
Changes in the Sexual Behavior of Partners in Each Trimester of Pregnancy in Otwock in Polish Couples

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. General Procedures
2.2. Participants
2.3. Recruitment Criteria
- for men: x/y/M
- for women: x/y/K
2.4. Collection Variables
2.5. The Self-Assessment of the Respondents Sexual Satisfaction Scale (SARSS) and Davies’ Sexual Satisfaction Scale (DSSS)
- Physical sexual satisfaction—relating to the assessment of the quality of sexual contact in a relationship, the sexual abilities of the partner, and the satisfaction of their own sexual needs in a relationship. The score obtained from the examined individual was in the range of 11 to 55;
- Emotional sexual satisfaction—measures the affective feelings towards sex and the partner’s behavior as well as the feelings towards their partner. The score obtained from the examined individual was in the range of 4 to 20;
- Control-related sexual satisfaction—relates to the assessment of their own influence over how, when and if at all the person has sexual contact. The score obtained from the examined individual was in the range of 6 to 30.
2.6. Statistical Analysis
2.7. Ethics
3. Results
3.1. Results of the Characteristics of Women, Men and Couples Participating in the Study
3.2. Evaluation of Relationship with the Current Partner and Assessment of Own and Partner’s Physical Attractiveness
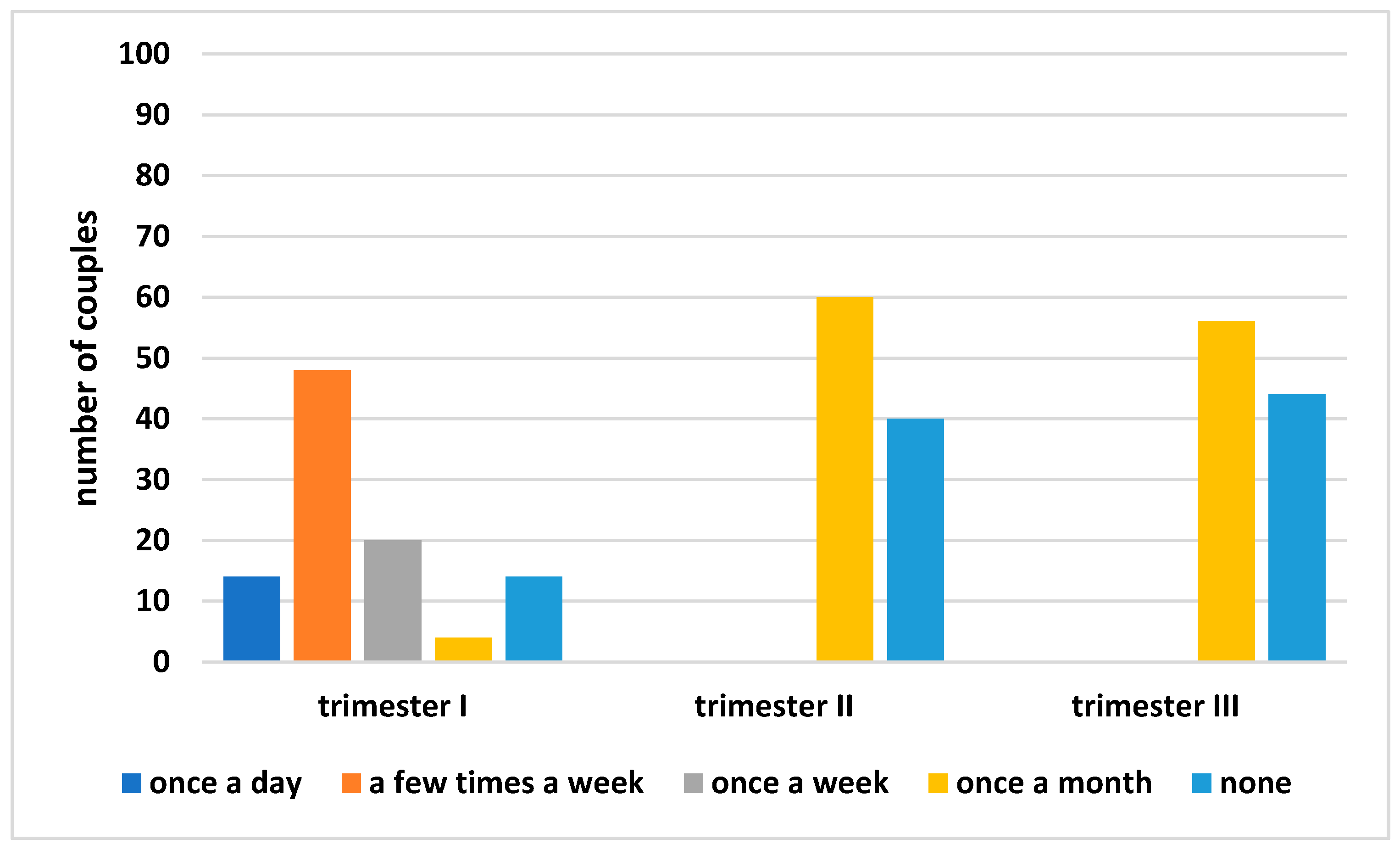
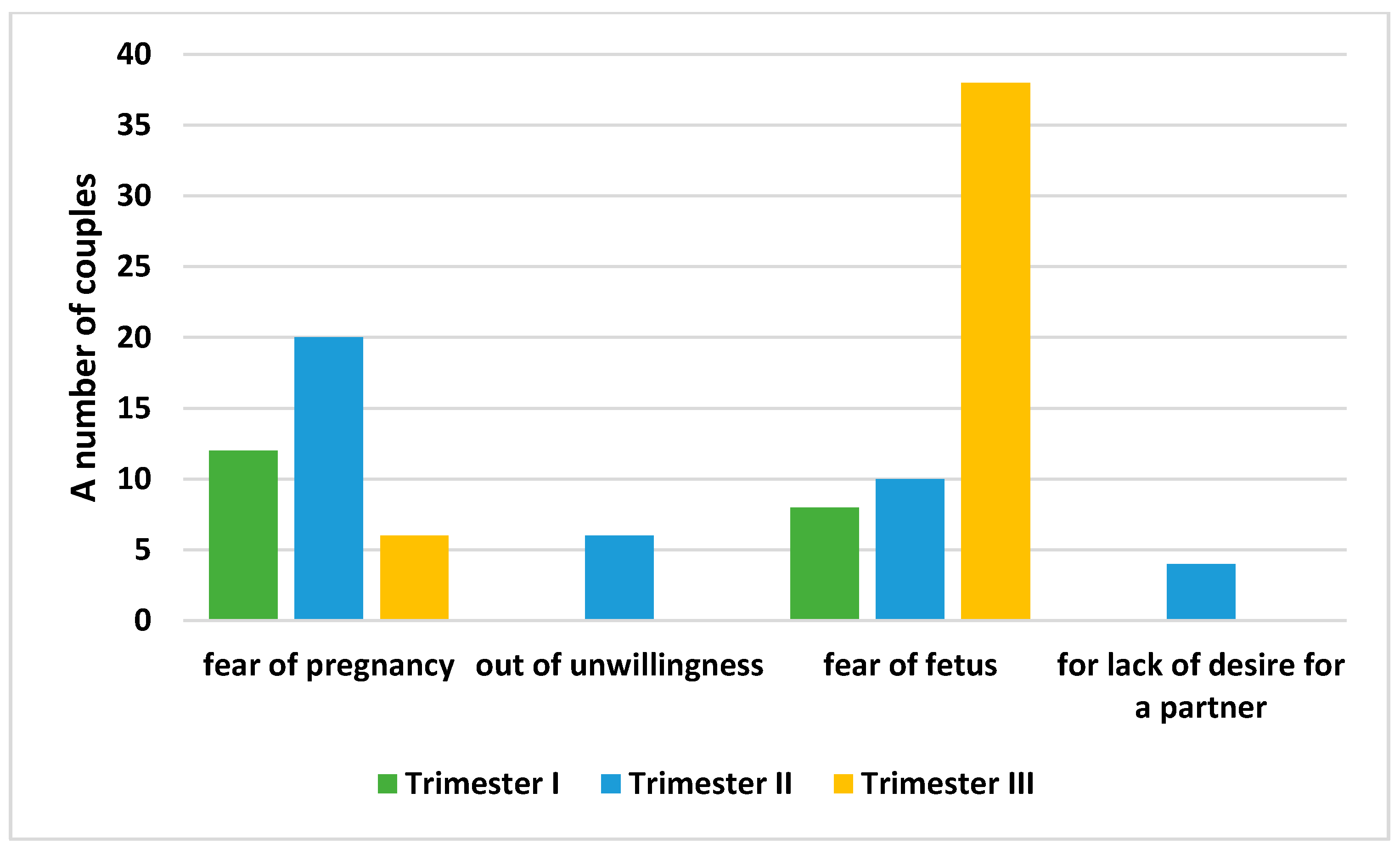
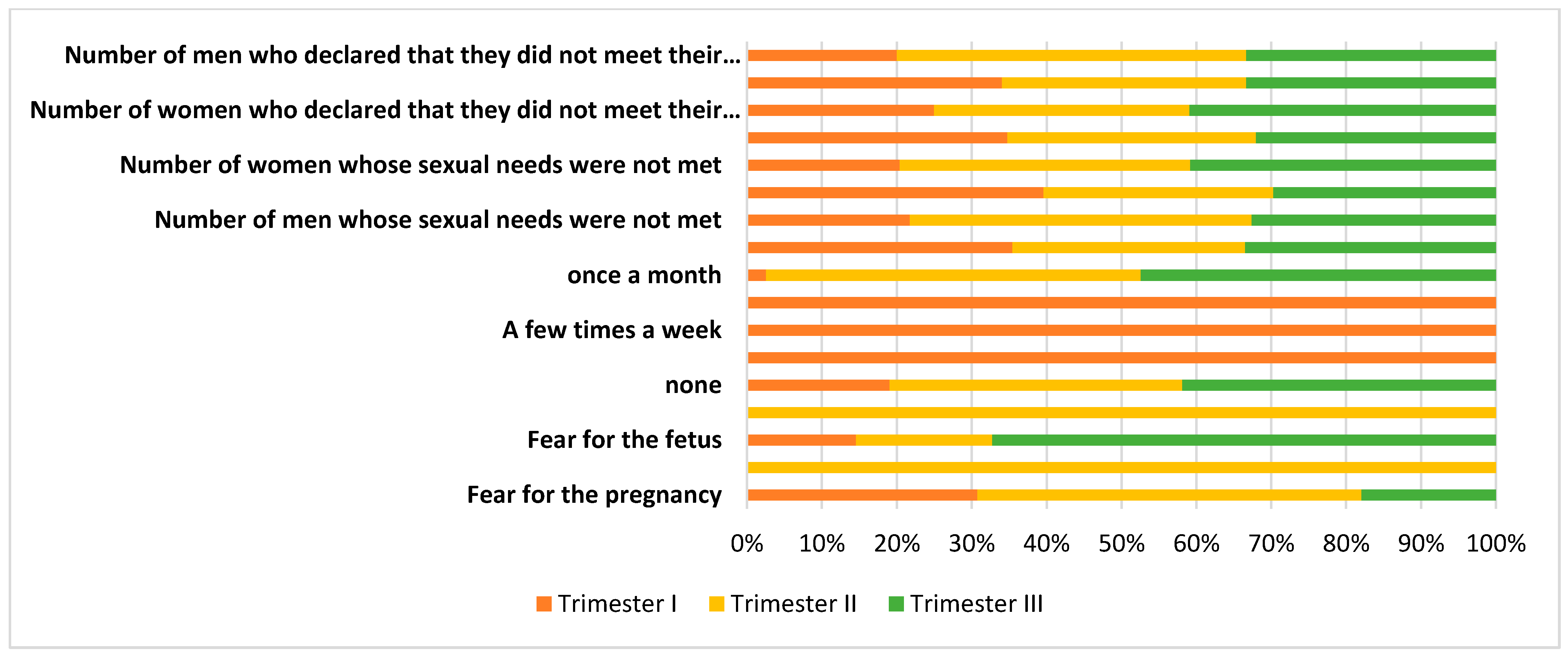
3.3. Characteristics of Partnerships and Sexual Activity during Pregnancy
3.4. The Results of Sexual Satisfaction of the Respondents during Pregnancy Based on Self-Assessment and the Davies’s Sexual Satisfaction Scale
3.5. Sources of Information about Sexual Contact during Pregnancy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Int. Sexual Health. 2019. Available online: https://www.who.int/health-topics/sexual-health (accessed on 5 November 2018).
