
Spatial Analysis of COVID-19 Vaccine Centers Distribution: A Case Study of the City of Jeddah, Saudi Arabia

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
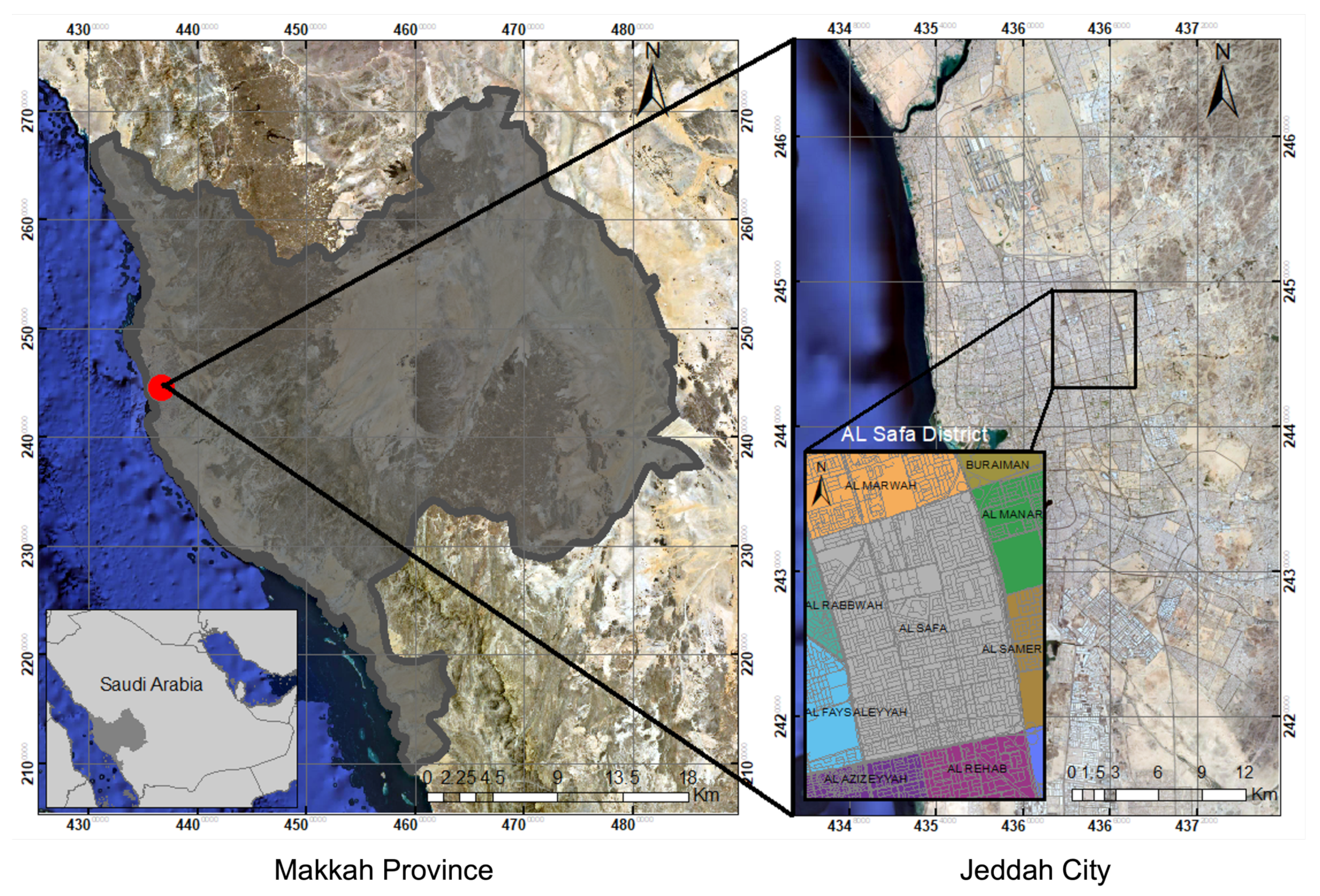
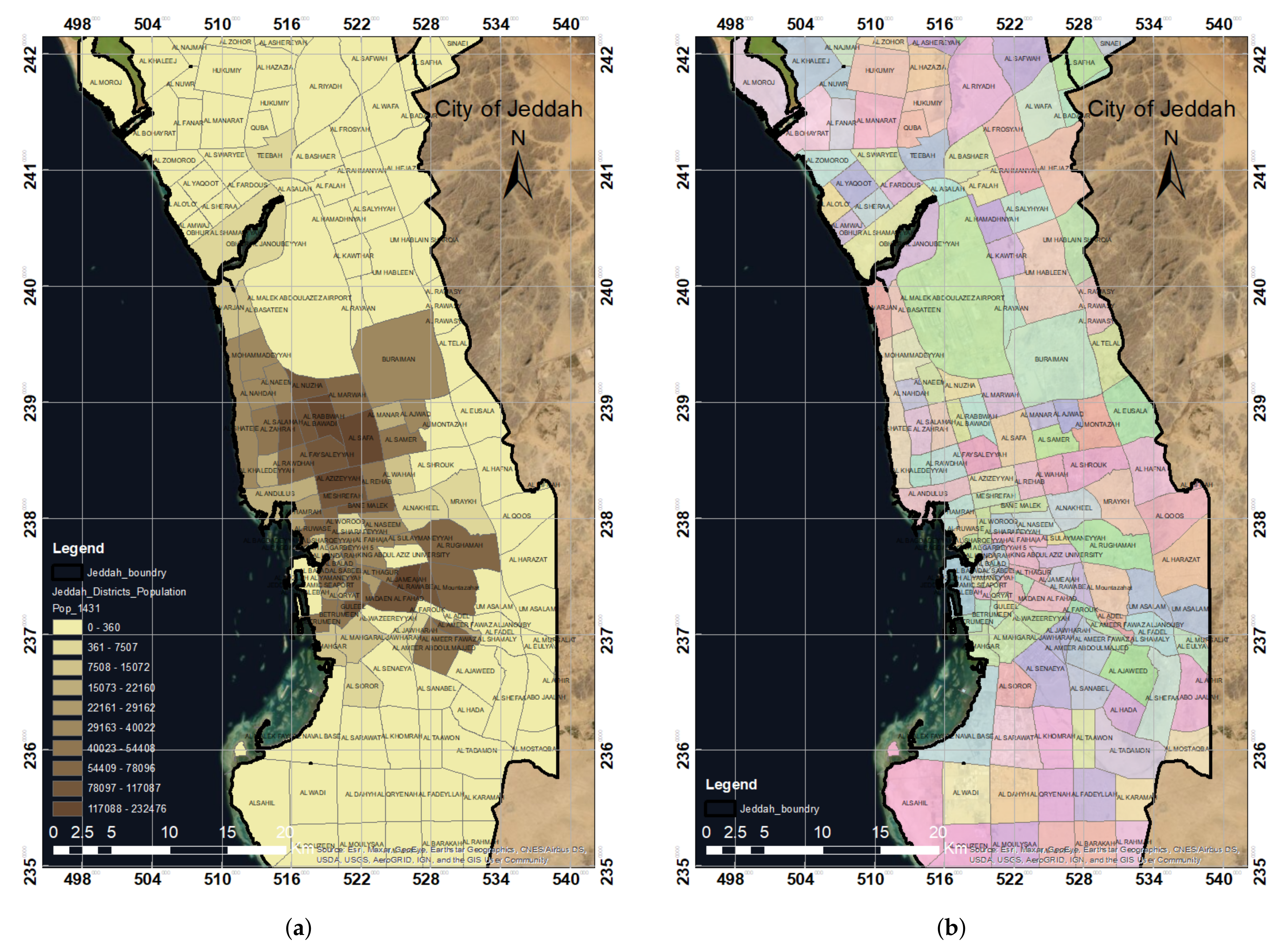
