
Literature Cases Summarized Based on Their Polysomnographic Findings in Rett Syndrome


Abstract
:1. Introduction
2. Materials and Methods
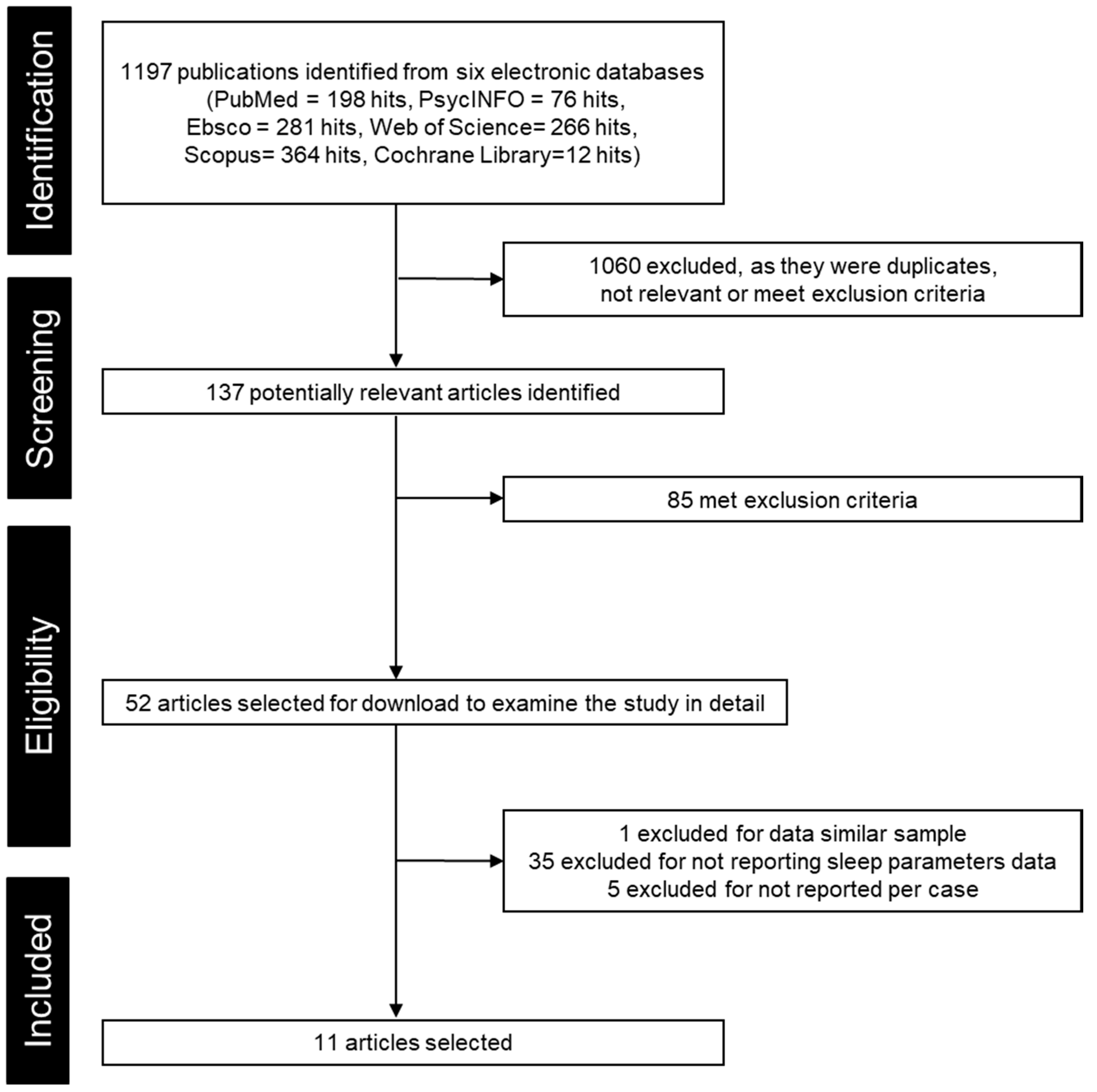
2.1. Case Selection
2.2. Data Collection and Analysis
2.3. Statistical Analysis

{kind=link}
{kind=link}
{kind=link}
| Author(Year) | Country | Gender: n | Age Mean ± SD [Range], y | Gene (n) | Classification, Stage(n) | Diagnosis | Sleep Assessment Tool | Sleep Scoring Guideline | Sleep Issue Investigated | Type of Study |
|---|---|---|---|---|---|---|---|---|---|---|
| Cacciatori et al., 2020 [27] | Italy | M: 1 | 0.8 | MECP2 | C, G | Home sleep test | AASM Scoring Manual Version 2.2 | SDB | Case report | |
| Sarber et al., 2019 [28] | United States | M: 2 F: 11 | 10.3 ± 4.9, [2.6–17.4] | MECP2 (11) | Classic | C, G | PSG | AASM 2007–2017 | SDB, sleep structure | Case-series |
| Amaddeo et al., 2019 [13] | France | F:17 | 9.5 ± 2.8 [6–16] | MECP2 (11) | G | PSG | AASM 2007 | SDB, sleep structure | Case-series | |
| Ohno et al., 2016 [29] | Japan | F: 1 | 6.6 | MECP2 | G | PSG | ? | SDB, sleep structure | Case report | |
| Bassett et al., 2016 [30] | United States | F:14 | 7.8 ± 4.9, [1.9–17.6] | PSG | ? | SDB | Case-series 3 | |||
| Hagebeuk et al., 2012(a) [31] | the Netherlands | F:12 | 9.5 ± 8.8, [3–33] | MECP2 (9) | III (9) and IV(1) | C [6], G | PSG | AASM 2007 | SDB | Case-series |
| Hagebeuk et al., 2012(b) [11] | the Netherlands | F:4 | 6.5 ± 5.8, [2–15] | CDKL5 | G | PSG | AASM 2007 | SDB, sleep structure | Case-series | |
| d’Orsi et al., 2009 [32] | Italy | F: 1 | 2 | MECP2 | G | PSG 1 | AASM | EEG, SDB | Case report | |
| Schluüter et al., 1995 [33] | Germany | F:2 | 13 ± 5.7, [9, 17] | PSG 2 | Schlüter 1993 | SDB, EEG, sleep structure | Case-series | |||
| Aldrich et al., 1990 [34] | United States | F: 4 | 7.0 ± 3.0, [4–11] | III (4) | C [35] | PSG | Rechtschaffen and Kales 1968 | EEG, sleep structure, SDB | Case-series | |
| Nomura et al., 1985 [15] | Japan | F: 5 | 5.8 ± 4.4, [2–12] | PSG | Segawa? | EEG, sleep structure | Case-series |
| Parameters | Age (year) | TST (min) | SEI (%) | WASO (min) | SOL (min) | N1 (%) | N2 (%) | N3 (%) | REM (%) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Typically developing individuals | mean ± SD | 9.39 ± 5.50 | 490.94 ± 26.56 | 89.53 ± 2.59 | 32.06 ± 14.27 | 25.81 ± 5.73 | 7.15 ± 0.52 | 39.69 ± 6.56 | 30.40 ± 4.84 | 21.32 ± 2.10 | |
| n | 209 | 209 | 209 | 209 | 209 | 209 | 209 | 209 | 209 | ||
| Total RTT group | mean ± SD | 8.38 ± 3.88 | 417.30 ± 154.18 | 70.14 ± 21.84 | 189.21 ± 165.06 | 23.56 ± 45.62 | 9.51 ± 10.35 | 34.51 ± 16.83 | 41.05 ± 21.19 | 14.74 ± 9.28 | |
| n | 33 | 27 | 27 | 27 | 8 | 30 | 30 | 31 | 31 | ||
| SMD (p) | 1.29 (0.000) | 2.53 (0. 000) | −2.77 (0.000) | 0.23 (0.53) | −0.65 (0.001) | 0.61 (0.002) | −1.21 (0.000) | 1.72 (0.000) | |||
| Gene | MECP2 | mean ± SD | 8.79 ± 2.28 | 368.20 ± 89.19 | 65.93 ± 20.07 | 223.97 ± 180.98 | 1.70 ± 1.71 | 32.47 ± 16.86 | 51.93 ± 19.90 | 13.03 ± 9.58 | |
| n | 16 | 15 | 15 | 15 | 15 | 15 | 16 | 16 | |||
| SMD (p) | 3.60 (0.000) | 4.19 (0.000) | −4.04 (0.000) | 8.22 (0.000) | 0.95 (0.000) | −3.09 (0.000) | 2.58 (0.000) | ||||
| CDKL5 | mean ± SD | 6.50 ± 5.80 | 666.23 ± 110.38 | 70.58 ± 11.69 | 238.97 ± 98.98 | 38.80 ± 63.25 | 25.01 ± 4.28 | 43.34 ± 14.89 | 22.77 ± 13.15 | 8.88 ± 6.58 | |
| n | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | 4 | ||
| SMD (p) | −5.95 (0.000) | 6.47 (0.000) | −11.22 (0.000) | −1.38 (0.01) | −24.57 (0.000) | −0.54 (0.28) | 1.51 (0.003) | 5.58 (0.000) | |||
| Missing | mean ± SD | 8.46 ± 4.88 | 384.90 ± 159.35 | 77.81 ± 28.32 | 99.15 ± 134.94 | 8.33 ± 15.39 | 14.52 ± 9.26 | 34.10 ± 17.88 | 31.87 ± 16.92 | 19.36 ± 8.12 | |
