
Validation of the English Version of the General Dietary Behavior Inventory (GDBI-E)

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Development of the General Dietary Behavior Inventory in the English Language
2.2. Participants and Study Design
2.3. Study Variables
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics of the GDBI-E
3.2. Sample Description and Descriptive Statistics
3.3. Inferential Statistical Analyses of GDBI-E Score and Sociodemographic Variables
3.4. Construct and Criterion Validation: GDBI-E Score Intercorrelations
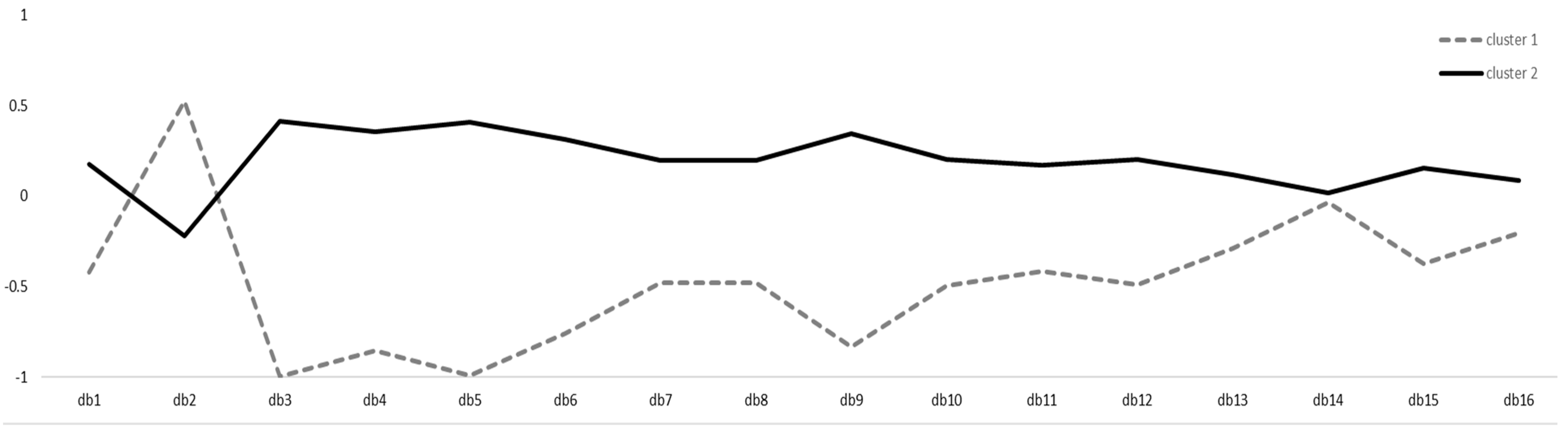
3.5. Construct and Criterion Validation: Cluster Analysis and Cluster Assignment Intercorrelations
4. Discussion
4.1. Limitations
4.2. Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clancy, F.; Prestwich, A.; Caperon, L.; O’Connor, D.B. Perseverative Cognition and Health Behaviors: A Systematic Review and Meta-Analysis. Front. Hum. Neurosci. 2016, 10, 534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheeran, P.; Maki, A.; Montanaro, E.; Avishai-Yitshak, A.; Bryan, A.; Klein, W.M.; Miles, E.; Rothman, A.J. The Impact of Changing Attitudes, Norms, and Self-Efficacy on Health-Related Intentions and Behavior: A Meta-Analysis. Health Psychol. 2016, 35, 1178. [Google Scholar] [CrossRef] [PubMed]
- White, R.L.; Babic, M.J.; Parker, P.D.; Lubans, D.R.; Astell-Burt, T.; Lonsdale, C. Domain-Specific Physical Activity and Mental Health: A Meta-Analysis. Am. J. Prev. Med. 2017, 52, 653–666. [Google Scholar] [CrossRef] [PubMed]
- Lake, A.A.; Hyland, R.M.; Rugg-Gunn, A.J.; Wood, C.E.; Mathers, J.C.; Adamson, A.J. Healthy Eating: Perceptions and Practice (the ASH30 Study). Appetite 2007, 48, 176–182. [Google Scholar] [CrossRef]
- Marijn Stok, F.; Renner, B.; Allan, J.; Boeing, H.; Ensenauer, R.; Issanchou, S.; Kiesswetter, E.; Lien, N.; Mazzocchi, M.; Monsivais, P. Dietary Behavior: An Interdisciplinary Conceptual Analysis and Taxonomy. Front. Psychol. 2018, 9, 1689. [Google Scholar] [CrossRef] [Green Version]
- Leonhäuser, I.-U.; Meier-Gräwe, U.; Möser, A.; Zander, U.; Köhler, J. Essalltag in Familien; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2009; ISBN 978-3-531-16053-5. [Google Scholar]