2.1. Study Area
2.2. Data
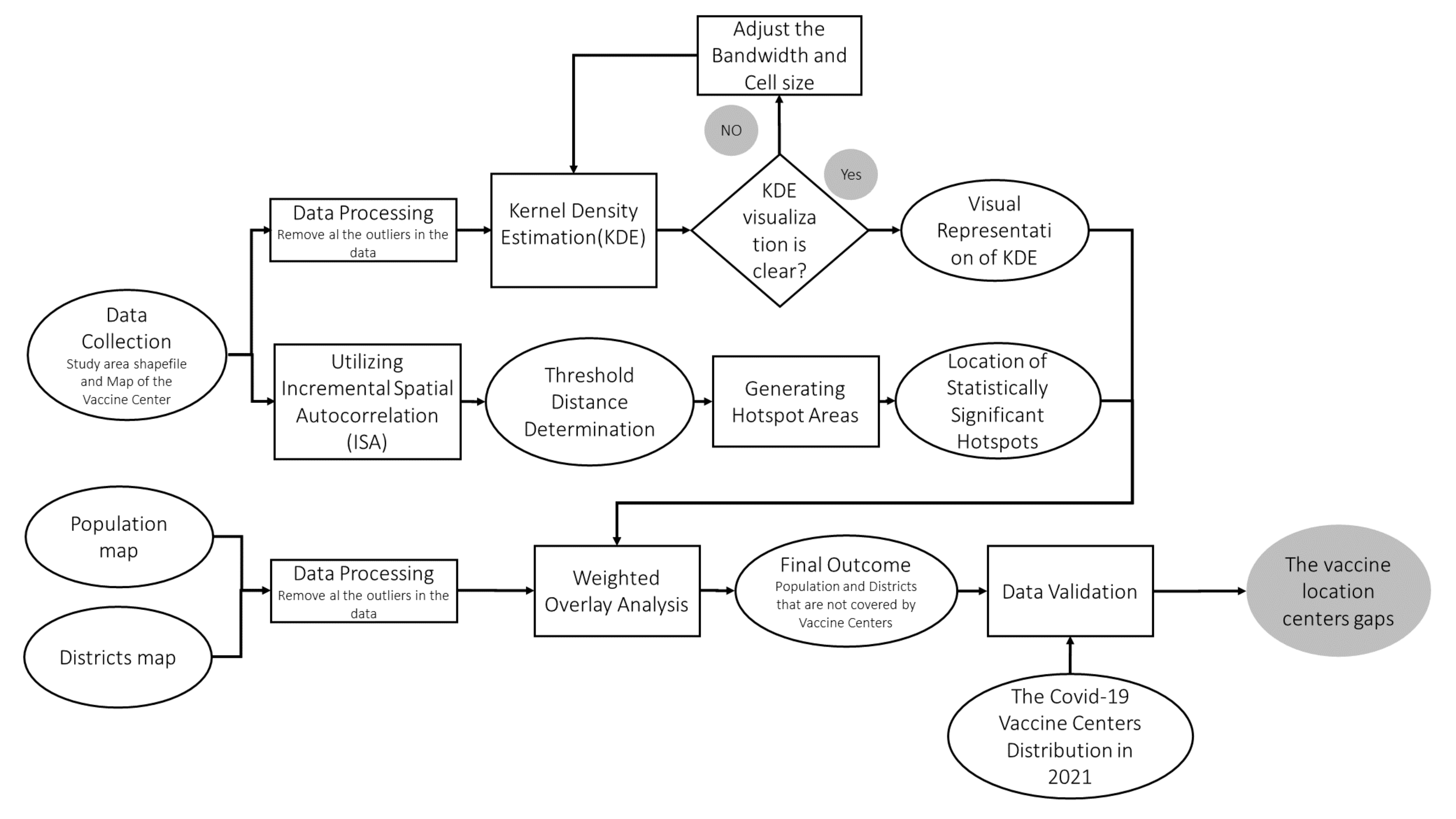
2.3. Analytical Approach
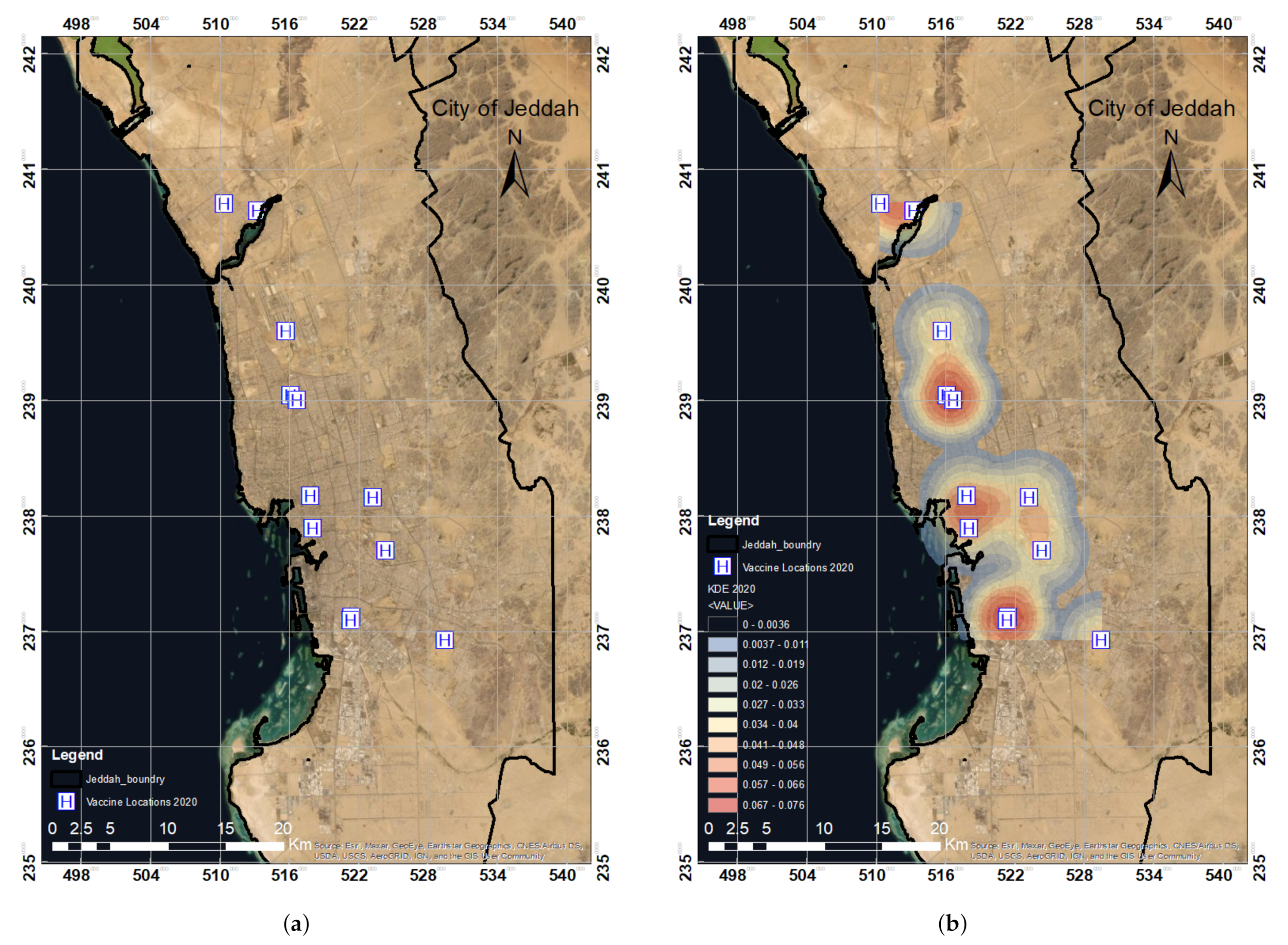
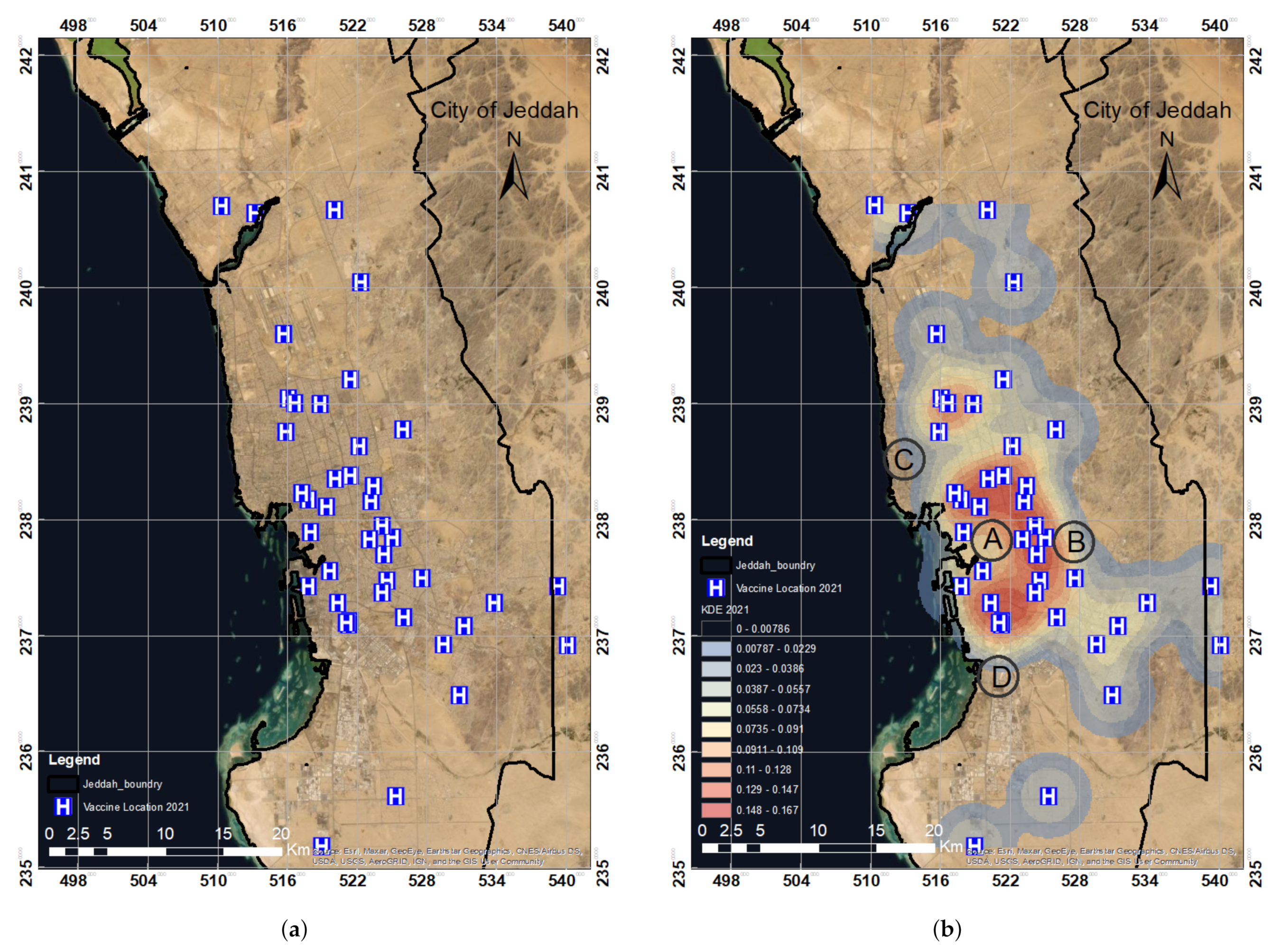
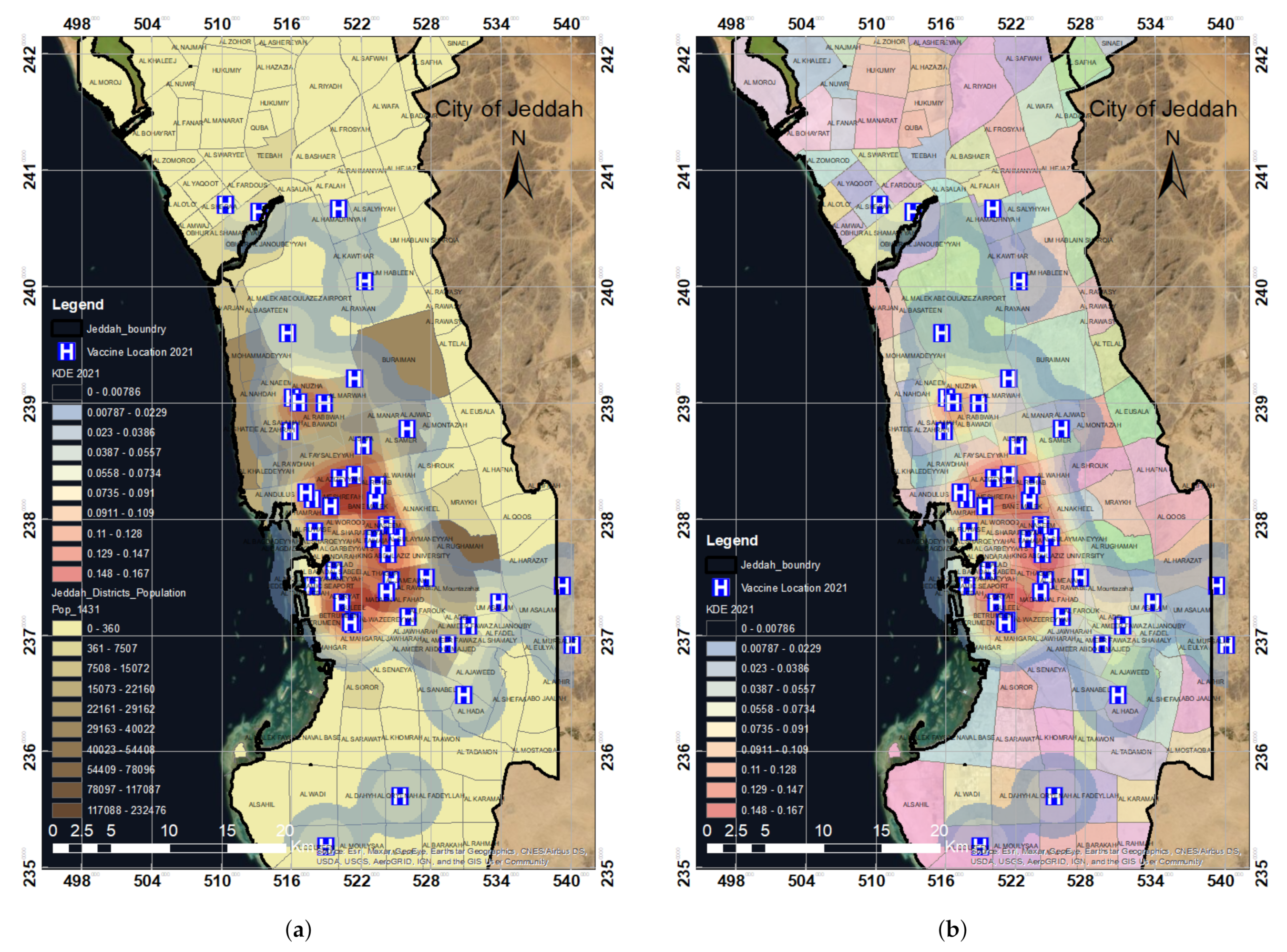
2.3.1. Kernel Density Estimation (KDE)