| n | 13 | 8 | 8 | 8 | 4 | 11 | 11 | 11 | 11 | ||
| K-W ANOVA test between gene strata | H (1, N = 19) = 9.00 p = 0.003 | H (1, N = 19) = 0.09 p = 0.73 | H (1, N = 19) = 0.81 p = 0.37 | H (1, N = 19) = 9.29 p = 0.002 | H (1, N = 19) = 1.21 p = 0.27 | H (1, N = 20) =6.51 p = 0.01 | H (1, N = 20) = 1.08 p = 0.30 | ||||
| Epilepsy | Not have | mean ± SD | 8.23 ± 2.04 | 405.67 ± 37.23 | 82.33 ± 8.39 | 87.38 ± 41.96 | 1.17 ± 0.29 | 38.33 ± 14.01 | 41.33 ± 14.01 | 18.67 ± 7.23 | |
| n | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | |||
| SMD (p) | 3.20 (0.000) | 2.66 (0.000) | −3.74 (0.000) | 11.50 (0.000) | 0.20 (0.73) | −2.18 (0.000) | 1.20 (0.04) | ||||
| Have | mean ± SD | 8.65 ± 3.66 | 430.64 ± 153.8 | 69.67 ± 19.94 | 200.93 ± 168.11 | 23.56 ± 45.62 | 9.58 ± 10.95 | 35.73 ± 18.57 | 42.52 ± 24.4 | 11.73 ± 8.61 | |
| n | 22 | 22 | 22 | 22 | 8 | 22 | 22 | 22 | 22 | ||
| SMD (p) | 1.14 (0.000) | 3.04 (0.000) | −3.20 (0.000) | 0.23 (0.53) | −0.72 (0.001) | 0.47 (0.04) | −1.39 (0.000) | 2.92 (0.000) | |||
| Missing | mean ± SD | 7.23 ± 4.60 | 288 ± 284.26 | 57.01 ± 55.77 | 213 ± 275.77 | 14.23 ± 8.192 | 26.88 ± 7.32 | 35.48 ± 8.29 | 23.81 ± 6.04 | ||
| n | 16 | 2 | 2 | 2 | 5 | 5 | 6 | 6 | |||
| K-W ANOVA test between epilepsy strata | H (1, N = 25) = 0.06 p =0.80 | H (1, N = 25) = 1.28 p = 0.26 | H (1, N = 25) = 2.02 p = 0.16 | H (1, N = 25) = 1.03 p = 0.31 | H (1, N = 25) = 0.11 p = 0.74 | H (1, N = 25) = 0.02 p = 0.90 | H (1, N = 25) = 1.37 p = 0.24 | ||||
| Scoliosis | Have | mean ± SD | 9.48 ± 2.76 | 365.82 ± 102.02 | 66.24 ± 19.48 | 212.97 ± 172.35 | 2.21 ± 3.02 | 34.29 ± 20.28 | 50.53 ± 23.33 | 12.35 ± 9.16 | |
| n | 17 | 17 | 17 | 17 | 17 | 17 | 17 | 17 | |||
| SMD (p) | 3.35 (0.000) | 4.03 (0.000) | −3.76 (0.000) | 5.20 (0.000) | 0.65 (0.01) | −2.58 (0.000) | 2.82 (0.000) | ||||
| Missing | mean ± SD | 7.23 ± 4.60 | 504.81 ± 191.46 | 76.78 ± 25.01 | 148.81 ± 151.71 | 23.56 ± 45.62 | 19.06 ± 8.50 | 34.80 ± 11.67 | 29.53 ± 10.29 | 17.64 ± 8.89 | |
| n | 16 | 10 | 10 | 10 | 8 | 13 | 13 | 14 | 14 | ||
| A&T history | Not have | mean ± SD | 8.67 ± 2.07 | 364.91 ± 105.17 | 63.91 ± 23.08 | 249.69 ± 205.99 | 131.64 ± 1.63 | 27.73 ± 15.82 | 57.27 ± 19.87 | 12.64 ± 10.77 | |
| n | 11 | 11 | 11 | 11 | 11 | 11 | 11 | 11 | |||
| SMD (p) | 3.67 (0.000) | 4.61 (0.000) | −4.70 (0.000) | 8.92 (0.000) | 1.65 (0.000) | −4.23 (0.000) | 2.81 (0.000) | ||||
| Have | mean ± SD | 9.94 ± 2.68 | 404.40 ± 61.33 | 73.80 ± 7.92 | 143.61 ± 46.96 | 1.50 ± 2.06 | 39.40 ± 17.98 | 45.80 ± 20.01 | 12.80 ± 6.14 | ||
| n | 5 | 5 | 5 | 5 | 5 | 5 | 5 | 5 | |||
| SMD (p) | 3.13 (0.000) | 5.64 (0.000) | −7.18(0.000) | 9.59 (0.000) | 0.04 (0.93) | −2.79 (0.000) | 3.79 (0.000) | ||||
| Missing | mean ± SD | 7.74 ± 4.94 | 475.56 ± 205.93 | 74.71 ± 24.70 | 149.46 ± 143.94 | 23.56 ± 45.62 | 18.56 ± 8.38 | 38.10 ± 16.68 | 27.56 ± 12.51 | 16.93 ± 9.00 | |
| n | 17 | 11 | 11 | 11 | 8 | 14 | 14 | 15 | 15 | ||
| K-W ANOVA test between A&T history strata | H (1, N = 16) = 0.03 p =0.87 | H (1, N = 16) = 1.04 p = 0.31 | H (1, N = 16) = 1.16 p = 0.28 | H (1, N = 16) = 0.06 p = 0.82 | H (1, N = 16) = 1.41 p = 0.23 | H (1, N = 16) = 0.93 p = 0.34 | H (1, N = 16) = 0.03 p = 0.87 | ||||
3. Results
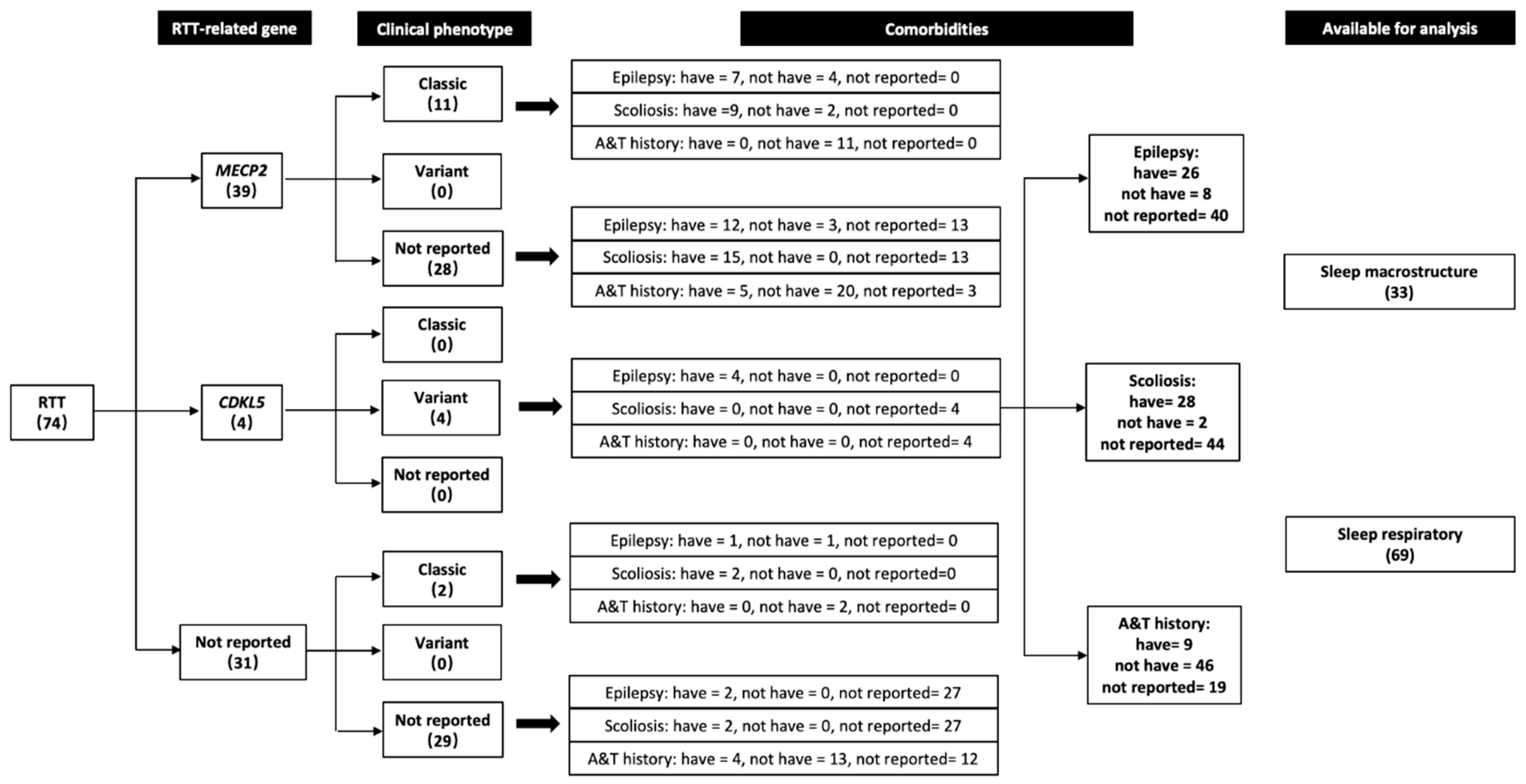
3.1. Cases Extracted from the Literature
3.2. Standard Sleep Macrostructure Parameters
3.2.1. TST (min)
3.2.2. SEI (%)
3.2.3. WASO (min)
3.2.4. SOL (min)
3.2.5. N1 (%) Stage
3.2.6. N2 (%) Stage
3.2.7. N3 (%) Stage
3.2.8. REM (%)
3.3. Sleep Respiratory Parameters of Literature Cases
3.4. Polysomnographic Parameters Correlated to Age
