
A Simple Method to Quantify Outward Leakage of Medical Face Masks and Barrier Face Coverings: Implication for the Overall Filtration Efficiency

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Theoretical Model
2.2. Experimental Set Up
2.3. Data Analysis
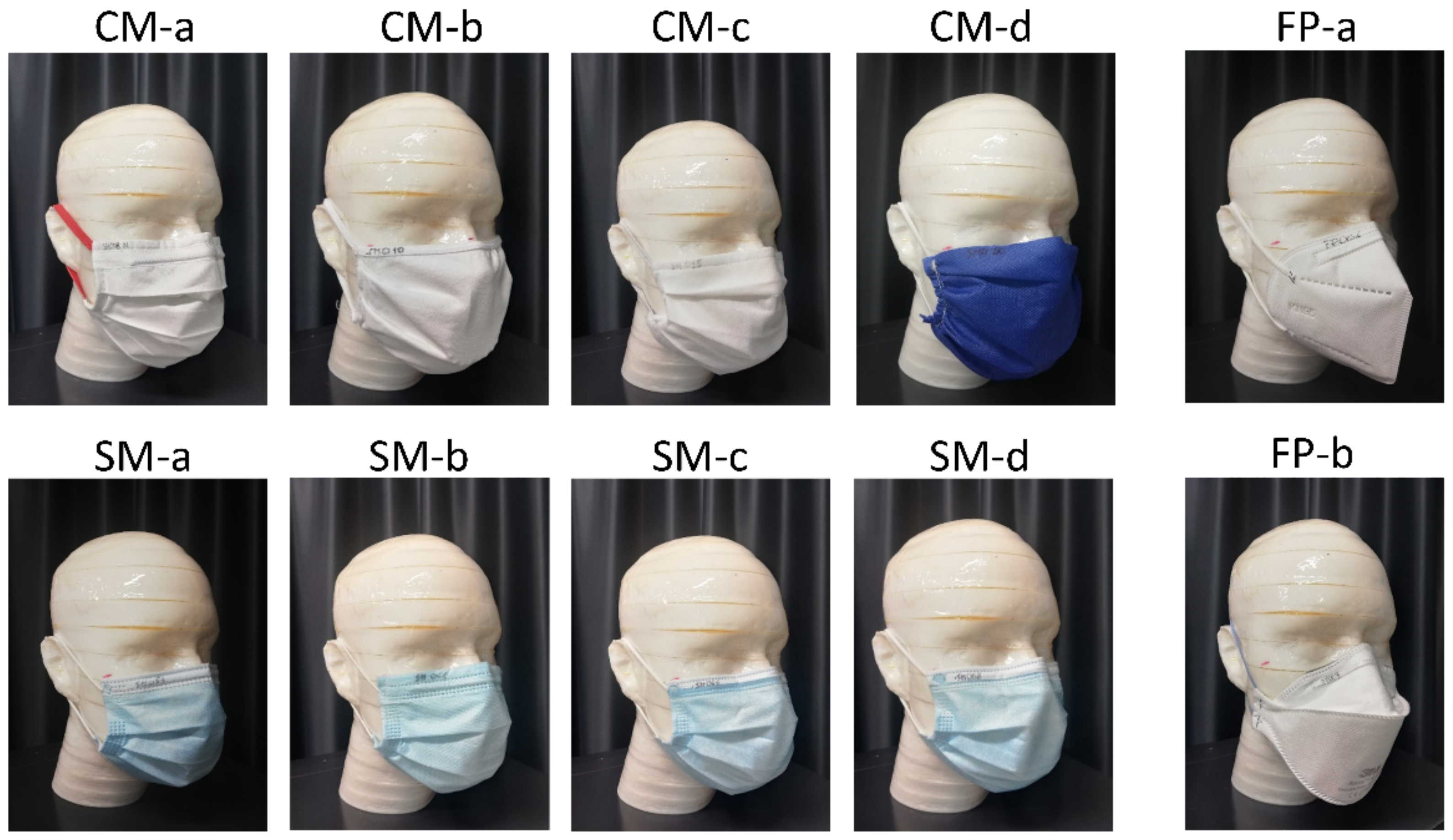
2.4. Facemasks and Respirators Tested in the Study
2.5. Statistical Analysis
3. Results
3.1. Mask Resistance Features
3.2. Leak Quantification according to Mask Type
3.3. Leakage Quantification according to Wearing Style
3.4. Total Filtration Efficiency
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Yu, C.; Qu, J.; Zhang, L.; Jiang, S.; Huang, D.; Chen, B.; Zhang, Z.; Guan, W.; Ling, Z.; et al. Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1275–1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aliabadi, A.A.; Rogak, S.N.; Green, S.I.; Bartlett, K.H. CFD Simulation of Human Coughs and Sneezes: A Study in Droplet Dispersion, Heat, and Mass Transfer. ASME Int. Mech. Eng. Congr. Expo. 2010, 7, 1051–1060. [Google Scholar] [CrossRef]
- Leung, N.H.L.; Chu, D.K.W.; Shiu, E.Y.C.; Chan, K.-H.; McDevitt, J.J.; Hau, B.J.P.; Yen, H.-L.; Li, Y.; Ip, D.K.M.; Peiris, J.S.M.; et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat. Med. 2020, 26, 676–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, W.E.; Li, Z.; Chiew, C.J.; Yong, S.E.; Toh, M.P.; Lee, V.J. Presymptomatic Transmission of SARS-CoV-2—Singapore, January 23–March 16, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 411–415. [Google Scholar] [CrossRef] [Green Version]
- Bae, S.H.; Shin, H.; Koo, H.-Y.; Lee, S.W.; Yang, J.M.; Yon, D.K. Asymptomatic Transmission of SARS-CoV-2 on Evacuation Flight. Emerg. Infect. Dis. 2020, 26, 2705–2708. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Sun, W.; Huang, J.; Gamber, M.; Wu, J.; He, G. Indirect Virus Transmission in Cluster of COVID-19 Cases, Wenzhou, China, 2020. Emerg. Infect. Dis. 2020, 26, 1343–1345. [Google Scholar] [CrossRef]
- Xie, C.; Zhao, H.; Li, K.; Zhang, Z.; Lu, X.; Peng, H.; Wang, D.; Chen, J.; Zhang, X.; Wu, D.; et al. The evidence of indirect transmission of SARS-CoV-2 reported in Guangzhou, China. BMC Public Health 2020, 20, 1202. [Google Scholar] [CrossRef]