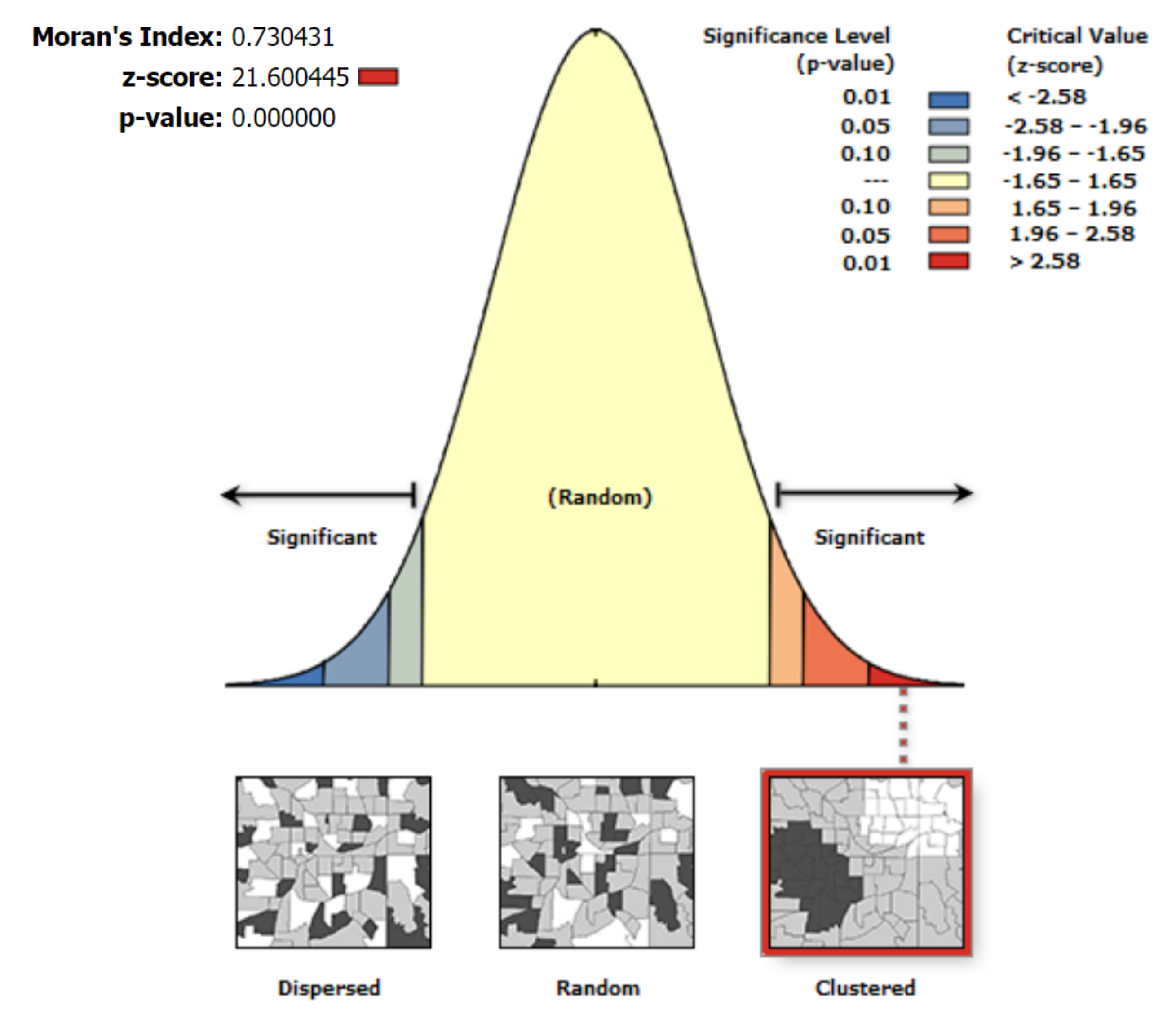
2.3.2. Incremental Spatial Autocorrelation (ISA)
- To estimate the spatial autocorrelation, first, a default minimum distance is chosen. The ISA technique then evaluates the distance between features to ensure that each segment has a neighbor. In this research, 2 km (kilometers) was set as the default distance for the ISA technique. The spatial autocorrelation values are then computed by increasing the distance incrementally.
