Exercises on Posture, Spinal and Chest Mobility among Female University Students Compared to Currently Popular Training Programs. Int. J. Environ. Res. Public Health 2022, 19, 3728. https://doi.org/10.3390/ijerph19063728
Csepregi É, Gyurcsik Z, Veres-Balajti I, Nagy AC, Szekanecz Z, Szántó S. Effects of Classical Breathing Exercises on Posture, Spinal and Chest Mobility among Female University Students Compared to Currently Popular Training Programs. International Journal of Environmental Research and Public Health. 2022; 19(6):3728. https://doi.org/10.3390/ijerph19063728
Chicago/Turabian StyleCsepregi, Éva, Zsuzsanna Gyurcsik, Ilona Veres-Balajti, Attila Csaba Nagy, Zoltán Szekanecz, and Sándor Szántó. 2022. "Effects of Classical Breathing Exercises on Posture, Spinal and Chest Mobility among Female University Students Compared to Currently Popular Training Programs" International Journal of Environmental Research and Public Health 19, no. 6: 3728. https://doi.org/10.3390/ijerph19063728