- Engelmann, G.; Marsall, M.; Skoda, E.-M.; Knoll-Pientka, N.; Bäuerle, L.; Stroebele-Benschop, N.; Teufel, M.; Bäuerle, A. Development and Validation of the General Dietary Behavior Inventory (GDBI) in Scope of International Nutrition Guidelines. Nutrients 2021, 13, 1328. [Google Scholar] [CrossRef]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and Validation of a Food Frequency Questionnaire in Spain. Int. J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef]
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and Validity of a Semiquantitative Food Frequency Questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef]
- Arbit, N.; Ruby, M.; Rozin, P. Development and Validation of the Meaning of Food in Life Questionnaire (MFLQ): Evidence for a New Construct to Explain Eating Behavior. Food Qual. Prefer. 2017, 59, 35–45. [Google Scholar] [CrossRef]
- Van Strien, T.; Frijters, J.E.; Van Staveren, W.A.; Defares, P.B.; Deurenberg, P. The Predictive Validity of the Dutch Restrained Eating Scale. Int. J. Eat. Disord. 1986, 5, 747–755. [Google Scholar] [CrossRef]
- Blomquist, K.K.; Roberto, C.A.; Barnes, R.D.; White, M.A.; Masheb, R.M.; Grilo, C.M. Development and Validation of the Eating Loss of Control Scale. Psychol. Assess. 2014, 26, 77–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luce, K.H.; Crowther, J.H. The Reliability of the Eating Disorder Examination—Self-report Questionnaire Version (EDE-Q). Int. J. Eat. Disord. 1999, 25, 349–351. [Google Scholar] [CrossRef]
- Guenther, P.M.; Casavale, K.O.; Reedy, J.; Kirkpatrick, S.I.; Hiza, H.A.B.; Kuczynski, K.J.; Kahle, L.L.; Krebs-Smith, S.M. Update of the Healthy Eating Index: HEI-2010. J. Acad. Nutr. Diet. 2013, 113, 569–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [Green Version]
- Joint FAO/WHO Consultation. Preparation and Use of Food-Based Dietary Guidelines; WHO Technical Report Series 880; World Health Organization: Geneva, Switzerland, 1998; ISBN 9241208805. [Google Scholar]
- World Health Organization. Healthy Diet—Fact Sheet No. 394. Available online: https://www.who.int/en/news-room/fact-sheets/detail/healthy-diet (accessed on 10 November 2020).
- German Nutrition Society. 10 Guidelines of the German Nutrition Society (DGE) for a Wholesome Diet. Available online: https://www.dge.de/ernaehrungspraxis/vollwertige-ernaehrung/10-regeln-der-dge/en/ (accessed on 10 January 2022).