- The ideal threshold distance is the one with the highest Z-score. The threshold distance in this investigation was determined to be 2 km. This determined distance was utilized in the spatial mechanisms to generate clustering in the data.
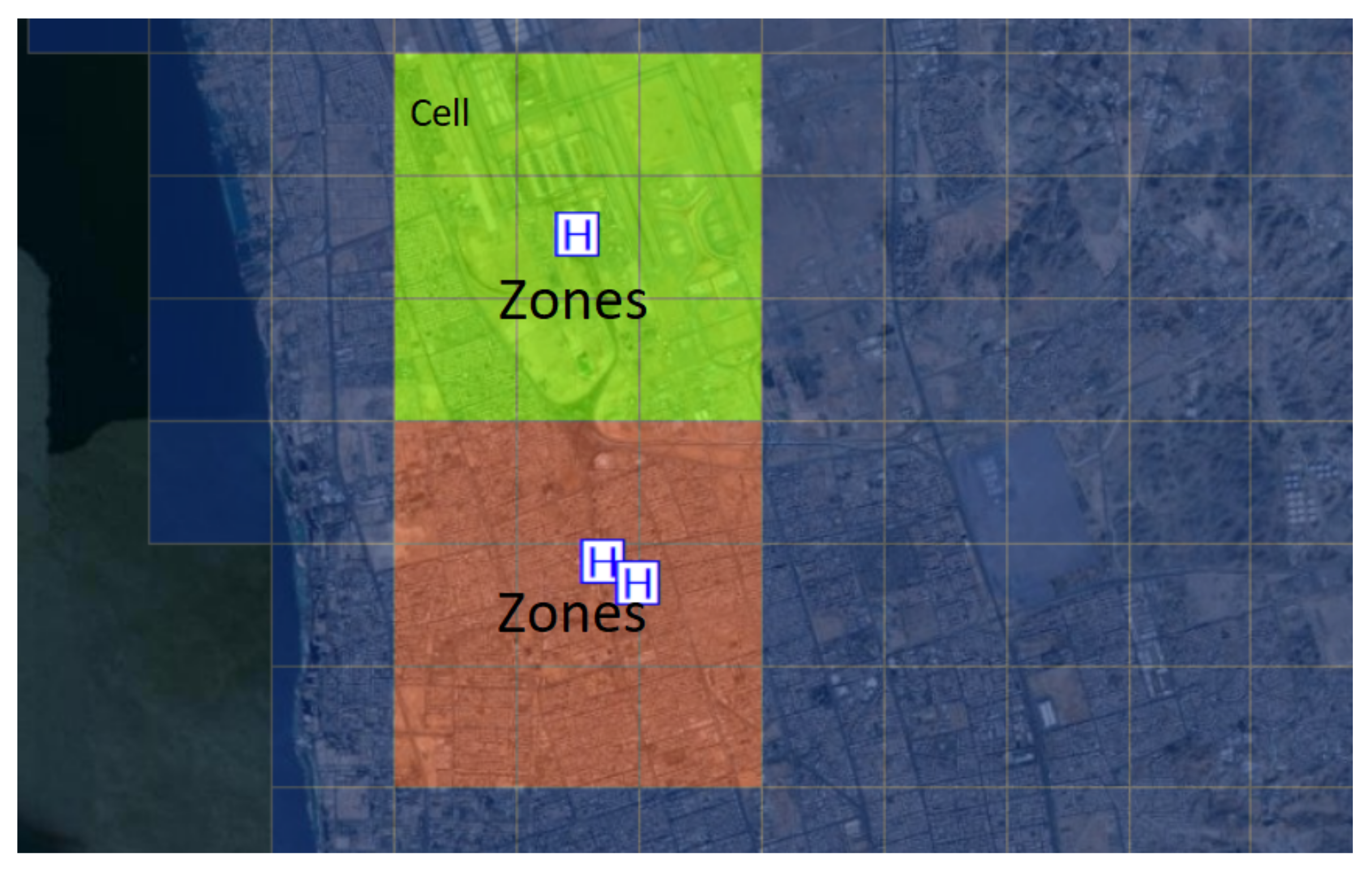
2.3.3. Hotspot Analysis
2.3.4. Hotspot Selection Criteria
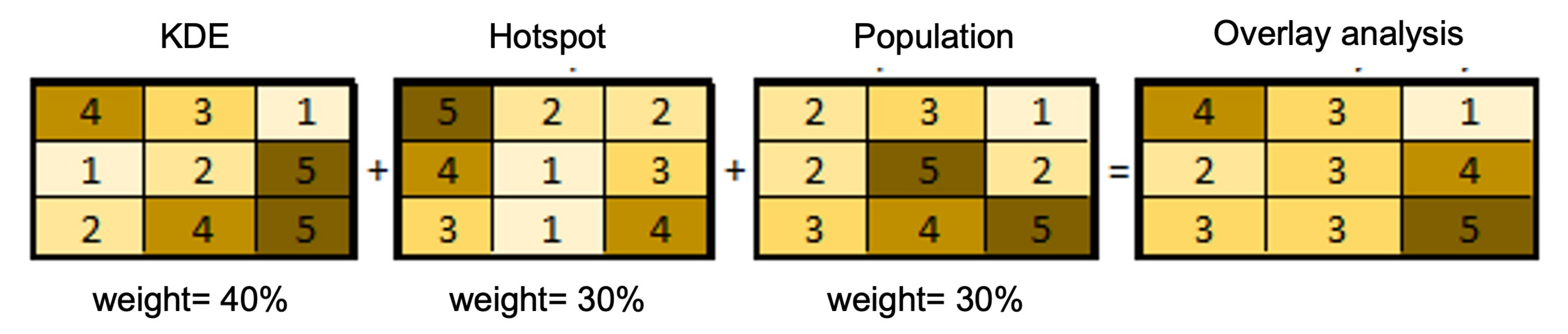
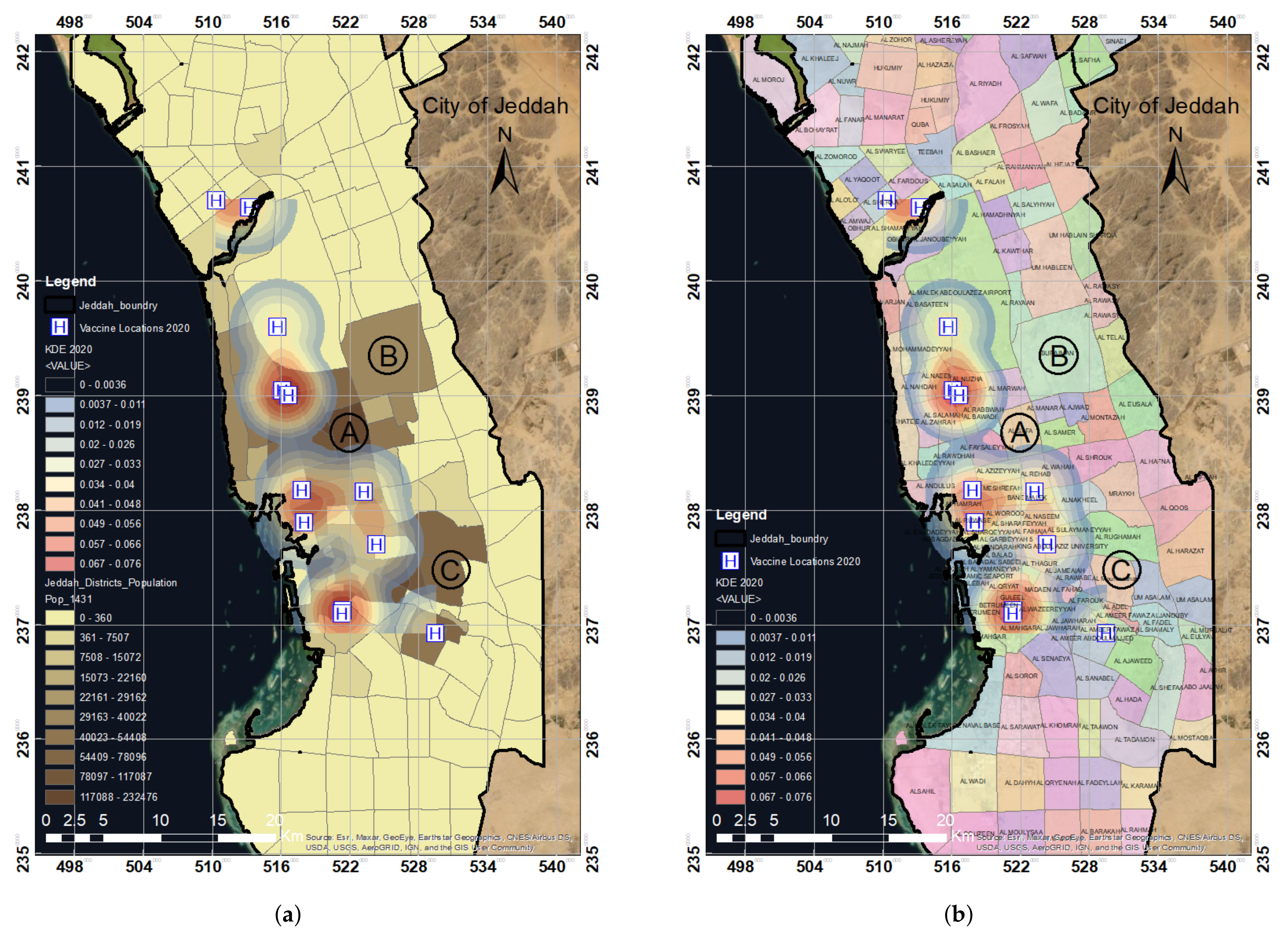
2.3.5. Weighted Overlay
3. Results and Discussion
3.1. Spatial Analysis of COVID-19 Vaccination Sites in the Year 2020 in Jeddah
3.2. Statistical Significance Analysis for Spatial-Pattern Discovery
3.3. Results Validation
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease 2019 (COVID-19): Situation Report, 51. 2020. Available online: https://apps.who.int/iris/handle/10665/331475 (accessed on 12 September 2021).
- World Health Organization. Weekly Epidemiological Update—29 December 2020. 2020. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update—29-december-2020 (accessed on 12 September 2021).
- Venter, M.; Richter, K. Towards effective diagnostic assays for COVID-19: A review. J. Clin. Pathol. 2020, 73, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Jon, C.; Kai, K. Countries test tactics in ‘war’ against COVID-19. Science 2020, 367, 1287–1288. [Google Scholar] [CrossRef] [Green Version]
- Beeching, N.J.; Fletcher, T.E.; Beadsworth, M.B. COVID-19: Testing times. BMJ 2020, 369, m1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliver, S.E.; Gargano, J.W.; Marin, M.; Wallace, M.; Curran, K.G.; Chamberland, M.; McClung, N.; Campos-Outcalt, D.; Morgan, R.L.; Mbaeyi, S.; et al. The advisory committee on immunization practices’ interim recommendation for use of Pfizer-BioNTech COVID-19 vaccine—United States, December 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1922. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19: Where are we on vaccines and variants? BMJ 2021, 372, n597. [Google Scholar] [CrossRef]
- World Health Organization. WHO Concept for Fair Access and Equitable Allocation of COVID-19 Health Products. Available online: https://www.who.int/docs/default-source/coronaviruse/who-covid19-vaccine-allocation-final-working-version-9sept.pdf (accessed on 12 September 2021).
