
Pregnancy Activity Levels and Impediments in the Era of COVID-19 Based on the Health Belief Model: A Cross-Sectional Study




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Respondents
2.2. Materials
2.2.1. Survey Tool
2.2.2. Pregnancy Physical Activity-Related Health Belief Model Assessment
2.2.3. Data Collection
2.3. Statistical Methods
3. Results
3.1. Demographic Characteristics
3.2. Health Belief Level (HBL) and Prenatal Physical Activity
3.3. Physical Activity Expenditure during Pregnancy
3.4. The Association between Demographic Factors, Health Belief Model Dimensions, and Pregnancy Physical Activity
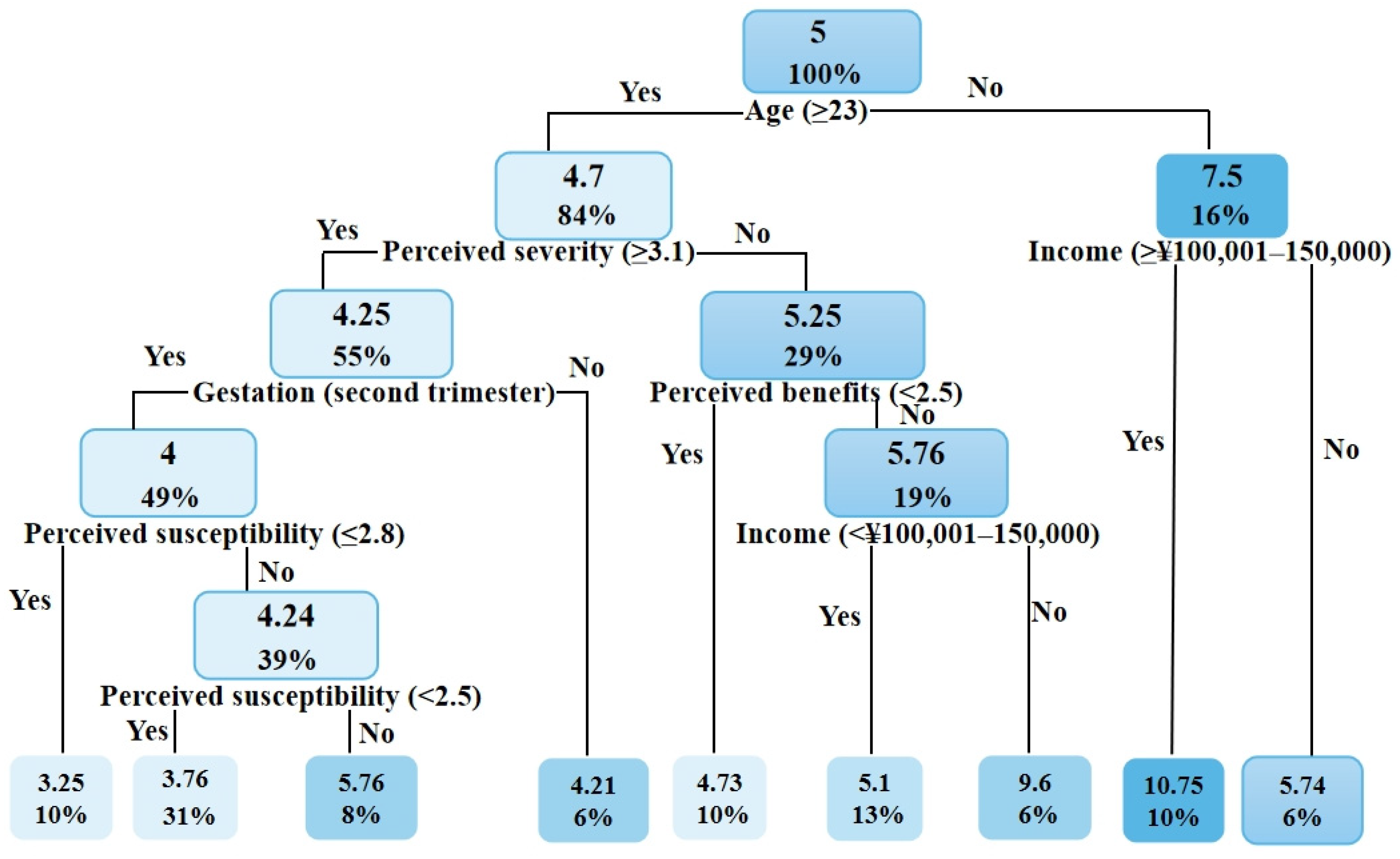
3.5. Construction of Classification and Regression Tree (CART)
4. Discussion
4.1. Overview of Hypothesis Validation Findings
4.1.1. Health-Belief Level (HBL)
4.1.2. Physical Activity Status of Pregnant Women
4.1.3. Connection between Health Belief, Demographic Factors, and Prenatal Physical Activity
4.2. Classification and Regression Tree
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leite, J.; Pereira, G. The situation of women among progress and challenges. J. Contemp. Public Law 2021, 1, 143. [Google Scholar]
- Assembly, G. Sustainable development goals. SDGs Transform Our World 2015, 82, 20–23. [Google Scholar]
- Boron, A. Epigenetic impact of the parents’ physical activity on the health of their children. Balt. J. Health Phys. Act. 2021, 13, 87–95. [Google Scholar] [CrossRef]
- Hinman, S.K.; Smith, K.B.; Quillen, D.M.; Smith, M.S. Exercise in pregnancy: A clinical review. Sports Health 2015, 7, 527–531. [Google Scholar] [CrossRef] [Green Version]
- Vargas-Terrones, M.; Barakat, R.; Santacruz, B.; Fernandez-Buhigas, I.; Mottola, M.F. Physical exercise programme during pregnancy decreases perinatal depression risk: A randomised controlled trial. Br. J. Sports Med. 2019, 53, 348–353. [Google Scholar] [CrossRef]