4. Discussion
4.1. Sleep Macrostructure
4.1.1. Total Sleep Time, Wakefulness after Sleep Onset, Sleep Efficiency
4.1.2. Stages N1, N2 and N3
4.1.3. Rapid Eye Movement Sleep
4.2. Sleep Respiratory Events
4.3. Associations with Age
4.4. Limitations and Future Scope
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neul, J.L.; Kaufmann, W.E.; Glaze, D.G.; Christodoulou, J.; Clarke, A.J.; Bahi-Buisson, N.; Leonard, H.; Bailey, M.E.; Schanen, N.C.; Zappella, M.; et al. Rett syndrome: Revised diagnostic criteria and nomenclature. Ann. Neurol. 2010, 68, 944–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amir, R.E.; Van den Veyver, I.B.; Wan, M.; Tran, C.Q.; Francke, U.; Zoghbi, H.Y. Rett syndrome is caused by mutations in X-linked MECP2, encoding methyl-CpG-binding protein 2. Nat. Genet. 1999, 23, 185–188. [Google Scholar] [CrossRef] [PubMed]
- Scala, E.; Ariani, F.; Mari, F.; Caselli, R.; Pescucci, C.; Longo, I.; Meloni, I.; Giachino, D.; Bruttini, M.; Hayek, G.; et al. CDKL5/STK9 is mutated in Rett syndrome variant with infantile spasms. J. Med. Genet. 2005, 42, 103–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roche-Martinez, A.; Gerotina, E.; Armstrong-Moron, J.; Sans-Capdevila, O.; Pineda, M. FOXG1, a new gene responsible for the congenital form of Rett syndrome. Revista De Neurologia 2011, 52, 597–602. [Google Scholar] [CrossRef]
- Laurvick, C.L.; de Klerk, N.; Bower, C.; Christodoulou, J.; Ravine, D.; Ellaway, C.; Williamson, S.; Leonard, H. Rett syndrome in Australia: A review of the epidemiology. J. Pediatrics. 2006, 148, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Hagberg, B.; Hanefeld, F.; Percy, A.; Skjeldal, O. An update on clinically applicable diagnostic criteria in Rett syndrome. Comments to Rett Syndrome Clinical Criteria Consensus Panel Satellite to European Paediatric Neurology Society Meeting, Baden Baden, Germany, 11 September 2001. Eur. J. Pediatr. Neurol. 2002, 6, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Hagberg, B. Clinical manifestations and stages of Rett syndrome. Ment. Retard. Dev. Disabil. Res. Rev. 2002, 8, 61–65. [Google Scholar] [CrossRef]
- Boban, S.; Wong, K.; Epstein, A.; Anderson, B.; Murphy, N.; Downs, J.; Leonard, H. Determinants of sleep disturbances in Rett syndrome: Novel findings in relation to genotype. Am. J. Med. Genetics Part A 2016, 170, 2292–2300. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.; Leonard, H.; Jacoby, P.; Ellaway, C.; Downs, J. The trajectories of sleep disturbances in Rett syndrome. J. Sleep Res. 2015, 24, 223–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boban, S.; Leonard, H.; Wong, K.; Wilson, A.; Downs, J. Sleep disturbances in Rett syndrome: Impact and management including use of sleep hygiene practices. Am. J. Med. Genetics Part A 2018, 176, 1569–1577. [Google Scholar] [CrossRef] [PubMed]
- Hagebeuk, E.E.; van den Bossche, R.A.; de Weerd, A.W. Respiratory and sleep disorders in female children with atypical Rett syndrome caused by mutations in the CDKL5 gene. Dev. Med. Child Neurol. 2012, 55, 480–484. [Google Scholar] [CrossRef] [PubMed]
- Carotenuto, M.; Esposito, M.; D'Aniello, A.; Rippa, C.D.; Precenzano, F.; Pascotto, A.; Bravaccio, C.; Elia, M. Polysomnographic findings in Rett syndrome: A case-control study. Sleep Breath 2013, 17, 93–98. [Google Scholar] [CrossRef]
- Amaddeo, A.; De Sanctis, L.; Arroyo, J.O.; Khirani, S.; Bahi-Buisson, N.; Fauroux, B. Polysomnographic findings in Rett syndrome. Eur. J. Paediatr. Neurol. EJPN 2019, 23, 214–221. [Google Scholar] [CrossRef] [Green Version]