- MacIntyre, C.R.; Chughtai, A.A. Facemasks for the prevention of infection in healthcare and community settings. BMJ 2015, 350, h694. [Google Scholar] [CrossRef]
- Sinha, P.; Reifler, K.; Rossi, M.; Sagar, M. Coronavirus Disease 2019 Mitigation Strategies Were Associated With Decreases in Other Respiratory Virus Infections. Open Forum Infect. Dis. 2021, 8, 105. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Nguyen, T.M.; Kim, J.H. Infectious Respiratory Diseases Decreased during the COVID-19 Pandemic in South Korea. Int. J. Environ. Res. Public Health 2021, 18, 6008. [Google Scholar] [CrossRef] [PubMed]
- MacIntyre, C.R.; Cauchemez, S.; Dwyer, D.E.; Seale, H.; Cheung, P.; Browne, G.; Fasher, M.; Wood, J.; Gao, Z.; Booy, R.; et al. Face Mask Use and Control of Respiratory Virus Transmission in Households. Emerg. Infect. Dis. 2009, 15, 233–241. [Google Scholar] [CrossRef]
- Howard, J.; Huang, A.; Li, Z.; Tufekci, Z.; Zdimal, V.; van der Westhuizen, H.-M.; von Delft, A.; Price, A.; Fridman, L.; Tang, L.-H.; et al. An evidence review of face masks against COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2014564118. [Google Scholar] [CrossRef] [PubMed]
- Faridi, S.; Brook, R.D.; Hassanvand, M.S.; Nodehi, R.N.; Shamsipour, M.; Tajdini, M.; Naddafi, K.; Sadeghian, S. Cardiovascular health effects of wearing a particulate-filtering respirator to reduce particulate matter exposure: A randomized crossover trial. J. Hum. Hypertens. 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Faridi, S.; Nodehi, R.N.; Sadeghian, S.; Tajdini, M.; Hoseini, M.; Yunesian, M.; Nazmara, S.; Hassanvand, M.S.; Naddafi, K. Can respirator face masks in a developing country reduce exposure to ambient particulate matter? J. Expo. Sci. Environ. Epidemiol. 2020, 30, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Deng, Z.; Shi, D. How effective is a mask in preventing COVID-19 infection? Med. Devices Sens. 2021, 4, e10163. [Google Scholar] [CrossRef]
- Order: Wearing of Face Masks While on Conveyances and at Transportation Hubs|Quarantine|CDC. Available online: https://www.cdc.gov/quarantine/masks/mask-travel-guidance.html (accessed on 29 November 2021).