- Ferrari, N.; Joisten, C. Impact of physical activity on course and outcome of pregnancy from pre- to postnatal. Eur. J. Clin. Nutr. 2021, 75, 1698–1709. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126. [Google Scholar]
- Ferguson, B. ACSM’s guidelines for exercise testing and prescription 9th Ed. 2014. J. Can. Chiropr. Association 2014, 58, 328. [Google Scholar]
- Boone, T. The ASEP exercise physiologists’ way of prescribing exercise medicine. J. Exerc. Physiol. 2018, 21, 10–20. [Google Scholar]
- Meah, V.L.; Strynadka, M.C.; Khurana, R.; Davenport, M.H. Physical activity behaviors and barriers in multifetal pregnancy: What to expect when you’re expecting more. Int. J. Environ. Res. Public Health 2021, 18, 3907. [Google Scholar] [CrossRef]
- Connelly, M.; Brown, H.; van der Pligt, P.; Teychenne, M. Modifiable barriers to leisure-time physical activity during pregnancy: A qualitative study investigating first time mother’s views and experiences. BMC Pregnancy Childbirth 2015, 15, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horak, T.A.; Osman, A. Exercise in pregnancy: Review. Obstet. Gynaecol. Forum 2012, 22, 13–16. [Google Scholar]
- Short, C.E.; Vandelanotte, C.; Rebar, A.; Duncan, M.J. A comparison of correlates associated with adult physical activity behavior in major cities and regional settings. Health Psychol. 2014, 33, 1319–1327. [Google Scholar] [CrossRef] [PubMed]
- Decision of the CPC Central Committee and the State Council on Implementing the Universal Two-Child Policy Reform and Improving the Management of Family Planning Services. Available online: http://www.gov.cn/gongbao/content/2016/content_5033853.htm (accessed on 31 December 2015).