- Marcus, C.L.; Carroll, J.L.; McColley, S.A.; Loughlin, G.M.; Curtis, S.; Pyzik, P.; Naidu, S. Polysomnographic characteristics of patients with Rett syndrome. J. Pediatrics. 1994, 125, 218–224. [Google Scholar] [CrossRef]
- Nomura, Y.; Segawa, M.; Higurashi, M. Rett syndrome—an early catecholamine and indolamine deficient disorder? Brain Dev. 1985, 7, 334–341. [Google Scholar] [CrossRef]
- Julu, P.O.; Kerr, A.M.; Apartopoulos, F.; Al-Rawas, S.; Engerstrom, I.W.; Engerstrom, L.; Jamal, G.A.; Hansen, S. Characterisation of breathing and associated central autonomic dysfunction in the Rett disorder. Arch. Dis. Child. 2001, 85, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Julu, P.O.; Witt Engerström, I. Assessment of the maturity-related brainstem functions reveals the heterogeneous phenotypes and facilitates clinical management of Rett syndrome. Brain Dev. 2005, 27 (Suppl. 1), S43–S53. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Lin, J.S.; Spruyt, K. Sleep problems in Rett syndrome animal models: A systematic review. J. Neurosci. Res. 2020. [Google Scholar] [CrossRef]
- Spruyt, K. Sleep problems in individuals with Rett Syndrome: A Meta-Review. (submitted).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. for the PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhat, S.; Ming, X.; Dekermenjian, R.; Chokroverty, S. Continuous spike and wave in slow-wave sleep in a patient with Rett syndrome and in a patient with Lhermitte-Duclos syndrome and neurofibromatosis 1. J. Child Neurol. 2014, 29, NP176–NP180. [Google Scholar] [CrossRef]
- Iber, C.; Ancoli-Israel, S.; Chesson, A.L.; Quan, S.F. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; American Academy of Sleep Medicine: Darien, IL, USA, 2007; Volume 1. [Google Scholar]
- Scholle, S.; Beyer, U.; Bernhard, M.; Eichholz, S.; Erler, T.; Graness, P.; Goldmann-Schnalke, B.; Heisch, K.; Kirchhoff, F.; Klementz, K.; et al. Normative values of polysomnographic parameters in childhood and adolescence: Quantitative sleep parameters. Sleep Med. 2011, 12, 542–549. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung and Blood Institute. Development and Use of Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 10 February 2022).
- DelRosso, L.M.; Picchietti, D.L.; Spruyt, K.; Bruni, O.; Garcia-Borreguero, D.; Kotagal, S.; Owens, J.A.; Simakajornboon, N.; Ferri, R. Restless sleep in children: A systematic review. Sleep Med. Rev. 2021, 56, 101406. [Google Scholar] [CrossRef] [PubMed]
- Braam, W.; Spruyt, K. Reference intervals for 6-Sulfatoxymelatonin in urine: A meta-analysis. Sleep Med. Rev. 2022, 101614. [Google Scholar] [CrossRef]
- Cacciatori, E.; Lelii, M.; Russo, S.; Alari, V.; Masciadri, M.; Guez, S.; Patria, M.F.; Marchisio, P.; Milani, D. Sleep disordered breathing and daytime hypoventilation in a male with MECP2 mutation. Am. J. Med. Genetics. Part A 2020, 182, 2982–2987. [Google Scholar] [CrossRef]
- Sarber, K.M.; Howard, J.J.M.; Dye, T.J.; Pascoe, J.E.; Simakajornboon, N. Sleep-Disordered Breathing in Pediatric Patients With Rett Syndrome. J. Clin. Sleep Med. JCSM 2019, 15, 1451–1457. [Google Scholar] [CrossRef]
- Ohno, K.; Saito, Y.; Ueda, R.; Togawa, M.; Ohmae, T.; Matsuda, E.; Fujiyama, M.; Maegaki, Y. Effect of Serotonin 1A Agonists and Selective Serotonin Reuptake Inhibitors on Behavioral and Nighttime Respiratory Symptoms in Rett Syndrome. Pediatric Neurol. 2016, 60, 54–59.e51. [Google Scholar] [CrossRef] [PubMed]
- Bassett, E.; Heinle, R.; Johnston, D. Sleep Apnea in Patients With Rett Syndrome: Roles for Polysomnography and Adenotonsillectomy. J. Child Neurol. 2016, 31, 1633–1634. [Google Scholar] [CrossRef] [PubMed]