- When and How to Use Masks. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/when-and-how-to-use-masks (accessed on 29 November 2021).
- Okeagu, C.N.; Reed, D.S.; Sun, L.; Colontonio, M.M.; Rezayev, A.; Ghaffar, Y.A.; Kaye, R.J.; Liu, H.; Cornett, E.M.; Fox, C.J.; et al. Principles of supply chain management in the time of crisis. Best Pract. Res. Clin. Anaesthesiol. 2021, 35, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Rondinone, D.L.; Godfrey, A.B.; Arangdad, S.R.; Jose, A.U.; Khamkar, A.A.; Anilkumar, A.P.; Girgaonkar, R. Challenges in the Supply Chain for Personal Protective Equipment (PPE) during COVID-19. J. Text. Appar. Technol. Manag. 2021, 12, 1–23. [Google Scholar]
- Tessarolo, F.; Nollo, G.; Maniglio, D.; Rigoni, M.; Benedetti, L.; Helfer, F.; Corradi, I.; Rovati, L.; Ferrari, A.; Piccini, M.; et al. Testing Surgical Face Masks in an Emergency Context: The Experience of Italian Laboratories during the COVID-19 Pandemic Crisis. Int. J. Environ. Res. Public Health 2021, 18, 1462. [Google Scholar] [CrossRef]
- Krishan, B.; Gupta, D.; Vadlamudi, G.; Sharma, S.; Chakravortty, D.; Basu, S. Efficacy of homemade face masks against human coughs: Insights on penetration, atomization, and aerosolization of cough droplets. Phys. Fluids 2021, 33, 093309. [Google Scholar] [CrossRef]
- Hao, W.; Xu, G.; Wang, Y. Factors influencing the filtration performance of homemade face masks. J. Occup. Environ. Hyg. 2021, 18, 128–138. [Google Scholar] [CrossRef] [PubMed]
- ASTM F23. Committee on Personal Protective Clothing and Equipment. ASTM F3502-21. Standard Specification for Barrier Face Coverings. 2021. Available online: https://www.astm.org/f3502-21.html (accessed on 14 March 2022).
- European Committee for Standardisation Workshop Agreement. CWA 17553:2020 E; Community Face Coverings—Guide to Minimum Requirements, Methods of Testing and Use. CEN-CENELEC: Brussels, Belgium, 2020.
- European Center for Disease Prevention and Control. Using Face Masks in the Community Using Face Masks in the Community—Reducing COVID-19 Transmission from Potentially Asymptomatic or Pre-Symptomatic People through the Use of Face Masks, ECDC-European Center for Disease Prevention and Control, ECDC Technical Report, Stockholm, 8 April 2020. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/COVID-19-use-face-masks-community.pdf (accessed on 15 March 2022).
- Advice on the Use of Masks in the Community, during Home Care and in Healthcare Settings in the Context of the Novel Coronavirus (COVID-19) Outbreak. Available online: https://www.who.int/publications-detail-redirect/advice-on-the-use-of-masks-in-the-community-during-home-care-and-in-healthcare-settings-in-the-context-of-the-novel-coronavirus-(2019-ncov)-outbreak (accessed on 9 November 2020).
- European Committee for Standardization European Standard. EN 14683:2019+AC; Medical Face Masks—Requirements and Test Methods. European Standard: Brussels, Belgium, 2019.
- Standard Test Method for Evaluating the Bacterial Filtration Efficiency (BFE) of Medical Face Mask Materials, Using a Biological Aerosol of Staphylococcus Aureus—F2101-19 2019. Available online: https://www.astm.org/f2101-19.html (accessed on 14 March 2022).
- European Committee for Standardization European Standard. EN 149:2009+A1; Respiratory Protective Devices—Filtering Half Masks to Protect against Particles—Requirements, Testing, Marking. ASTM International: West Conshohocken, PA, USA, 2009.