- Department of Economic and Social Affairs Disability in United Nations (DESAD). The 17 Sustainable Development Goals (SDGs) to Transform Our World). 2021. Available online: https://www.un.org/development/desa/disabilities/envision2030.html (accessed on 22 February 2022).
- Smedley, J.; Jancey, J.M.; Dhaliwal, S.; Zhao, Y.; Monteiro, S.M.D.R.; Howat, P. Women’s reported health behaviours before and during pregnancy: A retrospective study. Health Educ. J. 2013, 73, 28–40. [Google Scholar] [CrossRef]
- Sui, Z.; Moran, L.J.; Dodd, J.M. Physical activity levels during pregnancy and gestational weight gain among women who are overweight or obese. Health Promot. J. Austr. 2013, 24, 206–213. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social learning theory and the health belief model. Health Educ. Q. 1988, 15, 175–183. [Google Scholar] [CrossRef]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhao, Y.; Dong, S.; Xiong, Y.; Hu, X. Reliability and validity of the Chinese version of the Pregnancy Physical Activity Questionnaire (PPAQ). Chin. Nurs. Res. 2013, 48, 825–827. [Google Scholar]
- Shephard, R. Compendium of physical activities: A second update of codes and MET values. Sports Med. 2011, 2012, 126–127. [Google Scholar]
- ACOG Committee Obstetric Practice; ACOG Committee opinion. Exercise during pregnancy and the postpartum period. Obs. Gynecol 2002, 99, 171–173. [Google Scholar]
- Yang, C.; Kasales, C.J.; Ouyang, T.; Peterson, C.M.; Sarwani, N.I.; Tappouni, R.; Bruno, M. A succinct rating scale for radiology report quality. SAGE Open Med. 2014, 2. [Google Scholar] [CrossRef] [PubMed]
- DeVellis, R.F.; Thorpe, C.T. Scale Development: Theory and Applications, 3rd ed.; DeVellis, R.F., Ed.; Sage publications: Thousand Oaks, CA, USA, 2021; p. 31. [Google Scholar]
- Loh, W.-Y. Classification and regression trees. WIREs Data Min. Knowl. Discov. 2011, 1, 14–23. [Google Scholar] [CrossRef]
- Symons Downs, D.; Hausenblas, H.A. Exercising for two: Examining pregnant women’s second trimester exercise intention and behavior using the framework of the theory of planned behavior. Women’s Health Issues 2003, 13, 222–228. [Google Scholar] [CrossRef]
- Da Costa, D.; Ireland, K. Perceived benefits and barriers to leisure-time physical activity during pregnancy in previously inactive and active women. Women Health 2013, 53, 185–202. [Google Scholar] [CrossRef]
- Janakiraman, B.; Gebreyesus, T.; Yihunie, M.; Genet, M.G. Knowledge, attitude, and practice of antenatal exercises among pregnant women in Ethiopia: A cross-sectional study. PLoS ONE 2021, 16, e0247533. [Google Scholar] [CrossRef]
- Bort-Roig, J.; Gilson, N.D.; Puig-Ribera, A.; Contreras, R.S.; Trost, S.G. Measuring and influencing physical activity with smartphone technology: A systematic review. Sports Med. 2014, 44, 671–686. [Google Scholar] [CrossRef]
- Füzéki, E.; Groneberg, D.A.; Banzer, W. Physical activity during COVID-19 induced lockdown: Recommendations. J. Occup. Med. Toxicol. 2020, 15, 25. [Google Scholar] [CrossRef]
- Hori, N.; Shiraishi, M.; Harada, R.; Kurashima, Y. Association of lifestyle changes due to the COVID-19 pandemic with nutrient intake and physical activity levels during pregnancy in Japan. Nutrients 2021, 13, 3799. [Google Scholar] [CrossRef]