- Our World in Data. COVID-19 Vaccination Policy. Available online: https://ourworldindata.org/grapher/covid-vaccination-policy (accessed on 12 September 2021).
- Franch-Pardo, I.; Napoletano, B.M.; Rosete-Verges, F.; Billa, L. Spatial analysis and GIS in the study of COVID-19. A review. Sci. Total Environ. 2020, 739, 140033. [Google Scholar] [CrossRef]
- Ahasan, R.; Alam, M.S.; Chakraborty, T.; Hossain, M.M. Applications of GIS and geospatial analyses in COVID-19 research: A systematic review. F1000Research 2020, 9, 1379. [Google Scholar] [CrossRef]
- Bag, R.; Ghosh, M.; Biswas, B.; Chatterjee, M. Understanding the spatio-temporal pattern of COVID-19 outbreak in India using GIS and India’s response in managing the pandemic. Reg. Sci. Policy Pract. 2020, 12, 1063–1103. [Google Scholar] [CrossRef]
- Shariati, M.; Mesgari, T.; Kasraee, M.; Jahangiri-Rad, M. Spatiotemporal analysis and hotspots detection of COVID-19 using geographic information system (March and April, 2020). J. Environ. Health Sci. Eng. 2020, 18, 1499–1507. [Google Scholar] [CrossRef]
- Niu, B.; Liang, R.; Zhang, S.; Zhang, H.; Qu, X.; Su, Q.; Zheng, L.; Chen, Q. Epidemic analysis of COVID-19 in Italy based on spatiotemporal geographic information and Google Trends. Transbound. Emerg. Dis. 2021, 68, 2384–2400. [Google Scholar] [CrossRef]
- Cuadros, D.F.; Branscum, A.J.; Mukandavire, Z.; Miller, F.D.; MacKinnon, N. Dynamics of the COVID-19 epidemic in urban and rural areas in the United States. Ann. Epidemiol. 2021, 59, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Raymundo, C.E.; Oliveira, M.C.; Eleuterio, T.D.A.; André, S.R.; da Silva, M.G.; Queiroz, E.R.D.S.; Medronho, R.D.A. Spatial analysis of COVID-19 incidence and the sociodemographic context in Brazil. PLoS ONE 2021, 16, e0247794. [Google Scholar] [CrossRef] [PubMed]
- Al-Kindi, K.M.; Alkharusi, A.; Alshukaili, D.; Al Nasiri, N.; Al-Awadhi, T.; Charabi, Y.; El Kenawy, A.M. Spatiotemporal assessment of COVID-19 spread over Oman using GIS techniques. Earth Syst. Environ. 2020, 4, 797–811. [Google Scholar] [CrossRef] [PubMed]
- MohammadEbrahimi, S.; Mohammadi, A.; Bergquist, R.; Dolatkhah, F.; Olia, M.; Tavakolian, A.; Pishgar, E.; Kiani, B. Epidemiological characteristics and initial spatiotemporal visualisation of COVID-19 in a major city in the Middle East. BMC Public Health 2021, 21, 1373. [Google Scholar] [CrossRef]
- Lieberman-Cribbin, W.; Tuminello, S.; Flores, R.M.; Taioli, E. Disparities in COVID-19 testing and positivity in New York City. Am. J. Prev. Med. 2020, 59, 326–332. [Google Scholar] [CrossRef]
- Sarwar, S.; Waheed, R.; Sarwar, S.; Khan, A. COVID-19 challenges to Pakistan: Is GIS analysis useful to draw solutions? Sci. Total Environ. 2020, 730, 139089. [Google Scholar] [CrossRef]
- Whitehead, J.; Scott, N.; Carr, P.A.; Lawrenson, R. Will access to COVID-19 vaccine in Aotearoa be equitable for priority populations? N. Z. Med. J. 2021, 134, 25–34. [Google Scholar] [CrossRef]
- Krzysztofowicz, S.; Osińska-Skotak, K. The Use of GIS Technology to Optimize COVID-19 Vaccine Distribution: A Case Study of the City of Warsaw, Poland. Int. J. Environ. Res. Public Health 2021, 18, 5636. [Google Scholar] [CrossRef]
- Wong, C.A.; Dowler, S.; Moore, A.F.; Sosne, E.F.; Young, H.; Tenenbaum, J.D.; Burns, C.E.; Jones, S.; Smelyanskaya, M.; Kinsley, K.H. COVID-19 vaccine administration, by race and ethnicity—North Carolina, December 14, 2020–April 6, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 991. [Google Scholar] [CrossRef]
- Alemdar, K.D.; Kaya, Ö.; Çodur, M.Y.; Campisi, T.; Tesoriere, G. Accessibility of Vaccination Centers in COVID-19 Outbreak Control: A GIS-Based Multi-Criteria Decision Making Approach. ISPRS Int. J. Geo-Inf. 2021, 10, 708. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Memish, Z.A. COVID-19 in the Eastern Mediterranean Region and Saudi Arabia: Prevention and therapeutic strategies. Int. J. Antimicrob. Agents 2020, 55, 105968. [Google Scholar] [CrossRef] [PubMed]
- Assiri, A.; Al-Tawfiq, J.A.; Alkhalifa, M.; Al Duhailan, H.; Al Qahtani, S.; Dawas, R.A.; El Seoudi, A.A.; Alomran, N.; Omar, O.A.; Alotaibi, N.; et al. Launching COVID-19 vaccination in Saudi Arabia: Lessons learned, and the way forward. Travel Med. Infect. Dis. 2021, 43, 102119. [Google Scholar] [CrossRef] [PubMed]
- Dano, U.L. Flash flood impact assessment in Jeddah City: An analytic hierarchy process approach. Hydrology 2020, 7, 10. [Google Scholar] [CrossRef] [Green Version]
- Abubakar, I.R.; Aina, Y.A. Achieving sustainable cities in Saudi Arabia: Juggling the competing urbanization challenges. In E-Planning and Collaboration: Concepts, Methodologies, Tools, and Applications; IGI Global: Hershey, PA, USA, 2018; pp. 234–255. [Google Scholar] [CrossRef]
- Murad, A.; Khashoggi, B.F. Using GIS for disease mapping and clustering in Jeddah, Saudi Arabia. ISPRS Int. J. Geo-Inf. 2020, 9, 328. [Google Scholar] [CrossRef]
- De Smith, M.; Goodchild, M.; Longley, P. Geospatial Analysis: A Comprehensive Guide to Principles, Techniques and Software Tools; Matador: Leicester, UK, 2009. [Google Scholar]
- Srikanth, L.; Srikanth, I. A Case Study on Kernel Density Estimation and Hotspot Analysis Methods in Traffic Safety Management. In Proceedings of the 2020 International Conference on COMmunication Systems & NETworkS (COMSNETS), Bengaluru, India, 7–11 January 2020; pp. 99–104. [Google Scholar] [CrossRef]