- Darby, S.; Chulliyallipalil, K.; Przyjalgowski, M.; McGowan, P.; Jeffers, S.; Giltinan, A.; Lewis, L.; Smith, N.; Sleator, R.D. COVID-19: Mask efficacy is dependent on both fabric and fit. Future Microbiol. 2021, 16, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Fischer, E.P.; Fischer, M.C.; Grass, D.; Henrion, I.; Warren, W.S.; Westman, E. Low-cost measurement of face mask efficacy for filtering expelled droplets during speech. Sci. Adv. 2020, 6, eabd3083. [Google Scholar] [CrossRef] [PubMed]
- Grinshpun, S.A.; Haruta, H.; Eninger, R.M.; Reponen, T.; McKay, R.T.; Lee, S.-A. Performance of an N95 Filtering Facepiece Particulate Respirator and a Surgical Mask during Human Breathing: Two Pathways for Particle Penetration. J. Occup. Environ. Hyg. 2009, 6, 593–603. [Google Scholar] [CrossRef]
- Arumuru, V.; Pasa, J.; Samantaray, S.S. Experimental visualization of sneezing and efficacy of face masks and shields. Phys. Fluids 2020, 32, 115129. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, M.A.; Ghasemieshkaftaki, M.; Bluyssen, P.M. Testing of outward leakage of different types of masks with a breathing manikin head, ultraviolet light and coloured water mist. Intell. Build. Int. 2021, 1–19. [Google Scholar] [CrossRef]
- Mueller, J.T.; Karimi, S.; Poterack, K.A.; Seville, M.T.A.; Tipton, S.M. Surgical mask covering of N95 filtering facepiece respirators: The risk of increased leakage. Infect. Control Hosp. Epidemiol. 2021, 42, 627–628. [Google Scholar] [CrossRef] [PubMed]
- Tcharkhtchi, A.; Abbasnezhad, N.; Seydani, M.Z.; Zirak, N.; Farzaneh, S.; Shirinbayan, M. An overview of filtration efficiency through the masks: Mechanisms of the aerosols penetration. Bioact. Mater. 2021, 6, 106–122. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, J.; Wang, J. Quantitative modeling of the impact of facemasks and associated leakage on the airborne transmission of SARS-CoV-2. Sci. Rep. 2021, 11, 19403. [Google Scholar] [CrossRef] [PubMed]
- Gupta, J.K.; Lin, C.-H.; Chen, Q. Characterizing exhaled airflow from breathing and talking. Indoor Air 2010, 20, 31–39. [Google Scholar] [CrossRef]
- Homaeigohar, S.; Elbahri, M. Nanocomposite Electrospun Nanofiber Membranes for Environmental Remediation. Materials 2014, 7, 1017–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindsley, W.G.; Blachere, F.M.; Beezhold, D.H.; Law, B.F.; Derk, R.C.; Hettick, J.M.; Woodfork, K.; Goldsmith, W.T.; Harris, J.R.; Duling, M.G.; et al. A comparison of performance metrics for cloth masks as source control devices for simulated cough and exhalation aerosols. Aerosol Sci. Technol. 2021, 55, 1125–1142. [Google Scholar] [CrossRef]
- Pettit, N.; Zaidi, A.; O’Neill, B.; Doehring, M. Use of Adhesive Tape to Facilitate Optimal Mask Positioning and Use in the Emergency Department: A Randomized Controlled Trial. Ann. Emerg. Med. 2021, 79, 58–63.e1. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, S. Flow in porous media I: A theoretical derivation of Darcy’s law. Transp. Porous Media 1986, 1, 3–25. [Google Scholar] [CrossRef]