- Ghesquière, L.; Garabedian, C.; Drumez, E.; Lemaître, M.; Cazaubiel, M.; Bengler, C.; Vambergue, A. Effects of COVID-19 pandemic lockdown on gestational diabetes mellitus: A retrospective study. Diabetes Metab. J. 2021, 47, 101201. [Google Scholar] [CrossRef]
- Withers, M.; Kharazmi, N.; Lim, E. Traditional beliefs and practices in pregnancy, childbirth and postpartum: A review of the evidence from Asian countries. Midwifery 2018, 56, 158–170. [Google Scholar] [CrossRef]
- Lee, D.T.S.; Ngai, I.S.L.; Ng, M.M.T.; Lok, I.H.; Yip, A.S.K.; Chung, T.K.H. Antenatal taboos among Chinese women in Hong Kong. Midwifery 2009, 25, 104–113. [Google Scholar] [CrossRef] [PubMed]
- Dichter, M.N.; Sander, M.; Seismann-Petersen, S.; Köpke, S. COVID-19: It is time to balance infection management and person-centered care to maintain mental health of people living in German nursing homes. Int. Psychogeriatr. 2020, 32, 1157–1160. [Google Scholar] [CrossRef] [PubMed]
- Gentil, P.; de Lira, C.A.B.; Coswig, V.; Barroso, W.K.S.; Vitorino, P.V.d.O.; Ramirez-Campillo, R.; Martins, W.; Souza, D. Practical recommendations relevant to the use of resistance training for COVID-19 survivors. Front. Physiol. 2021, 12, 142. [Google Scholar] [CrossRef]
- Li, J.; Zhou, F.L.; Huang, S.R.; Zhai, J.G.; Cai, W.Z. A survey on health beliefs and health behaviors of pregnant women. J. Nurs. 2017, 32, 25–28. [Google Scholar]
- Young, M.D.; Plotnikoff, R.C.; Collins, C.E.; Callister, R.; Morgan, P.J. Social cognitive theory and physical activity: A systematic review and meta-analysis. Obes. Rev. 2014, 15, 983–995. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Gao, H.; Jin, Z.; Zhu, J.; Yu, H.; Jiang, Y.; Zou, J. Application of a knowledge, attitude, belief, and practice model in pain management of patients with acute traumatic fractures and alcohol dependence. Pain Res. Manag. 2022, 2022, 8110896. [Google Scholar] [CrossRef]
- Ahmadi, K.; Amiri-Farahani, L.; Haghani, S.; Hasanpoor-Azghady, S.B.; Pezaro, S. Exploring the intensity, barriers and correlates of physical activity In Iranian pregnant women: A cross-sectional study. BMJ Open Sport Exerc. Med. 2021, 7, e001020. [Google Scholar]
- Garland, M.; Wilbur, J.; Semanik, P.; Fogg, L. Correlates of physical activity during pregnancy: A systematic review with implications for evidence-based practice. Worldviews Evid.-Based Nurs. 2019, 16, 310–318. [Google Scholar] [CrossRef]
- Levesque, A.; Li, H.Z. The relationship between culture, health conceptions, and health practices: A qualitative–quantitative approach. J. Cross-Cult. Psychol. 2014, 45, 628–645. [Google Scholar] [CrossRef]
- Tucker, E.A.; Fouts, H.N. Connections between prenatal physical activity and breastfeeding decisions. Qual. Health Res. 2016, 27, 700–713. [Google Scholar] [CrossRef]
- Tugut, N.; Yesildag Celik, B.; Yılmaz, A. Health literacy and its association with healthperception in pregnant women. J. Health Lit. 2021, 6, 9–20. [Google Scholar]
- Yu, H.; Sun, C.; Sun, B.; Chen, X.; Tan, Z. Systematic review and meta-analysis of the relationship between actual exercise intensity and rating of perceived exertion in the overweight and obese population. Int. J. Environ. Res. Public Health 2021, 18, 12912. [Google Scholar] [CrossRef] [PubMed]
- Fitness Facilities and Institutions Statistics. Available online: http://www.stats.gov.cn/tjsj/ndsj/2020/indexch.htm (accessed on 31 December 2019).