- Rossi, M.A.; Impett, E.A.; Dawson, S.J.; Vannier, S.; Kim, J.; Rosen, N.O. A Longitudinal Investigation of Couples’ Sexual Growth and Destiny Beliefs in the Transition to Parenthood. Arch. Sex. Behav. 2022, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Sassine, D.; Ghulmiyyah, L.; Atallah, S.; Ghieh, D.; Saleh, N.; Slim, S.; Rameh, G. Sexual Changes during Pregnancy in a Middle-Eastern Population. Sex. Cult. 2020, 24, 1232–1251. [Google Scholar] [CrossRef]
- Aydin, M.; Cayonu, N.; Kadihasanoglu, M.; Irkilata, L.; Atilla, M.K.; Kendirci, M. Comparison of sexual functions in pregnant and non-pregnant women. Urol. J. 2015, 12, 2339–2344. [Google Scholar]
- Gałązka, I.; Drosdzol-Cop, A.; Naworska, B.; Czajkowska, M.; Skrzypulec-Plinta, V. Changes in the Sexual Function during Pregnancy. J. Sex. Med. 2015, 12, 445–454. [Google Scholar] [CrossRef]
- Yildiz, H. The relation between prepregnancy sexuality and sexual function during pregnancy and the postpartum period: A prospective study. J. Sex Marital Ther. 2015, 41, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Seven, M.; Akyuz, A.; Güngör, S. Predictors of sexual function during pregnancy. J. Obstet. Gynaecol. 2015, 35, 691–695. [Google Scholar] [CrossRef]
- Jawed-Wessel, S.; Sevick, E. The Impact of Pregnancy and Childbirth on Sexual Behaviors: A Systematic Review. J. Sex Res. 2017, 54, 411–423. [Google Scholar] [CrossRef]
- Łepecka–Klusek, C.; Syty, K.; Pilewska–Kozak, A.B.; Jakiel, G. Sense of own attractiveness among women in advanced pregnancy. Prog. Health Sci. 2015, 5, 7–13. [Google Scholar]
- Lew-Starowicz, Z.; Skrzypulec, V. (Eds.) Podstawy Seksuologii; PZWL: Warszawa, Poland, 2010. [Google Scholar]
- Fuchs, A.; Czech, I.; Sikora, J.; Fuchs, P.; Lorek, M.; Skrzypulec-Plinta, V.; Drosdzol-Cop, A. Sexual Functioning in Pregnant Women. Int. J. Environ. Res. Public Health 2019, 16, 4216. [Google Scholar] [CrossRef] [Green Version]
- Jawed-Wessel, S.; Santo, J.; Irwin, J. Sexual Activity and Attitudes as Predictors of Sexual Satisfaction during Pregnancy: A Multi-Level Model Describing the Sexuality of Couples in the First 12 Weeks. Arch. Sex. Behav. 2019, 48, 843–854. [Google Scholar] [CrossRef]
- Bartellas, E.; Crane, J.M.G.; Daley, M.; Bennett, K.A.; Hutchens, D. Sexuality and sexual activity in pregnancy. BJOG Int. J. Obstet. Gynaecol. 2000, 107, 964–968. [Google Scholar] [CrossRef] [PubMed]
- Anğın, A.D.; Özkaya, E.; Çetin, M.; Gün, I.; Sakin, O.; Ertekin, L.T.; Denizli, R.; Koyuncu, K.; Akalın, E.E. Comparison of female sexual function and sexual function of their partners between groups of pregnant and non-pregnant women. Ginekol. Pol. 2020, 91, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Fok, W.Y.; Chan, L.Y.S.; Yuen, P.M. Sexual behavior and activity in Chinese pregnant women. Acta Obstet. Gynecol. Scand. 2005, 84, 934–938. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, A.; Murkoff, H.; Hathaway, S. W Oczekiwaniu na Dziecko: Poradnik dla Przyszłych Matek i Ojców; Rebis, Dom Wydawniczy: Poznań, Poland, 2002. [Google Scholar]