- Hauner, H.; Bechthold, A.; Boeing, H.; Brönstrup, A.; Buyken, A.; Leschik-Bonnet, E.; Linseisen, J.; Schulze, M.; Strohm, D.; Wolfram, G. Evidence-Based Guideline of the German Nutrition Society: Carbohydrate Intake and Prevention of Nutrition-Related Diseases. Ann. Nutr. Metab. 2012, 60 (Suppl. S1), 1–58. [Google Scholar] [CrossRef]
- Wolfram, G.; Bechthold, A.; Boeing, H.; Ellinger, S.; Hauner, H.; Kroke, A.; Leschik-Bonnet, E.; Linseisen, J.; Lorkowski, S.; Schulze, M.; et al. Evidence-Based Guideline of the German Nutrition Society: Fat Intake and Prevention of Selected Nutrition-Related Diseases. Ann. Nutr. Metab. 2015, 67, 141–204. [Google Scholar] [CrossRef] [PubMed]
- Osgood, C.E. The Nature and Measurement of Meaning. Psychol. Bull. 1952, 49, 197–237. [Google Scholar] [CrossRef] [Green Version]
- Campbell, D.T.; Fiske, D.W. Convergent and Discriminant Validation by the Multitrait-Multimethod Matrix. Psychol. Bull. 1959, 56, 81–105. [Google Scholar] [CrossRef] [Green Version]
- Carlson, K.D.; Herdman, A.O. Understanding the Impact of Convergent Validity on Research Results. Organ. Res. Methods 2012, 15, 17–32. [Google Scholar] [CrossRef]
- Aggarwal, A.; Monsivais, P.; Cook, A.J.; Drewnowski, A. Positive Attitude toward Healthy Eating Predicts Higher Diet Quality at All Cost Levels of Supermarkets. J. Acad. Nutr. Diet. 2014, 114, 266–272. [Google Scholar] [CrossRef] [Green Version]
- Dickson-Spillmann, M.; Siegrist, M.; Keller, C. Development and Validation of a Short, Consumer-Oriented Nutrition Knowledge Questionnaire. Appetite 2011, 56, 617–620. [Google Scholar] [CrossRef]
- Breyer, B. Social Trust Scale (ESS). In ZIS—The Collection Items and Scales for the Social Sciences; GESIS Leibniz Institute for the Social Sciences: Mannheim, Germany, 2015. [Google Scholar] [CrossRef]
- Lipkus, I. The Construction and Preliminary Validation of a Global Belief in a Just World Scale and the Exploratory Analysis of the Multidimensional Belief in a Just World Scale. Personal. Individ. Differ. 1991, 12, 1171–1178. [Google Scholar] [CrossRef]
- Cheung, F.; Lucas, R.E. Assessing the Validity of Single-Item Life Satisfaction Measures: Results from Three Large Samples. Qual. Life Res. 2014, 23, 2809–2818. [Google Scholar] [CrossRef] [Green Version]
- Milton, K.; Bull, F.C.; Bauman, A. Reliability and Validity Testing of a Single-Item Physical Activity Measure. Br. J. Sports Med. 2011, 45, 203–208. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- RStudio Team. RStudio: Integrated Development for R; RStudio, PBC: Boston, MA, USA, 2020. [Google Scholar]
- Revelle, W. Psych: Procedures for Psychological, Psychometric, and Personality Research; Northwestern University: Evanston, IL, USA, 2021. [Google Scholar]
- Lüdecke, D. SjPlot: Data Visualization for Statistics in Social Science. Available online: https://CRAN.R-project.org/package=sjPlot (accessed on 10 January 2022).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis, Use R! 2nd ed.; Springer: Cham, Switzerland, 2016; ISBN 978-3-319-24277-4. [Google Scholar]
- Wickham, H.; François, R.; Henry, L.; Müller, K.; RStudio. Dplyr: A Grammar of Data Manipulation; RStudio, PBC: Boston, MA, USA, 2021. [Google Scholar]
- Fox, J.; Weisberg, S. An R Companion to Applied Regression, 3rd ed.; SAGE: Los Angeles, CA, USA, 2019; ISBN 978-1-5443-3647-3. [Google Scholar]
- Kassambara, A.; Mundt, F. Factoextra: Extract and Visualize the Results of Multivariate Data Analyses. Available online: https://CRAN.R-project.org/package=factoextra (accessed on 10 January 2022).