- Duncan, S.; Bodurtha, P.; Naqvi, S. The protective performance of reusable cloth face masks, disposable procedure masks, KN95 masks and N95 respirators: Filtration and total inward leakage. PLoS ONE 2021, 16, e0258191. [Google Scholar] [CrossRef]
- Cappa, C.D.; Asadi, S.; Barreda, S.; Wexler, A.S.; Bouvier, N.M.; Ristenpart, W.D. Expiratory aerosol particle escape from surgical masks due to imperfect sealing. Sci. Rep. 2021, 11, 12110. [Google Scholar] [CrossRef]
- Hariharan, P.; Sharma, N.; Guha, S.; Banerjee, R.K.; D’Souza, G.; Myers, M.R. A computational model for predicting changes in infection dynamics due to leakage through N95 respirators. Sci. Rep. 2021, 11, 10690. [Google Scholar] [CrossRef]
- Tang, J.W.; Liebner, T.J.; Craven, B.A.; Settles, G.S. A schlieren optical study of the human cough with and without wearing masks for aerosol infection control. J. R. Soc. Interface 2009, 6, S727–S736. [Google Scholar] [CrossRef] [Green Version]
- Arumuru, V.; Samantaray, S.S.; Pasa, J. Double masking protection vs. comfort—A quantitative assessment. Phys. Fluids 2021, 33, 077120. [Google Scholar] [CrossRef]
- Kwong, L.H.; Wilson, R.; Kumar, S.; Crider, Y.S.; Sanchez, Y.R.; Rempel, D.; Pillarisetti, A. Review of the Breathability and Filtration Efficiency of Common Household Materials for Face Masks. ACS Nano 2021, 15, 5904–5924. [Google Scholar] [CrossRef] [PubMed]
- Hill, W.C.; Hull, M.S.; MacCuspie, R.I. Testing of Commercial Masks and Respirators and Cotton Mask Insert Materials using SARS-CoV-2 Virion-Sized Particulates: Comparison of Ideal Aerosol Filtration Efficiency versus Fitted Filtration Efficiency. Nano Lett. 2020, 20, 7642–7647. [Google Scholar] [CrossRef]
- Leith, D.; L’Orange, C.; Volckens, J. Quantitative Protection Factors for Common Masks and Face Coverings. Environ. Sci. Technol. 2021, 55, 3136–3143. [Google Scholar] [CrossRef]
- Tessarolo, F.; Nollo, G.; Benedetti, L.; Helfer, F.; Rovati, L.; Ferrari, A.; Marchetti, G.; Reverberi, F.; Baglio, S.; Tuccitto, N.; et al. Measuring breathability and bacterial filtration efficiency of face masks in the pandemic context: A round robin study with proficiency testing among non-accredited laboratories. Measurement 2021, 189, 110481. [Google Scholar] [CrossRef]
- Taborri, J.; Stocchi, B.; Calabro, G.; Rossi, S. Repeatability and Reproducibility in the Breathability Measurement of Surgical Masks; IEEE: Lausanne, Switzerland, 2021. [Google Scholar]
- Bergman, M.S.; Zhuang, Z.; Hanson, D.; Heimbuch, B.K.; McDonald, M.J.; Palmiero, A.J.; Shaffer, R.E.; Harnish, D.; Husband, M.; Wander, J.D. Development of an Advanced Respirator Fit-Test Headform. J. Occup. Environ. Hyg. 2014, 11, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Johnson, G.R.; Morawska, L.; Ristovski, Z.D.; Hargreaves, M.; Mengersen, K.; Chao, C.Y.H.; Wan, M.P.; Li, Y.; Xie, X.; Katoshevski, D.; et al. Modality of human expired aerosol size distributions. J. Aerosol Sci. 2011, 42, 839–851. [Google Scholar] [CrossRef]