- Hayman, M.; Alfrey, K.-L.; Cannon, S.; Alley, S.; Rebar, A.L.; Williams, S.; Short, C.E.; Altazan, A.; Comardelle, N.; Currie, S.; et al. Quality, features, and presence of behavior change techniques in mobile apps designed to improve physical activity in pregnant women: Systematic search and content analysis. JMIR Mhealth Uhealth 2021, 9, e23649. [Google Scholar] [CrossRef]
- Yu, H.; He, J.; Wang, X.; Yang, W.; Sun, B.; Szumilewicz, A. A comparison of functional features of Chinese and US mobile apps for pregnancy and postnatal care: A systematic app store search and content analysis. Front. Public Health 2022, 10, e826896. [Google Scholar] [CrossRef] [PubMed]
- Szumilewicz, A.; Santos-Rocha, R.; Worska, A.; Piernicka, M.; Yu, H.; Pajaujiene, S.; Shojaeian, N.-A.; Moviedo-Caro, M.A. How to HIIT while pregnant? The protocol characteristics and effects of high intensity interval training implemented during pregnancy—A systematic review. Balt. J. Health Phys. Act. 2022, 14, 16. [Google Scholar]
- Davis, P.J.; Singer, J.L.; Bonanno, G.A.; Schwartz, G.E. Repression and response bias during an affective memory recognition task. Aust. J. Psychol. 1988, 40, 147–157. [Google Scholar] [CrossRef]
- Li, J.; Zhou, F.L.; Huang, S.R.; Zhai, J.G.; Cai, W.Z. A survey of primipara and multiparous women’s cognition of exercise during pregnancy and their physical activity. Chin. Gen. Med. 2016, 19, 4. [Google Scholar]
- Zhang, Y.; Dong, S.; Zuo, J.; Hu, X.; Zhang, H.; Zhao, Y. Physical activity level of urban pregnant women in Tianjin, China: A cross-sectional study. PLoS ONE 2014, 9, e109624. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dimensions | Item Number | Items | Cronbach’s α |
|---|---|---|---|
| Perceived severity (Belief about how serious a condition and its sequelae are) | 1 | Prenatal physical inactivity is a severe problem. | 0.75 |
| 2 | Prenatal physical inactivity can lead to complications, such as obesity, gestational diabetes and gestational hypertension, preeclampsia, and urinary incontinence. | ||
| 3 | Prenatal physical inactivity can lead to anxiety and depression. | ||
| 4 | Prenatal physical inactivity can lead to post-term pregnancy and cesarean section. | ||
| Perceived susceptibility (Belief about the chances of experiencing a risk or acquiring a condition or disease) | 5 | Pregnant women do not engage in physical activity. | 0.91 |
| 6 | Fear of miscarriage can lead to prenatal physical inactivity. | ||
| 7 | Some habits can cause prenatal physical inactivity, including disinterest, indolence, and busyness. | ||
| 8 | Financial burdens, inadequate equipment, and lack of professional guidance can cause prenatal physical inactivity. | ||
| 9 | Recommendations from family members, doctors, and other pregnant women can cause prenatal physical inactivity. | ||
| Health motivation (Awareness of prevention of a risk, condition, or disease) | 10 | I usually value my health and fetal health. | 0.78 |
| 11 | I usually take the initiative to acquire prenatal physical activity knowledge. | ||
| Perceived benefits (Belief in the efficacy of the advised action to reduce the risk or seriousness of an impact) | 12 | Correct and reasonable prenatal physical activity are feasible. | 0.92 |
| 13 | I can prevent pregnancy complications, such as obesity, gestational diabetes and gestational hypertension, preeclampsia, and urinary incontinence, if I get enough prenatal physical activity. | ||
| 14 | I can regulate anxiety and depression if I get enough prenatal physical activity. | ||
| 15 | I can promote the health of the fetus if I get enough prenatal physical activity. | ||
| 16 | I can reduce adverse pregnancy outcomes if I get enough prenatal physical activity. | ||