- Erbil, N. Sexual function of pregnant women in the third trimester. Alex. J. Med. 2018, 54, 139–142. [Google Scholar] [CrossRef] [Green Version]
- Ilska, M.; Przybyła-Basista, H.; Ilski, A.; Cnota, W. Aktywność i Satysfakcja Seksualna Kobiet w Ciąży Prawidłowej Oraz Wysokiego Ryzyka. Ginekol. Poloz. 2018, 2, 34–41. [Google Scholar]
- Sayle, A.E.; Savitz, D.A.; Thorp, J.M.; Hertz-Picciotto, I.; Wilcox, A.J. Sexual activity during late pregnancy and risk of preterm delivery. Obstet. Gynecol. 2001, 97, 283–289. [Google Scholar] [CrossRef]
- Maroufizadeh, S.; Hosseini, M.; Foroushani, A.R.; Omani-Samani, R.; Amini, P. Application of the dyadic data analysis in behavioral medicine research: Marital satisfaction and anxiety in infertile couples. BMC Med. Res. Methodol. 2018, 18, 117. [Google Scholar] [CrossRef]
- Kenny, D.A.; Kashy, D.A.; Cook, W.L. Dyadic Data Analysis; Guilford Press: New York, NY, USA, 2020. [Google Scholar]
- Ramsdell, E.L.; Franz, M.; Brock, R.L. A Multifaceted and Dyadic Examination of Intimate Relationship Quality during Pregnancy: Implications for Global Relationship Satisfaction. Fam. Process 2020, 59, 556–570. [Google Scholar] [CrossRef]
- Molgora, S.; Acquati, C.; Fenaroli, V.; Saita, E. Dyadic coping and marital adjustment during pregnancy: A cross-sectional study of Italian couples expecting their first child. Int. J. Psychol. 2019, 54, 277–285. [Google Scholar] [CrossRef]
- Forsberg, H.; Eliason, M.J. Healthcare providers’ pregnancy prevention counseling of trans and non-binary assigned female at birth (TNB/AFAB) patients. J. Homosex. 2022, 69, 356–383. [Google Scholar] [CrossRef]
- Bonnington, A.; Dianat, S.; Kerns, J.; Hastings, J.; Hawkins, M.; De Haan, G.; Obedin-Maliver, J. Society of Family Planning clinical recommendations: Contraceptive counseling for transgender and gender diverse people who were female sex assigned at birth. Contraception 2020, 102, 70–82. [Google Scholar] [CrossRef] [PubMed]
- Moseson, H.; Fix, L.; Hastings, J.; Stoeffler, A.; Lunn, M.R.; Flentje, A.; Lubensky, M.E.; Capriotti, M.R.; Ragosta, S.; Forsberg, H.; et al. Pregnancy intentions and outcomes among transgender, nonbinary, and gender-expansive people assigned female or intersex at birth in the United States: Results from a national, quantitative survey. Int. J. Transgender Health 2020, 22, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Naukowiec.org. Available online: https://www.naukowiec.org/dobor.html (accessed on 10 October 2017).