- Pan, J.; Harb, C.; Leng, W.; Marr, L.C. Inward and outward effectiveness of cloth masks, a surgical mask, and a face shield. Aerosol Sci. Technol. 2021, 55, 718–733. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mask ID | DP (Pa/cm2) | BFE (%) | Mask Type (Manufacturer Claim) | Filter Material | No. Layers (Details) | Fiber Structure | Total Mask Size (cm2) | Filtering Area (cm2) | Fitting System | Nose Piece |
|---|---|---|---|---|---|---|---|---|---|---|
| CM-a | 315 | 96 | Community, reusable | 100% cotton | 2 | Woven fabric | 393 | 329 | Ear loops | Metal wire |
| CM-b | 56 | 91 | Community, reusable | 92% cotton 8% PU | 2 | Knitted fabric | 259 | 225 | Ear loops | None |
| CM-c | 10 | 94 | Community, reusable | PP | 3 (SSS) | Non-woven | 347 | 308 | Ear loops | None |
| CM-d | 7 | 91 | Community, single use | PP | 1 (S) | Non-woven | 396 | 356 | Ear loops | None |
| SM-a | 28 | >99 | Surgical Type I, single use | PP | 3 (SMS) | Non-woven | 271 | 188 | Ear loops | Metal wire |
| SM-b | 77 | 98 | Surgical Type I, single use | PP | 3 (SSS) | Non-woven | 286 | 207 | Ear loops | Metal wire |
| SM-c | 35 | >99 | Surgical type I, single use | PP | 3 (SMS) | Non-woven | 277 | 200 | Ear loops | Metal wire |
| SM-d | 30 | >99 | Surgical Type IIR, single use | PP | 3 (SMS) | Non-woven | 272 | 200 | Ear loops | Metal wire |
| FP-a | 58 | 91 | FFP2 respirator | PP | 3 (SMS) | Non-woven | 252 | 192 | Ear loops | Metal wire |
| FP-b | 53 | >99 | FFP2 respirator | PP | 3 (SMS) | Non-woven | 255 | 173 | Head loops | Metal wire + foam |
| Mask ID | Wearing Style | Fleak (%) (Mean ± Uncertainty) | TFE (%) (Mean ± Uncertainty) | ||||
|---|---|---|---|---|---|---|---|
| @30 L/min | @90 L/min | @160 L/min | @30 L/min | @90 L/min | @160 L/min | ||
| SM-a | IFU | 86 ± 10 | 75 ± 4 | 65 ± 3 | 14 ± 10 | 25 ± 4 | 35 ± 3 |
| Nose | 93 ± 10 | 86 ± 4 | 78 ± 2 | 7 ± 10 | 14 ± 4 | 22 ± 2 | |
| Ear | 87 ± 10 | 78 ± 4 | 70 ± 3 | 13 ± 10 | 21 ± 4 | 30 ± 3 | |
| Nape | 79 ± 11 | 63 ± 4 | 53 ± 3 | 21 ± 11 | 36 ± 4 | 47 ± 3 | |
| SM-b | IFU | 91 ± 4 | 81 ± 2 | 72 ± 2 | 9 ± 4 | 19 ± 2 | 27 ± 2 |
| Nose | 97 ± 4 | 93 ± 2 | 89 ± 1 | 3 ± 4 | 7 ± 2 | 11 ± 1 | |
| Ear | 88 ± 4 | 77 ± 2 | 69 ± 2 | 12 ± 4 | 23 ± 2 | 31 ± 2 | |
| Nape | 88 ± 4 | 72 ± 2 | 64 ± 2 | 12 ± 4 | 27 ± 2 | 36 ± 2 | |
| SM-c | IFU | 85 ± 7 | 67 ± 3 | 56 ± 3 | 14 ± 7 | 33 ± 3 | 44 ± 3 |
| Nose | 95 ± 7 | 87 ± 3 | 80 ± 2 | 5 ± 7 | 13 ± 3 | 19 ± 2 | |
| Ear | 81 ± 7 | 66 ± 3 | 58 ± 3 | 19 ± 7 | 34 ± 3 | 42 ± 3 | |
| Nape | 71 ± 8 | 52 ± 4 | 43 ± 4 | 29 ± 8 | 47 ± 4 | 56 ± 4 | |
| SM-d | IFU | 86 ± 7 | 71 ± 3 | 60 ± 3 | 14 ± 7 | 29 ± 3 | 39 ± 3 |