- Hagebeuk, E.E.; Bijlmer, R.P.; Koelman, J.H.; Poll-The, B.T. Respiratory disturbances in rett syndrome: Don't forget to evaluate upper airway obstruction. J. Child Neurol. 2012, 27, 888–892. [Google Scholar] [CrossRef] [PubMed]
- d'Orsi, G.; Demaio, V.; Scarpelli, F.; Calvario, T.; Minervini, M.G. Central sleep apnoea in Rett syndrome. Neurol. Sci. 2009, 30, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Schluter, B.; Aguigah, G.; Buschatz, D.; Trowitzsch, E.; Aksu, F. Polysomnographic recordings of respiratory disturbances in Rett syndrome. J. Sleep Res. 1995, 4, 203–207. [Google Scholar] [CrossRef]
- Aldrich, M.S.; Garofalo, E.A.; Drury, I. Epileptiform abnormalities during sleep in Rett syndrome. Electroencephalogr. Clin. Neurophysiol. 1990, 75, 365–370. [Google Scholar] [CrossRef]
- Hagberg, B.; Witt-Engerstrom, I. Rett syndrome: A suggested staging system for describing impairment profile with increasing age towards adolescence. Am. J. Med. Genetics 1986, 1, 47–59. [Google Scholar] [CrossRef] [PubMed]
- Kerr, A.M.; Nomura, Y.; Armstrong, D.; Anvret, M.; Belichenko, P.V.; Budden, S.; Cass, H.; Christodoulou, J.; Clarke, A.; Ellaway, C.; et al. Guidelines for reporting clinical features in cases with MECP2 mutations. Brain Dev. 2001, 23, 208–211. [Google Scholar] [CrossRef]
- Mari, F.; Azimonti, S.; Bertani, I.; Bolognese, F.; Colombo, E.; Caselli, R.; Scala, E.; Longo, I.; Grosso, S.; Pescucci, C.; et al. CDKL5 belongs to the same molecular pathway of MeCP2 and it is responsible for the early-onset seizure variant of Rett syndrome. Hum. Mol. Genet. 2005, 14, 1935–1946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rusconi, L.; Salvatoni, L.; Giudici, L.; Bertani, I.; Kilstrup-Nielsen, C.; Broccoli, V.; Landsberger, N. CDKL5 expression is modulated during neuronal development and its subcellular distribution is tightly regulated by the C-terminal tail. J. Biol. Chem. 2008, 283, 30101–30111. [Google Scholar] [CrossRef] [Green Version]
- Bebbington, A.; Percy, A.; Christodoulou, J.; Ravine, D.; Ho, G.; Jacoby, P.; Anderson, A.; Pineda, M.; Ben Zeev, B.; Bahi-Buisson, N.; et al. Updating the profile of C-terminal MECP2 deletions in Rett syndrome. J. Med. Genet. 2010, 47, 242–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glaze, D.G.; Frost, J.D., Jr.; Zoghbi, H.Y.; Percy, A.K. Rett's syndrome: Characterization of respiratory patterns and sleep. Ann. Neurol. 1987, 21, 377–382. [Google Scholar] [CrossRef]
- Brown, R.E.; Basheer, R.; McKenna, J.T.; Strecker, R.E.; McCarley, R.W. Control of sleep and wakefulness. Physiol. Rev. 2012, 92, 1087–1187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dijk, D.J.; Landolt, H.P. Sleep Physiology, Circadian Rhythms, Waking Performance and the Development of Sleep-Wake Therapeutics. Handb. Exp. Pharmacol. 2019, 253, 441–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franken, P.; Tobler, I.; Borbely, A.A. Sleep homeostasis in the rat: Simulation of the time course of EEG slow-wave activity. Neurosci. Lett. 1991, 130, 141–144. [Google Scholar] [CrossRef]
- Altevogt, B.M.; Colten, H.R. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem; The National Academies: Washington, DC, USA, 2006. [Google Scholar] [CrossRef] [PubMed]
- Saper, C.B.; Fuller, P.M.; Pedersen, N.P.; Lu, J.; Scammell, T.E. Sleep state switching. Neuron 2010, 68, 1023–1042. [Google Scholar] [CrossRef] [Green Version]
- Weaving, L.S.; Christodoulou, J.; Williamson, S.L.; Friend, K.L.; McKenzie, O.L.; Archer, H.; Evans, J.; Clarke, A.; Pelka, G.J.; Tam, P.P.; et al. Mutations of CDKL5 cause a severe neurodevelopmental disorder with infantile spasms and mental retardation. Am. J. Hum. Genet. 2004, 75, 1079–1093. [Google Scholar] [CrossRef] [Green Version]