| Perceived barriers (Belief about the tangible and psychological costs of the advised action) | 17 | It is difficult for me to participate in physical activity without being in good physical condition. | 0.85 |
| 18 | I am lazy and have no interest in pregnancy exercise. | ||
| 19 | It is hard for me to get involved in pregnancy exercise if I do not have enough money and belong to a professional maternity organization. | ||
| 20 | It is hard for me to get involved in prenatal physical activity without other people supporting me. | ||
| Cues to action (Strategies to activate readiness and promote awareness) | 21 | Prenatal physical activity information on TV commercials and publication propaganda impact me. | 0.80 |
| 22 | Prenatal physical activity experiences from family members and friends impact me. | ||
| 23 | Views of doctors and coaches on prenatal physical activity impact me. | ||
| Self-efficacy (Confidence in one’s ability to take action) | 24 | I am willing to participate in prenatal physical activity. | 0.81 |
| 25 | I can complete the assigned task while participating in prenatal physical activity. | ||
| 26 | I can make up my mind to correct my bad habits while participating in prenatal physical activity. | ||
| 27 | I can exercise independently during pregnancy. | ||
| Overall | 0.91 | ||
| Variable | N (%) |
|---|---|
| Chinese citizen | 414 (100%) |
| Age (years) | |
| 20–25 | 161 (38.9%) |
| 26–34 | 202 (48.9%) |
| 35+ | 51 (12.2%) |
| Body mass index | |
| Underweight | 41 (9.8%) |
| Normal weight | 289 (69.9%) |
| Overweight | 59 (14.2%) |
| Obese | 25 (6.1%) |
| Nationality | |
| Han | 259 (62.5%) |
| Minority | 155 (37.5%) |
| Annual revenue per capita | |
| Less than CNY 50,000 per year | 108 (26%) |
| CNY 50,001–100,000 per year | 104 (25%) |
| CNY 100,001–150,000 per year | 48 (11.5%) |
| More than CNY 150,000 per year | 128 (31.1%) |
| Unsure/would rather not say | 26 (6.4%) |
| Highest educational level | |
| No schooling or primary school | 4 (1%) |
| Secondary/high school | 59 (14.2%) |
| Technical or further educational institution | 84 (20.3%) |
| Bachelor’s degree | 208 (50.3%) |
| Master’s degree | 59 (14.2%) |
| Highest educational level (spouse) | |
| No schooling or primary school | 8 (2%) |
| Secondary/high school | 78 (18.9%) |
| Technical or further educational institution | 76 (18.3%) |
| Bachelor’s degree | 193 (46.6%) |
| Master’s degree | 59 (14.2%) |
| What is your current number of children? | |
| None | 244 (58.9%) |
| 1 child | 122 (29.5%) |
| 2 children | 45 (10.9%) |
| 3 or more children | 3 (0.7%) |
| Pregnancy for the first time | |
| Yes | 126 (42.6%) |
| No | 170 (57.4%) |
| Trimester of gestation | |
| First trimester | 99 (33.4%) |
| Second trimester | 96 (32.4%) |
| Third trimester | 101 (34.2%) |
| Residential zone | |
| Urban | 141 (34.1%) |
| Suburban | 133 (32.1%) |
| Rural | 140 (33.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, H.; He, J.; Szumilewicz, A. Pregnancy Activity Levels and Impediments in the Era of COVID-19 Based on the Health Belief Model: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 3283. https://doi.org/10.3390/ijerph19063283
Yu H, He J, Szumilewicz A. Pregnancy Activity Levels and Impediments in the Era of COVID-19 Based on the Health Belief Model: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(6):3283. https://doi.org/10.3390/ijerph19063283
Chicago/Turabian StyleYu, Hongli, Juan He, and Anna Szumilewicz. 2022. "Pregnancy Activity Levels and Impediments in the Era of COVID-19 Based on the Health Belief Model: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 6: 3283. https://doi.org/10.3390/ijerph19063283