- Maechler, M.; Rousseeuw, P.; Struyf, A.; Hubert, M.; Hornik, K.; Studer, M.; Roudier, P.; Gonzalez, J.; Kozlowski, K.; Schubert, E.; et al. Finding Groups in Data: Cluster Analysis Extended Rousseeuw et al. Available online: https://CRAN.R-project.org/package=cluster (accessed on 10 January 2022).
- Harrell, F.E., Jr. Hmisc: Harrell Miscellaneous. Available online: https://cran.r-project.org/package=Hmisc (accessed on 10 January 2022).
- R Core Team. Foreign: Read Data Stored by “Minitab”, “S”, “SAS”, “SPSS”, “Stata”, “Systat”, “Weka”, “DBase”. Available online: https://CRAN.R-project.org/package=foreign (accessed on 10 January 2022).
- Kodinariya, T.M.; Makwana, P.R. Review on Determining Number of Cluster in K-Means Clustering. Int. J. Adv. Res. Comput. Sci. Manag. Stud. 2013, 1, 90–95. [Google Scholar]
- Rousseeuw, P.J. Silhouettes: A Graphical Aid to the Interpretation and Validation of Cluster Analysis. J. Comput. Appl. Math. 1987, 20, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Ansell, E.B.; Grilo, C.M.; White, M.A. Examining the Interpersonal Model of Binge Eating and Loss of Control over Eating in Women. Int. J. Eat. Disord. 2012, 45, 43–50. [Google Scholar] [CrossRef] [Green Version]
- Ivanova, I.V.; Tasca, G.A.; Proulx, G.; Bissada, H. Does the Interpersonal Model Apply across Eating Disorder Diagnostic Groups? A Structural Equation Modeling Approach. Compr. Psychiatry 2015, 63, 80–87. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Baumeister, R.F. Binge Eating as Escape from Self-Awareness. Psychol. Bull. 1991, 110, 86. [Google Scholar] [CrossRef]
- Polivy, J.; Herman, C.P. Causes of Eating Disorders. Annu. Rev. Psychol. 2002, 53, 187–213. [Google Scholar] [CrossRef] [Green Version]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; SAGE Publications Ltd.: Los Angeles, CA, USA, 2013; ISBN 1-4462-4918-2. [Google Scholar]
- Mazzocchi, M.; Brasili, C.; Sandri, E. Trends in Dietary Patterns and Compliance with World Health Organization Recommendations: A Cross-Country Analysis. Public Health Nutr. 2008, 11, 535–540. [Google Scholar] [CrossRef] [Green Version]
- Fresán, U.; Sabaté, J. Vegetarian Diets: Planetary Health and Its Alignment with Human Health. Adv. Nutr. 2019, 10, S380–S388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cacau, L.T.; De Carli, E.; de Carvalho, A.M.; Lotufo, P.A.; Moreno, L.A.; Bensenor, I.M.; Marchioni, D.M. Development and Validation of an Index Based on EAT-Lancet Recommendations: The Planetary Health Diet Index. Nutrients 2021, 13, 1698. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Garnett, T.; Tilman, D.; Wood, A.; DeClerck, F.; Jonell, M.; et al. Food in the Anthropocene: The EAT–Lancet Commission on Healthy Diets from Sustainable Food Systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Cacau, L.T.; Benseñor, I.M.; Goulart, A.C.; Cardoso, L.O.; Lotufo, P.A.; Moreno, L.A.; Marchioni, D.M. Adherence to the Planetary Health Diet Index and Obesity Indicators in the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Nutrients 2021, 13, 3691. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F. Eating Habits and Lifestyle Changes during COVID-19 Lockdown: An Italian Survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Gardner, M.P.; Wansink, B.; Kim, J.; Park, S.-B. Better Moods for Better Eating?: How Mood Influences Food Choice. J. Consum. Psychol. 2014, 24, 320–335. [Google Scholar] [CrossRef]