- Obrochta, C.A.; Chambers, C.; Bandoli, G. Psychological distress in pregnancy and postpartum. Women Birth 2020, 33, 583–591. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, E.T.; Kolbuszewska, M.T.; Dawson, S.J. Perinatal Sexual Dysfunction: The Importance of the Interpersonal Context. Curr. Sex. Health Rep. 2021, 13, 55–65. [Google Scholar] [CrossRef]
- Lorenz, T.K.; Ramsdell, E.L.; Brock, R.L. Communication changes the effects of sexual pain on sexual frequency in the pregnancy to postpartum transition. J. Psychosom. Obstet. Gynecol. 2020, 2020, 1–8. [Google Scholar] [CrossRef]
- Carpenter, E.; Everett, B.G.; Greene, M.Z.; Haider, S.; Hendrick, C.E.; Higgins, J.A. Pregnancy (im) possibilities: Identifying factors that influence sexual minority women’s pregnancy desires. Soc. Work Health Care 2020, 59, 180–198. [Google Scholar] [CrossRef]
- Masters, W.H.; Johnson, V.E. Human Sexual Response Little; Brown: Boston, MA, USA, 1966. [Google Scholar]
- Kyndely, K. The Sexuality of Women in Pregnancy and Postpartum: A Review. Med. Asp. Hum. Sex 1978, 7, 28–32. [Google Scholar] [CrossRef]
- Imieliński, K.; Imieliński, C. Sexual problems among women during pregnancy. In Sexologists from Criminal Law to the Gynecology; Imieliński, K., Ed.; Polska Akademia Wiedzy Seksuologicznej: Warszawa, Poland, 1997; pp. 211–214. [Google Scholar]
- Kremska, A.; Wróbel, R.; Kołodziej, B.; Barnaś, E. Zachowania seksualne kobiet w ciąży. In Przegląd Medyczny Uniwersytetu Rzeszowskiego i Narodowego Instytutu Leków w Warszawie; Wydawnictwo Uniwersytetu Rzeszowskiego: Rzeszów, Poland, 2013; Volume 5, pp. 75–85. [Google Scholar]
- Anzaku, S.A.; Ogbe, E.A.; Ogbu, G.I.; Edem, B.E.; Ngwan, S.D. Evaluation of changes in sexual response and factors influencing sexuality during pregnancy among Nigerian women in Jos, Nigeria. Int. J. Reprod. Contracept. Obstet. Gynecol. 2016, 5, 3576–3582. [Google Scholar] [CrossRef] [Green Version]
- Yarhouse, M.A.; Morgan, T.; Anthony, K.; Sadusky, J. Celibate gay Christians: Sexual identity and religious beliefs and practices. J. Pastor. Care Couns. 2017, 71, 52–59. [Google Scholar] [CrossRef]
- Perry, S.L.; Whitehead, A.L. Only bad for believers? Religion, pornography use, and sexual satisfaction among American men. J. Sex Res. 2019, 56, 50–61. [Google Scholar] [CrossRef]
- Jung, P. Sexual pleasure: A Roman Catholic perspective on women’s delight. Theol. Sex. 2000, 2000, 26–47. [Google Scholar] [CrossRef]
- Staruch, M.; Kucharczyk, A.; Zawadzka, K.; Wielgos, M.; Szymusik, I. Sexual activity during pregnancy. Neuroendocrinol. Lett. 2016, 37, 53–58. [Google Scholar] [PubMed]
- Ribeiro, M.C.; de Tubino Scanavino, M.; do Amaral, M.L.S.A.; de Moraes Horta, A.L.; Torloni, M.R. Beliefs about sexual activity during pregnancy: A systematic review of the literature. J. Sex Marital Ther. 2017, 43, 822–832. [Google Scholar] [CrossRef]
- Lew-Starowicz, Z.; Skrzypulec-Plinta, V. Seksualność Kobiet w Okresie Ciąży i Połogu. In Seksuologia; Lew-Starowicz, M., Lew-Starowicz, Z., Skrzypulec-Plinta, V., Eds.; PZWL: Warszawa, Poland, 2017; pp. 147–154. [Google Scholar]
- Skrzypulec, V.; Wit, M.; Kowalczyk, R.; Jabłoński, K.; Drosdzol, A. Jakość życia seksualnego w okresie ciąży. Ann. Acad. Med. Siles. 2005, 59, 373–376. [Google Scholar]
- Malarewicz, A.; Szymkiewicz, J.; Rogala, J. Sexuality of pregnant women. Ginekol. Pol. 2006, 77, 736–737. [Google Scholar]