| Nose | 95 ± 7 | 90 ± 2 | 83 ± 2 | 5 ± 7 | 10 ± 2 | 17 ± 2 | |
| Ear | 85 ± 7 | 7 ± 3 | 65 ± 2 | 15 ± 7 | 25 ± 3 | 35 ± 2 | |
| Nape | 82 ± 7 | 65 ± 3 | 53 ± 3 | 18 ± 7 | 34 ± 3 | 46 ± 3 | |
| CM-a | IFU | 95 ± 2 | 90 ± 1 | 85 ± 1 | 5 ± 2 | 10 ± 1 | 15 ± 1 |
| Nose | 98 ± 2 | 96 ± 1 | 93 ± 1 | 2 ± 1 | 4 ± 1 | 7 ± 0 | |
| Ear | 97 ± 2 | 92 ± 1 | 88 ± 1 | 3 ± 2 | 7 ± 1 | 12 ± 1 | |
| Nape | 96 ± 2 | 92 ± 1 | 88 ± 1 | 4 ± 2 | 8 ± 1 | 12 ± 1 | |
| CM-b | IFU | 86 ± 5 | 73 ± 3 | 66 ± 2 | 13 ± 5 | 24 ± 2 | 31 ± 2 |
| Nose | 89 ± 5 | 82 ± 2 | 74 ± 2 | 10 ± 5 | 17 ± 2 | 24 ± 2 | |
| Ear | 96 ± 5 | 88 ± 2 | 82 ± 2 | 4 ± 5 | 11 ± 2 | 16 ± 1 | |
| Nape | 88 ± 5 | 74 ± 3 | 63 ± 2 | 11 ± 5 | 24 ± 2 | 34 ± 2 | |
| CM-c | IFU | 43 ± 28 | 18 ± 10 | 10 ± 7 | 53 ± 26 | 77 ± 10 | 84 ± 7 |
| Nose | 62 ± 28 | 31 ± 10 | 18 ± 7 | 36 ± 26 | 65 ± 9 | 77 ± 6 | |
| Ear | 36 ± 28 | 15 ± 11 | 8 ± 7 | 60 ± 27 | 80 ± 10 | 86 ± 7 | |
| Nape | 29 ± 28 | 11 ± 11 | 5 ± 7 | 67 ± 27 | 83 ± 10 | 89 ± 7 | |
| CM-d | IFU | 74 ± 38 | 44 ± 13 | 29 ± 8 | 24 ± 34 | 51 ± 11 | 64 ± 7 |
| Nose | 74 ± 38 | 59 ± 13 | 48 ± 7 | 24 ± 34 | 38 ± 11 | 47 ± 7 | |
| Ear | 74 ± 38 | 36 ± 13 | 24 ± 8 | 24 ± 34 | 58 ± 12 | 69 ± 7 | |
| Nape | 48 ± 38 | 31 ± 13 | 24 ± 8 | 47 ± 34 | 63 ± 12 | 69 ± 7 | |
| FP-a | IFU | 33 ± 10 | 22 ± 6 | 18 ± 5 | 61 ± 9 | 71 ± 5 | 74 ± 4 |
| FP-b | IFU | 11 ± 10 | 9 ± 6 | 8 ± 5 | 88 ± 10 | 90 ± 6 | 91 ± 5 |
| Mask ID | Changes in Fleak for Wearing Styles Alternative to Instructions for Use | ||
|---|---|---|---|
| IFU vs. NOSE | IFU vs. EAR | IFU vs. NAPE | |
| CM-a | ↑ * | ↑ * | ↓ * |
| CM-b | ↑ * | ↑ * | ↔ |
| CM-c | ↑ | ↓ | ↓ * |
| CM-d | ↑ | ↓ | ↓ * |
| SM-a | ↑ * | ↑ | ↓ |
| SM-b | ↑ | ↓ | ↓ * |
| SM-c | ↑ * | ↔ | ↓ * |
| SM-d | ↑ * | ↑ | ↓ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiera, S.; Cristoforetti, A.; Benedetti, L.; Nollo, G.; Borro, L.; Mazzei, L.; Tessarolo, F. A Simple Method to Quantify Outward Leakage of Medical Face Masks and Barrier Face Coverings: Implication for the Overall Filtration Efficiency. Int. J. Environ. Res. Public Health 2022, 19, 3548. https://doi.org/10.3390/ijerph19063548
Chiera S, Cristoforetti A, Benedetti L, Nollo G, Borro L, Mazzei L, Tessarolo F. A Simple Method to Quantify Outward Leakage of Medical Face Masks and Barrier Face Coverings: Implication for the Overall Filtration Efficiency. International Journal of Environmental Research and Public Health. 2022; 19(6):3548. https://doi.org/10.3390/ijerph19063548
Chicago/Turabian StyleChiera, Silvia, Alessandro Cristoforetti, Luca Benedetti, Giandomenico Nollo, Luca Borro, Lorenzo Mazzei, and Francesco Tessarolo. 2022. "A Simple Method to Quantify Outward Leakage of Medical Face Masks and Barrier Face Coverings: Implication for the Overall Filtration Efficiency" International Journal of Environmental Research and Public Health 19, no. 6: 3548. https://doi.org/10.3390/ijerph19063548