- St Louis, E.K. Sleep and Epilepsy: Strange Bedfellows No More. Minerva Pneumol. 2011, 50, 159–176. [Google Scholar] [PubMed]
- Goffin, D.; Zhou, Z.J. The neural circuit basis of Rett syndrome. Front Biol. 2012, 7, 428–435. [Google Scholar] [CrossRef] [Green Version]
- Ammanuel, S.; Chan, W.C.; Adler, D.A.; Lakshamanan, B.M.; Gupta, S.S.; Ewen, J.B.; Johnston, M.V.; Marcus, C.L.; Naidu, S.; Kadam, S.D. Heightened Delta Power during Slow-Wave-Sleep in Patients with Rett Syndrome Associated with Poor Sleep Efficiency. PLoS ONE 2015, 10, e0138113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinar-Sierra, J.; Toledano, M.A.; Franco, C.; Campos-Castello, J.; Gonzalez-Hidalgo, M.; Oliete, F.; Garcia-Nart, M. Rett's syndrome: A neurophysiological study. Neurophysiol. Clin. 1990, 20, 35–42. [Google Scholar] [CrossRef]
- Garofalo, E.A.; Drury, I.; Goldstein, G.W. eeg abnormalities aid diagnosis of rett syndrome. Pediatric Neurol. 1988, 4, 350–353. [Google Scholar] [CrossRef] [Green Version]
- Frauscher, B.; von Ellenrieder, N.; Ferrari-Marinho, T.; Avoli, M.; Dubeau, F.; Gotman, J. Facilitation of epileptic activity during sleep is mediated by high amplitude slow waves. Brain 2015, 138, 1629–1641. [Google Scholar] [CrossRef] [Green Version]
- Williams, S.R.; Turner, J.P.; Crunelli, V. Gamma-hydroxybutyrate promotes oscillatory activity of rat and cat thalamocortical neurons by a tonic GABAB, receptor-mediated hyperpolarization. Neuroscience 1995, 66, 133–141. [Google Scholar] [CrossRef]
- Dijk, D.J.; Hayes, B.; Czeisler, C.A. Dynamics of electroencephalographic sleep spindles and slow wave activity in men: Effect of sleep deprivation. Brain Res. 1993, 626, 190–199. [Google Scholar] [CrossRef]
- Buzsaki, G.; Bickford, R.G.; Ponomareff, G.; Thal, L.J.; Mandel, R.; Gage, F.H. Nucleus basalis and thalamic control of neocortical activity in the freely moving rat. J. Neurosci. 1988, 8, 4007–4026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gottesmann, C. GABA mechanisms and sleep. Neuroscience 2002, 111, 231–239. [Google Scholar] [CrossRef]
- Chao, H.T.; Chen, H.; Samaco, R.C.; Xue, M.; Chahrour, M.; Yoo, J.; Neul, J.L.; Gong, S.; Lu, H.C.; Heintz, N.; et al. Dysfunction in GABA signalling mediates autism-like stereotypies and Rett syndrome phenotypes. Nature 2010, 468, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Marks, G.A.; Shaffery, J.P.; Oksenberg, A.; Speciale, S.G.; Roffwarg, H.P. A functional role for REM sleep in brain maturation. Behav Brain Res 1995, 2510, 1–11. [Google Scholar] [CrossRef]
- Peever, J.; Fuller, P.M. The Biology of REM Sleep. Curr. Biol. 2017, 27, R1237–R1248. [Google Scholar] [CrossRef]
- Del Rio-Bermudez, C.; Blumberg, M.S. Sleep as a window on the sensorimotor foundations of the developing hippocampus. Hippocampus 2022, 32, 89–97. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Carskadon, M.A.; Guilleminault, C.; Vitiello, M.V. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: Developing normative sleep values across the human lifespan. Sleep 2004, 27, 1255–1273. [Google Scholar] [CrossRef]
- Johnston, M.V.; Ammanuel, S.; O'Driscoll, C.; Wozniak, A.; Naidu, S.; Kadam, S.D. Twenty-four hour quantitative-EEG and in-vivo glutamate biosensor detects activity and circadian rhythm dependent biomarkers of pathogenesis in Mecp2 null mice. Front. Syst. Neurosci. 2014, 8, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, C.J.; Lydic, R.; Baghdoyan, H.A. Sleep duration varies as a function of glutamate and GABA in rat pontine reticular formation. J. Neurochem. 2011, 118, 571–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thapa, S.; Venkatachalam, A.; Khan, N.; Naqvi, M.; Balderas, M.; Runge, J.K.; Haag, A.; Hoch, K.M.; Glaze, D.G.; Luna, R.A.; et al. Assessment of the gut bacterial microbiome and metabolome of girls and women with Rett Syndrome. PLoS ONE 2021, 16, e0251231. [Google Scholar] [CrossRef] [PubMed]