- Martin, C.K.; Rosenbaum, D.; Han, H.; Geiselman, P.J.; Wyatt, H.R.; Hill, J.O.; Brill, C.; Bailer, B.; Miller-III, B.V.; Stein, R.; et al. Change in Food Cravings, Food Preferences, and Appetite during a Low-Carbohydrate and Low-Fat Diet. Obesity 2011, 19, 1963–1970. [Google Scholar] [CrossRef] [Green Version]
- Stevens, J.; McClain, J.E.; Truesdale, K.P. Selection of Measures in Epidemiologic Studies of the Consequences of Obesity. Int. J. Obes. 2008, 32, S60–S66. [Google Scholar] [CrossRef] [Green Version]
- Dobbelsteyn, C.; Joffres, M.; MacLean, D.; Flowerdew, G.; The Canadian Heart Health Surveys Research Group. A Comparative Evaluation of Waist Circumference, Waist-to-Hip Ratio and Body Mass Index as Indicators of Cardiovascular Risk Factors. The Canadian Heart Health Surveys. Int. J. Obes. 2001, 25, 652–661. [Google Scholar] [CrossRef] [Green Version]
- Brug, J.; van der Ploeg, H.P.; Loyen, A.; Ahrens, W.; Allais, O.; Andersen, L.F.; Cardon, G.; Capranica, L.; Chastin, S.; De Bourdeaudhuij, I. Determinants of Diet and Physical Activity (DEDIPAC): A Summary of Findings. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feskens, E.J.M.; Frewer, L.J.; Gregory, P.; Grusak, M.; Parnell, W.; Scholten, M.C.T.; Wenink, J.; McKhann, H.; Byrne, P.; Gøtke, N. FACCE JPI-JPI HDHL Priority Joint Actions to Contribute to the European Strategy on Food and Nutrition Security: Outcomes of the Grand Debate Nutrition Security—A Whole System Approach. Available online: https://edepot.wur.nl/407464 (accessed on 10 January 2022).
- Müller, M.J. From BMI to Functional Body Composition. Eur. J. Clin. Nutr. 2013, 67, 1119–1121. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Item | Mean | SD | Skew | Response Distribution | ||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | ||||
| db1 | 3.48 | 1.19 | −0.30 | 3% | 25% | 14% | 35% | 22% |
| db2 | 2.68 | 1.61 | 0.29 | 38% | 16% | 9% | 17% | 21% |
| db3 | 4.43 | 0.97 | −1.77 | 2% | 6% | 6% | 19% | 67% |
| db4 | 3.99 | 1.08 | −0.80 | 2% | 11% | 17% | 29% | 42% |
| db5 | 4.20 | 0.91 | −1.08 | 1% | 5% | 13% | 35% | 46% |
| db6 | 3.41 | 1.26 | −0.32 | 8% | 17% | 24% | 26% | 24% |
| db7 | 3.93 | 1.21 | −0.91 | 6% | 8% | 20% | 22% | 45% |
| db8 | 2.74 | 1.25 | 0.22 | 19% | 28% | 23% | 20% | 10% |
| db9 | 3.68 | 1.07 | −0.54 | 3% | 12% | 23% | 37% | 25% |
| db10 | 3.93 | 1.23 | −0.98 | 5% | 13% | 9% | 29% | 44% |
| db11 | 4.04 | 1.28 | −1.19 | 7% | 10% | 8% | 24% | 52% |
| db12 | 2.72 | 0.95 | −0.10 | 12% | 23% | 48% | 14% | 3% |
| db13 | 3.34 | 1.26 | −0.24 | 9% | 19% | 25% | 25% | 22% |
| db14 | 3.70 | 1.46 | −0.67 | 11% | 16% | 10% | 17% | 46% |
| db15 | 2.51 | 1.37 | 0.42 | 32% | 24% | 16% | 18% | 10% |
| db16 | 3.36 | 1.31 | −0.28 | 10% | 20% | 20% | 25% | 25% |
| GDBI-E score | 56.14 | 7.62 | −0.46 | |||||