- Khalesi, Z.B.; Bokaie, M.; Attari, S.M. Effect of pregnancy on sexual function of couples. Afr. Health Sci. 2018, 18, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Yang, X.; Fan, X.; Sun, Y.; Tan, C.; Wang, Y.; Zhu, W.; Ren, D. Decreased Sexual Desire among Middle-Aged and Old Women in China and Factors Influencing It: A Questionnaire-Based Study. Evid. Based Complementary Altern. Med. 2021, 2021, 6649242. [Google Scholar] [CrossRef]
- Chang, S.R.; Chen, K.H.; Lin, H.H.; Yu, H.J. Comparison of overall sexual function, sexual intercourse/activity, sexual satisfaction, and sexual desire during the three trimesters of pregnancy and assessment of their determinants. J. Sex. Med. 2011, 8, 2859–2867. [Google Scholar] [CrossRef]
- Hanafy, S.; Srour, N.E.; Mostafa, T. Female sexual dysfunction across the three pregnancy trimesters: An Egyptian study. Sex Health 2014, 11, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Makara-Studzińska, M.; Plewik, I.; Kryś, K.M. Sexual activity of women in different trimesters of pregnancy. EJMT 2015, 2, 1–9. [Google Scholar]
- Sipiński, A.; Kazimierczak, M.; Buchacz, P.; Sipińska, K. Zachowania seksualne kobiet ciężarnych. Wiad. Lek. 2004, 57, 281–284. [Google Scholar] [PubMed]
- Jiang, M.; Yan, G.; Deng, H.; Liang, H.; Lin, Y.; Zhang, X. The efficacy of regular penis-root masturbation, versus Kegel exercise in the treatment of primary premature ejaculation: A quasi-randomised controlled trial. Andrologia 2020, 52, e13473. [Google Scholar] [CrossRef] [PubMed]
- Grinde, B. Sexual Behavior in Modern Societies: An Interdisciplinary Analysis. Sex Cult. 2021, 25, 2075–2091. [Google Scholar] [CrossRef]
- Rowland, D.; Donarski, A.; Graves, V.; Caldwell, C.; Hevesi, B.; Hevesi, K. The experience of orgasmic pleasure during partnered and masturbatory sex in women with and without orgasmic difficulty. J. Sex Marital Ther. 2019, 45, 550–561. [Google Scholar] [CrossRef]
- Bowman, C.P. Masturbation. In The SAGE Encyclopedia of Psychology and Gender; Nadal, L.L., Ed.; SAGE Publishing Inc.: Thousand Oaks, CA, USA, 2017; pp. 1123–1124. [Google Scholar]
- Papp, L.J.; Hagerman, C.; Gnoleba, M.A.; Erchull, M.J.; Liss, M.; Miles-McLean, H. Exploring perceptions of slut-shaming on Facebook: Evidence for a reverse sexual double standard. Gend. Issues 2015, 32, 57–76. [Google Scholar] [CrossRef]
- Herdt, G. The Sambia: Ritual, Sexuality, and Change in Papua New Guinea; Cengage Learning: Belmont, CA, USA, 2005. [Google Scholar]
- Haus, K.R.; Thompson, A.E. An examination of the sexual double standard pertaining to masturbation and the impact of assumed motives. Sex Cult. 2020, 24, 809–834. [Google Scholar] [CrossRef]
- Baranowski, M. Katechizm Kościoła Katolickiego. 1994. Available online: http://www.katechizm.opoka.org.pl/ (accessed on 26 August 2021).
- Burton, N. For Better for Worse: Should I Get Married? Acheron Press: Exeter, UK, 2017. [Google Scholar]
- Ma, G.C.; Zou, Z.J.; Lai, Y.F.; Zhang, X.; Zhang, Y. Regular penis-root masturbation, a novel behavioral therapy in the treatment of primary premature ejaculation. Asian J. Androl. 2019, 21, 631. [Google Scholar] [PubMed]
- Farhan, R.; Yousuf, R.; Hussain, S.N.F.; Khan, M.; Bilal, Z.; Khan, M.; Khan, S.A. Sexual Knowledge in Post-Myocardial Infarction Patients: A Cross-Sectional Study. Cureus 2020, 12, e8480. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Consent to participate in the study | Cack of consent for participation in the study |
| Heterosexual couple with a single physiological pregnancy | complicated pregnancy (at risk of preterm labor, diabetes, arterial hypertension, placenta previa, cervical insufficiency, in vitro pregnancy) |