- Elia, M.; Ferri, R.; Musumeci, S.A.; Del Gracco, S.; Bottitta, M.; Scuderi, C.; Miano, G.; Panerai, S.; Bertrand, T.; Grubar, J.C. Sleep in subjects with autistic disorder: A neurophysiological and psychological study. Brain Dev. 2000, 22, 88–92. [Google Scholar] [CrossRef]
- Miano, S.; Bruni, O.; Elia, M.; Scifo, L.; Smerieri, A.; Trovato, A.; Verrillo, E.; Terzano, M.G.; Ferri, R. Sleep phenotypes of intellectual disability: A polysomnographic evaluation in subjects with Down syndrome and Fragile-X syndrome. Clin. Neurophysiol. 2008, 119, 1242–1247. [Google Scholar] [CrossRef]
- Miano, S.; Bruni, O.; Elia, M.; Musumeci, S.A.; Verrillo, E.; Ferri, R. Sleep breathing and periodic leg movement pattern in Angelman Syndrome: A polysomnographic study. Clin. Neurophysiol 2005, 116, 2685–2692. [Google Scholar] [CrossRef]
- Gombos, F.; Bódizs, R.; Kovács, I. Atypical sleep architecture and altered EEG spectra in Williams syndrome. J. Intellect. Disabil. Res. 2011, 55, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Picchioni, D.; Reith, R.M.; Nadel, J.L.; Smith, C.B. Sleep, plasticity and the pathophysiology of neurodevelopmental disorders: The potential roles of protein synthesis and other cellular processes. Brain Sci. 2014, 4, 150141201. [Google Scholar] [CrossRef] [Green Version]
- Fasolino, M.; Zhou, Z. The Crucial Role of DNA Methylation and MeCP2 in Neuronal Function. Genes 2017, 8, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Na, E.S.; Nelson, E.D.; Kavalali, E.T.; Monteggia, L.M. The Impact of MeCP2 Loss- or Gain-of-Function on Synaptic Plasticity. Neuropsychopharmacology 2013, 38, 212–219. [Google Scholar] [CrossRef] [Green Version]
- Young, D.; Nagarajan, L.; de Klerk, N.; Jacoby, P.; Ellaway, C.; Leonard, H. Sleep problems in Rett syndrome. Brain Dev. 2007, 29, 609–616. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, J.M.; Ward, C.S.; Neul, J.L. Breathing challenges in Rett syndrome: Lessons learned from humans and animal models. Respir. Physiol. Neurobiol. 2013, 189, 280–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, D.D.; Deguchi, K.; Antallfy, B. Survey of MeCP2 in the Rett syndrome and the non-Rett syndrome brain. J. Child Neurol. 2003, 18, 683–687. [Google Scholar] [CrossRef] [PubMed]
- Caballero, I.M.; Hendrich, B. MeCP2 in neurons: Closing in on the causes of Rett syndrome. Hum. Mol. Genet. 2005, 14, R19–R26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, M.V.; Du, F.; Felice, C.A.; Shan, X.; Nigam, A.; Mandel, G.; Robinson, J.K.; Ballas, N. MeCP2 is critical for maintaining mature neuronal networks and global brain anatomy during late stages of postnatal brain development and in the mature adult brain. J. Neurosci. 2012, 32, 1002–10034. [Google Scholar] [CrossRef]



| Parameters | Age | AHI | OAHI | CAI | OAI | ODI | SpO2% Nadir | SpO2% Mean | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Total RTT group {* cases excluded} | mean ± SD | 8.93 ± 5.15 {8.86 ± 55.37} | 12.25 ± 23.89 {11.92 ± 23.67} | 6.53 ± 8.67 {6.80 ± 9.30} | 6.8 ± 25.09 {8.54 ± 28.40} | 1.9 ± 3.91 {2.08 ± 4.81} | 18.62 ± 31.9 {19.01 ± 32.48} | 84.37 ± 14.42 {85.53 ± 10.85} | 96.25 ± 1.89 {96.14 ± 2.02} | |
| n | 69 {59} | 63 {53} | 42 {32} | 31 {24} | 15 {13} | 31 {23} | 66 {56} | 36 {29} | ||
| Gene | MECP2 | mean ± SD | 8.71 ± 5.33 | 14.77 ± 28.32 | 6.36 ± 9.06 | 12.18 ± 34.53 | 0 | 19.59 ± 33.82 | 83.59 ± 11.71 | 96.07 ± 11.76 |