| Variable | n | % | Missing n (%) | GDBI-E Score Mean (SD) |
|---|---|---|---|---|
| Gender | 20 (8%) | |||
| Female | 206 | 78% | 56.5 (7.4) | |
| Male | 37 | 14% | 54.8 (7.8) | |
| Marital status | 21 (8%) | |||
| Married | 90 | 34% | 56.0 (7.1) | |
| Living in a relationship | 70 | 27% | 55.6 (8.3) | |
| Single | 74 | 28% | 56.7 (6.8) | |
| Other | 8 | 3% | 59.4 (9.3) | |
| Educational degree | 21 (8%) | |||
| High school | 18 | 7% | 55.7 (7.2) | |
| College | 20 | 8% | 54.3 (6.3) | |
| Vocational training | 13 | 5% | 57.3 (6.8) | |
| Bachelor’s degree or equivalent | 103 | 39% | 56.3 (7.4) | |
| Master’s degree or equivalent | 63 | 24% | 56.7 (7.2) | |
| Doctorate/PhD | 20 | 8% | 55.0 (10.3) | |
| Other | 5 | 2% | 57.8 (7.7) | |
| General diet | 16 (6%) | |||
| Omnivore diet | 123 | 47% | 56.1 (7.2) | |
| Vegetarian diet | 31 | 12% | 53.1 (9.1) | |
| Vegan diet | 76 | 29% | 58.1 (6.7) | |
| Other | 17 | 6% | 54.8 (7.7) | |
| Food intolerance | 16 (6%) | |||
| No | 198 | 75% | 55.7 (7.1) | |
| Yes | 49 | 19% | 58.3 (8.5) | |
| Continent | 20 (8%) | |||
| Africa | 32 | 12% | 55.5 (6.4) | |
| Asia | 13 | 5% | 55.6 (7.5) | |
| Australia and Oceania | 35 | 13% | 56.2 (7.5) | |
| Europe | 128 | 49% | 56.6 (7.5) | |
| North America | 33 | 13% | 55.5 (8.3) | |
| South America | 2 | 1% | 62.0 (2.8) | |
| Native language | 20 (8%) | |||
| English | 171 | 65% | 56.0 (7.3) | |
| Other | 72 | 27% | 56.8 (7.8) |
| Scales | GDBI-E Score |
|---|---|
| convergent validity | |
| attitude towards healthy food | 0.33 *** |
| nutrition knowledge | 0.19 ** |
| discriminant validity | |
| interpersonal trust | 0.13 * |
| belief about a just world | 0.01 |
| criterion validity | |
| BMI | −0.17 ** |
| life satisfaction | 0.15 * |
| physical health | 0.27 *** |
| mental health | 0.31 *** |
| Scales | GDBI-E Cluster |
|---|---|
| convergent validity | |
| attitude towards healthy food | 0.26 *** |
| nutrition knowledge | 0.25 *** |
| discriminant validity | |
| interpersonal trust | 0.10 |
| belief about a just world | −0.06 |
| criterion validity | |
| BMI | −0.15 * |
| life satisfaction | 0.18 ** |
| physical health | 0.21 *** |
| mental health | 0.25 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marsall, M.; Engelmann, G.; Skoda, E.-M.; Stroebele-Benschop, N.; Teufel, M.; Bäuerle, A. Validation of the English Version of the General Dietary Behavior Inventory (GDBI-E). Int. J. Environ. Res. Public Health 2022, 19, 2883. https://doi.org/10.3390/ijerph19052883
Marsall M, Engelmann G, Skoda E-M, Stroebele-Benschop N, Teufel M, Bäuerle A. Validation of the English Version of the General Dietary Behavior Inventory (GDBI-E). International Journal of Environmental Research and Public Health. 2022; 19(5):2883. https://doi.org/10.3390/ijerph19052883
Chicago/Turabian StyleMarsall, Matthias, Gerrit Engelmann, Eva-Maria Skoda, Nanette Stroebele-Benschop, Martin Teufel, and Alexander Bäuerle. 2022. "Validation of the English Version of the General Dietary Behavior Inventory (GDBI-E)" International Journal of Environmental Research and Public Health 19, no. 5: 2883. https://doi.org/10.3390/ijerph19052883