- Kalinic, M.; Krisp, J.M. Kernel density estimation (KDE) vs. hot-spot analysis–detecting criminal hot spots in the City of San Francisco. In Proceedings of the 21st Conference on Geo-Information Science, Lund, Sweden, 12–15 June 2018. [Google Scholar]
- Silverman, B.W. Density Estimation for Statistics and Data Analysis; Routledge: Oxfordshire, UK, 2018. [Google Scholar]
- Gibin, M.; Longley, P.; Atkinson, P. Kernel density estimation and percent volume contours in general practice catchment area analysis in urban areas. In Proceedings of the GISRUK, Maynooth, Ireland, 11–13 April 2007; pp. 11–13. [Google Scholar]
- Xie, Z.; Yan, J. Kernel density estimation of traffic accidents in a network space. Comput. Environ. Urban Syst. 2008, 32, 396–406. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Liu, P.; Chen, J.; Wang, H. Comparative analysis of the spatial analysis methods for hotspot identification. Accid. Anal. Prev. 2014, 66, 80–88. [Google Scholar] [CrossRef]
- O’Sullivan, D.; Wong, D.W. A surface-based approach to measuring spatial segregation. Geogr. Anal. 2007, 39, 147–168. [Google Scholar] [CrossRef]
- Erdogan, S.; Yilmaz, I.; Baybura, T.; Gullu, M. Geographical information systems aided traffic accident analysis system case study: City of Afyonkarahisar. Accid. Anal. Prev. 2008, 40, 174–181. [Google Scholar] [CrossRef]
- Anderson, T.K. Kernel density estimation and K-means clustering to profile road accident hotspots. Accid. Anal. Prev. 2009, 41, 359–364. [Google Scholar] [CrossRef]
- Blazquez, C.A.; Celis, M.S. A spatial and temporal analysis of child pedestrian crashes in Santiago, Chile. Accid. Anal. Prev. 2013, 50, 304–311. [Google Scholar] [CrossRef]
- Thakali, L.; Kwon, T.J.; Fu, L. Identification of crash hotspots using kernel density estimation and kriging methods: A comparison. J. Mod. Transp. 2015, 23, 93–106. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, S.; Yoshiki, S.; Saeki, R.; Mimura, Y.; Ando, R.; Nanba, S. Development and application of traffic accident density estimation models using kernel density estimation. J. Traffic Transp. Eng. 2016, 3, 262–270. [Google Scholar] [CrossRef] [Green Version]
- Songchitruksa, P.; Zeng, X. Getis–Ord spatial statistics to identify hot spots by using incident management data. Transp. Res. Rec. 2010, 2165, 42–51. [Google Scholar] [CrossRef]
- Pulugurtha, S.S.; Krishnakumar, V.K.; Nambisan, S.S. New methods to identify and rank high pedestrian crash zones: An illustration. Accid. Anal. Prev. 2007, 39, 800–811. [Google Scholar] [CrossRef]
- Chainey, S.; Tompson, L.; Uhlig, S. The utility of hotspot mapping for predicting spatial patterns of crime. Secur. J. 2008, 21, 4–28. [Google Scholar] [CrossRef]
- Gatrell, A.; Bailey, T. Interactive spatial data analysis in medical geography. Soc. Sci. Med. 1996, 42, 843–855. [Google Scholar] [CrossRef]
- Levin, N.; Levine, N. CrimeStat III-A Spatial Statistics Program for the Analysis of Crime Incident Locations; US Department of Justice: Houston, TX, USA, 2004. [Google Scholar]
- Levine, N. CrimeStat: A Spatial Statistical Program for the Analysis of Crime Incidents. In Encyclopedia of GIS; Shekhar, S., Xiong, H., Zhou, X., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 381–388. [Google Scholar] [CrossRef]
- Brimicombe, A.J. On being more robust about ‘hot spots’. In Proceedings of the Seventh Annual Crime Mapping Research Conference, Boston, MA, USA, 31 March–3 April 2004; pp. 234–240. [Google Scholar]
- Keskin, F.; Yenilmez, F.; Çolak, M.; Yavuzer, I.; Düzgün, H.S. Analysis of traffic incidents in METU campus. Procedia-Soc. Behav. Sci. 2011, 19, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Ha, H.H.; Thill, J.C. Analysis of traffic hazard intensity: A spatial epidemiology case study of urban pedestrians. Comput. Environ. Urban Syst. 2011, 35, 230–240. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data | GIS Data Type | Data Format | Source |
|---|---|---|---|
| Jeddah base map | Pixel | Raster | Esri, Maxar, GeoEye, Earthstar Geographics, |
| CNES/Airbus DS, USDA, USGS, AeroGRID, | |||
| IGN, and the GIS User Community | |||
| Vaccination centers | Point | Vector | Saudi Ministry of Health |
| Population distribution | Polygon | Vector | Jeddah Municipality |
| Districts distribution | Polygon | Vector | Jeddah Municipality |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faisal, K.; Alshammari, S.; Alotaibi, R.; Alhothali, A.; Bamasag, O.; Alghanmi, N.; Bin Yamin, M. Spatial Analysis of COVID-19 Vaccine Centers Distribution: A Case Study of the City of Jeddah, Saudi Arabia. Int. J. Environ. Res. Public Health 2022, 19, 3526. https://doi.org/10.3390/ijerph19063526
Faisal K, Alshammari S, Alotaibi R, Alhothali A, Bamasag O, Alghanmi N, Bin Yamin M. Spatial Analysis of COVID-19 Vaccine Centers Distribution: A Case Study of the City of Jeddah, Saudi Arabia. International Journal of Environmental Research and Public Health. 2022; 19(6):3526. https://doi.org/10.3390/ijerph19063526
Chicago/Turabian StyleFaisal, Kamil, Sultanah Alshammari, Reem Alotaibi, Areej Alhothali, Omaimah Bamasag, Nusaybah Alghanmi, and Manal Bin Yamin. 2022. "Spatial Analysis of COVID-19 Vaccine Centers Distribution: A Case Study of the City of Jeddah, Saudi Arabia" International Journal of Environmental Research and Public Health 19, no. 6: 3526. https://doi.org/10.3390/ijerph19063526