| n | 39 | 39 | 36 | 16 | 1 | 27 | 38 | 25 | ||
| CDKL5 | mean ± SD | 6.5 ± 5.80 | 1.48 ± 2.29 | 90.67 ± 3.21 | 96.30 ± 0.52 | |||||
| n | 4 | 4 | - | - | - | - | 3 | 3 | ||
| Missing | mean ± SD | 9.63 ± 4.82 | 9.49 ± 14.57 | 7.58 ± 6.33 | 1.05 ± 1.53 | 2.04 ± 4.02 | 12.05 ± 14.20 | 88.16 ± 9.95 | 96.77 ± 0.79 | |
| n | 26 | 20 | 6 | 15 | 14 | 4 | 25 | 8 | ||
| K-W ANOVA test between gene strata | H (1, N = 43) = 3.47 p = 0.06 | NA | NA | NA | NA | H (1, N = 42) = 1.22, p = 0.27 | H (1, N = 28) = 0.13, p = 0.91 | |||
| Epilepsy | Not have | mean ± SD | 9.75 ± 4.22 | 7.44 ± 6.85 | 6.29 ± 6.84 | 0.33 ± 0.58 | 3.33 ± 3.22 | 88.50 ± 4.40 | 97.33 ± 1.16 | |
| n | 8 | 8 | 8 | 3 | - | 3 | 8 | 3 | ||
| Have | mean ± SD | 9.87 ± 3.76 | 17.16 ± 32.78 | 8.34 ±10.56 | 13.50 ± 36.89 | 25.32 ± 40.10 | 84.45 ±11.94 | 96.50 ± 2.03 | ||
| n | 22 | 22 | 22 | 14 | - | 14 | 22 | 14 | ||
| Missing | mean ± SD | 8.23 ± 5.93 | 10.15 ± 19.07 | 3.40 ± 4.52 | 1.48 ± 1.81 | 1.90 ± 3.91 | 15.18 ± 24.98 | 85.74 ± 11.50 | 95.89 ± 1.85 | |
| n | 39 | 33 | 12 | 14 | 15 | 14 | 36 | 19 | ||
| K-W ANOVA test between epilepsy strata | H (1, N = 30) = 0.12, p = 0.73 | H (1, N = 30) = 0.06, p = 0.81 | H (1, N = 17) = 0.14, p =0.71 | NA | H (1, N = 17) = 1.44, p = 0.23 | H (1, N = 30) = 0.06, p = 0.81 | H (1, N = 17) = 0.71, p = 0.40 | |||
| Scoliosis | Not have | mean ± SD | 7.0 ± 2.69 | 4.20 ± 3.96 | 3.35 ± 3.46 | 90.20 ± 1.27 | ||||
| n | 2 | 2 | 2 | - | - | - | 2 | - | ||
| Have | mean ± SD | 10.03 ± 3.84 | 15.31 ± 29.32 | 8.10 ± 9.88 | 11.18 ± 33.65 | 21.44 ± 37.19 | 85.19 ± 10.85 | 96.65 ± 1.90 | ||
| n | 28 | 28 | 28 | 17 | - | 17 | 28 | 17 | ||
| Missing | mean ± SD | 8.23 ± 5.93 | 10.15 ± 19.07 | 3.40 ± 4.52 | 1.48 ± 1.81 | 1.90 ± 3.91 | 15.18 ± 24.98 | 85.74 ± 11.50 | 98.89 ± 1.85 | |
| n | 39 | 33 | 12 | 14 | 15 | 14 | 36 | 19 | ||
| K-W ANOVA test between scoliosis strata | H (1, N = 30) = 0.21, p = 0.65 | H (1, N = 30) = 0.17, p = 0.68 | NA | NA | NA | H (1, N = 30) = 0.69, p = 0.41 | NA | |||
| A&T history | Not have | mean ± SD | 9.09 ± 5.45 | 12.46 ± 24.85 | 6.88 ± 9.43 | 9.10 ± 29.65 | 2.25 ± 4.32 | 18.81 ± 33.89 | 83.91 ± 11.64 | 95.96 ± 2.33 |
| n | 46 | 46 | 34 | 22 | 12 | 21 | 45 | 21 | ||
| Have | mean ± SD | 10.27 ± 2.37 | 5.80 ± 4.22 | 5.21 ± 4.56 | 0.81 ±0.94 | 0.75 ± 1.06 | 6.31 ± 7.75 | 86.89 ±12.79 | 96.70 ± 1.19 | |
| n | 9 | 9 | 7 | 7 | 2 | 7 | 9 | 7 | ||
| Missing | mean ± SD | 7.53 ± 5.36 | 18.30 ± 31.17 | 4 | 2.45 ± 3.47 | 0 | 45.93 ± 44.28 | 91.23 ± 2.52 | 96.61 ± 0.69 | |
| n | 14 | 8 | 1 | 2 | 1 | 3 | 12 | 8 | ||
| K-W ANOVA test between A&T history strata | H (1, N = 55) = 0.05, p = 0.83 | H (1, N = 55) = 0.10, p = 0.76 | H (1, N = 29) = 0.03, p = 0.87 | H (1, N = 14) = 0.08, p = 0.78 | H (1, N = 28) = 0.86, p = 0.35 | H (1, N = 54) = 1.46, p = 0.23 | H (1, N = 28) = 0.44, p = 0.51 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.-Y.; Spruyt, K. Literature Cases Summarized Based on Their Polysomnographic Findings in Rett Syndrome. Int. J. Environ. Res. Public Health 2022, 19, 3422. https://doi.org/10.3390/ijerph19063422
Zhang X-Y, Spruyt K. Literature Cases Summarized Based on Their Polysomnographic Findings in Rett Syndrome. International Journal of Environmental Research and Public Health. 2022; 19(6):3422. https://doi.org/10.3390/ijerph19063422
Chicago/Turabian StyleZhang, Xin-Yan, and Karen Spruyt. 2022. "Literature Cases Summarized Based on Their Polysomnographic Findings in Rett Syndrome" International Journal of Environmental Research and Public Health 19, no. 6: 3422. https://doi.org/10.3390/ijerph19063422