| Treatment or diagnosis of infertility | |
| First-time pregnancy, diagnosed during the first trimester of pregnancy (up to the 12th week) | Treatment of diagnosis of sexual dysfunction |
| Regular gynecological visits during pregnancy, in line with the plan of care for the pregnant woman | Incorrectly completed or incomprehensible questionnaires |
| Correct completion of the set of research questionnaires by people in certain pregnancy trimesters. | Significant gaps in the responses to the questionnaires |
| Insufficient knowledge of the Polish language in speech and writing |
| Parameter | Women | Men | p-Value | |
|---|---|---|---|---|
| Place of residence | Village | 14 | 4 | p = 0.25 |
| Urban < 100,000 citizens | 68 | 86 | p = 0.19 | |
| Urban > 100,000 citizens | 18 | 10 | p = 0.43 | |
| Education | Vocational education | 8 | 8 | p = 1.0 |
| Secondary education | 16 | 32 | p = 0.10 | |
| Higher education | 76 | 60 | p = 0.16 | |
| Occupation | Blue-collar worker | 14 | 54 | p = 0.27 |
| White-collar worker | 76 | 40 | p = 0.52 | |
| Unemployment | 10 | 6 | p = 0.85 | |
| Relationship status | Marriage | 66 | 66 | p = 1.0 |
| Partnership | 34 | 34 | p = 1.0 | |
| Duration of relationship (years) | 3.22 ± 0.23 | 3.80 ± 0.14 | p = 0.02 | |
| Factor | Women | Men | p-Value |
|---|---|---|---|
| Assessment of the relationship | 8.64 ± 0.18 | 8.84 ± 0.21 | p = 0.92 |
| Assessment of own physical attractiveness | 4.88 ± 1.37 | 7.2 ± 0.14 | p = 0.00 * |
| Assessment of partner’s physical attractiveness | 8.7 ± 0.16 | 9.4 ± 0.11 | p = 0.76 |
| First Trimester | Second Trimester | Third Semester | p-Value of the Post Hoc Tukey Test | ||||
|---|---|---|---|---|---|---|---|
| * p = 0.00 | * p = 0.00 | * p = 0.00 | |||||
| Frequency | Women (n = 28) | Men (n = 76) | Women (n = 8) | Men (n = 100) | Women (n = 8) | Men (n = 100) | |
| 1 | 0 | 20 | 0 | 4 | 0 | 8 | p = 0.00 a,b |
| 2 | 0 | 30 | 0 | 40 | 0 | 32 | p = 0.00 a,b |
| 3 | 0 | 26 | 0 | 56 | 0 | 60 | p = 0.00 a,b |
| 4 | 28 | 0 | 2 | 0 | 2 | 0 | p = 0.00 a,b |
| First Trimester | Second Trimester | Third Semester | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Women (n = 100) | Men (n = 100) | Women (n = 100) | Men (n = 100) | Women (n = 100) | Men (n = 100) | ||
| Self-esteem | 7.24 | 8.82 | 5.88 | 8.78 | 5.78 | 8.58 | p = 0.05 * p = 0.99 ** |
| Sexual satisfaction scale | 71.02 ± 10.66 | 73.20 ± 10.72 | 64.28 ± 8.39 | 72.64 ± 12.15 | 63.08 ± 10.55 | 72.18 ± 10.55 | p = 0.00 * p = 0.00 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kulhawik, R.; Zborowska, K.; Grabarek, B.O.; Boroń, D.; Skrzypulec-Plinta, V.; Drosdzol-Cop, A. Changes in the Sexual Behavior of Partners in Each Trimester of Pregnancy in Otwock in Polish Couples. Int. J. Environ. Res. Public Health 2022, 19, 2921. https://doi.org/10.3390/ijerph19052921
Kulhawik R, Zborowska K, Grabarek BO, Boroń D, Skrzypulec-Plinta V, Drosdzol-Cop A. Changes in the Sexual Behavior of Partners in Each Trimester of Pregnancy in Otwock in Polish Couples. International Journal of Environmental Research and Public Health. 2022; 19(5):2921. https://doi.org/10.3390/ijerph19052921
Chicago/Turabian StyleKulhawik, Robert, Katarzyna Zborowska, Beniamin Oskar Grabarek, Dariusz Boroń, Violetta Skrzypulec-Plinta, and Agnieszka Drosdzol-Cop. 2022. "Changes in the Sexual Behavior of Partners in Each Trimester of Pregnancy in Otwock in Polish Couples" International Journal of Environmental Research and Public Health 19, no. 5: 2921. https://doi.org/10.3390/ijerph19052921